
Abstract
Objectives
The aim of this study was to investigate and compare the severity of kidney damage following lower limb ischemia–reperfusion and direct kidney ischemia–reperfusion.
Methods
Thirty Sprague Dawley male rats were randomly divided into three groups; lower extremity ischemia–reperfusion group (Group 2), renal ischemia–reperfusion group (Group 3) and control (anesthesia and median laparotomy only) (Group 1). In group 3, 1-h ischemia was performed on the kidney and in group 2, 1-h ischemia was performed on the left lower extremity. This procedure was followed by reperfusion for 24 h. Renal tissues were removed after the reperfusion period and the groups were evaluated for glutathioneperoxidase activity, malondialdehyde and GSH levels, and furthermore, their histolopathological scores were calculated.
Results
Renal malondialdehyde levels were significantly higher in Group 2 and Group 3 than they were in the Control group. There was no significant difference in renal malondialdehyde levels between Group 2 and Group 3. Kidney glutathione (GSH) levels were statistically lower in Group 2 and Group 3 than in the Control group. No statistically significant difference was found between Group 2 and Group 3 regarding their GSH levels. In histological evaluation, there was no statistically significant difference between Group 2 and Group 3 in terms of kidney damage score.
Conclusions
This study has identified that lower extremity ischemia induces remote kidney damage with similar features to kidney injury, occurring after direct kidney ischemia–reperfusion.
Introduction
Tissue injury after ischemia reperfusion (IR) is still a widely studied subject. 1 The mechanism and the course of injury underlying the IR injury are complex, involving multiple factors and many cell types, and can vary depending on the tissues and organs affected, as well as the duration of tissue ischemia. As a rule, reperfusion of acutely ischemic tissues triggers a potent release of oxygen-free radicals and cytokines, which stimulate an innate immune response with subsequent leukocyte recruitment, endothelial dysfunction, and tissue damage.2,3
In relation to this, there are many experimental studies about IR.2,4 There are two methods generally used in experimental IR studies: in the first application, IR is created in a specific organ and the reperfusion injury is observed in the same organ.4–6 In the second application, following the lower extremity IR, reperfusion injury in the remote organ is examined.2,7–9 For example, reperfusion injury in the kidney tissue can be examined by both tracking the lower extremity IR, and the specific kidney IR.2,5,10 However, there is no study investigating whether there is more damage in the kidney tissue with the lower extremity (remote organ) IR, or in the specific IR of the kidney. If the kidney can be shown to have as much kidney damage with lower extremity IR as the specific kidney IR, especially in vascular operations including limb reperfusion, knowing that the kidney is affected at the same rate as the relevant extremity will not only change our treatment strategies, but also help us to develop new treatment modalities. This concept constitutes the main goal of our study.
In most of the studies, direct and indirect IR injury can be detected in tissues using direct microscopic evaluation with hematoxylin eosin (H&E) and Masson’s trichrome staining. These techniques show tubular atrophy, tubular dilatation, brush border loss, hyaline casts and interstitial bleeding in kidney. In this study, we also used terminal deoxynucleotidyl transferase-mediated dUTP-biotin nick end labeling technique (TUNEL) to demonstrate apoptotic cells in the kidney tissue which will also contribute the evaluation of tissue damage. IR injury can also be detected as a reply to accumulation of free oxygen radicals. So, the changes can be seen in the cellular enzymatic and non-enzymatic antioxidant systems, such as glutathione (GSH), vitamins, superoxide dismutase, catalase and glutathione peroxidase (GPx). As a response to accumulation of free oxygen radicals which also yields an increase in fatty acid reactions and this process causes the release of toxic aldehyde metabolites, such as malondialdehyde (MDA). Histopathological examination was performed by using GSH, GPx activity and MDA to demonstrate tissue damage.11,12
Therefore, in this study, two injury types are investigated: one originating from a remote organ, lower extremity, and one created inside the examined organ, kidney. Histological (microscopic tissue damage indicators)/biochemical comparisons (MDA, GSH, GPx activity) were made to determine the severity of the injuries.
Method
Animals
Thirty randomly selected Sprague Dawley male rats weighing 400–520 g were used in our study. All animals were housed individually in cages and kept on a 12-h light/dark cycle with unlimited access to food (Standard rodent chow) and fresh water. The study was approved by the DokuzEylül University Animal Experiments Local Ethics Committee under the protocol number: 25/2016.
