
Abstract
For more than a century, research on psychopathology has focused on categorical diagnoses. Although this work has produced major discoveries, growing evidence points to the superiority of a dimensional approach to the science of mental illness. Here we outline one such dimensional system—the Hierarchical Taxonomy of Psychopathology (HiTOP)—that is based on empirical patterns of co-occurrence among psychological symptoms. We highlight key ways in which this framework can advance mental-health research, and we provide some heuristics for using HiTOP to test theories of psychopathology. We then review emerging evidence that supports the value of a hierarchical, dimensional model of mental illness across diverse research areas in psychological science. These new data suggest that the HiTOP system has the potential to accelerate and improve research on mental-health problems as well as efforts to more effectively assess, prevent, and treat mental illness.
Keywords
Dating back to Kraepelin and other early nosologists, research on psychopathology has been framed around mental disorder categories (e.g., What biological malfunctions typify generalized anxiety disorder? How does antisocial personality disorder disrupt close relationships?). This paradigm has produced valuable insights into the nature and origins of psychiatric problems. Yet there is now abundant evidence that categorical approaches to mental illness are hindering scientific progress. Grounded in decades of research, an alternate framework has emerged that characterizes psychopathology using empirically derived dimensions that cut across the boundaries of traditional diagnoses. Recent efforts by a consortium of researchers to review and integrate findings relevant to this framework have given rise to a proposed consensus dimensional system, the Hierarchical Taxonomy of Psychopathology (HiTOP; Hierarchical Taxonomy of Psychopathology, 2018; Kotov et al., 2017).
Here, we first summarize the rationale behind dimensional rubrics for mental illness and briefly sketch the topography of the HiTOP system (for detailed reviews, see Kotov et al., 2017; Krueger et al., 2018). Second, we explain how HiTOP can be used to improve research practices and theory testing. Third, we review new evidence for the utility of HiTOP dimensions across various research contexts, from developmental psychology to neuroscience. Finally, we offer some practical recommendations for conducting HiTOP-informed research.
A Brief History of HiTOP
Mental illness is a leading burden on public-health resources and the global economy (DiLuca & Olesen, 2014; Vos et al., 2016). Recent decades have witnessed the development of improved social science methodologies and powerful new tools for quantifying variation in the genome and brain, leading to initial optimism that psychopathology might be more readily explained and objectively defined (e.g., Hyman, 2007). Yet the billions of dollars spent on research have failed to yield much in the way of new cures, objective assays, or other major breakthroughs (Shackman & Fox, 2018).
A growing number of clinical practitioners and researchers—including the architects of the National Institute of Mental Health Research Domain Criteria (RDoC)—have concluded that this past underperformance reflects problems with categorical diagnoses rather than any intrinsic limitation of prevailing approaches to understanding risk factors and treatment methods (Gordon & Redish, 2016). Categorical diagnoses—such as those codified in the Diagnostic and Statistical Manual of Mental Disorders (DSM) and the International Classification of Diseases (ICD)—pose several well-documented barriers to discovering the nature and origins of psychopathology, including pervasive comorbidity, low symptom specificity, marked diagnostic heterogeneity, and poor reliability (Clark, Cuthbert, Lewis-Fernández, Narrow, & Reed, 2017; Markon, Chmielewski, & Miller, 2011; Regier et al., 2013). Regarding reliability, for instance, the field trials for the fifth edition of the DSM (DSM–5; American Psychiatric Association, 2013) found that approximately 40% of diagnoses examined did not reach the cutoff for acceptable interrater agreement (Regier et al., 2013). Attesting to symptom-profile heterogeneity in the DSM, more than 600,000 symptom presentations satisfy diagnostic criteria for posttraumatic stress disorder (Galatzer-Levy & Bryant, 2013).
