
Abstract
Introduction
Chronic liver disease is a public health burden worldwide. Portal hypertension is a major portosystemic abnormality in chronic liver disease. This study aimed to determine the main, right, and the left portal vein diameter in patients with chronic liver disease.
Materials and methods
A cross-sectional study was carried out at the Abubakar Tafawa Balewa University Teaching Hospital, Bauchi, northeastern Nigeria from December 2018 to September 2019. Ethical clearance was obtained from the institutional review board. A total of 200 subjects were recruited comprising 100 patients with chronic liver disease and 100 age-matched controls, aged 18 years and above. A transabdominal ultrasound scan was carried out measuring the main, right, and left portal vein diameter while lying supine and/or in the right anterior oblique position after overnight fasting, or 6 hours before the scan. Data analysis was done using SPSS version 22.0. Descriptive statistics (mean, standard deviation) and Pearson’s correlation were used.
Results
There were 106(53%) males and 94(47%) females, aged between 18 and 73 years with a mean age of 46.79 ± 15.43. The main, right, and left portal vein diameter in patients with chronic liver disease was 14.51 ± 0.78 mm, 6.83 ± 0.81 mm, and 6.26 ± 0.74 mm, which were higher than those of their control. The portal vein diameter positively correlated (weak) with age and respiratory phases among participants (P < 0.05).
Conclusion
This study found the main, right, and left portal vein diameter among patients with chronic liver disease to be larger than those of the controls. Ultrasonography is a reliable diagnostic tool in evaluating portosystemic pathologies.
Introduction
Chronic liver disease (CLD) is a public health burden worldwide, particularly in developing countries where human immunodeficiency virus (HIV), hepatitis B virus (HBV), and hepatitis C virus (HCV) are endemic. 1 2 CLD has a range of etiologies with HBV, HCV, and HIV, hepatotoxic drug ingestion, alcohol consumption, nonalcoholic fatty liver disease (NAFLD), autoimmune disease, and cryptogenic hepatopathy being encountered commonly in daily practice. 3 CLD is a progressive deterioration of liver functions for more than six months, which includes synthesis of clotting factors, other proteins, detoxification of harmful products of metabolism, and excretion of bile.4–6 It is a continuous process of inflammation, destruction, and regeneration of liver parenchyma, which leads to fibrosis and cirrhosis. The spectrum of etiologies is broad and includes toxins, alcohol abuse for a prolonged time, infection, autoimmune diseases, genetic and metabolic disorders. 7 Cirrhosis is the final stage of CLD due to the disruption in liver architecture, widespread nodule formation, vascular reorganization, neo-angiogenesis, and deposition of an extracellular matrix. The underlying mechanism of fibrosis and cirrhosis at a cellular level is the recruitment of stellate cells and fibroblasts, resulting in fibrosis, while parenchymal regeneration relies on hepatic stem cells.6–8
The portal vein is unique. It drains blood from the capillaries of the intestinal wall and spleen to the capillaries of hepatic sinusoids. 9 The portal vein is not a true vein because it does not drain to the heart. Instead, it supplies metabolic substrates to the liver and, to maintain that, ingested substances are first processed by the liver before entering normal circulation (first-pass effect). 10 The length of the portal vein is of surgical importance especially in interventional procedures like liver transplant, transhepatic portal vein embolization, and pancreatectomy. 11
The major abnormality of the portal venous system in CLD is portal hypertension, from increased resistance to portal venous flow as a result of the enlargement of the intra- and extrahepatic portal vein and subsequent development of portosystemic collaterals. 9 Radiological imaging for CLD assessment involves the examination of morphological features on ultrasonography and other cross-sectional imaging systems like computed tomography (CT) and magnetic resonance imaging (MRI). Current imaging techniques like sono-elastography and MR elastography are now widely used in the diagnosis of CLD, while others like MRI diffusion, perfusion, hepatobiliary contrast agents, and CT using dual-energy and perfusion are still being investigated. 3 However, ultrasonography is preferred because it is relatively safe, cheap, noninvasive, and readily accepted by most patients. It provides real-time imaging and Doppler capability, does not have risk associated with ionizing radiation, and is widely available for evaluating those patients presenting with CLD. It is also important in monitoring patient workup and response to therapy. 12 The gold standard in the diagnosis of CLD is liver biopsy. 8 However, its invasive nature, risk of complications and intra- and interobserver variability makes it unacceptable for some patients. Also, it is not practicable to use repeatedly as a method of monitoring and workup of patients. 3 Noninvasive alternative methods are serologic test and radiologic evaluations. The serological test is not reliable as it is plagued by extraneous factors like active hepatitis or Gilbert’s syndrome that result in false positive findings and cannot quantify the level of the disease process. 3
Materials and methods
A cross-sectional study was conducted at the Abubakar Tafawa Balewa University Teaching Hospital (ATBUTH), Bauchi, northeastern Nigeria from December 2018 to September 2019. A total of 200 subjects were recruited comprising 100 CLD patients and 100 apparently healthy age-matched control subjects, aged 18 years and above. Ethical approval was obtained from the ethical committee and the head of the Radiology Department in ATBUTH. Written and informed consent was also obtained from the participants before joining in the study. Participant recruitment was voluntary and from the general outpatient department and medical wards, while aged-matched controls were recruited from the hospital staff and students from the School of Nursing in ATBUTH.
