
Abstract
Introduction:
Limb body wall complex is a rare polymalformative syndrome which consists of an abdominal and/or thoracic wall defect with an extremely short umbilical cord associated with kyphoscoliosis, intestinal malrotation, and lower limb defects.
Case report:
A 31-year-old primigravida presented with monochorionic monoamniotic twin pregnancy with discordant anomaly. One fetus had exomphalos, acrania, bilateral talipes, a single umbilical artery, kyphoscoliosis and a short umbilical cord, findings suggestive of limb body wall complex. An ultrasound one week later revealed an unfortunate intrauterine fetal demise of both twins. The postmortem examination confirmed the antenatal diagnosis of limb body wall complex. Since the parents were anxious to avoid any risk of recurrence in subsequent pregnancies, skin samples of both babies were sent for genetic workup. The Chromosomal Micro Array of both fetuses was reported to be normal.
Discussion:
Different pathophysiologic mechanisms have been proposed to explain the anomalies associated with limb body wall complex. These include early amnion rupture, vascular disruption, and embryonic maldevelopment. Differential diagnosis must be made with isolated gastroschisis, isolated omphalocele, and other polymalformative syndromes such as pentalogy of Cantrell.
Conclusion:
Early morphological assessment of the fetus at the time of the first-trimester screening scan can be of utmost importance to diagnose a polymalformative syndrome, which may be incompatible with life. An omphalocele, even in the absence of genetic or chromosomal abnormalities, may be associated with a lethal syndrome, that is, limb body wall complex. This should specifically be thought of and searched for, especially in fetuses who present with omphalocele in combination with curvature abnormalities of the spine.
Keywords
Introduction
