
Abstract
Objectives
The objective of this study was to evaluate the efficacy and safety in patients with acute lower extremity deep venous thrombosis who underwent pharmacomechanical thrombectomy (PMT, AngioJet mechanical thrombus aspiration).
Methods
In this retrospective, 424 consecutive patients with acute lower extremity deep venous thrombosis from three institutions were enrolled in the study from January 2015 to December 2018. Of these, patients were divided into two groups, AngioJet group (n = 186) and catheter-directed thrombolysis (CDT) group (n = 238). Evaluation indexes including limb circumference difference, length of stay (LOS), urokinase dosage, periprocedural complications, follow-up imaging findings and villalta scores were analyzed from the medical records.
Results
A total of 424 patients diagnosed with acute lower extremity deep venous thrombosis were collected in this study. These patients were categorized into AngioJet group and CDT group. Significant differences were observed between the two groups with respect to the thigh circumference difference (5.32 ± 1.85 cm vs. 4.69 ± 2.15 cm; p = 0.04), calf circumference difference (2.79 ± 1.54 cm vs. 2.35 ± 1.25 cm; p = 0.01), thigh detumescence rate (72.19 ± 19.55% vs. 65.35 ± 17.26%; p = 0.00) and calf detumescence rate (62.79 ± 18.56% vs. 55.75 ± 17.27%; p = 0.00). The mean dose of urokinase in AngioJet group was 95.16 ± 45.89 million IU significantly less than that in the CDT group 293.76 ± 42.71 million IU (p = 0.00). The overall bleeding complication rate was 9.91% (19 patients in AngioJet group and 23 patients in CDT group), which included three major (0.71%, 3/424) and 39 minor (9.2%,39/424) events. In the AngioJet group, serum creatinine (sCr) concentration and urine erythrocyte from the hemolysis caused by the mechanical process were higher than baseline data at admission (p = 0.00, p = 0.00). The postoperative red blood cell and hemoglobin in two groups were lower than baseline data (p = 0.00, p = 0.00). Compared with CDT, AngioJet thrombectomy has significantly lower estimated incidence of PTS in the follow-up.
Conclusion
AngioJet thrombectomy has stronger clearance ability for acute lower extremity deep venous thrombosis leading to significant reduction in the consumption of hospital resources, total dose of thrombolytic agents, and infusion time, thereby preventing adverse bleeding events, but patients with renal insufficiency should be careful. Ideal short-term and medium-term efficacy and safety are certain.
Keywords
Introduction
Over the years, different options for thrombus treatment have been introduced to restore patency, save valve function, and reduce the occurrence of post-thrombotic syndrome (PTS). Although approximately half of the patients received conservative treatment (anticoagulation and stockings) with definite improvement in symptoms, some patients still require intervention, especially those with extensive iliofemoral DVT that still require more aggressive therapy. 1 The conventional conservative management of acute lower extremity DVT aims to prevent thrombus propagation and to decrease the risks of pulmonary embolization (PE) and DVT recurrence. However, this treatment is ineffective at reducing thrombus burden and consequently does not prevent PTS. 2
Surgical thrombectomy is mainly used for phlegmasia cerulea dolens and phlegmasia alba dolens, but the thrombus recurrence is higher due to large trauma. Recently, Trends in endovascular interventions advocate for more aggressive management of acute lower extremity DVT(within 14 days of symptom onset) with enhanced clearing thrombus; the aim is to relieve acute symptoms and prevent long-term PTS.3–5 The use of AngioJet thrombectomy to treat acute lower extremity DVT may reduce long-term morbidity in DVT patients by restoring the patency of the veins. 6 However, the prognosis of acute lower extremity DVT with AngioJet thrombectomy management has not yet been fully explored. In this study, we analyzed the short-term and mid-term efficacy and safety of AngioJet thrombectomy for the treatment of acute lower extremity DVT and investigate the development of PTS.