Transabdominal ultrasonography was carried out on all subjects measuring the main, right, and left portal vein diameters while lying supine on a couch. Participants’ height was measured while standing erect against a meter rule with the head in Frankfurts’ plane and their weight was measured to the nearest kilogram using a clinical weighing scale. Body mass index was measured using the Quetelet’s formula: BMI = weight (kg)/height (m2). 13 Data analysis was done using SPSS version 22.0 (IBM, Chicago, Illinois, USA). Descriptive statistics (mean, standard deviation) and Pearson’s correlation were used.
Inclusion and exclusion criteria
Patients diagnosed with CLD referred for an abdominal ultrasound and apparently healthy subjects with normal ultrasound findings of the liver formed the inclusion criteria while critically sick patients, pregnant women, patients on hepatotoxic drugs such as antituberculous and antiretroviral drugs were excluded from this study.
Equipment used
An ALOKA SSD-1000 (IP-1233EV, SN-57324, Japan) ultrasound machine with a 3.5 MHz curvilinear transducer was used. Measurements were performed using the electronic calipers on the ultrasound machine after freezing the image. Anthropometric parameters, like height, weight, and body mass index of each participant, were measured and calculated. A clinical weighing scale (ZT WHO Scale) was used to measure their weight to the nearest kilogram and their height was measured while standing against a meter rule.
Scanning technique
Transabdominal scans were performed with the subjects in the supine and/or in the right anterior oblique position after overnight fasting, or 6 hours before the scan, to reduce excess bowel gas that may obscure the main portal vein and distends the biliary ducts. 9 10 14 Subjects were exposed from the xiphisternum to the pelvic brim, ultrasound gel was applied to the right upper quadrant of the abdomen, and the transducer placed on the epigastrium in both the transverse and longitudinal planes to assess the main, right, and left portal veins. 9 10 The intrahepatic portal veins may be imaged via a subcoastal or intercoastal approach with the patient in supine, right anterior oblique, or left posterior oblique position. 9 15 Gas in the duodenum and antrum may also obscure the distal extrahepatic portal vein. Placing the patients in the right anterior oblique position may help to displace the gas. If bowel gas interference still persisted, the patients were asked to drink water and rest in a right lateral decubitus position for 3–5 minutes. This might displace the gas and also provide an acoustic window for better visualization. 14 16 The main portal vein is seen behind the neck of the pancreas, at the level of L1/L2 vertebrae, and divides at the porta hepatis into the right and left branches. 10 14 The diameter was measured by placing two cursors on the internal walls of the portal vein. 15 Anteroposterior (AP) and transverse diameter of the main portal vein, right portal vein, and left portal vein were measured at their midportions. The AP diameter from proximal to the distal wall was obtained using the longitudinal view, while the transverse diameter from the medial to the lateral wall was obtained from the transverse view. 10 16 A consultant radiologist (sonologist) with over 15 years post qualification training and wealth of experience in clinical sonography practice performed the scan alone, to avoid interobserver error. 11 16 To reduce intraobserver error, the PVD was measured three times and the mean value of the three measurements was recorded as the final value. 16 17 All measurements obtained were recorded on a data capture sheet; the analysis was done using SPSS version 20.0. Descriptive statistics (mean, standard deviation, frequency, and percentages) and paired sample t-test were used to compare the mean values of the PVD in CLD patients and their age-matched control subject. Pearson’s correlation was used to determine the relationship between PVD with age, gender, and respiratory phase of respiration. Statistical significance was considered at P < 0.05.
Results
Of the 100 patients diagnosed with CLD and 100 age-matched control subjects, there were 106 (53%) males and 94 (47%) females. The age range was from 18 to 73 years with a mean age of 35.7 ± 16.4. Participants within the age group of 18–29 years had the highest frequency with 69 (34.5%) and the least were those within the age range 66 years and above with 18 (9%). Participants with normal BMI had the highest frequency with 137 (68.5%) and the least were obese subjects with only eight (4%) among the studied population, as shown in Table 1.
