
Abstract
Objectives
The clinical outcomes, safety, and efficacy of endovascular management are explored for symptomatic isolated superior mesenteric artery dissection (ISMAD).
Methods
In this retrospective study, 51 consecutive patients with symptomatic ISMAD received endovascular management from three institutions between January 2011 and December 2019.These patients were categorized into group A (endovascular treatment was used as the first-line therapy) and group B(endovascular treatment was used as the second-line therapy). The general epidemiological data, clinical manifestations, first-episode symptoms, treatment process, imaging findings, follow-up outcomes were analyzed from the medical records.
Results
A total of 51 patients with endovascular management were collected in this study. Significant differences were observed between the two groups with respect to the course (150 h vs. 57 h; p < 0.001), intestinal ischemia (26.32% vs. 6,25%; p = 0.04) and dissection length (45.26 ± 13.78 mm vs. 63.37 ± 12.73 mm; p < 0.001). Technical success rate was 90.2% (46/51). There was significant difference in the MOD (42.27 ± 23.41 min vs. 76.63 ± 28.62 min p < 0.001), MPSRT (4.67 ± 2.65 h vs. 7.32 ± 2.49 h, p = 0.02), LOS (9.52 ± 3.72 days vs. 11.86 ± 4.13 days; p = 0.01) between the two groups. The bleeding complication rate was 7.84% (one patient in group A and three patients in group B). A total of 48 (94.12%, 48/51) patients were followed up for a median of 36.51 months (range, 4–87 months). Positive events of the SMA were achieved in 81.25% (39/48), and negative events of the SMA were achieved in 18.75% (8/48) based on the follow-up contrast-enhanced CT scan.
Conclusions
Endovascular management of symptomatic ISMAD has a high technical success rate and efficient at controlling symptoms. Furthermore, as more positive events occur, endovascular management should be encouraged early when pain persists after conservative management or there are signs of disease progression.
Introduction
Isolated superior mesenteric artery dissection (ISMAD) that is not associated with aortic dissection is a very rare condition. Increasing patients were diagnosed with advanced imaging technology and better learning curve, and hence ISMAD may not be as rare as previously reported, in particular in Asia (China. Japan and South Korea). 1 , 2 Patients were predominantly middle aged men and the initial manifestation was abdominal pain of acute onset, which had always potentially catastrophic pathology with variable and unpredictable outcomes. 3 Nevertheless, no consensus was formulated for the treatment of this rare disease. Conservative management, including antithrombotic agents, blood pressure control measures, and fasting, as initial treatment is sufficient according to European Society for Vascular Surgery guidelines, 4 because it generally has a benign course both clinically and morphologically. 5 During follow-up, the complete remodelling with conservative management varies from 15.2% to 64%5–8 which result in concerns over recurrent of symptoms in the long term. By contrast, endovascular management provided approximately 95% symptom reliefs. 2 When cases presents with complex features, it can be performed as a preferred solution in individuals suffering from persistence or aggravation of symptoms and signs, or those at risk of a rupture of an aneurysmal false lumen. However, the prognosis of symptomatic ISMAD with endovascular management has not yet been fully explored. Therefore, this study retrospectively analyzed the clinical data of symptomatic ISMADs to investigate the following clinical outcome based on endovascular management.
Methods
Patients
This retrospective study was approved by all participating institutional review boards with a waiver of informed consent. Initially, a total of consecutive156 patients from three institutions were enrolled in the study between January 2011 and December 2019. ISMAD was diagnosed with one of the following signs in the superior mesenteric artery (SMA) on the CT scan, which reviewed in Picture Archiving and Communications Systems(PACS): (1) double lumen can be detected in SMA, in which contrast material is filled; (2) an intimal flap is presented in SMA; (3) crescent-shaped area along the SMA wall with higher attenuation than blood, showing no contrast enhancement after intravenous administration of contrast material. 9 One hundred and five patients were excluded because all of them received conservative management or surgical procedures. Finally, 51 symptomatic ISMADs comprised the final study population (Figure 1). In these patients, endovascular management was used as the first-line for 19 patients (Group A).Of these patients, stent placement was performed in 10 patients including two cases of covered stents; stenting combined with coiling was performed in 6 patients(Figure 2); coils embolotherapy was performed in 2 patients; and endovascular thrombolysis was performed in 1 patient. 10 Thirty-two patients with endovascular management as second-line treatment (Group B), stent implantation was performed in 19 patients (Figure 3); stenting combined with coiling was performed in 7 patients; coils embolotherapy was performed in 4 patients (Figure 4); and endovascular thrombolysis was performed in 2 patients.