Methods
Patients
The present retrospective study was approved by the institutional review board, and the requirement for written informed consent was waived. A total of 424 consecutive patients with acute lower extremity DVT from the three institutions were enrolled in this retrospective study from January 2015 to December 2018. These patients were divided into two groups: the AngioJet group (n = 186) and the CDT group (n = 238). Clinical data were collected to compare the short-term and mid-term efficacy and safety of the two options. Evaluation indexes: limb circumference difference, length of stay (LOS), urokinase dosage, periprocedural complications, follow-up imaging findings and villalta scores. The patients were diagnosed by clinical symptoms, signs, and image examination. Computed tomography angiography (CTA) was performed pre- and post-operatively based on clinical suspicion of pulmonary embolism (PE). Postoperative red blood cell, hemoglobin, serum potassium, serum creatinine, blood urea nitrogen and urine erythrocyte of every patient were collected. The baseline value of each index was defined as the value at admission. The worst laboratory values within 48 h after intervention were chosen for subsequent analysis.
Inclusion and exclusion criteria
Inclusion criteria: (1) no previous history of thrombosis or surgery; (2) unilateral lower extremity DVT in the acute stage; (3) life expectancy ≥1 year; (4) no serious cardio-cerebrovascular, liver, kidney and lung and other important organ basic diseases; (5) no anticoagulation contraindications. Exclusion criteria: (1) bilateral lower extremity DVT; (2) DVT incidence ≥2 weeks or recurrence; (3) history of serious trauma or major surgery in the recent four weeks; pregnancy; uncontrollable hypertension (systolic blood pressure >180 mm Hg or diastolic blood pressure >110 mm Hg); and history of cerebral hemorrhage in the last three months;7,8 (4) life expectancy < 1 year; (5) contraindications to anticoagulant drugs, urokinase, and iodinated contrast media.
Endovascular thrombus removal
Initially, all patients were treated with anticoagulation(200 IU/kg dalteparin; Pfizer, New York, NY, USA or enoxaparin 100 IU/kg; Sanofi, Paris, France) consistent with current guidelines. 9 For safety, a retrievable or temporary inferior vena cava filter(IVCF, [Aegisy, Lifetech Scientific, Shenzheng, China]) was routinely implanted via a contralateral femoral puncture to prevent PE according to our national guideline. 10 AngioJet thrombectomy or CDT procedure was performed with IVCF protection, and during this process, venography was undertaken to evaluate thrombus distribution and therapeutic effect. The IVCF was removed after the procedure for all patients.
AngioJet group
Femoral vein or popliteal vein approach, 6Fr AngioJetTM thrombus suction catheter (Boston Scientific, USA 6Fr SolentTM) was introduced with 0.035 inch guide wire (Japanese Terumo Company) in the thrombosed vein segment. A power-pulsed spray technique was employed in involving thrombus using an AngioJet 6-F thrombectomy catheter with the AngioJet Ultra System (Boston Scientific, Natick, MA, USA). Doses of 250,000 IU of urokinase (Livzon Pharmaceutical Group. GuangZhou, China) diluted in 100 mL normal saline were infused throughout the thrombus during the process of AngioJet catheter withdrawal at a moving speed of 1 mm/s. After 15 min of dwell time allowing for initial thrombus dissolution, the AngioJet catheter was introduced to perform a mechanical rheolytic thrombectomy of the thrombosed venous segment. This sequence could be repeated until the thrombus cleared mostly (residual thrombus <30%), but the longest effective working time was limited to 300 s. CDT was underwent if significant residual thrombus remained on subsequent venograms. The patients were treated with hydration, diuresis and use of sodium bicarbonate, and blood routine test, liver and kidney function, coagulation function was detected post-operatively.
CDT group
Femoral or popliteal vein approach, an infusion catheter (UniFuse, AngioDynamics, Latham, NY, USA) with multiple-side hole was positioned within the thrombosed venous segment. Urokinase was micropumped through the infusion catheter (50 ml normal saline +250,000 IU, per 12 h), with heparin infusion at 300–500 IU/h through the access sheath. The activated partial thromboplastin time and fibrinogen level were measured every 4 h. When the fibrinogen level reached 1.5 g/L, the urokinase dosage was halved, and when it was decreased to 1.0 g/L, urokinase was replaced with heparinized saline. Venography was reviewed within 24 h after the procedure of CDT to monitor the progress of the lesion to adjust the position of the infusion catheter. CDT was terminated with one of the following conditions: (1) fibrinogen level <1.0 g/L; (2) serious bleeding complications or catheter-related infection; (3) complete dissolution of thrombus; (4) thrombolysis had no change on two successive venography studies.
