
Abstract
Introduction:
Pulmonary infarction is an ischaemic necrosis resulting from pulmonary arterial occlusion, occurring in approximately one-third of pulmonary thromboembolism cases. While computed tomography angiography remains the gold standard for diagnosis, its use in follow-up is limited by radiation exposure. Thoracic ultrasonography, a bedside, radiation-free and repeatable modality, may serve as an alternative tool for monitoring pulmonary infarction.
Case Report:
We present a 44-year-old woman who developed sudden dyspnoea and back pain 1 week after venous surgery. Computed tomography angiography confirmed pulmonary thromboembolism, and persistent flank pain was attributed to pulmonary infarction. Thoracic ultrasonography revealed a hypoechoic, pleural-based consolidation in the left hemithorax measuring 19 × 11 mm. The patient was treated with anticoagulation and followed weekly with thoracic ultrasonography. Her symptoms improved, and by the sixth week, the consolidation had completely resolved.
Discussion:
Pulmonary infarction has traditionally been associated with poor outcomes in older patients with comorbidities; however, it may also occur in young, otherwise healthy individuals. The clinical significance of pulmonary infarction remains uncertain, although some studies suggest potential associations with delayed recovery and functional impairment. Thoracic ultrasonography demonstrates good sensitivity and specificity in detecting pulmonary infarction and offers several advantages over computed tomography angiography for follow-up, including safety, accessibility and repeatability. Evidence suggests that infarct resolution typically occurs within 6 to 12 weeks, a period during which thoracic ultrasonography may be effectively utilised to monitor lesion regression.
Conclusion:
This case highlights the role of thoracic ultrasonography in the follow-up of pulmonary infarction. Although limited to peripheral, pleura-based lesions, thoracic ultrasonography represents a safe, practical and repeatable imaging modality for monitoring pulmonary infarction resolution and may reduce the need for repeated computed tomography angiography in clinical practice.
Introduction
Ultrasonography (US) platforms, which transmit sound waves to tissues via a probe and generate images from the reflected waves with the aid of a monitor, have been utilised in medicine since the 1940s. As solid organs predominantly reflect the transmitted sound waves, the application of US in lung imaging emerged at a later stage. Today, thoracic US (TUS) is effectively employed not only in diagnostic procedures such as imaging pleural effusions and peripheral lung tumours, as well as evaluating pleuroparenchymal diseases, but also in guiding a wide range of interventional procedures. These include thoracocentesis, pleural biopsy, pleural catheter placement, biopsy of thoracic wall or supraclavicular metastases and biopsy of peripheral pulmonary lesions. 1
Pulmonary infarction (PI) is defined as ischaemic tissue necrosis that develops in the area supplied by a pulmonary artery occluded by thrombus. Parenchymal PI can be observed in approximately 30% of pulmonary thromboembolism (PTE) cases; however, it remains unclear in which PTE patients PI develops, how the presence of PI affects the clinical course and prognosis of the disease and how long it takes for the infarction to resolve. Thoracic computed tomography angiography (CTA) is an effective and reliable modality for the initial diagnosis of PI. However, due to radiation exposure, its frequent use in the follow-up of resolution is not appropriate. 2
In this report, a case of PI monitored using TUS, which is a bedside imaging modality that does not expose the operator or the patient to radiation, is presented and discussed in the context of the current literature.
Case report
A 44-year-old woman presented to the emergency department with sudden-onset dyspnoea and back pain. Her medical history revealed no chronic diseases, but she had undergone surgery a week earlier due to venous insufficiency. On physical examination, no abnormalities were detected other than tachypnoea. Her vital signs were as follows: blood pressure 125/78 mmHg, pulse 79 beats/min, temperature 36°C, respiratory rate 26 breaths/min and oxygen saturation 95% on room air. Laboratory results showed an elevated C-reactive protein (CRP) level (41 mg/L) but were otherwise unremarkable (Table 1). A chest radiograph revealed no abnormalities (Figure 1). The thoracic CTA performed with a preliminary diagnosis of PTE and the results were compatible with PTE (Figure 2). In the echocardiography performed, the right heart chambers were normal, and the pulmonary artery pressure was 20 mmHg. The patient was commenced on therapeutic doses of low-molecular-weight heparin and oral anticoagulant therapy. The patient's severe left flank pain, which was refractory to non-steroidal anti-inflammatory drugs, was attributed to PI secondary to PTE (Figure 3).
Laboratory values of the case.