Study protocol
Intravenous catheters were introduced through the tail veins of all the rats. Intramuscular ketamine at a dose of 50 mg/kg, and intramuscular xylazine at a dose of 5 mg/kg were administered as part of the anesthesia protocol to all the rats; 100 IU heparin/kg heparinization was applied to all groups to provide standardization. Intramuscular xylazine was administered at a dose of 2.5 mg/kg to all postoperative rats as an analgesic. As an infection prophylaxis, all the rats received antibiotherapy with cefazolin at a dose of 50 mg/kg. In order to provide better exposure during the surgery, the subjects were shaved and the surgical area was disinfected with povidone iodine.
The rats were randomly divided into three groups. In the first group (Group 1-Control), a median midline laparotomy and kidney exploration was performed in order to obtain standardization after the anesthesia described above. To minimize heat and fluid loss from the peritoneal cavity, during the 1-h waiting period, abdominal incision was temporarily covered with wet warm gauze. The abdomen was closed. After 24 h, the rats were sacrificed with 150 mg/kg Pentothal and the kidney tissues were removed.
In the second group (Group 2-Lower limb IR), following the anesthesia protocol, the left femoral regions were squeezed with a tourniquet after heparinization for 1 h as described by Gokalp et al. 7 The Sonic Doppler examination confirmed the cessation of blood flow. In order to achieve standardization with other groups, the laparotomy and kidney exploration procedure was applied to this group as well during lower extremity ischemia. Incision was closed after reperfusion in the lower extremity. After 24 h, all the rats were sacrificed following the administration of 150 mg/kg pentothal and kidney tissues were removed.
In the third group (Group 3-kidney IR), the kidney ischemia was produced by clamping the left renal artery in the proximal part for 1 h using the method described by Li et al.; 5 24 h later, the subjects were sacrificed and the kidneys were harvested.
All interventions mentioned above were performed by the same pair of surgeons. There was no animal loss in the groups.
Homogenization
After all the rats were sacrificed and kidney tissues were removed, the samples were cleaned with saline solution and weighed. Kidney tissues were homogenized with phosphate buffer (PBS, pH 7.4) with the ultrasonic homogenizer (BandelinSonopuls, Germany). Homogenates were stored at −80°C for measuring glutathione peroxidase (GPx) activity, MDA and GSH levels.
Determination of MDA levels
MDA values were measured by the spectrophotometric (T80, PG instruments, UK) method using the Bioxytech MDA-586 kit (Oxis International, USA). The method of the kit is based on the reaction of MDA with a chromogenic reagent at 45°C. MDA values were determined from the standard curve by measuring the absorbance at 586 nm. Results were expressed as µM.
Determination of GSH levels
GSH levels were measured with the Bioxytech GSH-420 kit (Oxis International, USA). The method of the kit is based on the formation of chromophoric thione. The oxidizing glutathione is converted into a reduced form by adding reducing agent to the buffer-mixed supernatant. Chromophoric thione was formed by adding chromogen and increasing the pH value. GSH concentration was determined by measuring the absorbance at 420 nm. Results were expressed as µM/mg protein.
Detection of GPx activities
The GPx activity was determined by the Bioxytech GPx-340 kit (Oxis International, USA). GPx catalyzes the oxidation of glutathione (GSH) with cumene hydroperoxide. In the presence of glutathione reductase (GR) and NADPH, the oxidized glutathione (GSSG) was converted into a reduced form (GSH), while NADPH was converted into NADP by oxidation. GPx activities were determined by measuring the decrease in absorbance at 340 nm using a spectrophotometer. Results were expressed in mU/mL.