Percutaneous transluminal angioplasty (PTA) (MUSTANG balloon, Boston Scientific, Natick, MA, USA) and stent placement (WALLSTENT stent Boston Scientific, Natick, MA, USA) were performed to treat underlying iliocaval compression or stenosis (>50%) (Figure 1). Stents (18–20 mm and 14–16 mm in diameter) were placed in the iliocaval and iliofemoral veins covered the entire diseased venous segment (20% larger and 2 cm longer than the stenotic segment). Oral warfarin, INR (International Normalized Ratio) was maintained 2.0--3.0, or oral rivaroxaban at a dose of 15 mg/day for a time period of 12 months after discharge. All patients were advised to use elastic compression stockings with a below knee (30–40 mm Hg at the ankle) for at least one year consecutively.
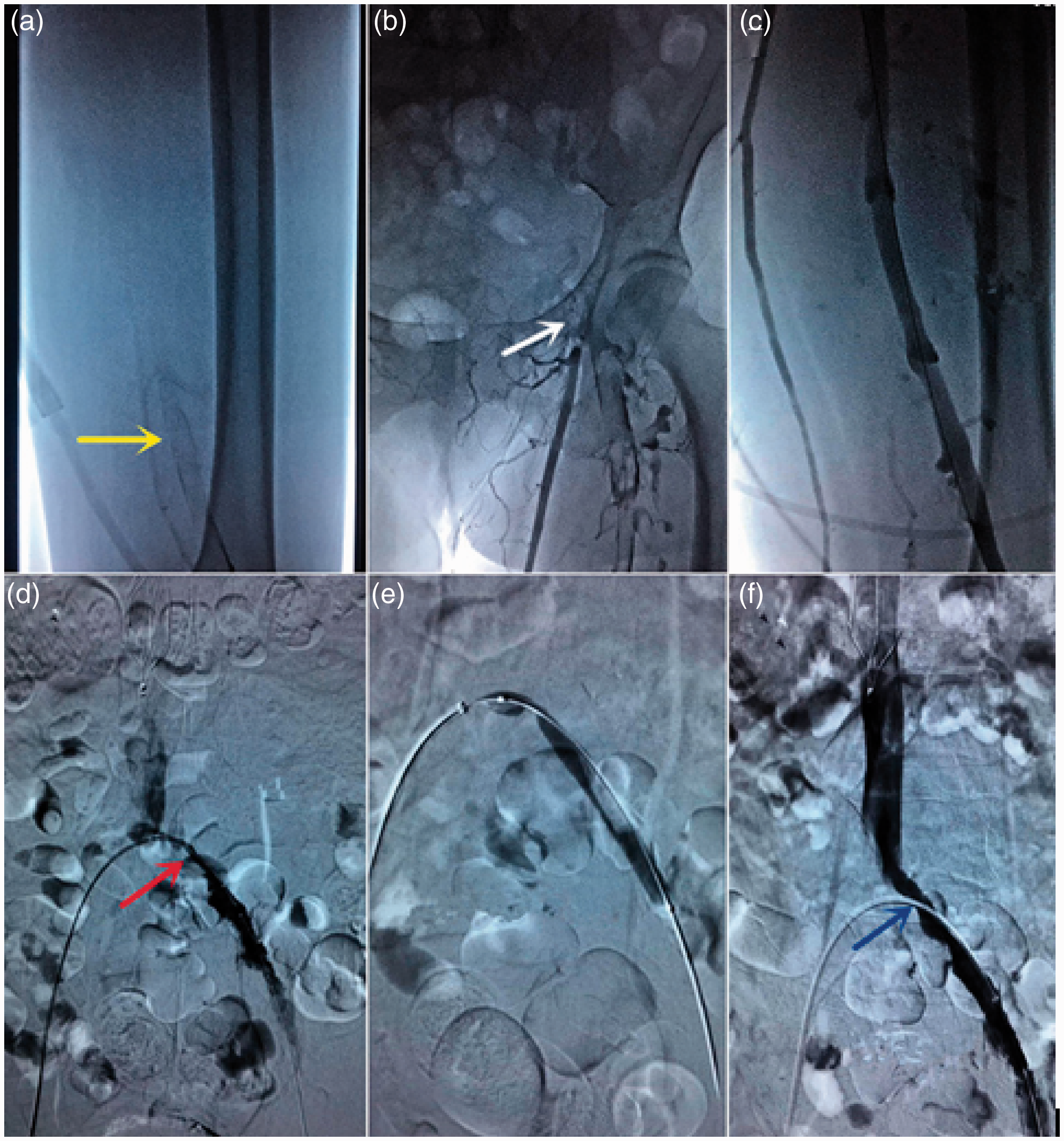
A 54-year-old male patient with acute pain and leg swelling in the left lower extremity due to acute Iliac/diatal femoral deep vein thrombosis (DVT). Initial venography in the prone position shows acute iliofemoral DVT (yellow arrow a; white arrow b). A venogram shows femoral venous patency, valve intact and smooth (c), but the common iliac vein is stenosis (red arrow d).The stenotic iliac vein was dilated with an angioplasty balloon (e). A venogram after stenting shows no stenosis or residual thrombus (blue arrow f).