Demographic characteristics of participants.
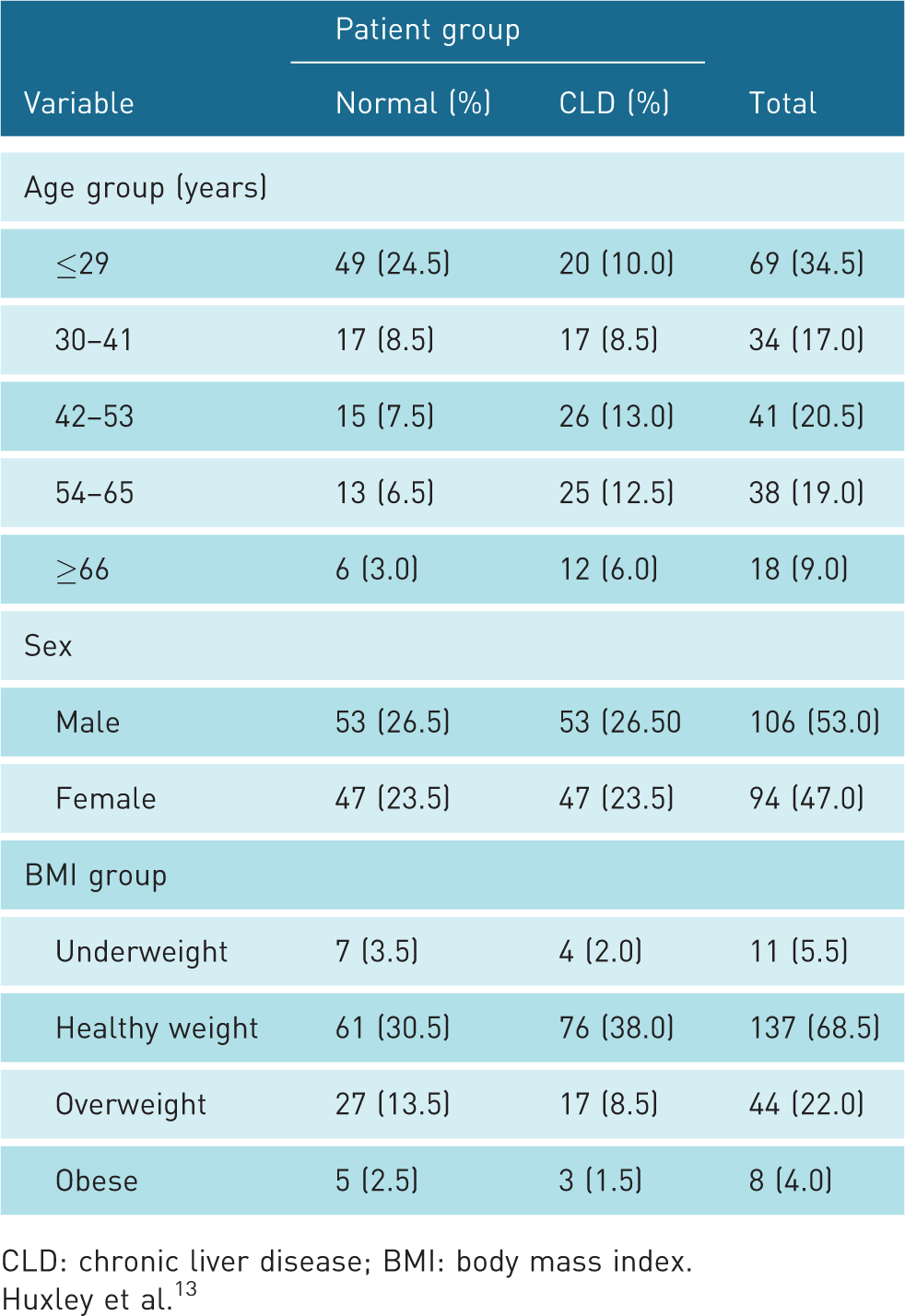
CLD: chronic liver disease; BMI: body mass index.
Huxley et al. 13
The mean values of main, right, and left portal vein diameter in patients with CLD during inspiration and expiration were 16.6 ± 0.76, 6.9 ± 0.89, 6.3 ± 0.81 and 14.3 ± 0.79, 6.7 ± 0.72, 6.1 ± 0.67, respectively, as shown in Table 2.
The main, right, and left portal vein diameter during inspiration and expiration.