Histological analysis
Kidney tissues were fixed in 10% buffered formalin. Tissues were processed by routine histological methods and embedded in paraffin blocks. Serial sections of 5 µm thickness were taken from the paraffin blocks with the microtome (Thermo Finesse M +) and then, these sections were stained with H&E and Masson’s trichrome staining. The slides were examined under a light microscope to score the tissue damage. Kidney damage was evaluated by tubular atrophy, tubular dilatation, brush border loss, hyaline casts and interstitial bleeding. The slides were analyzed semi-quantitatively and graded as follows: no damage (0, −), mild damage (1, +), moderate damage (2, ++) and severe damage (3, +++). 10
Paraffin sections were stained with in situ cell death detection kit (Roche, Germany) according to the kit protocol using the TUNEL (terminal deoxynucleotidyl transferase mediated dUTP-biotin nick end labeling) technique to demonstrate apoptotic cells in the tissue. Briefly, the sections were deparaffinized and deproteinized by proteinase K (20 µg/ml) for 15 min at room temperature. The sections were then rinsed and incubated in the TUNEL reaction mixture for 1 h at 37°C, rinsed again and visualized using diaminobenzidine (DAB) as substrate. The sections were counter-stained with Mayer’s hematoxylin. TUNEL-positive cells were evaluated by an image analysis system (CellSens Entry 1.7, Olympus) consisting of a microscope (Olympus CX-41) and a video camera (Olympus DP25). In each section, apoptotic cell count was performed in 10 different areas and a % rate was determined.
Statistical evaluation
All data were shown as mean ± SEM. The differences between the averages of the groups were evaluated in SPSS 22 program by using one-way ANOVA post hoc LSD test. P< 0.05 was based on significance level.