Outcomes assessments
Technical success is defined as uncomplicated access to the deep venous system (femoral vein or popliteal vein), and uncomplicated implementation of the AngioJet device for thrombectomy. Before and after the intervention, limb circumference was measured at 10 cm below the knee and 15 cm above the knee on both sides of the lower extremity, respectively. Next, the circumference difference of the affected limb and the healthy limb were calculated. The detumescence rate = (limb circumference difference before intervention − limb circumference difference after intervention)/limb circumference difference before intervention × 100%.
Vessel patency following thrombectomy was evaluated in accordance with the society of interventional radiology (SIR) grading system following thrombolysis (Grade I indicated <0% lysis; grade II indicated 50–90% lysis; and grade III indicated 100% lysis, without residual thrombus). 11 Complications were recorded in line with the SIR clinical practice guidelines. 12 A serious adverse event was defined as any event that is fatal or life threatening, results in persistent or significant disability, requires intervention to prevent permanent impairment/damage, or results in readmission or prolongation of hospitalization. Accordingly, nonserious events require no or nominal treatment, without additional/prolonged hospitalization. A major bleeding event was defined as intracranial bleeding or bleeding severe enough to result in death, surgery, cessation of therapy, or blood transfusion. Other bleeding events were classified as minor bleeding. Local ecchymoma and ecchymosis on the skin around the puncture site were defined as puncture site bleeding.
During follow-up, imaging was mainly performed to evaluate the venous patency using duplex ultrasound imaging, and attached venography was undertaken when it was difficult to obtain adequate images of venous patency with ultrasound, and for clinically suspected recurrence of thrombosis and restenosis. To determine the extent of PTS, Villalta score (range 0–33) was determined after 12 months. PTS was assessed via the Villalta score(no PTS (score 0–4), mild PTS (score 5–9), moderate PTS (score 10–14) or severe PTS (score ≥15, or presence of ulcer).13,14
Follow-up
Patients were seen in the outpatient clinic and were followed up by deep vein Doppler ultrasound of the lower extremity at three months, six months, and 12 months after discharge and annually thereafter. For the patients who underwent PTA, clinical follow-up was scheduled every six months after discharged. Those whose symptoms indicated worsening lesions underwent imaging evaluations immediately.
Statistical analyses
All statistical analyses were performed using SPSS 22.0 software (SPSS Inc., Chicago, IL, USA). Continuous variables are presented as the medians and ranges in the cases of nonparametric distributions, and comparisons were made using the Mann-Whitney test. Continuous variables are presented as the means and standard deviations in cases of parametric distributions, and comparisons were made using the independent t-test. Categorical variables were compared with the chi-square test or Fisher’s exact test, and they are reported as frequencies and percentages. The value of p < 0.05 was defined as a statistically significant value.
Results
Patients
From January 2015 to December 2018, 424 consecutive patients diagnosed with acute lower extremity DVT were collected in this study. These patients were categorized into AngioJet group and CDT group. Of these patients, 186 patients (91 men, median age, 53.5 years, range 21–77 years) were included in the AngioJet group; the remaining 238 patients (112 men, median age, 57 years, range 28–79 years) with acute lower extremity DVT were included in the CDT group. Notably, the left limb was most commonly affected (87.63% vs. 84.45%, p = 0.35) in two groups. Segment of thrombosis in both groups included Iliac/femoral vein (71.51% vs. 71.43%), and Iliofemoral/proximal popliteal vein (28.5% vs. 28.57%). However, the data in the two groups were not statistically significant (p = 0.6, p = 0.66, p = 0.99). Risk factors associated with acute lower extremity DVT were no reason (36.02% vs. 40.76%, p = 0.32), surgery (38.17% vs. 36.98%, p = 0.8), trauma(9.14% vs. 8.82%, p = 0.91), postnatal (10.22% vs. 9.66%, p = 0.85) and malignancy (6.45% vs. 3.78%, p = 0.21), respectively. In addition, approximately 11% of patients were diagnosed with PE, and 42% of patients accompanied by iliac vein compression syndrome (IVCS). Baseline patient characteristics and the risk factors for DVT are shown in Table 1.