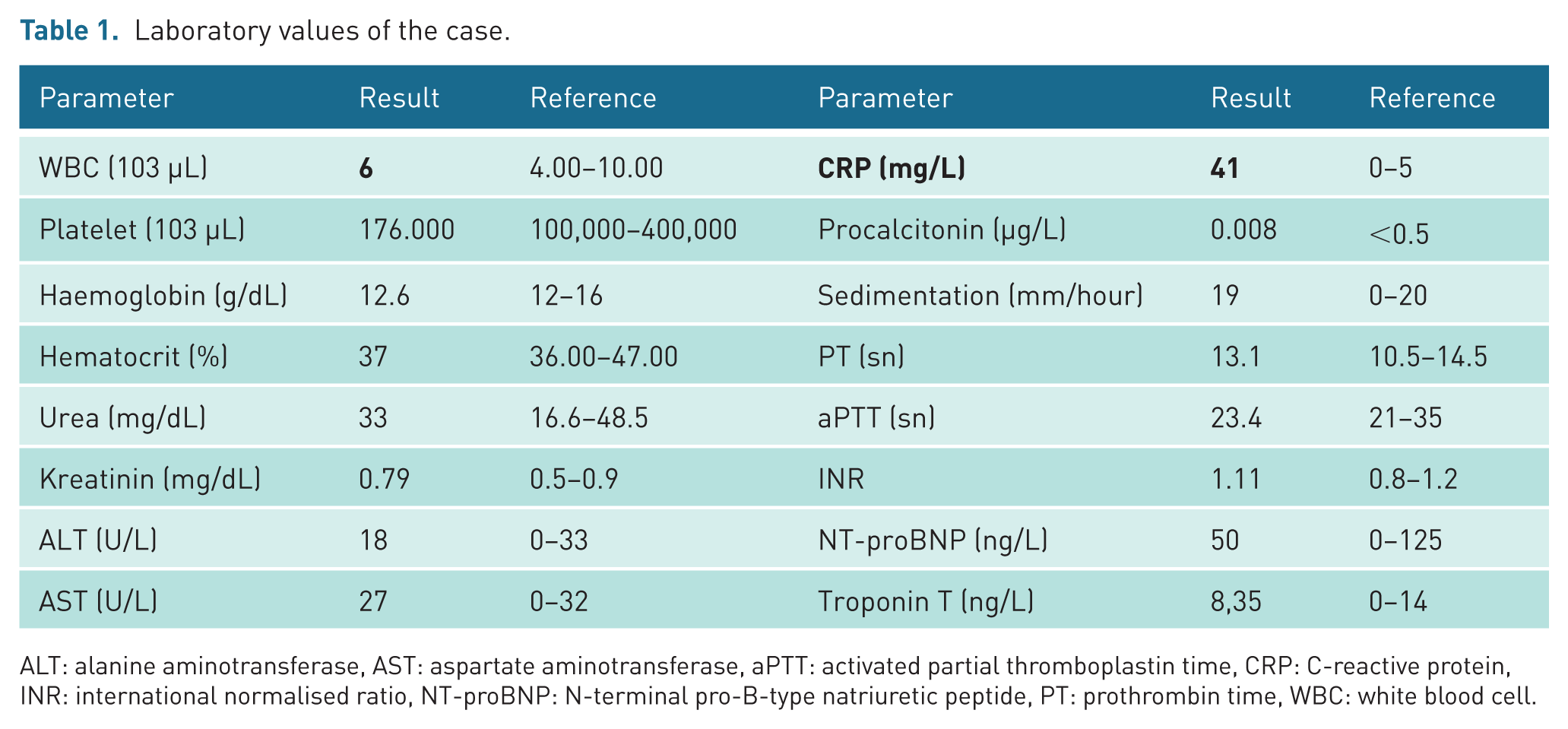
ALT: alanine aminotransferase, AST: aspartate aminotransferase, aPTT: activated partial thromboplastin time, CRP: C-reactive protein, INR: international normalised ratio, NT-proBNP: N-terminal pro-B-type natriuretic peptide, PT: prothrombin time, WBC: white blood cell.