Study flowchart.
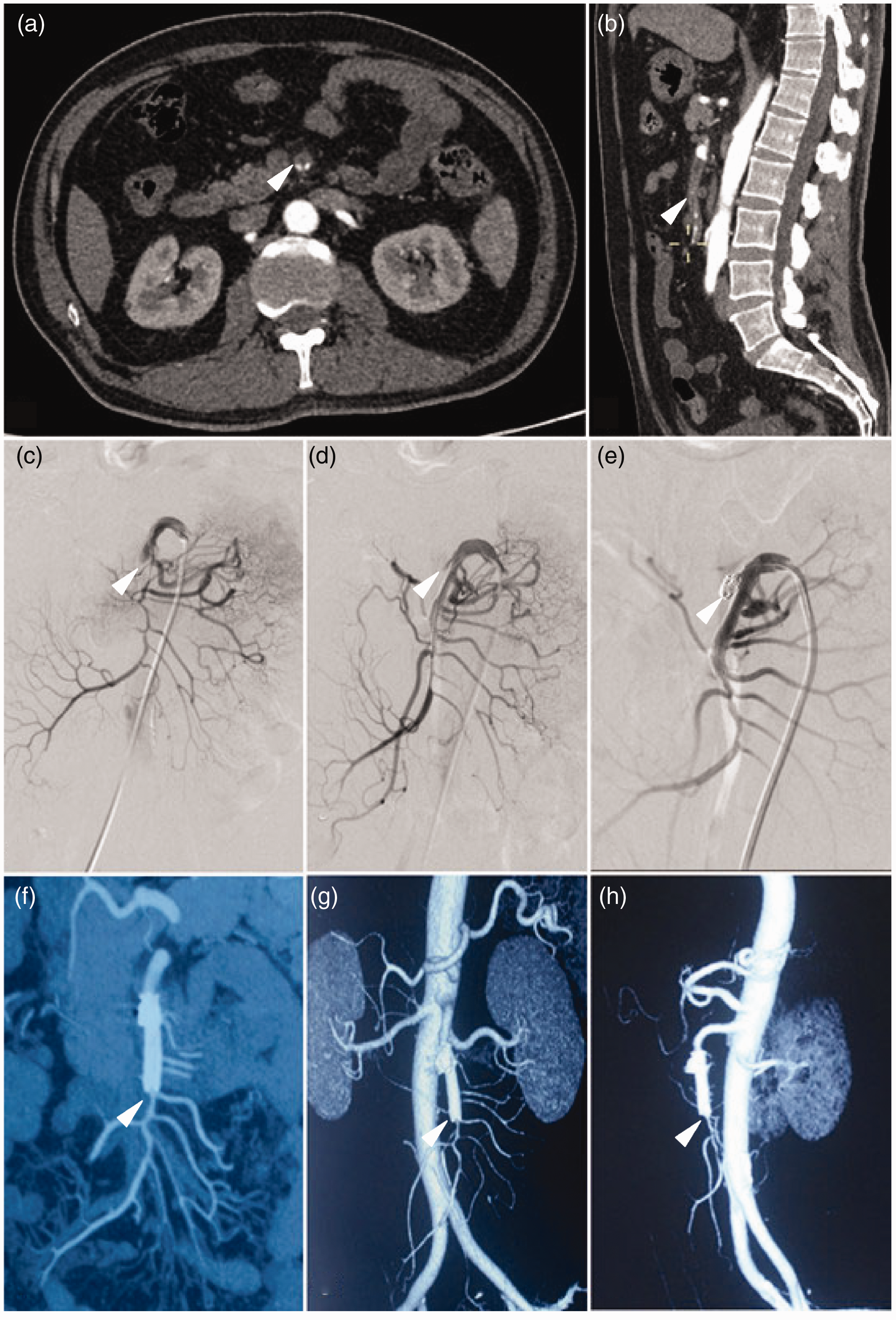
Emergency CT showed SMA occlusion leading to loss of distal blood flow (a, b arrow). Emergency selective mesenteric angiography was performed, which revealed a dissection in the SMA starting approximately 3.5 cm from its origin extending to the aortic orifice, without blood flow to the intestine via the SMA because of severe stenosis of the true lumen (c arrow). An 8 mm×60 mm EverFlex self-expanding bare stent and two coils were placed in the affected SMA, which resulted in excellent distal blood flow (d, e arrow). Follow-up CTA showed that the stent placed had no stenosis or thrombosis, thrombus in the false lumen, and blood flow in the distal end was unobstructed at 3, 6, 12 months postoperatively (f,g,h arrow).