Baseline patient characteristics and the risk factors for ADVT.
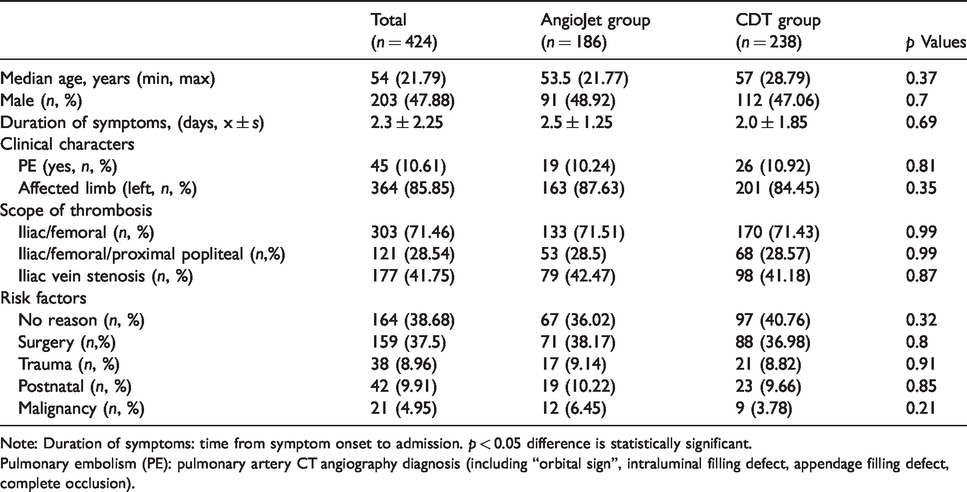
Note: Duration of symptoms: time from symptom onset to admission. p < 0.05 difference is statistically significant.
Pulmonary embolism (PE): pulmonary artery CT angiography diagnosis (including “orbital sign”, intraluminal filling defect, appendage filling defect, complete occlusion).
Clinical outcomes
Technical success rates were 100% in the AngioJet and CDT groups. All IVCFs were removed after the completion of treatment without complications. Thrombus clearance grade was achieved in grade I (19.35 vs. 16.81), grade II (57.53 vs. 65.55) and grade III (23.12 vs. 17.65), respectively, which were statistically significant (p = 0.02). Moreover, significant differences were observed between the two groups with respect to the thigh circumference difference (5.32 ± 1.85 cm vs. 4.69 ± 2.15 cm; p = 0.04), calf circumference difference (2.79 ± 1.54 cm vs. 2.35 ± 1.25 cm; p = 0.01), thigh detumescence rate(72.19 ± 19.55% vs. 65.35 ± 17.26%; p = 0.00) and calf detumescence rate (62.79 ± 18.56% vs. 55.75 ± 17.27%; p = 0.00). Stents were implanted 74 vs. 93 limbs in the both groups (p = 0.88, Table 2).
Postoperative efficacy evaluation of Angiojet group and CDT group.
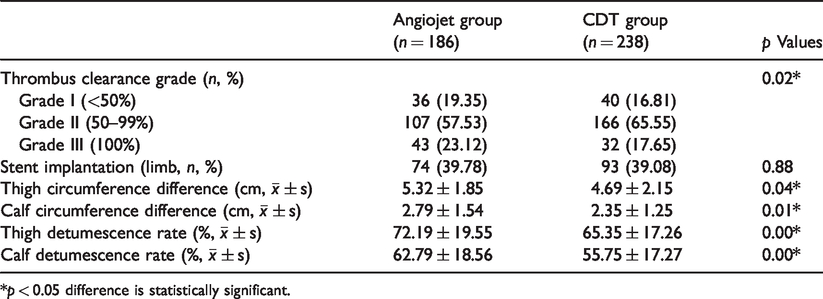
*p < 0.05 difference is statistically significant.