Results
MDA levels
The mean MDA levels of all groups are presented in Figure 1. MDA levels of renal IR and limb IR groups were significantly higher than the Control group (P < 0.001 and P = 0.002, respectively). There was no significant difference in MDA levels between renal IR and limb IR groups (P > 0.05).

MDA levels in rat kidneys. Data are means ± SEM. *P < 0.05 compared to the Control group.
GSH levels
The mean GSH levels of all groups are shown in Figure 2. GSH levels of renal IR and limb IR groups were significantly decreased compared with the Control group (P = 0.024 and P = 0.009, respectively). There was no statistical difference in GSH levels between renal IR and limb IR groups (P > 0.05).
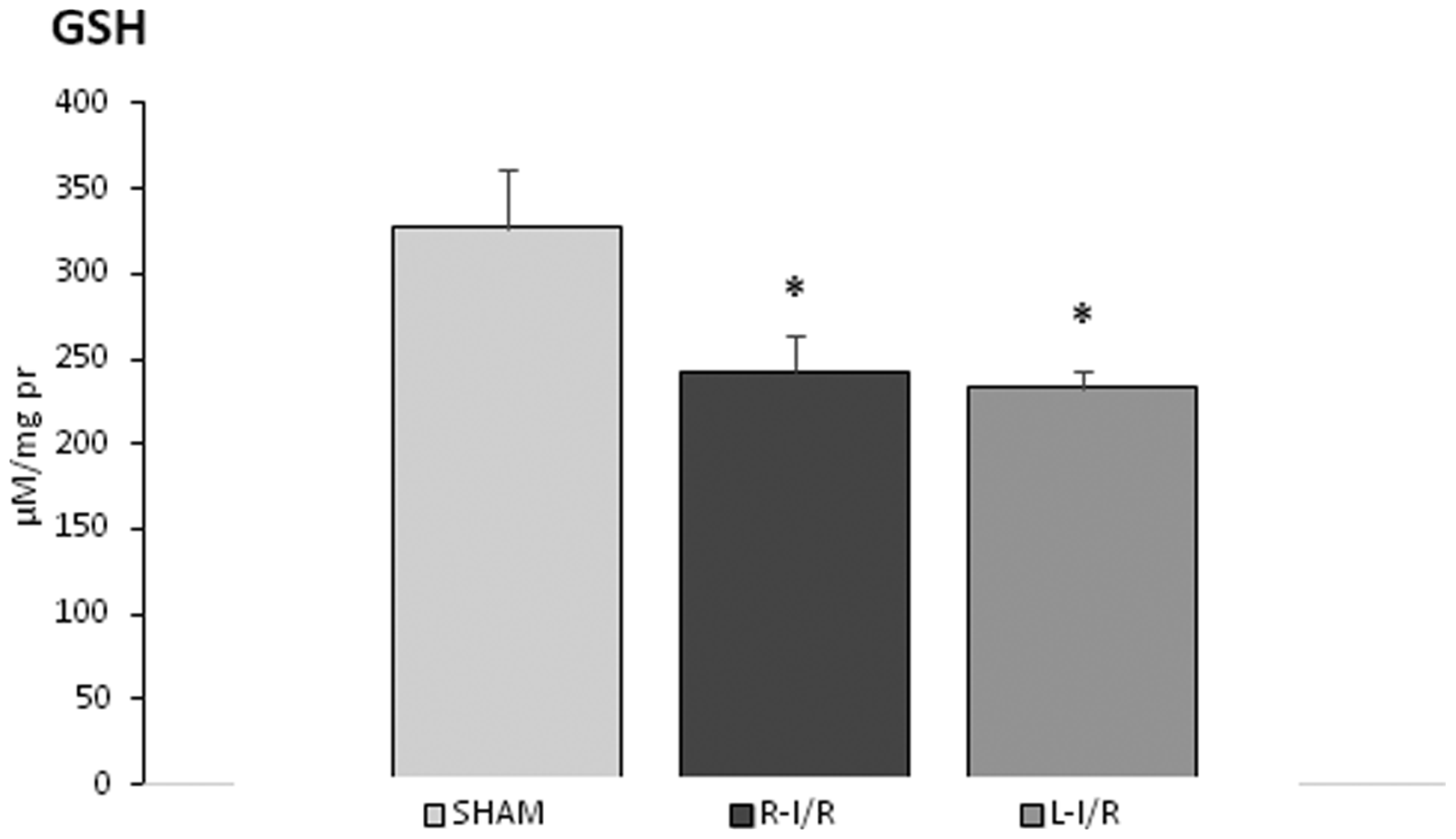
GSH levels in rat kidneys. Data are means ± SEM. *P < 0.05 compared to Control group.
GPx activity
The mean GPx values of all groups are presented in Figure 3. GPx values were significantly lower in renal IR group compared to the Control group (P = 0.027). In the limb IR group, GPx values were lower than the Control group, although it was not significant (P > 0.05). There was also no significant difference between renal IR and limb IR groups (P > 0.05).

GPx activities in rat kidneys. Data are means ± SEM. *P < 0.05 compared to Control group.
Histological analysis
Kidney sections stained with H&E are shown in Figure 4(a). Impaired renal histology was found in IR groups, while the histological appearance was normal in the Control group (Figure 4(aI)). In the limb IR group, tubular atrophy, loss of brush border, detachment of basement membrane from glomeruli, accumulation of hyaline casts in some areas were observed (Figure 