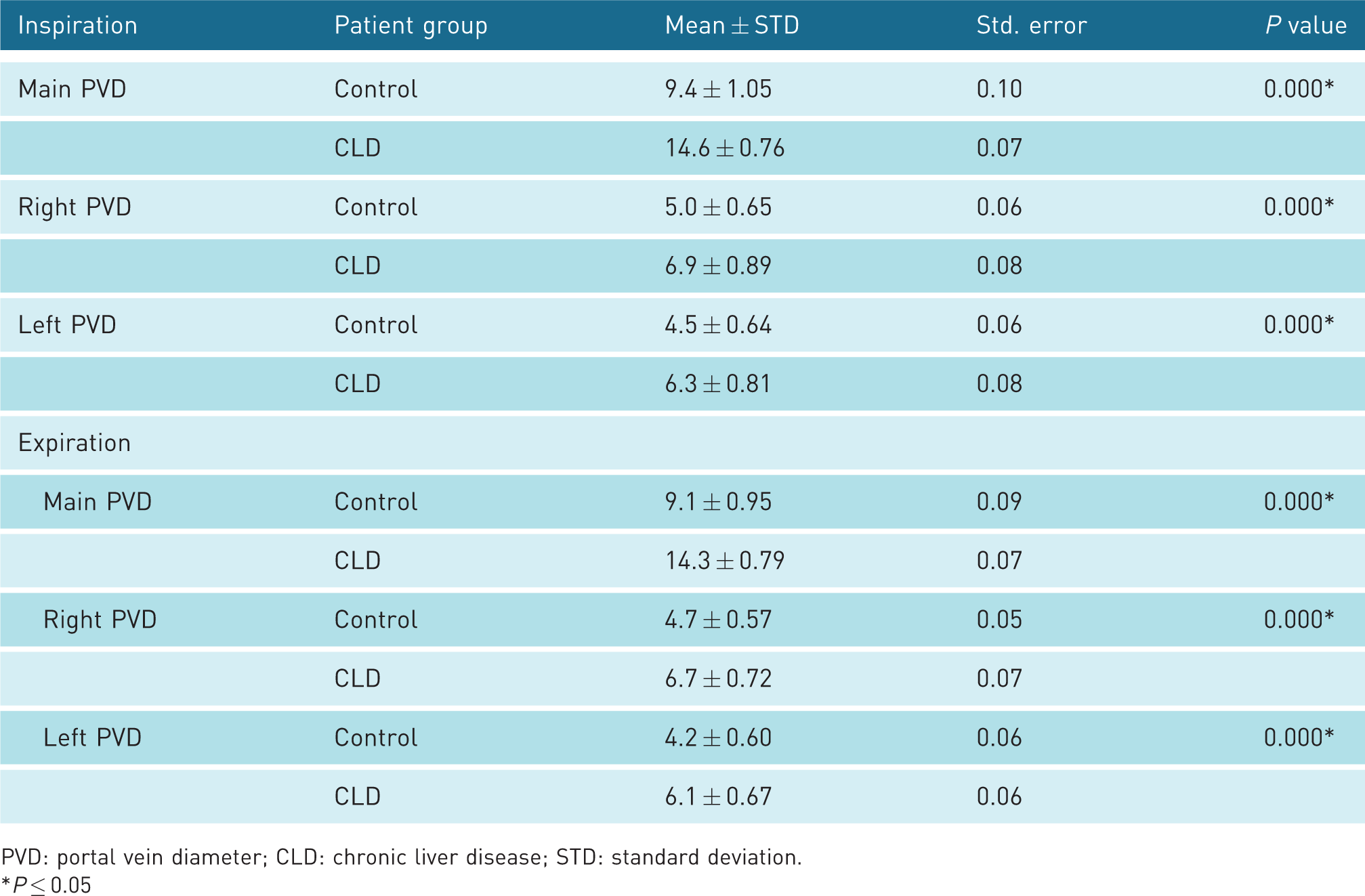
PVD: portal vein diameter; CLD: chronic liver disease; STD: standard deviation.*P ≤ 0.05
Participants of 66 years or older with CLD had the largest PVD with 15.0 ± 0.90, 6.8 ± 0.82, 6.0 ± 0.76 for the main, right, and left portal vein during inspiration and 14.5 ± 0.73, 6.6 ± 0.71, 6.1 ± 0.67 for the main, right, and left portal vein during expiration, as shown in Table 3.
The main, right, and left portal vein diameter during inspiration and expiration based on age.

PVD: portal vein diameter; CLD: chronic liver disease; STD: standard deviation.