The mean dose of urokinase in AngioJet group was 95.16 ± 45.89 million IU which was significantly less than that in the CDT group 293.76 ± 42.71 million IU (p = 0.00). There was significant difference in the LOS (8.16 ± 3.89 days vs. 12.56 ± 1.58 days; p = 0.01), IVCF retention time (7.69 ± 1.16 days vs. 10.24 ± 2.23 days; p = 0.00) between the two groups. Neither during nor after the procedure was serious adverse event observed. The overall bleeding complication rate was 9.91% (19 patients in AngioJet group and 23 patients in CDT group), which included three major (0.71%, 3/424) and 39 minor (9.2%, 39/424) events. During the treatment period, 15 patients (3.54%, 15/424) in the AngioJet group and 24 patients(5.66%, 24/424) in the CDT group experienced minor bleeding at the catheter insertion site, which was controlled in all of the cases by simple elevation of the limb and application of a compressive bandage and did not require further treatment. Major bleeding event involved gastrointestinal bleeding secondary to gastritis (one patient in the AngioJet group) and cerebral hemorrhage (two patients in the CDTgroup), and patients recovered well after aggressive treatment. All bleeding events were determined to be related to catheter access, anticoagulation, or thrombolytic drug; none was related to the AngioJet procedure. None of the patients suffered from symptomatic pulmonary embolism, death, or other procedure-related complications (Table 3).
Postoperative correlation indexes of Angiojet group and CDT group were compared.
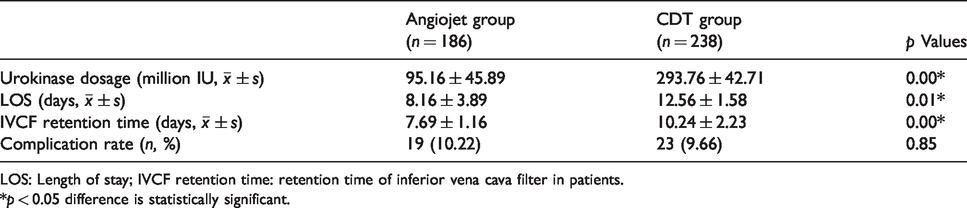
LOS: Length of stay; IVCF retention time: retention time of inferior vena cava filter in patients.
*p < 0.05 difference is statistically significant.
In the AngioJet group, serum creatinine (sCr) and urine erythrocyte from the hemolysis caused by the mechanical process were higher than baseline data at admission (p = 0.00, p = 0.00). The postoperative red blood cell and hemoglobin in two groups were lower than baseline data (p = 0.00, p = 0.00). There was no statistical difference in serum potassium and blood urea nitrogen in either group (Table 4).
Comparison of laboratory standards between admission and 48-h post-treatment Angiojet group.
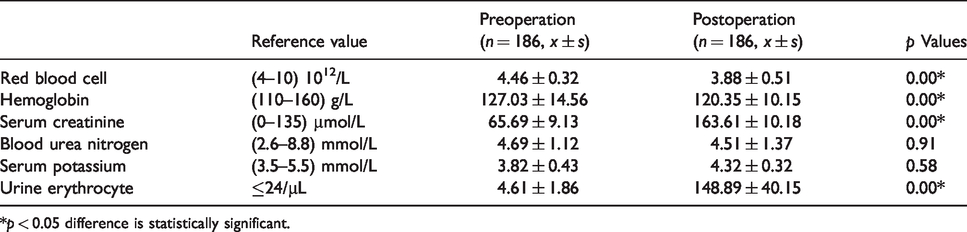
*p < 0.05 difference is statistically significant.
A total of 418 (98.58%, 418/424, three patients in both groups, respectively) patients were followed up for a median of 19 months (range, 1–49 months). Ten patients (5.46%, 10/183) developed PTS (Villalta score >5), including three patients with mild PTS and seven patients with moderate PTS in AngioJet group. In comparison, 31 patients (15.2%, 31/204) developed PTS. Of these patients, 11 patients with mild PTS and 16 patients with moderate PTS in the CDT group. Moreover, there were four patients with severe PTS (Villalta score > 15 or venous ulcer) in the present study during the follow-up. The estimated incidences of PTS were 3.6% vs. 17.1% and 19.8% vs. 60% at two and four years in both groups (Figure 2).