4(aII)). In the renal IR group, hyaline cast accumulation, tubular atrophy and hemorrhagic areas were observed more commonly (Figure 4(aIII)). In the sections stained with Masson’s trichrome, increased interstitial collagen was observed in IR groups (Figure 4 (bII) and (III), while there was no interstitial fibrosis in the Control group (Figure 4(bI)). Renal damage score was significantly higher in renal IR and limb IR groups compared to the Control group (Figure 5, P < 0.001). There was no significant difference between renal IR and limb IR groups (P > 0.05).
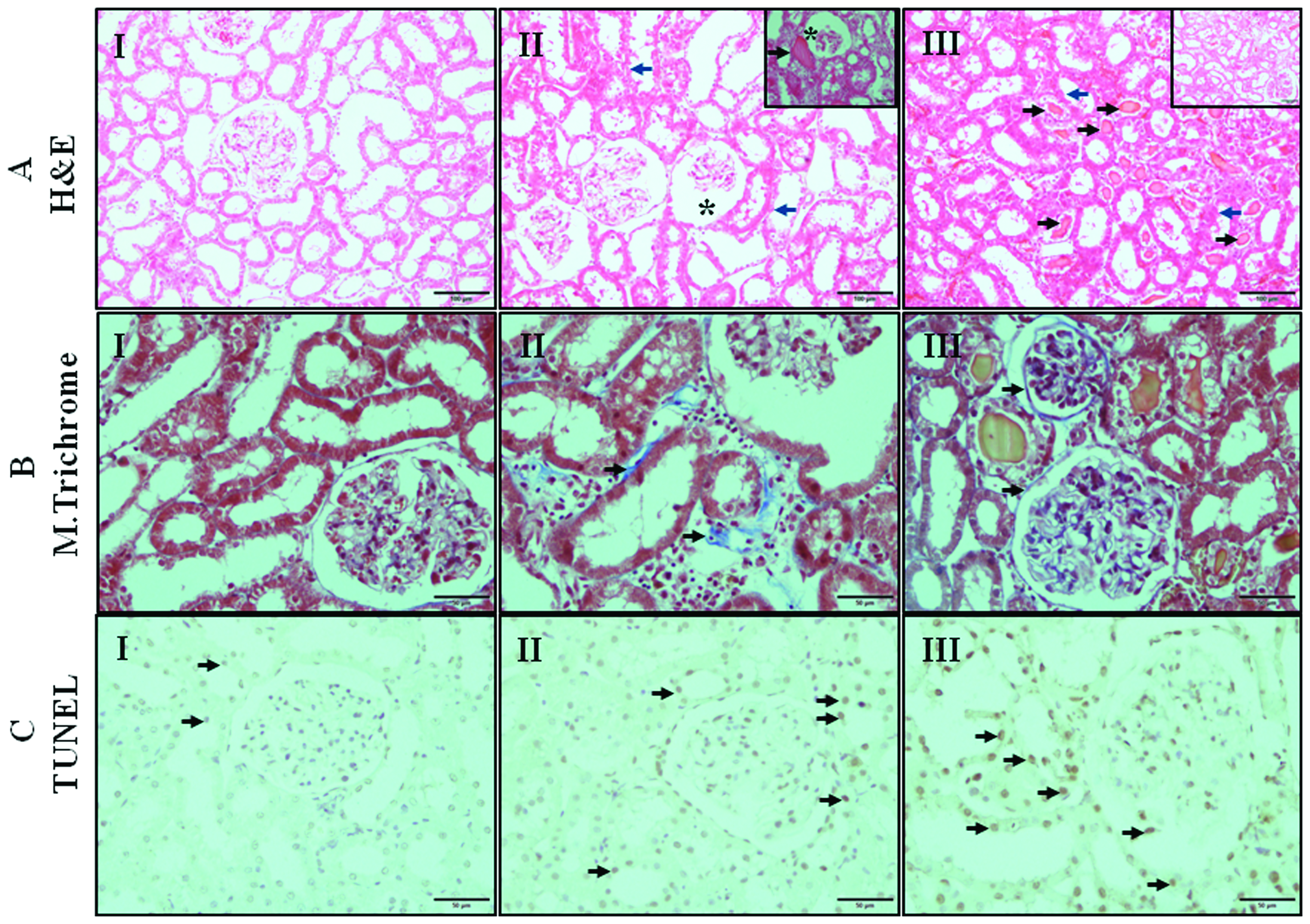
Light microscopic images of rat kidney sections. I; Control, II; Limb I/R, III; Renal I/R group. Upper (a): Hematoxylin&Eosin (H&E) stained sections. The morphology of kidney in the Control group was normal. In Limb I/R group, tubular atrophy, loss of brush border (blue arrows), detachment of basement membrane from glomeruli (stars), tubular hyaline casts (black arrow, inset). In Renal I/R group, tubular atrophy, loss of brush border (blue arrows), tubular hyaline casts (black arrows) and hemorrhagic areas (inset) can be seen. Middle (b): Masson’s trichrome stained sections. Collagen deposits (arrows). Lower (c): TUNEL staining. Representative photomicrographs of TUNEL-positive cells (arrows).

Kidney damage score. Data are means ± SEM. *P < 0.001 compared to Control group.
The kidney images of TUNEL staining are presented in Figure 4(c). There were more TUNEL-positive cells in IR groups compared to the Control group. TUNEL-positive cell ratio was significantly higher in renal and limb IR groups than in the Control group (Figure 6, P < 0.001). In renal IR group, the apoptosis rate was significantly higher than in limb IR group (P = 0.031).