Limb body wall complex (LBWC) or body stalk anomaly (BSA) is a rare polymalformative syndrome which has a reported incidence of 1 in 7500 pregnancies 1 and 1 in 14,000 to 1 in 31,000 births. 2 The condition consists of an abdominal and/or thoracic wall defect with an extremely short umbilical cord associated with kyphoscoliosis, intestinal malrotation, and lower limb defects. 3 Figure 1 elucidates the features of LBWC in comparison with a normal fetus (Figure 1).
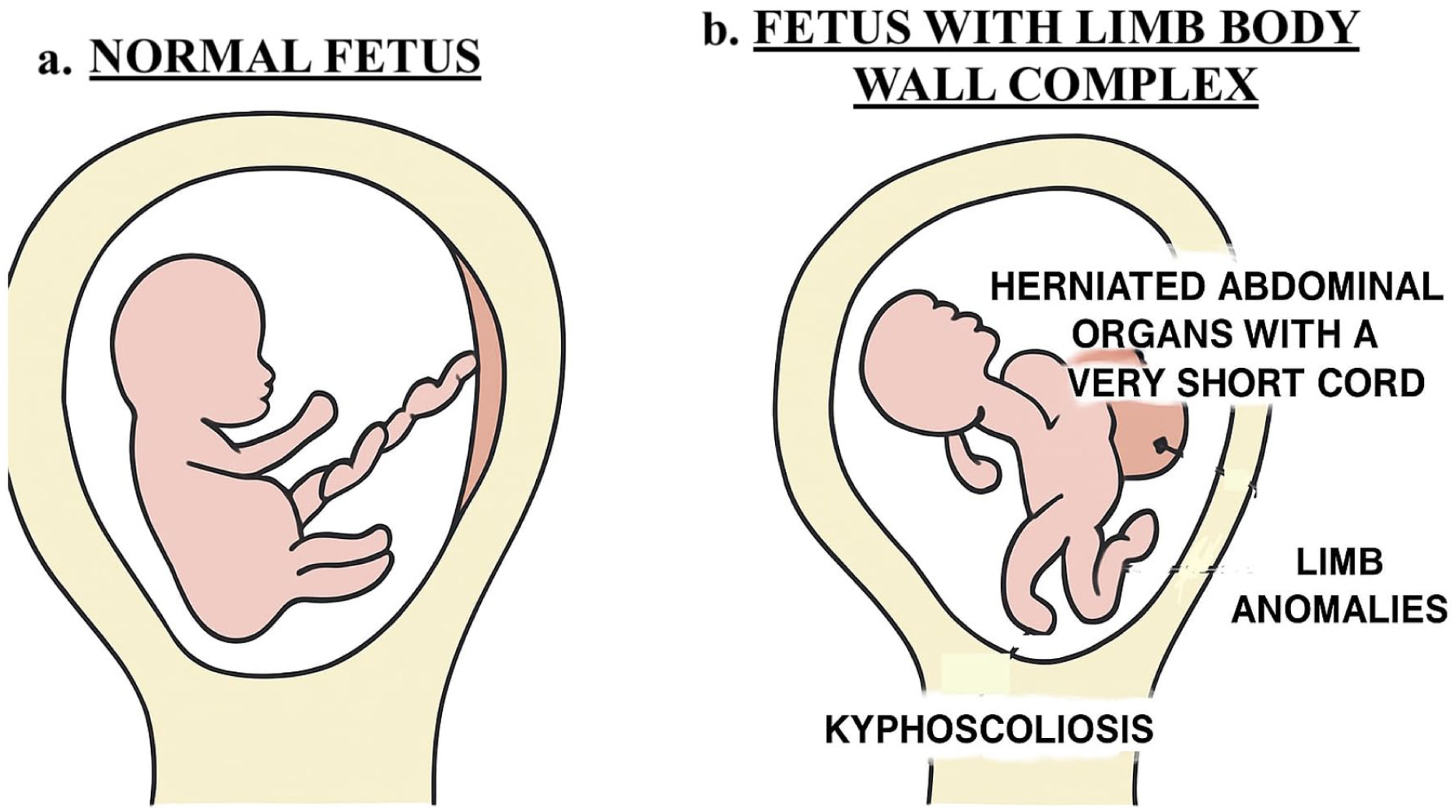
Diagrammatic representation showing (a) normal fetus and (b) fetus with limb body wall complex.
Occurrence of LBWC in monozygotic twins has been reported only rarely. 3 To the best of our knowledge, only seven cases of LBWC in a twin pregnancy have been reported so far, 4 of which only three were detected as a discordant anomaly in a monozygotic monoamniotic twin pregnancy. 4 Our case represents the fourth reported case of monochorionic monoamniotic (MCMA) twin pregnancy discordant for LBWC.
Case Report
A 31-year-old primigravida with no significant past or family history was referred to our fetal medicine centre at 16 weeks gestation because of a spontaneously conceived MCMA twin pregnancy with discordant anomaly. One of the fetuses was suspected to have exomphalos and acrania on a routine nuchal scan done elsewhere. A review ultrasound done at our centre confirmed a live MCMA twin pregnancy with one normal fetus. The other fetus was noted to have multiple anomalies: exomphalos (with fetal liver as content) (Figure 2), exposed brain tissue with frog-eye sign suggestive of acrania (Figure 3(a) and (b)), bilateral talipes (Figure 4), a single umbilical artery (Figure 5), curvature abnormalities of the spine (Figure 6), and a short umbilical cord. There was evidence of cord entanglement of the two fetuses, which was further confirmed on review of her previous scans. Given the above findings, a diagnosis of LBWC was suspected.
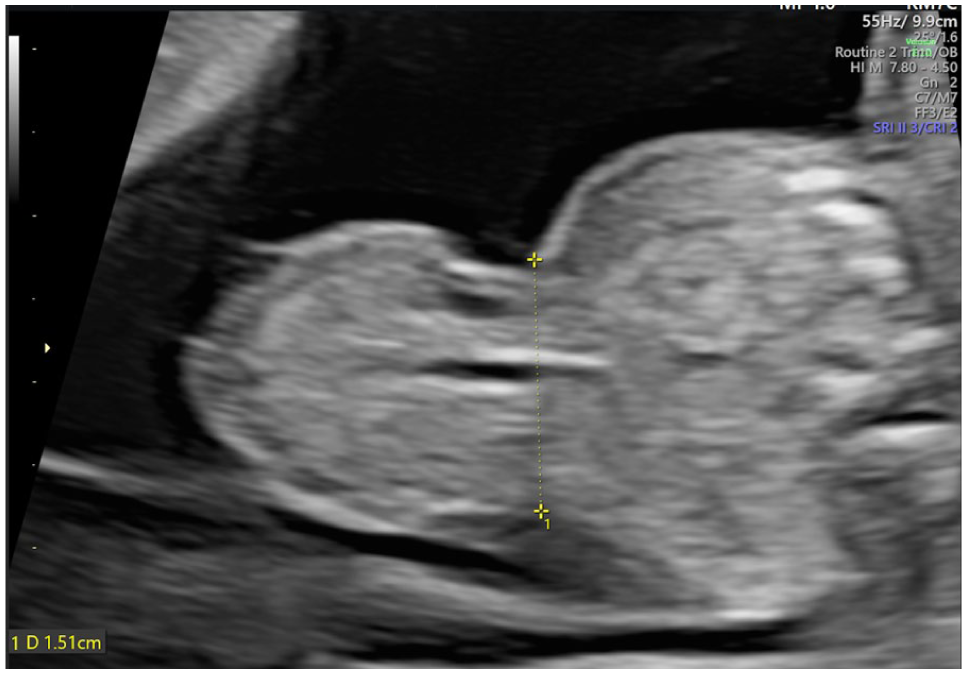
Ultrasound image of the affected fetus at 16 weeks’ gestation showing exomphalos with fetal liver as content.