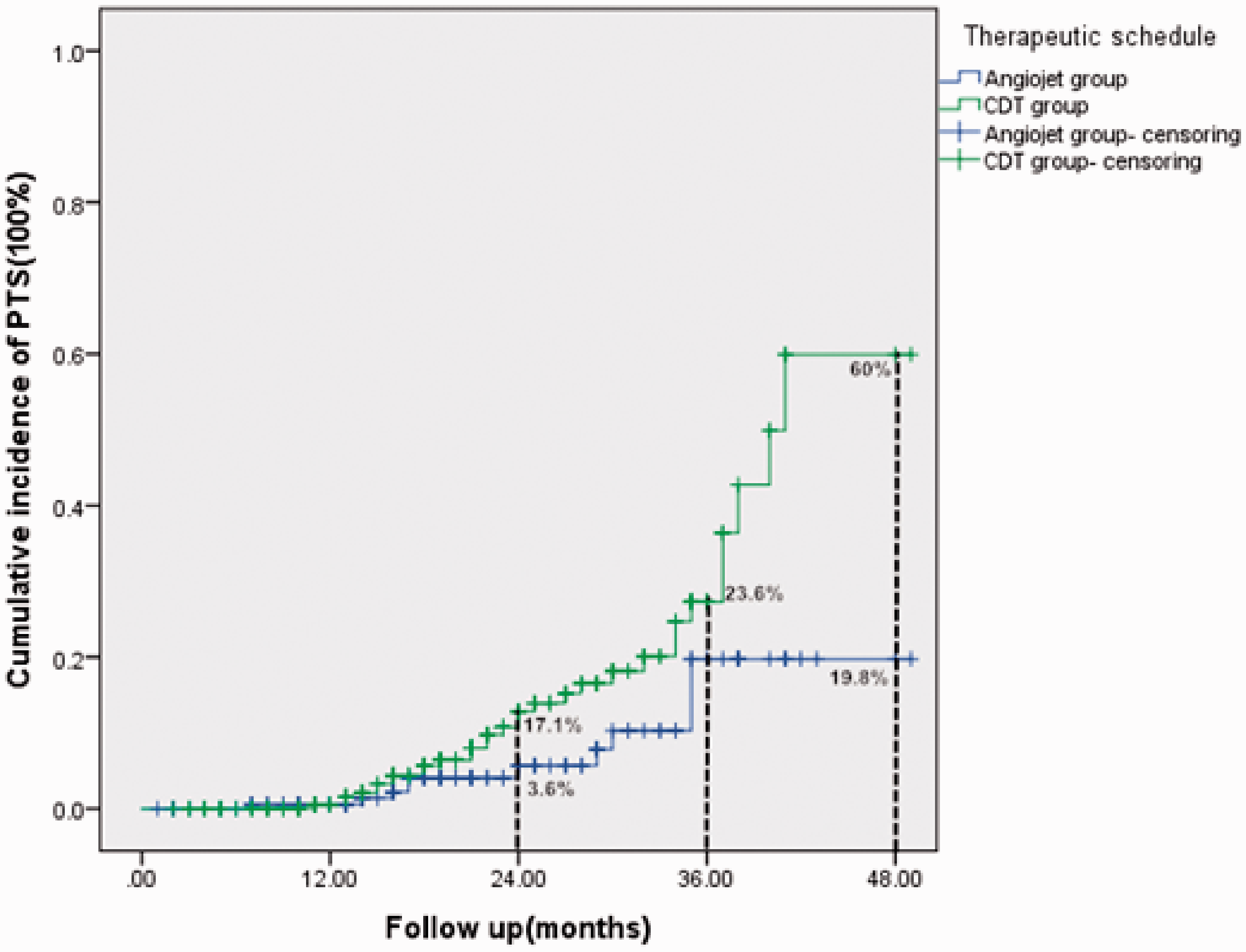
Kaplan–Meier graph of cumulative incidence of PTS in the both groups.