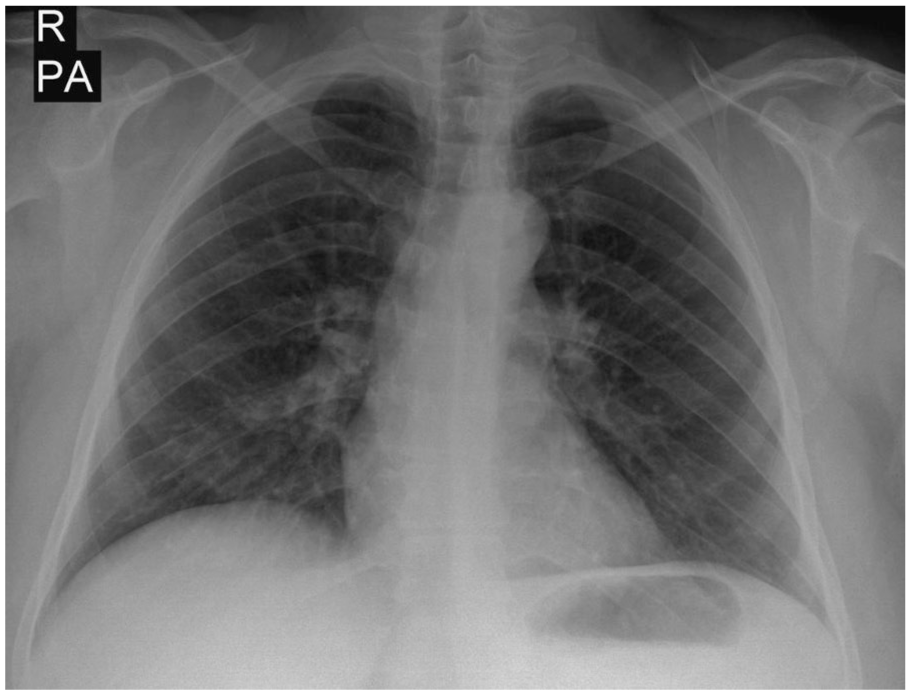
Posteroanterior chest radiograph obtained at the time of diagnosis.
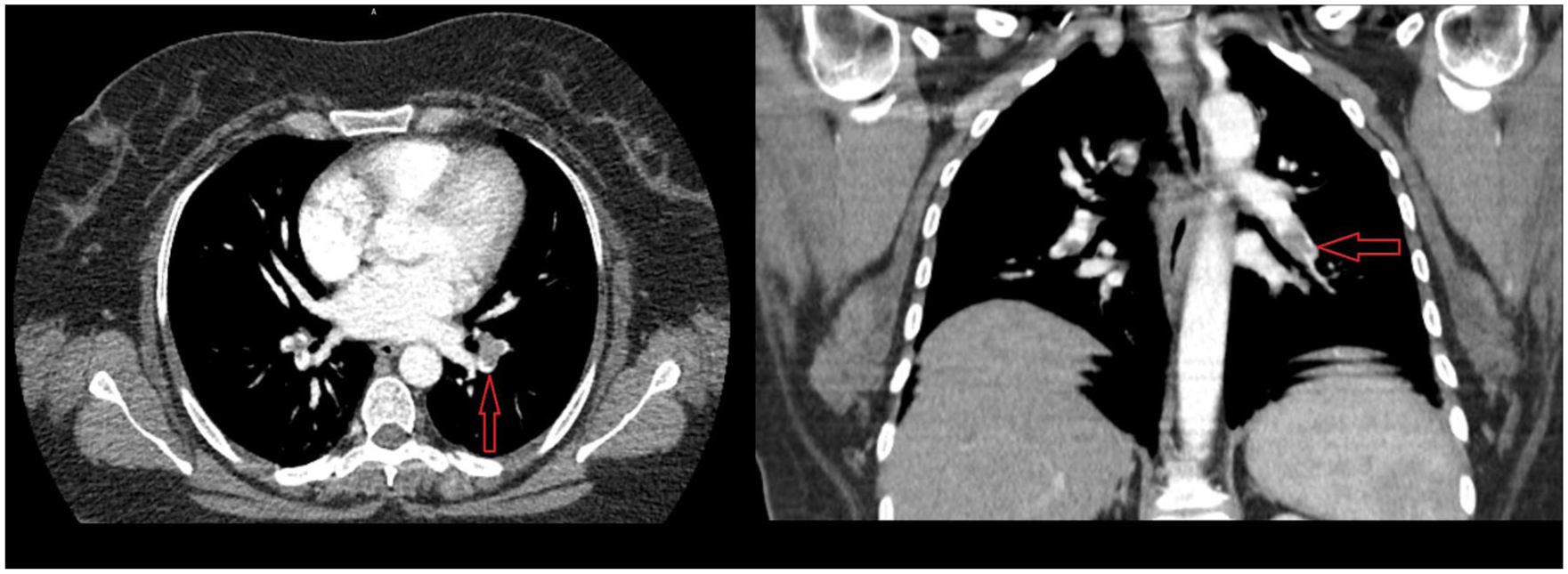
Thoracic computed tomography angiography demonstrating thrombus in the bilateral pulmonary arteries.