Addressing these problems requires a fundamentally different approach. HiTOP—like other dimensional proposals such as RDoC (e.g., Brown & Barlow, 2009; Cuthbert & Insel, 2013)—focuses on continuously distributed traits theorized to form the scaffolding for psychopathology. In the tradition of early factor analyses of disorder signs and symptoms in adults (e.g., Eysenck, 1944; Lorr, Klett, & McNair, 1963; Tellegen, 1985) and children (e.g., Achenbach, 1966; Achenbach, Howell, Quay, Conners, & Bates, 1991), a more recent quantitative analysis of psychological symptom co-occurrence has established a reproducible set of dimensions theorized to reflect the natural structure of psychological problems (Kotov et al., 2017).
Figure 1 provides a simplified schematic depiction of HiTOP, which features broad, heterogeneous constructs near the top of the model and specific, homogeneous dimensions near the bottom. HiTOP accounts for diagnostic comorbidity by positing dimensions (e.g., internalizing) that span multiple DSM diagnostic categories. It also models diagnostic heterogeneity by specifying fine-grain processes (e.g., worry, panic) that constitute the building blocks of mental illness. Indeed, profiles of narrow symptom dimensions (e.g., anhedonia, suicidality, situational fears) explain the variation on broad dimensions (e.g., elevated internalizing) in more detail.
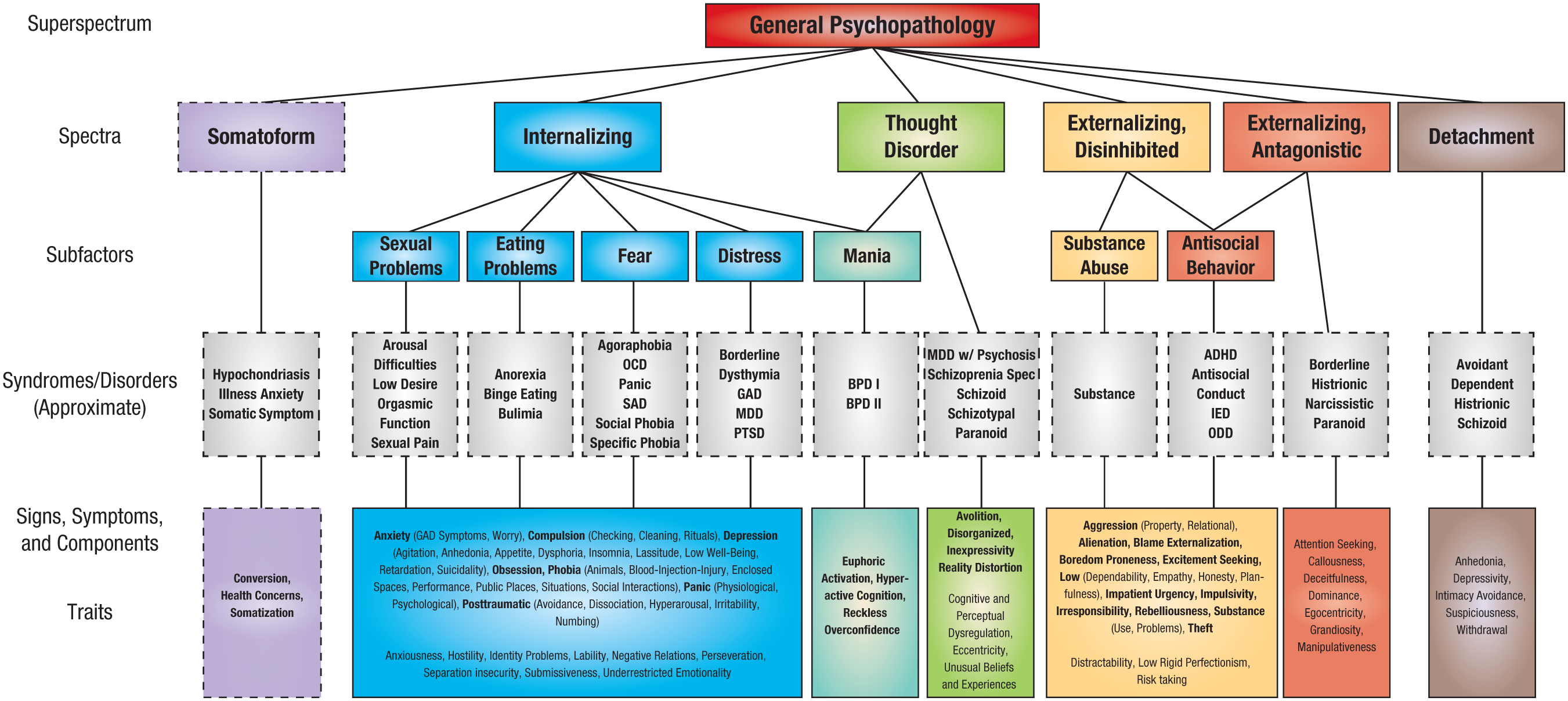
HiTOP consortium working model. Constructs higher in the figure are broader and more general, whereas constructs lower in the figure are narrower and more specific. Dashed lines denote provisional elements requiring further study. At the lowest level of the hierarchy (i.e., traits and symptom components), conceptually related signs and symptoms (e.g., phobia) are indicated in bold for heuristic purposes, with specific manifestations indicated in parentheses. ADHD = attention-deficit/hyperactivity disorder; BPD = bipolar disorder; GAD = generalized anxiety disorder; HiTOP = Hierarchical Taxonomy of Psychopathology; IED = intermittent explosive disorder; MDD = major depressive disorder; OCD = obsessive-compulsive disorder; ODD = oppositional defiant disorder; SAD = separation anxiety disorder; PD = personality disorder; PTSD = posttraumatic stress disorder.