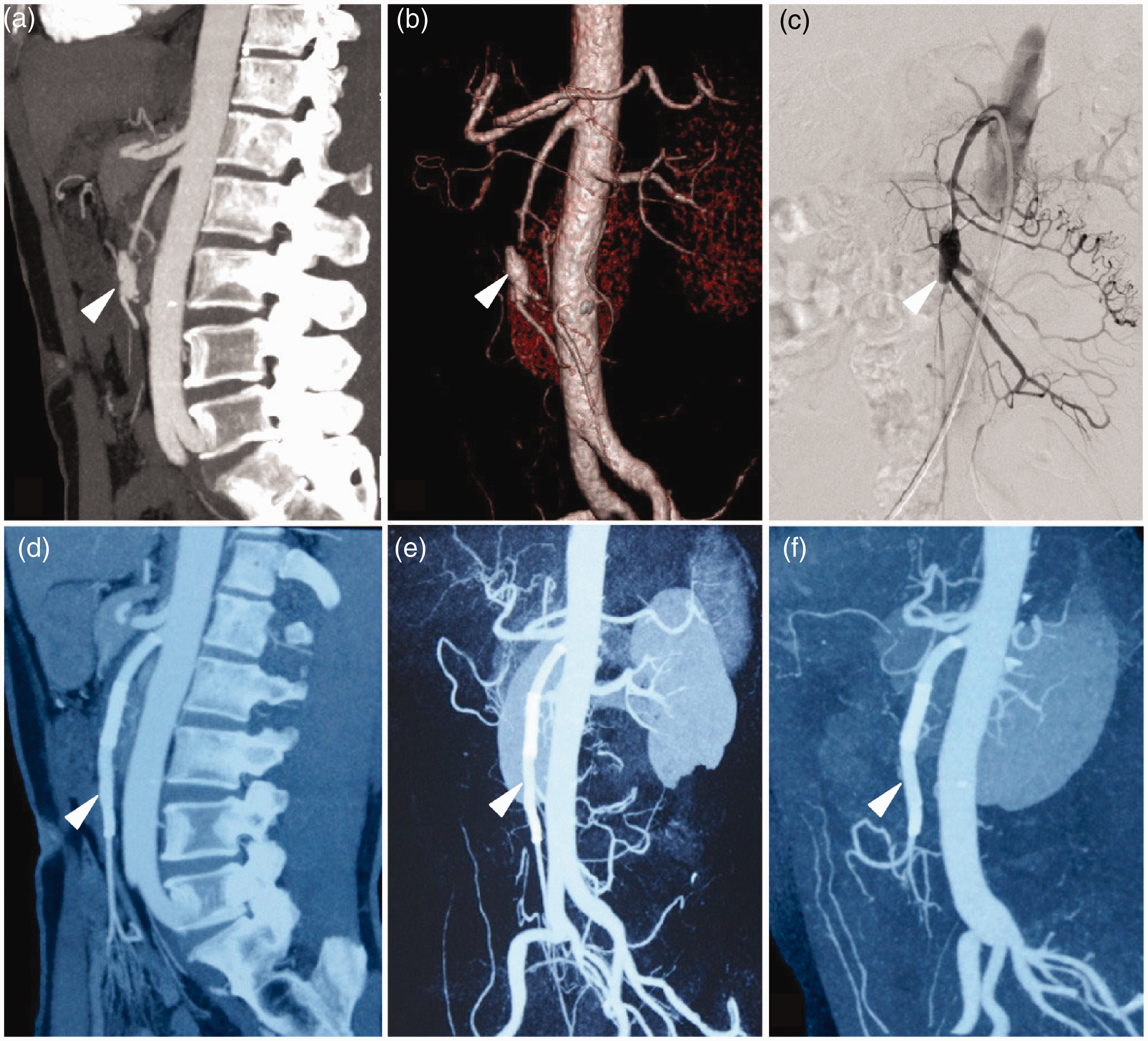
Example of failing conservative management of a symptomatic ISMAD with development of morphological worsening. A 56-year-old man presented with acute abdominal pain that had lasted for 3 h. Contrast-enhanced CT scan showed a ISMAD (type IIa) (a, b arrow). Abdominal pain worsened after four days of conservative management, and suprmesenteric angiography revealed true lumen compression severely (c arrow). Subsequently, two self-expanding bare stent (8 mm×60 mm EverFlex) was performed in the segment of the lesion. Follow-up CTA showed that the stent placed had no stenosis or thrombosis, thrombus in the false lumen, and blood flow in the distal end was unobstructed at 3, 12, 18 months postoperatively (d–f arrow).