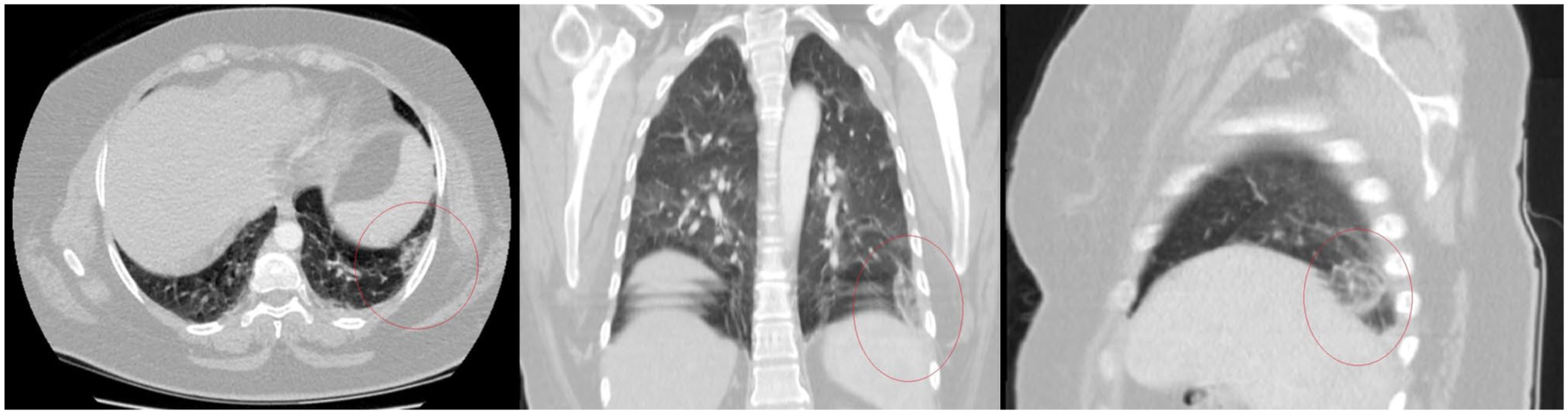
Thoracic computed tomography showing increased density in the posterior basal segment of the left lower lobe, suggestive of peripheral infarction.
TUS revealed a hypoechoic consolidation area measuring approximately 19 × 11 mm along the posterior axillary line of the left hemithorax. At the end of the first week of treatment, the patient, with an INR value of 2.2, was discharged with a planned weekly TUS follow-up. During outpatient follow-ups, the patient's symptoms improved significantly, and the back pain decreased. By the sixth week of treatment, the peripheral consolidation was observed to have diminished and completely resolved (Figure 4–9).
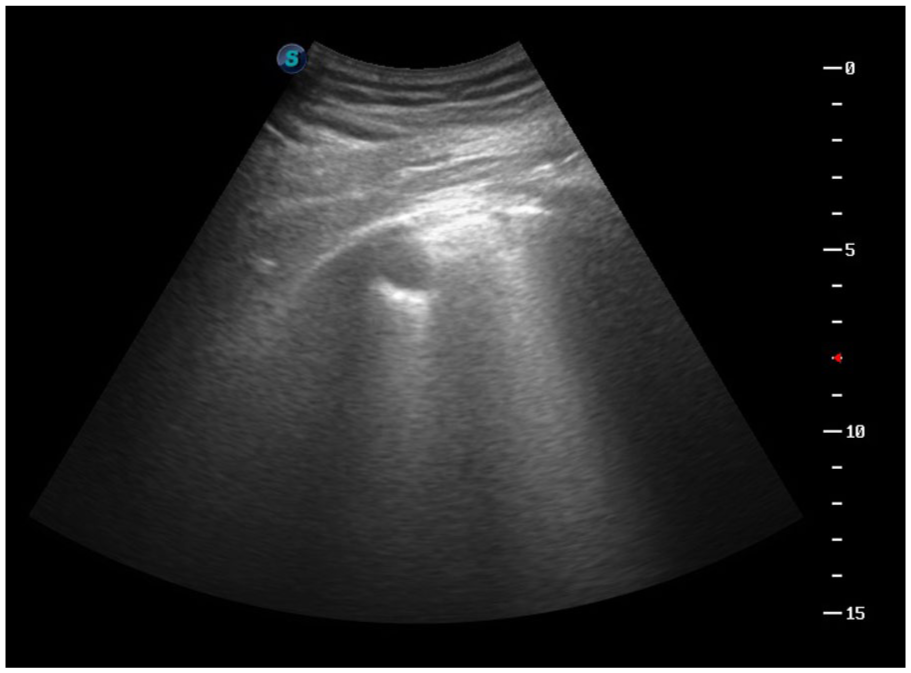
Thoracic ultrasound at the time of diagnosis revealing a hypoechoic area of consolidation measuring approximately 19 × 11 mm in the posterior axillary line of the left hemithorax.