Discussion
The optimal therapy goal of acute lower extremity DVT would prevent complications of venous thrombosis (PE and PTS), improve quality of life and lead to an improvement in symptoms with pain reduction rapidly. Compared with the CDT group, significant differences were observed in the AngioJet group with respect to the thigh circumference difference, calf circumference difference, thigh swelling rate and calf swelling rate. The mean dose of urokinase in AngioJet group was significantly less than that in the CDT group. AngioJet thrombectomy have been shown to be more effective in accelerating thrombolysis, reducing the amount of thrombolytic agent, and shortening hospital stay. The main reason for this difference may be that AngioJet thrombectomy was clearly able to immediately open the passage. However, the expenditure of therapy was often unacceptably high in China. In our study, it was found that the efficacy of AngioJet thrombectomy combinating CDT was significantly better than AngioJet use alone. The addition of CDT can improve the efficacy and result in shorter procedure times and satisfactory patient outcomes. From the imaging perspective, the walls and valves of the veins after thrombolysis were smoother than before the procedures. 15
In this study, sCr concentration which can reflect acute kidney injury (AKI) (AKI was defined as an absolute increase in sCr concentration of ≥26.4 mmol/L [0.3 mg/dL] or increase ≥50% from baseline within 48 h after operation) caused by the mechanical process was higher than baseline data at admission. Acute overwhelming intravascular hemolysis has been proved to cause tubular necrosis resulting from heme proteins and hemosiderin deposition (Figure 3). Given the inevitable gross hemoglobin in patients treated with AngioJet thrombectomy, we postulated that acute hemolysis caused might be the underlying reason for increased postoperative hemoglobinuria in the AngioJet group, which can increase the risk of AKI. For the prevention of Angiojet-related hemoglobinuria, it was some experience: (1) the thrombus is aspirated from the distal end to the proximal end, which can effectively reduce the absorption of hemolytic related substances; (2) there was limitation of aspiration volumes and time; and (3) a large amount of hydration is needed in the perioperative period. The infusion volume per hour is 1.0–1.5 ml/kg from preoperative 0.5 h–1 h to postoperative 6–12 h. Sodium bicarbonate alkalized urine makes the pH value > 6.5. (4) Every surgeon should keep renal protective measures in mind, including hydration, use of sodium bicarbonate, limitation of aspiration volumes and time, and postoperative vigilance.

The changes of hemoglobinuria at 24 h after AngioJet thrombectomy.
Iliac vein differing from other distal vein has to pass the entire volume of venous blood of the lower extremity; therefore, the IVCS typically leads to more pronounced venous hypertension. Stenosis caused by IVCS,if it was failed to be treated immediately,leading to the recanalization rate of the limb deep vein decreases while the incidence of PTS increases. In the treatment of IVCS, balloon angioplasty is inadequate for treating the venous system, and therefore stent placement is frequently required. 16 Current evidence has shown that stent placement after AngioJet thrombectomy or CDT in individuals with acute lower extremity DVT accompanied with IVCS is safe, efficacious, and durable.17,18 Therefore, we performed PTA and stent implantation after thrombus removal at the occlusion and stenosis area of outflow. The prevalence of PTS in the present study was 5.46% in Angiojet group, which was significantly lower than that 15.2% in CDT group. The results of the present study support the use of AngioJet thrombectomy in patients with symptomatic acute lower extremity DVT. However, it remains a major debate that treating acute lower extremity DVT patients accompanied with IVCS involves a decision as to when a stent should be released: immediately after thrombectomy or after thrombolysis.
Several limitations have to be noticed. First, the included study was a retrospective analysis, which was prone to bias resulting from confounding by indication. Prospective studies were possible owing to the high incidence of the disease. Second, venous insufficiency and PTS were associated with follow-up time, so longer follow-up was necessary. Despite inclusion and exclusion criteria, case mixing is inherent in observational studies and may affect the generality of current results. Finally, protein C and protein S deficiency are risk factors for acute lower extremity DVT, which were not detected in this study.
Conclusion
Compared with CDT, AngioJet thrombectomy has stronger clearance ability for acute lower extremity DVT leading to significant reduction in the consumption of hospital resources, total dose of thrombolytic agents, and infusion time, thereby preventing adverse bleeding events, but patients with renal insufficiency should be careful. Ideal short-term and medium-term efficacy and safety are certain.
Footnotes
Authors’ contribution
YX and XW contributed equally to this work.
Acknowledgements
The authors are grateful to all the participants for their involvement in the study. The authors also like to thank the Shengli Oilfield Central Hospital and Union Hospital, Tongji Medical College, Huazhong University of Science and Technology for helping them with data collection.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the Medical and Health Science and Technology Development Plan of Shandong Province, China (grant no. 2017WS688).