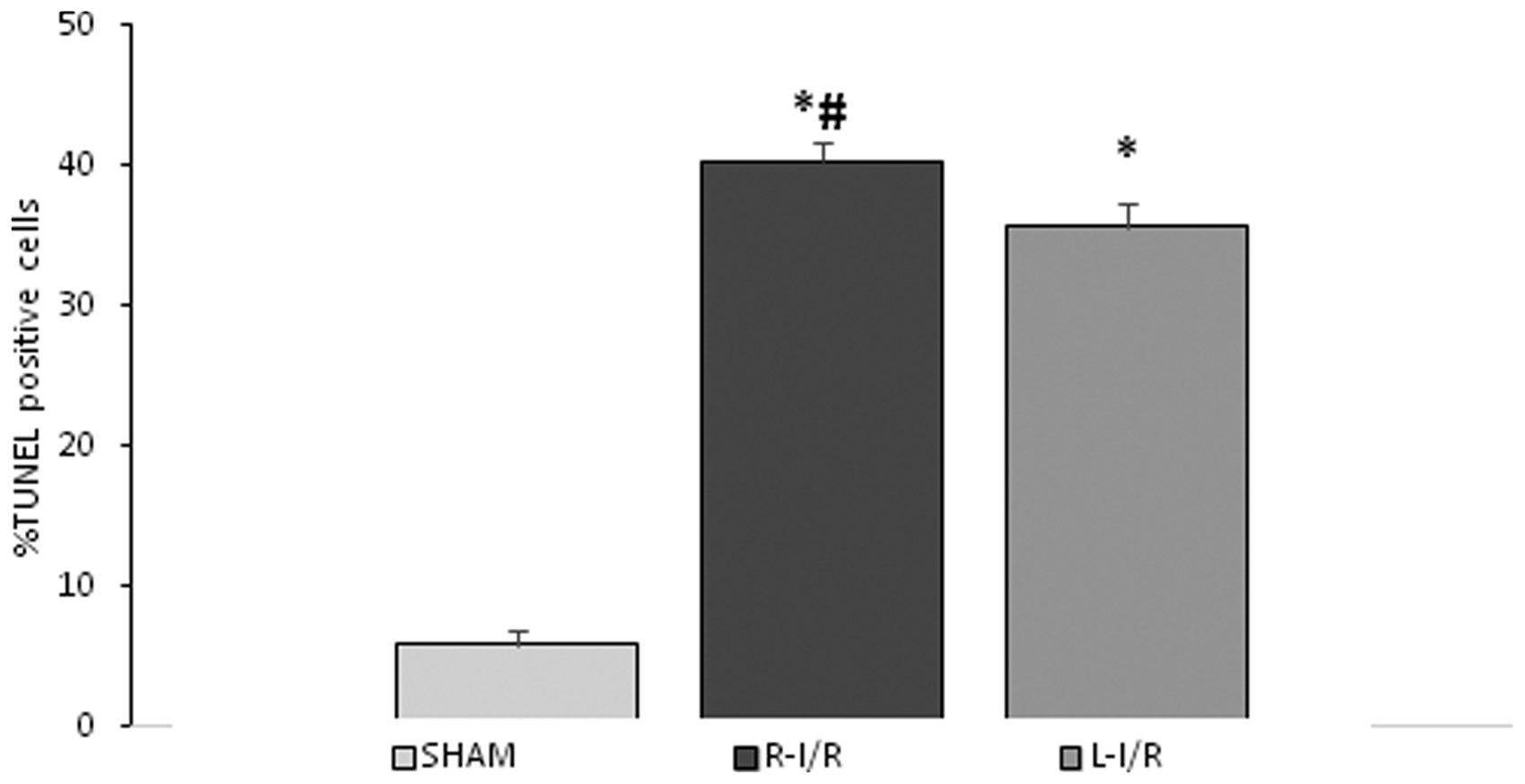
The percentage of TUNEL-positive cells of rat kidneys. Data are means ± SEM. *P < 0.001 compared to Control group. #P < 0.05 compared to Limb I/R group.
According to these histological findings, we concluded renal and limb IR injuries yielded similar renal damage scores for kidneys. Although the number of TUNEL-positive cells is statistically higher in the kidney IR group than in the limb IR group, these results indicate a similar risk for IR injury in both groups and the impact on kidneys by limb IR is not less than the direct kidney IR injury.
Discussion
Acute lower extremity ischemia and subsequent reperfusion is a frequent occurrence in common medical practice. Especially, vascular injuries, which require the tourniquet of the lower extremity, acute lower extremity arterial occlusions, aortic surgery, and peripheral arterial surgery often contains some degree of ischemia and reperfusion. 13
Reperfusion injury in the originating tissue as a response to IR is a relatively clear mechanism. 14 However, it is more interesting to encounter the reperfusion injury in kidney as a remote organ following IR of the lower extremity.