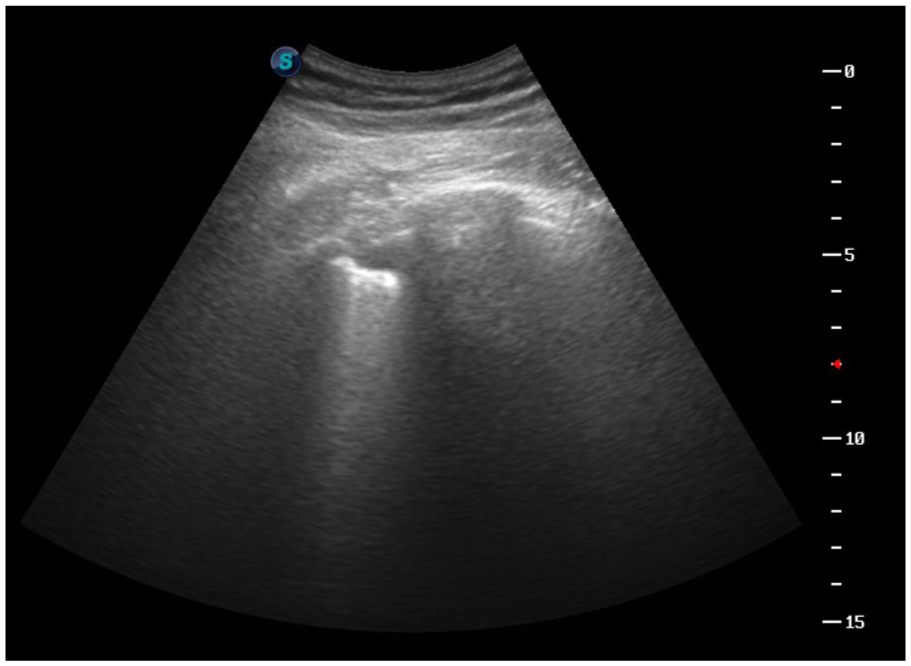
Thoracic ultrasound at 1 week after diagnosis showing a hypoechoic area of consolidation measuring approximately 17 × 10 mm in the posterior axillary line of the left hemithorax.
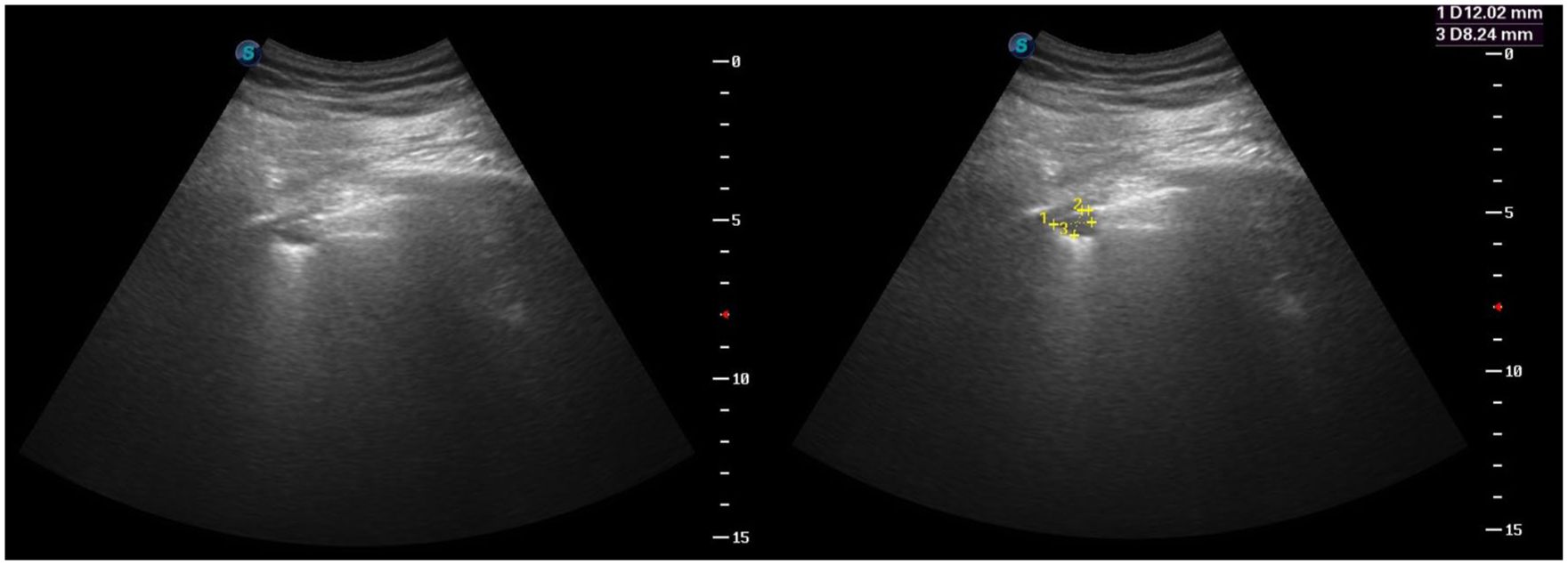
Thoracic ultrasound at 2 weeks after diagnosis demonstrating a hypoechoic area of consolidation measuring approximately 12 × 8 mm in the posterior axillary line of the left hemithorax.