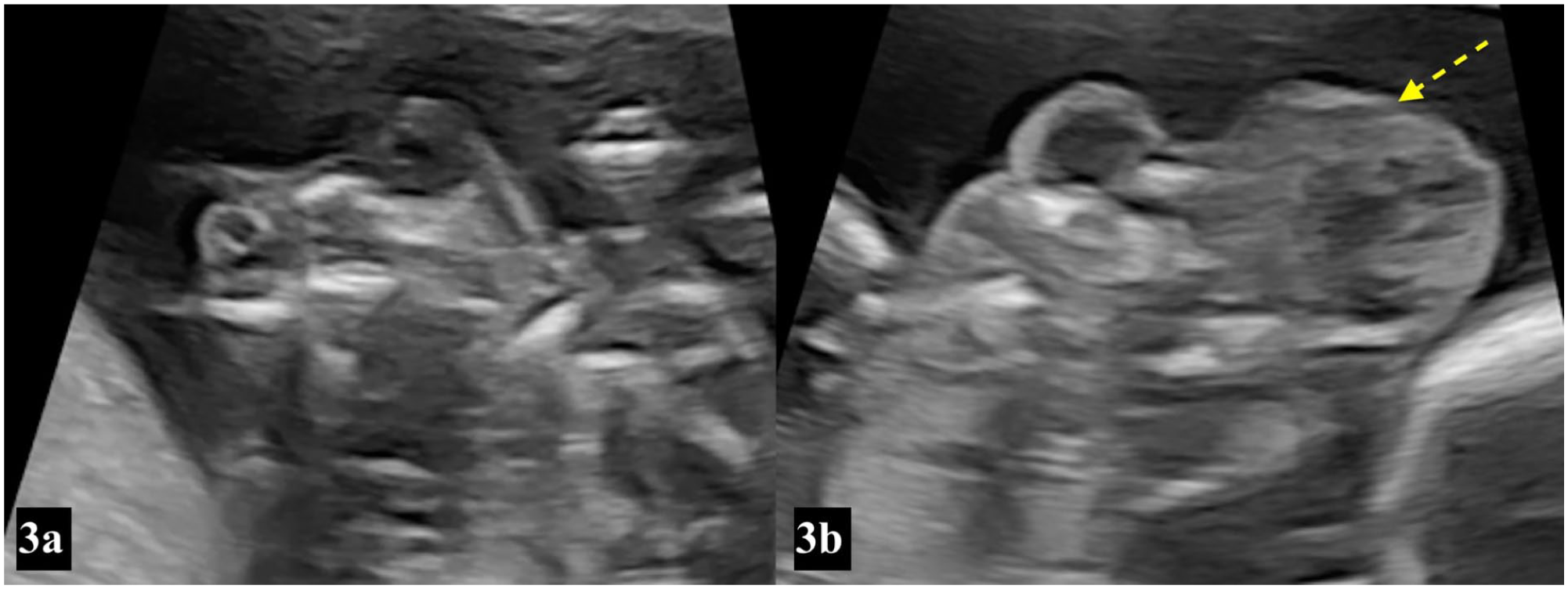
Ultrasound image of the affected fetus at 16 weeks’ gestation showing (a) frog eye sign and (b) exposed brain tissue suggestive of acrania (dotted arrow).