After 18 months of conservative treatment, the ISMAD developed into dissecting aneurysm. A 49-year-old man presented with acute abdominal pain that had lasted for 3 h. Contrast-enhanced CT scan showed a SMA dissecting aneurysm (a, b arrow). Subsequently, embolotherapy was performed in the segment of the lesion. Follow-up CTA showed that the thrombus in the false lumen and blood flow in the distal end were unobstructed at 12 months postoperatively (c–d arrow).
Definition
First-line treatment was defined as endovascular intervention immediately after diagnosis of ISMAD as these patients present a large dissecting aneurysm, peritonitis and persistent symptoms. Second-line treatment was defined as endovascular intervention after the failure of conservative treatment. Failure of conservative management was defined as the persistence or aggravation of symptoms and signs, increasing size of aneurysmal dilation, or appearance of local peritonitis after conservative management. 11 Persistent symptoms were defined as no change in or the aggravation of symptoms after a week of conservative treatment with antithrombotic agents. 12 Technical success was defined as successful deployment of intervention content (stents, coils and thrombolytic catheters) to the target locations. Operative duration was the period between the aortic artery angiography and the completion angiography. Procedure-related complications were classified as major and minor according to the guidelines of the Society of Interventional Radiology. 13 Systemic heparinization was defined as the administration of a weight-based dose of heparin (120 IU/kg), followed by 1000 IU per hour continuously during the procedure, controlling activated clotting time to a target of 150 s approximately.
Image analysis
Two experienced radiologists and two vascular surgeons reviewed all CT examinations and reached consensus. The lesions were categorized based on the Yun classification as follows: type I, patent true and false lumen revealing entry and re-entry sites (entry and re-entry tear visible, patent false lumen), type IIa (only entry tear visible, patent false lumen), type IIb (thrombosis of false lumen, patent true lumen), and type III (occlusion of true and false lumen). 14 ISMAD changes on CT scan were assessed and compared with the initial findings. Morphological characteristics were evaluated including location of laceration (distance between the ostium of the SMA and the origin of the dissection), length of dissection, TLRD (true lumen residual diameter, true lumen size compared with the adjacent normal SMA size), 15 branch involvement, signs in favor of the small bowel ischemia (wall thickening, thinning of the intestinal wall, abnormal contrast enhancement of bowel wall, intramural hematoma, pneumatosis, perforation, and peritonitis), 16 obliteration of the true lumen and aneurysm dissection formation (at least 50% larger than the adjacent normal mesenteric artery diameter). 17 The disease prognosis was categorized into positive or negative event through the analysis of initial and follow-up CT scans. Positive event was defined as the following: (1) complete remodeling (the absence of residual arterial dissection with no SMA stenosis and hemodynamics was restored to achieve functional repair completely), (2) Incomplete remodeling (improved true luminal patency and clinical symptoms compared with pre-operative status). Negative event included stent restenosis, dissecting aneurysm formation, new dissection and death.
Technique
All procedures were performed under an angiographic suite with a fixed digital subtraction angiography (DSA) platform (Artis Zee, Siemens, Muenchen, Germany). After systemic heparinization, the right common femoral artery access was gained via a 5 F sheath. A pigtail catheter was sent to above the celiac trunk for having a conventional DSA imaging of the abdominal aorta, and its visceral branches as to detect potential collateral perfusion into the SMA. Subsequently, the catheter was exchanged to Yashiro catheter (Yashiro type, Terumo Co., Tokyo, Japan) in order to selectively perform the SMA angiography. A therapeutic strategy was determined based on nature of the lesion. With the Yashiro catheter in situ, an 8 F sheath was then exchanged. The SMA true lumen was searched, and delivered to the primary dissection entry with a 0.035-inch Radifocus guidewire (Terumo, Tokyo, Japan). With the Radifocus guidewire in situ, an introducer (Flexor, Cook Medical, Bloomington, IN, USA) was advanced along the guidewire into distal SMA true lumen. A stent introducer was then advanced over the stiff guidewire, and a self-expandable stent was deployed. Self-expandable bare stents (Protege EverFlex, ev3, MN, USA) and covered stents (Jostent, Abbott Vascular, Abbott Park, IL, USA (n = 2) were placed. In general, the stent diameter was approximately 10% larger than that of normal SMA routinely and was at least 5 mm longer than each at the distal and proximal margins. In addition, coil embolization was employed in patients with dissecting aneurysm and some with type IIa if the false lumen and/or entry tear were overwhelmingly large. If the angle between the SMA and the aorta was smaller than 45°, the brachial artery approach was chosen. Finally, completion mesenteric angiography was repeated to evaluate the results, which included the stented patency as well as distal blood supply.