Thoracic ultrasound at 3 weeks after diagnosis showing a hypoechoic area of consolidation measuring approximately 12 × 6 mm in the posterior axillary line of the left hemithorax.
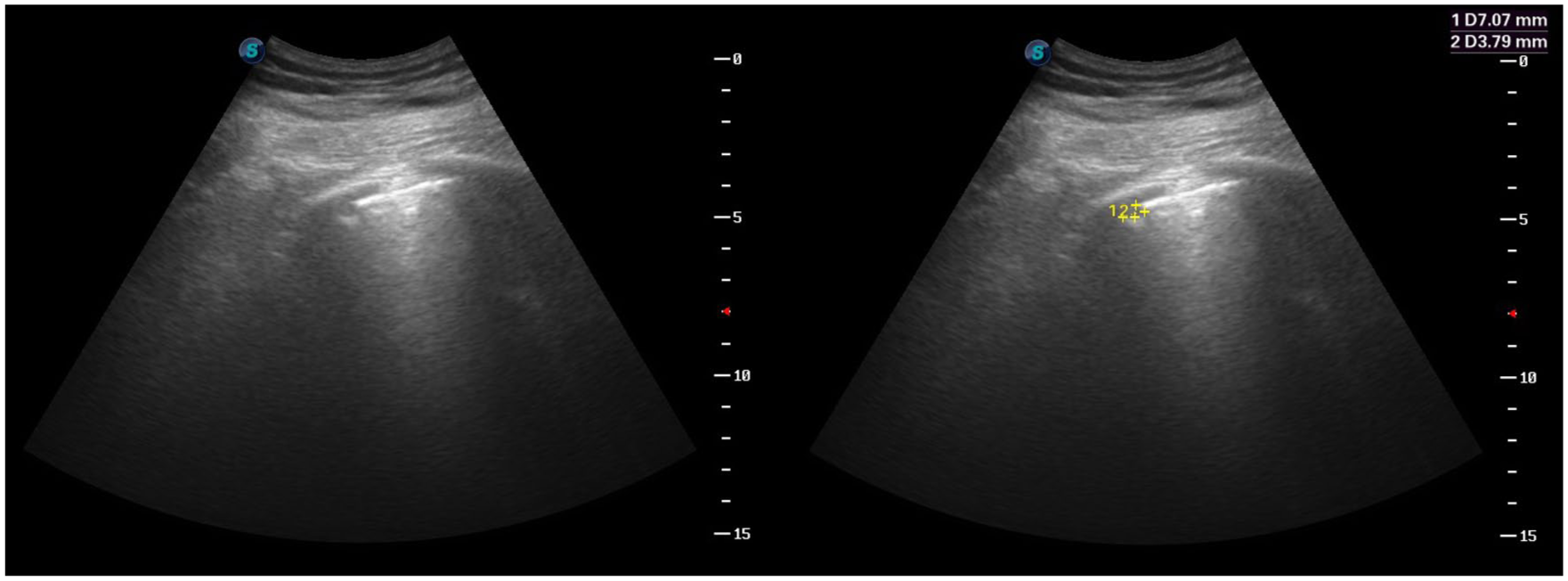
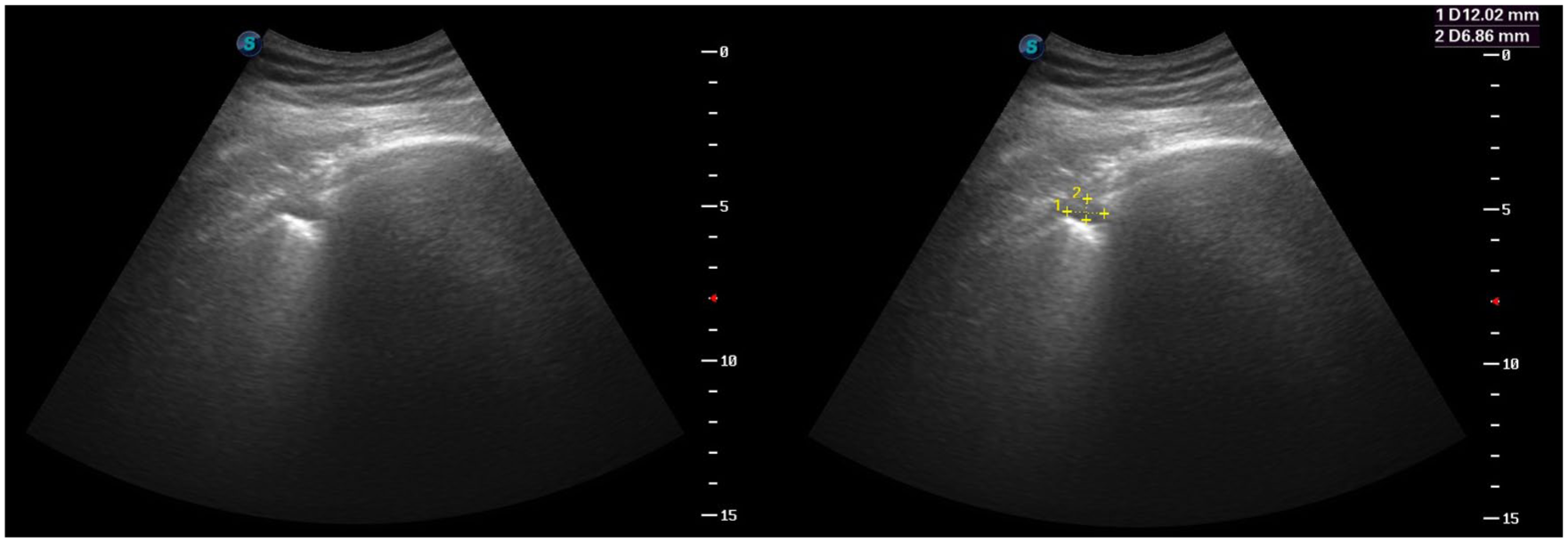
Thoracic ultrasound at 4 weeks after diagnosis revealing a hypoechoic area of consolidation measuring approximately 7 × 3 mm in the posterior axillary line of the left hemithorax.