The values of the PVD in the male subjects were larger than the female subjects with 14.8 ± 0.76 and 14.4 ± 0.69 during inspiration and, on expiration, the values were 14.3 ± 0.81 and 14.3 ± 0.78 as shown in Table 4.
The main, right, and left portal vein diameter during inspiration and expiration based on sex.

PVD: portal vein diameter; CLD: chronic liver disease; STD: standard deviation; SE: standard error.
Discussion
Ultrasonographic imaging plays a vital role in the assessment of the portal vein diameter, flow rate, and peak velocity which gives an accurate and reliable method of diagnosing conditions of the liver including CLD. The clinical manifestations of several CLDs are the direct consequence of portal hypertension, which is defined as an increase in portal venous pressure above the normal limit of 5–10 mmHg. 18 The severity of portal hypertension increases with the likelihood of development of complications including ruptured varices so early recognition is vital in clinical practice. 18
There were more males than females in this study. Previous studies 4 19 reported similar findings with the dominance of male subjects. This could perhaps be due to the more risky lifestyle of some male subjects like excessive alcohol consumption, cigarette smoking, and use of native herbs and roots, among others.
The portal vein diameter in this study was larger in patients with CLD than their age-matched controls. Previous studies conducted19–24 also reported an increase in the diameter of the portal vein in patients with CLD. Another study 25 opined that patients with a portal vein diameter greater than 12 mm were more predisposed to having portosystemic collaterals. Portal hypertension results in increase in size of the portal vein, splenomegaly, and formation of portosystemic collaterals at different sites. 4 18 Gastroesophageal collaterals arise from the anastomosis between the short gastric and coronary veins and the esophageal, azygos, and intercostal veins; this results in a formation of esophageal and gastric varices. Collaterals develop in areas where anatomic connections exist between the portal and systemic circulations. These vascular channels are normally closed but become dilated as a result of increased intravascular resistance to flow within the portal vein to return blood to systemic circulation. Gastroesophageal varices are responsible for the main complications of portal hypertension and massive upper gastrointestinal bleeding. 18 These findings were also similar to those obtained from CT imaging in another study. 26 This concordance in findings could possibly be a function of the similarities in design, diagnostic tool, expertise, and experiences of the operators, as ultrasonography has been reported as an operator-dependent imaging modality. 8 15
The diameter of the main portal vein in patients with CLD was significantly larger in males than females P ≤ 0.05, however, literature varies in demonstrating the variation in the gender of the portal vein diameter. Previous studies have reported higher values of PVD in males than females. 15 30 This perhaps could be due to the smaller stature of females compared to males, hence their body organs are also of smaller size. 27 28 However, the contrary opinion has been reported 16 29 and other studies have found no difference in diameter. 30 31
The diameter of right and left portal vein in patients with CLD in this study was also larger than those in the control subjects, with the right slightly larger than the left. Previous researchers had similar findings in their studies. 17 31 This perhaps could be due to the fact that the right lobe of the liver accounts for up to 60–65% of the hepatic size.
The diameter of the portal vein was found to increase as patients advanced in age. This is consistent with many previous publications which also report a strong influence of age on PVD. 10 22 30 32 33
The mean diameter of the main, right, and left portal vein was significantly larger during inspiration than expiration in our study (P ≤ 0.05), which is also consistent with the findings of others.16,34–36 The phases of respiration have been reported in several studies to greatly affect the size of portal vein irrespective of sex and patients’ condition. 15 31 36 The increase in the intra-abdominal gradient pressure during respiration has been reported to be the reason for distention (increased diameter) of vessels especially during inspiration and compression of vessels during expiration. 37 This perhaps may explain the reason for the variation in size during inspiration and expiration.
This was a single center study and therefore had a limited sample size. Furthermore, no information on portal vein hemodynamics in patients with CLD and their age-matched controls were available due to a lack of Doppler facility. It is hoped that further studies will address these limitations.
Conclusion
This study found the main, right, and left portal vein diameter among patients with CLD to be larger than those of their age-matched controls. The portal vein diameter correlated with increasing age and showed a significant difference between the two sexes and respiratory phases. Ultrasonography is a noninvasive, cost-effective, and reliable diagnostic tool in the evaluation of portosystemic pathologies owing to its safety, real-time, and dynamic nature.
Footnotes
Acknowledgments
We appreciate all the staff of Radiology department ATBUTH Bauchi for their assistance during the course of data collection.
Contributors
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics approval
Ethical approval was obtained from the research and ethics committee of Abubakar Tafawa Balewa University Teaching Hospital Bauchi.
The reference number is: ATBUTH (REC): 003/2019
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Guarantor
Geofery Luntsi (Corresponding author)