Anticoagulant regimen: during hospitalization, low molecular weight heparin (enoxaparin, Sanofi, Paris, France) at a dose of 100 IU/kg, subcutaneous injection, every 12 h; after discharge, oral warfarin (Qilu Pharmaceutical, Shandong, China), INR (International Sensitivity Index) controlled at 2.0–3.0, or oral rivaroxaban (Bayer Consumer Health, Germany) at a dose of 15 mg/day for a time period of three months. Antiplatelet regimen: during hospitalization, oral aspirin (Bayer Consumer Health, Germany) at a dosage of 100 mg/day and oral clopidogrel (Sanofi Pharma Bristol-Myers Squibb SNC, French) at a dosage of 75 mg/day; after discharge, oral aspirin at a dosage of 100 mg/day, for a time period ≥ 12 months; oral clopidogrel 75 mg/day, for a time period ≥ 6 months. Patients with concomitant disease, such as hypertension, diabetes mellitus, hyperlipidemia, were received by the appropriate guidelines-based therapy. Simultaneously, quitting smoking was necessary for patients with a history of smoking.
Follow-up
Patients without recurrent pain were followed up by contrast-enhanced CT scans at 3 months, 6 months, and 12 months after discharge and annually thereafter. More frequent evaluations were performed when needed. Those whose symptoms indicated worsening lesions underwent imaging evaluations immediately. Morphological changes, clinical presentations and complications were recorded.
Statistical analyses
Statistical analyses were performed using SPSS 22.0 software (SPSS Inc., Chicago, IL, USA). Continuous variables are presented as the medians and ranges in the cases of nonparametric distributions, and comparisons were made using the Mann–Whitney test. Continuous variables are presented as the means and standard deviations in cases of parametric distributions, and comparisons were made using the independent t-test. Categorical variables were compared with the Chi-square test or Fisher’s exact test, and they are reported as frequencies and percentages. A p value of < 0.05 was considered to be statistically significant.
Results
Patients
From January 2011 to December 2019, a total of 51 ISMADs with endovascular management were collected in this study; in all of these patients, 46 (90.2%, 46/51) patients were men. Of these, the median age was 57.79 years old (ranging from 29 to 68). Risk factors are associated with symptomatic ISMAD including tobacco smoking 57.89% vs. 53.13% (p = 0.74) and hypertension 47.37% vs. 43.75% (p = 0.8) in both groups. Among the 51 patients, 46 (90.2%, 46/51) had abdominal pain as the initial symptom accompanied by nausea and vomiting 19 (56.86%) patients. Moreover, 3.92% (2/51) had type I dissection, 33.33% (17/51) had type IIa dissection, 52.94% (27/51) had type IIb dissection, and 9.8% (5/51) patients had type III dissection. Branch involvement and aneurysm formation were seen in 23.53% (12/51) and 11.76% (6/51) of patients in two groups, respectively. In addition, In group A, the mean distance between the ostium of the SMA and the origin of the dissection was 25.61 ± 12.06 mm, and the mean length of ISMAD was 63.37 ± 12.73 mm. The course was 150 h (range 28–312 h). Intestinal ischemia in the affected vessel was detected in 26.32%. In group B, the mean distance between the ostium of the SMA and the origin of the dissection was 29.89 ± 13.37 mm, and the mean length of ISMAD was 45.26 ± 13.78 mm. The course was 57 h (range 6–97 h). Intestinal ischemia in the affected vessel was detected in 6.25%.The clinical features and imaging findings of the patients are summarized in Table 1.
Clinical features and imaging finding of patients with isolated superior mesenteric artery dissections with endovascular treatment.