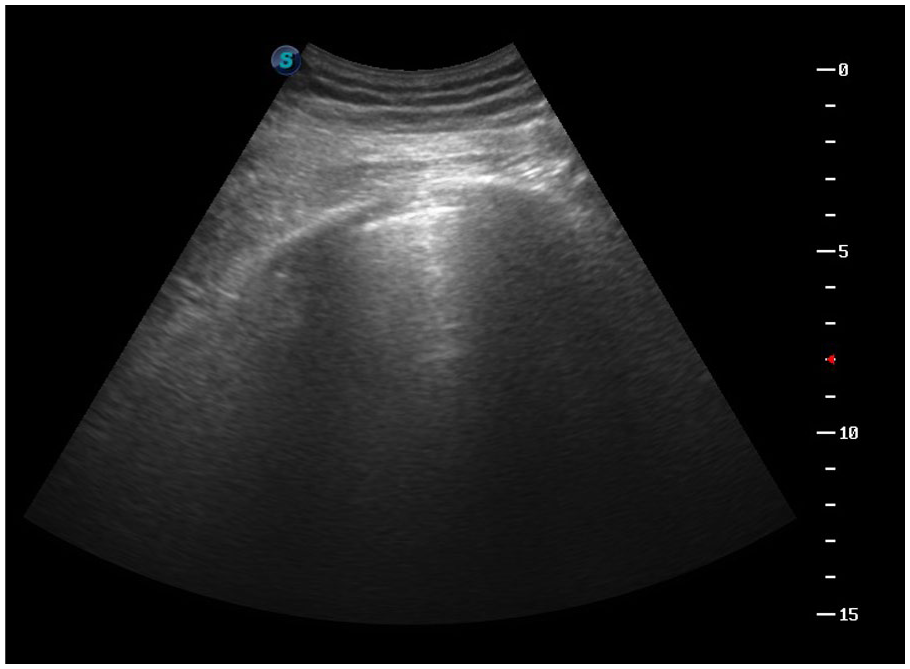
Normal sonographic appearance at the fifth week of diagnosis.
Discussion
PI is an ischaemic tissue necrosis that occurs in the area supplied by a pulmonary artery following its occlusion by a thrombus. While infarctions affecting other organs, such as the heart and brain, are often associated with high mortality, the clinical significance of parenchymal PI, which occurs in approximately 30% of PTE cases, remains incompletely understood. Specifically, it is still unclear which PTE patients are at risk of developing PI, how PI affects disease progression and prognosis and the time frame for its resolution. Historically, PI has been considered more common in elderly patients with significant cardiac comorbidities, where its presence has been associated with impaired cardiac function and poorer clinical outcomes. However, recent studies suggest that younger, otherwise healthy individuals without comorbidities may in fact be at a higher risk of PI due to a less-developed collateral blood supply. 3
PI, observed in approximately one-third of patients with PTE, has been the subject of numerous studies. The majority of these studies indicate that the presence of PI does not lead to a significant difference in mortality. 4 However, a few studies suggest that, even in the absence of a mortality difference, PI may be associated with certain adverse clinical outcomes. Cha et al. 5 found no difference in mortality between PTE patients with and without PI but reported a higher frequency of thrombolytic agent use in the PI group. Similarly, Kaptein et al. 6 observed that PTE patients with PI experienced greater functional limitations during a three-month follow-up period. In addition, secondary infections that develop within the infarcted lung tissue may negatively affect survival, further contributing to the potential clinical consequences of PI.