Pathophysiological pathways of reperfusion injury in kidney tissue can easily be explained by several mechanisms. The most common mechanisms are the release of free oxygen radicals and inflammation after reperfusion in that specific tissue. IR injury can lead to the production of large amounts of reactive oxygen species (ROS) in tubular epithelial cells (TECs), thus triggering mitochondrial damage and lipid peroxidation and causing devastating cell damage. The inflammatory factors produced by TECs cause a large number of inflammatory cells to migrate and infiltrate, further aggravating renal damage, and subsequently, inflammation amplification.15–17 However, the mechanism of reperfusion injury occurring in the kidneys after an IR event in the lower extremity is also associated with this mechanism. This is related to neutrophils, macrophages, pro-inflammatory cytokines and chemokines that are released from ischemic residual tissues after IR in the lower extremity.2,18,19 Spillage and amplification of these inflammatory responses systemically and often lead to a complex cytokine cascade or a storm that serves to perpetuate inflammatory reactions in remote organs, which may clinically manifest as multiple organ dysfunction (e.g. acute kidney injury and acute lung injury) and possibly death.2,3,20 There are several different settings to investigate IR in the literature; Dong et al. investigated tubular biomarkers after ischemia reperfusion injury of the kidney itself, and they used short- and long-term durations of ischemia(20 min-30 min-45 min ischemia followed by 1 day-3 day-7 day and 28-day reperfusion).They found that the effects of ischemia reperfusion injury deepen as the duration of ischemia increases, and visible effects of significant injury are present following even a 20-min ischemic period. 14 We were able to demonstrate significant reperfusion injury in kidneys following a 60-min ischemia of both the kidney itself and the lower extremity. Similar findings suggested the duration of ischemic period and reperfusion period in our study could create demonstrable injury in kidneys. There are also numerous studies investigating the protective effects of drugs on kidneys in rats following lower limb ischemia reperfusion, or following the ischemia reperfusion of the kidney itself; 6 , 21 Erbatur et al. 21 investigated the protective effects of dexmedetomidine on kidneys following lower limb ischemia and they illustrated the renoprotective effects of the drug. In another study Iscan et al. assessed the effects of Cilostazol and Rosuvastatin on kidney ischemia reperfusion and remote cardiac reperfusion injury. In their study, they reported the protective effects of the drugs on kidneys as well as cardiac muscle as a remote organ. 22
There are studies investigating the idea of reperfusion injury in specific tissues, as well as those investigating the protective effects of drugs following well studied animal IR models, but we have not seen any article in the literature trying to reveal the rate of kidney damage in two different settings: in the first setting, the IR was created in a remote organ, the lower extremity, and the injury in renal tissues was evaluated. In the second setting, the IR was created within the renal tissue and the injury was evaluated in the same tissue. The results of the two groups were compared in order to understand which of these two methods caused more reperfusion injury in the kidney using MDA, GSH, GPx activity and Tunel technique to demonstrate apoptotic cells in the tissue. First of all, we detected reperfusion injury in the kidney in both settings. But the most interesting finding was that the kidney reperfusion injury caused by these two methods yielded similar degrees of renal injury. These results were achieved by comparing MDA and GSH levels, and by our direct microscopic examination of the tissues compared. As a result, a severe reperfusion injury occurred in the kidneys following the IR of the lower extremity and this injury showed a number of similar key features as the IR injury of the kidney itself. In the light of these findings, it should be taken into consideration that the kidneys can be very susceptible to ischemic conditions originating from a remote source like a lower extremity IR. Overall, we believe this study strengthens the idea that the IR of remote organs may play an important role in remote renal injury, and thus necessary medical and operational measures should be taken in such cases.
The present study has limitations as not all the inflammatory processes responsible for tissue damage have been discussed, since this would be vast, but it can be considered for prospective controlled clinical studies in which biochemical inflammatory processes are examined in the future. Moreover, human trials should also be considered and planned to further investigate the effects of remote organ ischemia–reperfusion.
In conclusion, this study has identified lower extremity ischemia induced remote kidney damage, and it showed nearly similar features to the kidney injury occurring after direct kidney IR. The result of this study has gone some way towards enhancing our understanding that remote organs may be affected as well, following the IR of another organ and the surgeons must consider this remote IR risk during aortic and peripheric surgical procedures. The precise mechanism of remote kidney injury remains to be elucidated by further studies, which include different indicators for kidney injury. Thus, future experiments, using a broader range than the design of this study could shed more light on remote kidney injury and its underlying mechanisms.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study has been funded by Katip Celebi University, Medical School, Scientific Research Fund.