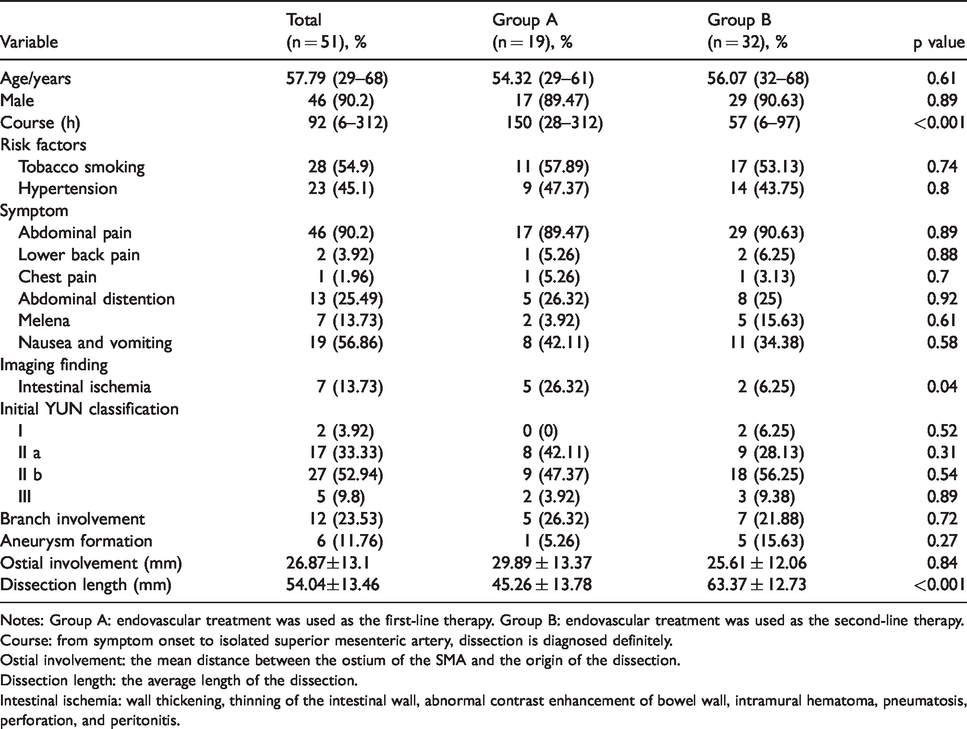
Notes: Group A: endovascular treatment was used as the first-line therapy. Group B: endovascular treatment was used as the second-line therapy.
Course: from symptom onset to isolated superior mesenteric artery, dissection is diagnosed definitely.
Ostial involvement: the mean distance between the ostium of the SMA and the origin of the dissection.
Dissection length: the average length of the dissection.
Intestinal ischemia: wall thickening, thinning of the intestinal wall, abnormal contrast enhancement of bowel wall, intramural hematoma, pneumatosis, perforation, and peritonitis.
Outcomes
The overall technical success was 90.2% (46/51). Five patients (one type III in group A, two type III and two type IIb in group B) were attributed to the extensive thrombus inside the true lumen of the dissection SMA and the guidewire failed to cross the occluded lesion. The treatment was transferred to conservative management with anticoagulant agents. Persistent symptoms were improved gradually in 7 days and 12 days after medication. There was significant difference in the MOD (42.27 ± 23.41 min vs. 76.63 ± 28.62 min p < 0.001), MPSRT (4.67 ± 2.65 h vs. 7.32 ± 2.49 h, p = 0.02), LOS (9.52 ± 3.72 days vs. 11.86 ± 4.13 days; p = 0.01) between the two groups (Table 2).The overall bleeding complication rate was 7.84% (one patient in group A and three patients in group B), which experienced minor bleeding at the catheter insertion site, which was controlled in all of the cases by simple elevation of the limb and application of a compressive bandage and did not require further treatment. In group A, one patient who presented with septic shock after stent placement died of multiple organ failure. 18 Another patient with peritonitis after stent placement performed small intestine resection; unfortunately, this patient died of short bowel syndrome.
Treatment of isolated superior mesenteric artery dissections.