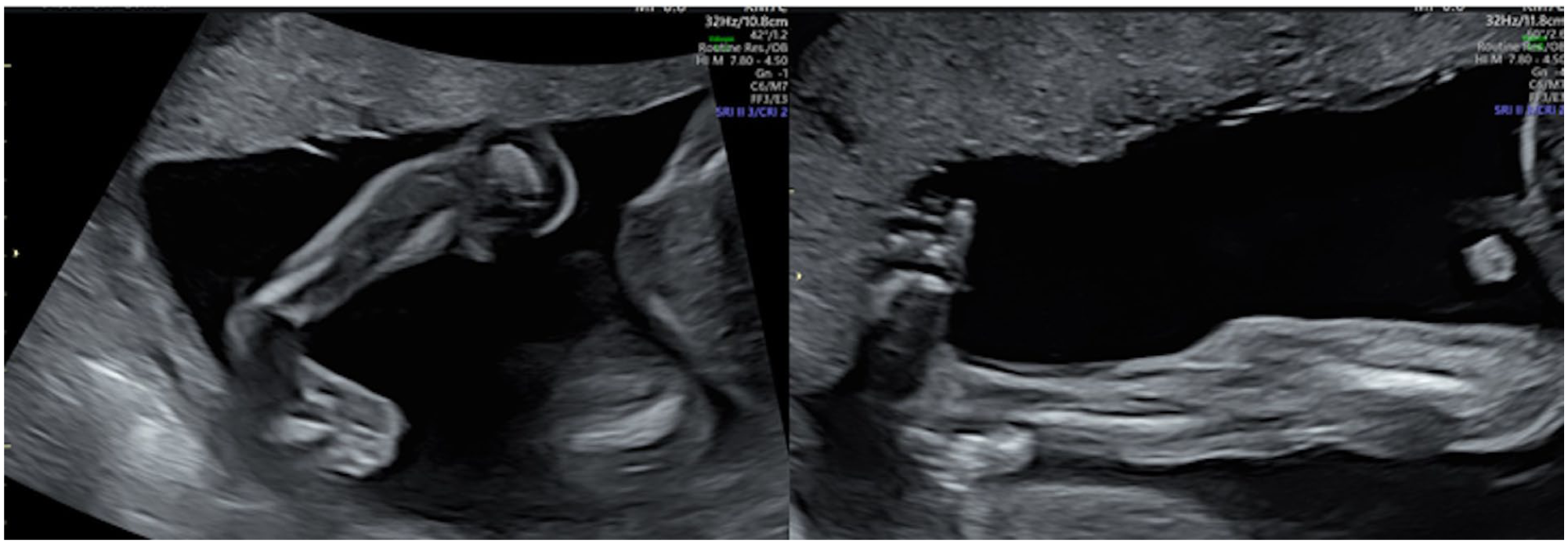
Ultrasound image of the affected fetus at 16 weeks’ gestation showing bilateral talipes.
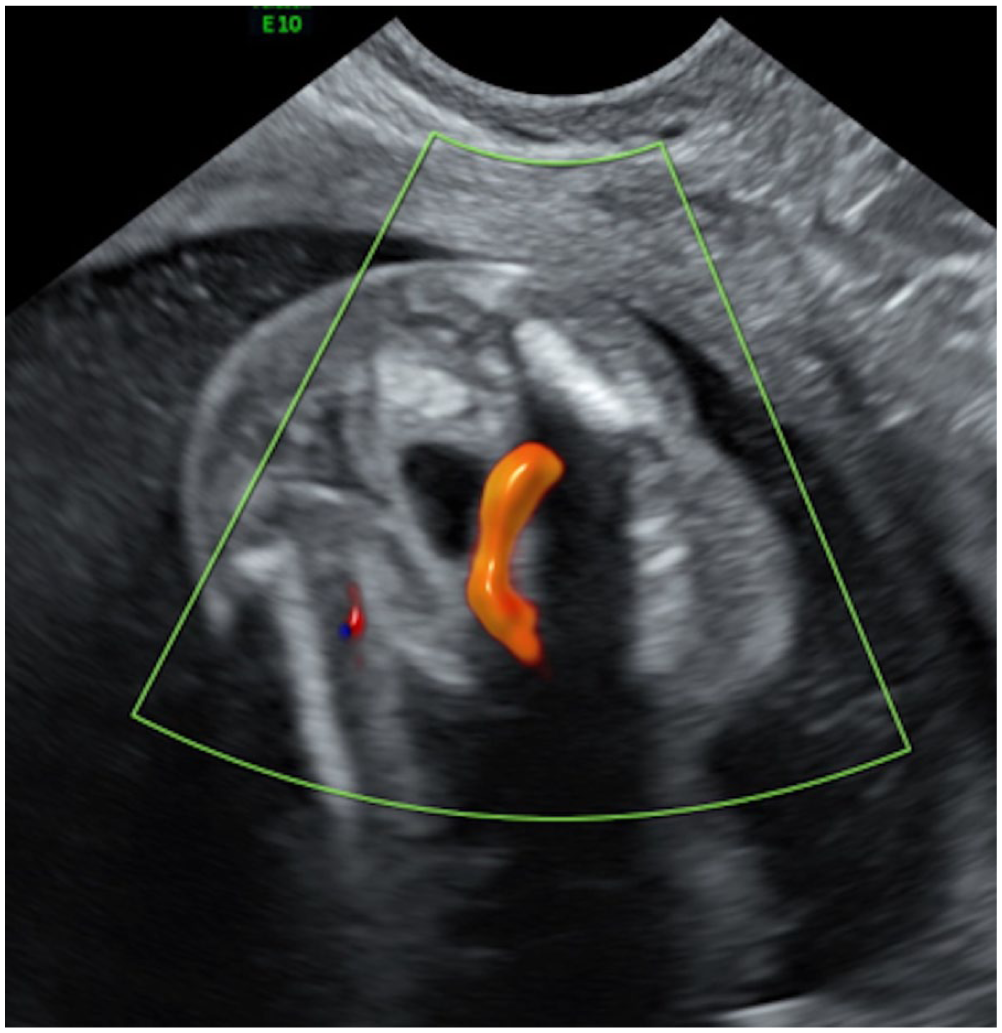
Ultrasound image of the affected fetus at 16 weeks’ gestation showing a single umbilical artery.

Three-dimensional color-rendered image of the affected fetus at 16 weeks’ gestation showing curvature abnormalities of the spine and acrania.
Since it was an MCMA twin pregnancy, the patient was planned for endoscopic cord occlusion of the affected fetus followed by laser transection of the cord to keep the healthy twin safe. Infection screening was sent before the scheduled procedure. The patient presented one week later with the reports of the infection screen when an ultrasound revealed an unfortunate intrauterine fetal demise of both twins.
Postnatally, on gross examination, the anomalous twin was noted to have an omphalocele, acrania with exposed brain tissue, abnormal hands (absent thumb, fourth and fifth digits with overlapping second and third digits), and bilateral talipes. The external examination confirmed the antenatal diagnosis of LBWC. Since the parents were anxious to avoid any risk of recurrence in subsequent pregnancies, skin samples of both babies were sent for genetic workup. The Chromosomal Micro Array of both fetuses was reported to be normal.
Discussion
The diagnosis of LBWC is based on the presence of two out of the three criteria as elucidated by Van Allen et al. in 1987: exencephaly/encephalocele along with facial clefts, thoraco- and/or abdominoschisis, and limb defects. 5 The condition consists of an abdominal and/or thoracic wall defect, an extremely short umbilical cord, kyphoscoliosis, intestinal malrotation, and lower limb defects. 3 The abdominal organs are seen outside the abdominal cavity and are found to be directly attached to the placenta. The umbilical cord usually contains a single umbilical artery. We found several of the above-mentioned defects in our case, namely exomphalos, kyphoscoliosis, single umbilical artery, short umbilical cord, and limb defects. Although acrania is not commonly seen in fetuses with LBWC, cranial defects such as execenphaly/encephalocele have been described as a part of the spectrum of associated anomalies. 5
Various studies have classified LBWC into different subtypes depending on the associated anomalies.6,7 However, it may not be necessary to distinctly differentiate these subtypes or to separate LBWC from related entities such as the Omphalocele, Exstrophy of bladder, Imperforate anus, Spinal defects (OEIS) complex, as emerging evidence suggests that these anomalies likely share overlapping pathogenetic mechanisms and may represent varying manifestations of a similar underlying developmental insult.