Chest radiography is not a useful tool for diagnosing PTE. Although historically significant, chest radiographs and the Hampton’s hump sign have low sensitivity (22%) in detecting PI. While novel imaging modalities such as MR-PET/CT have been explored for the diagnosis of PI, CTA remains the gold standard. 6 Despite CTA being the preferred imaging modality, TUS has shown promise in both diagnosing PTE and detecting PI in affected patients. TUS offers several advantages, including the absence of radiation exposure, bedside applicability, real-time imaging capabilities, cost-effectiveness and repeatability. A recent meta-analysis incorporating 18 studies and 2158 patients demonstrated that TUS has a specificity of 87% and a sensitivity of 80% in diagnosing PI. 7 Nazerian et al. 8 conducted a study on 450 patients diagnosed with pulmonary PTE to evaluate whether a diagnostic strategy based on TUS data could safely reduce the need for thoracic CTA. In their study, they identified a PI using right posterior TUS in a 60-year-old patient presenting with dyspnoea and right pleuritic pain. The infarcted area was surrounded by a small pleural effusion, demonstrating that PI can be effectively detected using TUS.
The development of PI in PTE remains an incompletely understood phenomenon. While radiological studies indicate that PI is present in approximately one-third (30%) of PTE cases, post-mortem studies suggest that its actual prevalence may be even higher. In a study by Chengsupanimit et al. 9 involving 74 patients with PI (mean age: 55 years), a 97% survival rate was reported on discharge. Follow-up assessments at the third and sixth months after discharge revealed a slight decline in survival rates (93% and 88%, respectively). The authors concluded that patients with PI may not necessarily have worse clinical outcomes compared to those without infarction. An important finding of this study was that PI persisted on follow-up CT scans for an average duration of 10 weeks (ranging from 1 to 21 weeks). Based on these findings, the authors recommended that patients diagnosed with PI should be monitored for at least 2 months following discharge. Given these considerations, detecting and diagnosing PI in PTE cases may hold clinical significance. In addition to diagnosing PI, determining the time frame for its resolution is a crucial aspect of patient management. However, the use of CT for follow-up is limited owing to concerns regarding high levels of radiation exposure, making it impractical for frequent monitoring. A review of the English-language literature reveals numerous studies demonstrating the utility of TUS in detecting PI in PTE cases. However, there is a notable scarcity of research evaluating the feasibility of using TUS for the follow-up of PI resolution. One of the few studies on this topic, conducted by Safai Zadeh et al., 10 retrospectively analysed a small cohort of patients with peripheral PI. In their study of 27 PTE, 26 out of 27 infarcted lesions (96.3%) persisted for an average duration of 10 weeks (range: 3–32 weeks). Notably, the size of the reference lesions had significantly decreased by the final follow-up examination (p < 0.05). Based on these findings, the authors concluded that TUS may be a useful modality for monitoring peripheral lesions suggestive of PI in PTE cases.
Conclusion
Infarction, defined as tissue necrosis and cell death due to ischaemia, is identified in a significant proportion of PTE cases. However, the impact of PI on disease prognosis and progression remains a topic of debate. Given this uncertainty, we emphasise the importance of both diagnosing and monitoring PI. It should be noted that TUS is limited to visualising peripherally located, pleura-based lesions. Nevertheless, considering its non-invasive nature and bedside applicability, we believe that TUS can be a valuable tool for the follow-up of PIs initially detected by USG during the diagnostic phase.
Footnotes
Ethical Considerations
Author Contributions
Conceptualisation: Coşkun Doğan, Göksel Menek
Data curation: Coşkun Doğan, Gönül Seven Yalçin
Formal analysis; Göksel Menek, Gönül Seven Yalçin
Funding acquisition: Coşkun Doğan, Mustafa Aydoğduoğlu, Sedanur Coşkun Tok
Investigation: Coşkun Doğan, Mustafa Aydoğduoğlu, Gönül Seven Yalçin
Methodology: Coşkun Doğan, Gönül Seven Yalçin, Sedanur Coşkun Tok
Project administration: Coşkun Doğan, Göksel Menek, Sedanur Coşkun Tok
Resources: Coşkun Doğan, Mustafa Aydoğduoğlu, Sedanur Coşkun Tok
Software: Coşkun Doğan, Göksel Menek, Mustafa Aydoğduoğlu
Supervision: Göksel Menek, Mustafa Aydoğduoğlu, Gönül Seven Yalçin
Validation: Coşkun Doğan, Mustafa Aydoğduoğlu, Gönül Seven Yalçin
Visualisation: Göksel Menek, Mustafa Aydoğduoğlu, Gönül Seven Yalçin
Roles/Writing – original draft and writing – review & editing: Coşkun Doğan
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.