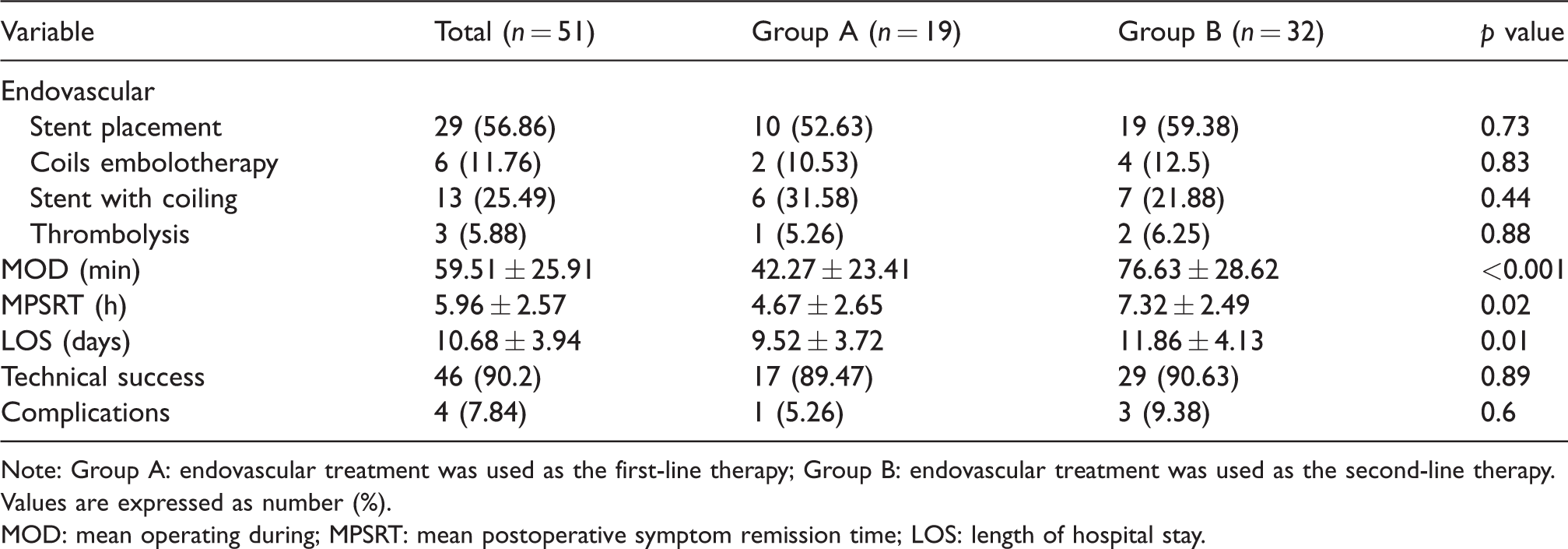
Note: Group A: endovascular treatment was used as the first-line therapy; Group B: endovascular treatment was used as the second-line therapy.
Values are expressed as number (%).
MOD: mean operating during; MPSRT: mean postoperative symptom remission time; LOS: length of hospital stay.
Clinical follow-up
A total of 48 (94.12%, 48/51) patients were followed up for a median of 36.51 months (range, 4–87 months). Positive event of the SMA was achieved in 81.25% (39/48), and negative event of the SMA was achieved in 18.75% (8/48) based on the follow-up contrast-enhanced CT scan. In the positive event, complete remodeling of the SMA was achieved 66.67% vs. 70% in the groups A and B. Moreover, incomplete remodeling accounted for 16.67% (3/18) and 10%(3/30) in the both groups, respectively. In group B, one patient with Yuntype IIa converted into dissecting aneurysm, and two patients developed new dissection; One patient in group A and two patients in group B treated with stents alone demonstrated recurrence, showing proximal stent restenosis. Endovascular management was performed again in these patients (Table 3).
Follow-up of patients treated for isolated superior mesenteric artery dissections.
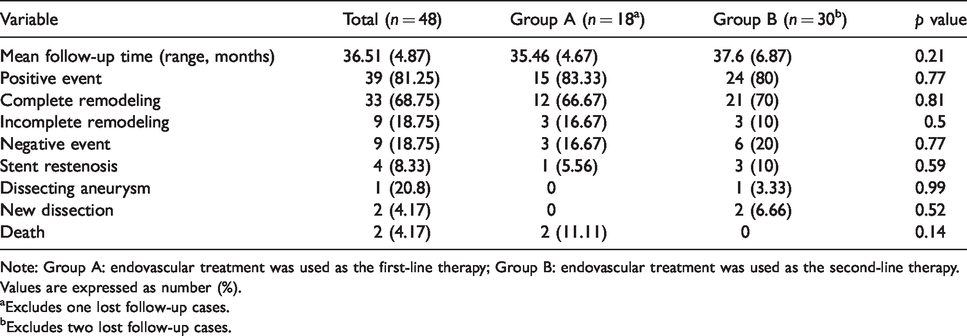
Note: Group A: endovascular treatment was used as the first-line therapy; Group B: endovascular treatment was used as the second-line therapy.
Values are expressed as number (%).
aExcludes one lost follow-up cases.
bExcludes two lost follow-up cases.