Different pathophysiologic mechanisms have been proposed to explain these anomalies. These include early amnion rupture, vascular disruption, and embryonic maldevelopment. Early amnion rupture before the coelomic cavity’s obliteration may lead to fibrous bands forming from the exposed chorionic surface. 5 Part of the fetus may pass out from the site of the ruptured amnion into the coelom, thus causing traumatic lesions on the fetal abdominal wall, skull, and spine. Van Allen et al. in 1987 suggested the theory of vascular disruption, also known as the endogenous theory. 5 He stated that the compromise of embryonic blood flow during the initial six weeks may lead to failure of closure of the ventral body wall. The association of LBWC with maternal cocaine abuse, a vasoconstrictive agent, supports this theory. The theory of embryonic maldevelopment stated that LBWC may occur due to the faulty folding process of the embryonal germinal disk along the three axes in the fifth week, which disrupts the normal transformation of the embryo into a cylindrical shape. 8 A fourth hypothesis of LBWC in monozygotic twins is an incomplete division of a single zygote, resulting in a common peritoneal cavity. 9
Various risk factors have been proposed for LBWC, such as primiparity, young maternal age, pre-gestational diabetes, maternal smoking, alcohol or cocaine use, and twin gestation. 8 Twinning has been documented in as high as 10.7% of cases with LBWC. 8 Our case was also a primigravida with twin gestation; however, she had none of the other risk factors. No gender predilection has been found for LBWC. This condition is almost always found to occur sporadically. 8 In general, the incidence of chromosomal abnormalities and genetic syndromes is not increased, as was seen in our case. 3 However, there may be a recurrence risk of this condition, as observed in two cases previously, 10 which may suggest a genetic predisposition. The literature has also reported a rare association with Trisomy 16 and maternal uniparental disomy (UPD) 16. 3 Hence, it can be safely suggested that invasive testing and genetic counseling should be discussed in such cases, and its impact on future pregnancies must be ascertained.
LBWC can be diagnosed on ultrasound as early as the first trimester. 1 The International Society of Ultrasound in Obstetrics and Gynecology (ISUOG) has suggested that assessment of the fetal anatomy should be included as routine at the time of first-trimester nuchal scan. Evaluation of the fetal anatomy during the first-trimester scan can be of great benefit in ruling out major fetal defects including acrania, exomphalos, and spine defects, among others. Maternal serum alpha-fetoprotein is found to be raised in these pregnancies, which may further aid in the diagnosis. 11
Differential diagnosis must be made with isolated gastroschisis, isolated omphalocele, and other polymalformative syndromes such as pentalogy of Cantrell, among others. 8 This is important, as the prognosis of LBWC is extremely poor compared to isolated gastroschisis or omphalocele.
LBWC is generally considered a uniformly fatal condition, with rare reports of short-term postnatal survival. 1 Management decisions for these pregnancies are individualized and guided by counseling and parental choice. Management of monochorionic twins discordant for a lethal structural anomaly is more challenging, as the antenatal demise of the affected fetus has direct implications on the healthy co-twin. Such pregnancies need to be referred to fetal medicine units for management. Optimal management plan for these pregnancies remains controversial. Management options for selective feticide in monochorionic twin pregnancies include radiofrequency or microwave ablation, bipolar cord coagulation, and laser ablation, among others. This protects the healthy co-twin from losing its blood into the terminated twin and its associated complications, including neurological sequelae.
Conclusion
Early morphological assessment of the fetus at the time of the first-trimester screening scan can be of utmost importance to diagnose a polymalformative syndrome, which may be incompatible with life. An omphalocele, even in the absence of genetic or chromosomal abnormalities, may be associated with a lethal syndrome, that is, LBWC. This should specifically be thought of and searched for, especially in fetuses who present with omphalocele in combination with curvature abnormalities of the spine.
Footnotes
Ethical considerations
Apollo Centre for Fetal Medicine and Therapy does not require ethical approval for reporting individual cases or case series.
Consent for publication
Written informed consent was obtained from the patient for her anonymous information including the images to be published in this article.
Author contributions
Dr T.A.V., Dr I.A., Dr A.P., Dr V.M., Dr S.C., and Dr A.K. contributed to this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Data availability statement
All relevant data supporting the findings of this case report are contained within the article. Additional details are available from the corresponding author upon request.
Guarantor
On behalf of all authors, Dr A.K. will act as the guarantor and will guarantee the manuscript’s accuracy and contributorship of all co-authors.