Discussion
The course of symptomatic ISMAD is more indolent than that of aortic dissection. Given its self-limited, the majority of reports have shown good clinical and morphological outcomes treated with conservative management.19–21 However, conservative management did not prevent the progression of the lesion, especially the SMA true lumen stenosis and dissection aneurysm formation. According to the management strategy based on clinical stages previously reported by our team, during the acute and subacute stages, the major complications were intestinal ischemia or necrosis owing to which cannot provide a time window for patients to establish collateral circulation. 18 In the present study, symptoms in group A of the patients were more severe than those of group B. One reason for this is that there was a time delay between onset of symptoms and admission to the department (150 h in the group A vs. 57 h in the group B; p < 0.001), which results in delayed treatment. In addition, the only death cases in this study were also in the group A due to intestinal necrosis, so when persistent symptoms or conservative treatment failed, endovascular management should be encouraged early in the acute or subacute stage. The aim of endovascular management is to attach the intimal rupture, prevent further progression of the dissection, and provide immediate relief from mesenteric ischemia. One study reported that the cumulative primary stent patency rate was 99.1%, and the cumulative event free survival rate was 99.0%, 95.8%, and 95.8% at one, three, and five years in patients with stents. 22 Therefore, endovascular management would be a safe and preferred alternative compared to surgical repair for ISMDs with conservative treatment failure.
No ideal stents for the SMA pathologies can be applied yet. Concerning the good flexibility, adapting to SMA physiological curvature and tapering anatomy and providing sufficient axial force, the self-expanding bare stents were recommended routinely. In contrast, there is evidence that covered stents may compromise the branches of the SMA and also aggravate bowel ischemia. 23 In our experience, it suggest that covered stent might be considered for type IIa or dissecting aneurysm in SMA trunk, given its generally proximal and local properties, whereas self-expanding bare stents are recommended for type IIb and type III dissections as there is no blood flow in the false lumen. When the type IIa dissection involves in multiple branches originating, the bare stents combined with the coils embolization can promote the thrombogenesis of the false lumen without affecting the collateral blood supply. In the current study, type I dissection did not require intervention, presumably due to progressive morphologic remodelling and satisfactory clinical improvement in the natural course of disease. The majority of endovascular management were performed for type II and type III modalities, mainly because of intestinal ischemia causing persistent symptoms. Since this was a retrospective study, the intensity of pain had not been quantified for additional analysis, yet all patients who previously had persistent symptoms resolved after endovascular management.
Technical success was 90.2% in this study. Failures occurred in five patients, guide wire failed access attributed to the advanced extensive thrombus in the true lumen. All of the five patients were converted to conservative management with anticoagulant agents; however, three of these patients occurred postprandial abdominal pain during follow-up. Failure of endovascular management in the ISMAD may not require urgent surgical conversion, and conservative management would be more preferred despite longer symptomatic duration and length of stay. However, potential problems, such as intestinal ischemia, postprandial abdominal pain, food aversion, and weight loss, may occur during the longer follow-up. Furthermore, patients in group B were more difficult to operate than in group A in this study. Significant differences were observed between the two groups with respect to the MOD (42.27 ± 23.41 min vs. 76.63 ± 28.62 min p < 0.001), MPSRT (4.67 ± 2.65 h vs. 7.32 ± 2.49 h, p = 0.02), and LOS (9.52 ± 3.72 days vs. 11.86 ± 4.13 days; p = 0.01). Perhaps the thrombus polarization in the false lumen may be difficult for the guidewire to reach the distal part of the lesion and difficult to use the self-expanding stent to expand the true lumen.
Several limitations have to be noticed. First, the included study was a retrospective analysis leading to a risk of selection bias. Even so, prospective studies were impossible owing to the extremely low incidence of the disease. Secondly, the small sample size could be a major limitation to provide the reliability of the endovascular treatment results. Meanwhile, the prognosis of ISMAD was determined by contrast-enhanced CT scan rather than by mesenteric angiography. Finally, the clinical follow-up was arranged in the first and sixth months after discharge, and every year thereafter; therefore, the exact time of SMA remodeling was unknown in this study.
In conclusion, endovascular management of symptomatic ISMD has a high technical success rate and efficient at controlling symptoms. Furthermore, as more positive events occur, endovascular management should be encouraged early when pain persists after conservative management or there are signs of disease progression.
Footnotes
Acknowledgements
The authors are grateful to all the participants for their involvement in the study. The authors would also like to thank the Shengli Oilfield Central Hospital and Union Hospital, Tongji Medical College, Huazhong University of Science and Technology for their collecting data.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics approval
Ethics approval was provided by the Binzhou Medical University Hospital ethics committee.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.