HiTOP is an evolving model. An international group of researchers has assembled to investigate this structure and update it as new data emerge (Krueger et al., 2018). 1 (The HiTOP consortium publishes updates and revisions to the model on its website.) Indeed, the explicit goal of the HiTOP project is to follow the evidence. The system is open for any type of revision that is supported by sufficient evidence; its core assumption is that a more valid nosology can be developed on the basis of the empirical pattern of clustering among psychopathology phenotypes (i.e., symptoms and maladaptive traits).
Refining this dimensional model is a key priority, but it is only one step in the evolution of HiTOP. Another key priority is to use HiTOP to improve and accelerate research focused on mental health and illness. As described in detail below, HiTOP has the potential to advance theories of psychopathology and make mental-health research more efficient and informative.
HiTOP as a Psychopathology Research Framework
A distinguishing feature of HiTOP is its hierarchical organization (Fig. 1). Various processes—some specific, others quite broad—are potentially implicated in the origins and consequences of psychological problems across the life span (Forbes, Tackett, Markon, & Krueger, 2016). The hierarchical structure implies that any cause or outcome of mental illness could emerge because of its effects on broad higher order dimensions, the syndromes, or specific lower order dimensions (Fig. 2). Take trauma, for example. Suppose that research based on the HiTOP framework establishes that trauma exposure better predicts variation in the internalizing spectrum than in its constituent syndromes (e.g., depression, posttraumatic distress). How would this result change our conceptualization of this research area? It would call for an expansion of our etiological models of posttraumatic distress to focus on the broad internalizing spectrum, including psychobiological processes shared by the mood and anxiety disorders. We might advise a moratorium on research studies that examine only one DSM disorder in relation to trauma exposure; instead, for maximum efficiency, we would simultaneously consider various aspects of the internalizing spectrum (e.g., worry, rituals, insomnia, irritability) as outcomes in research studies. In addition, when making policy decisions regarding prevention and intervention resources, we might prioritize screening trauma-exposed individuals for the full range of internalizing problems, not just posttraumatic stress disorder. In sum, thinking hierarchically about mental illness can promote more efficient research practices and more nuanced theory.
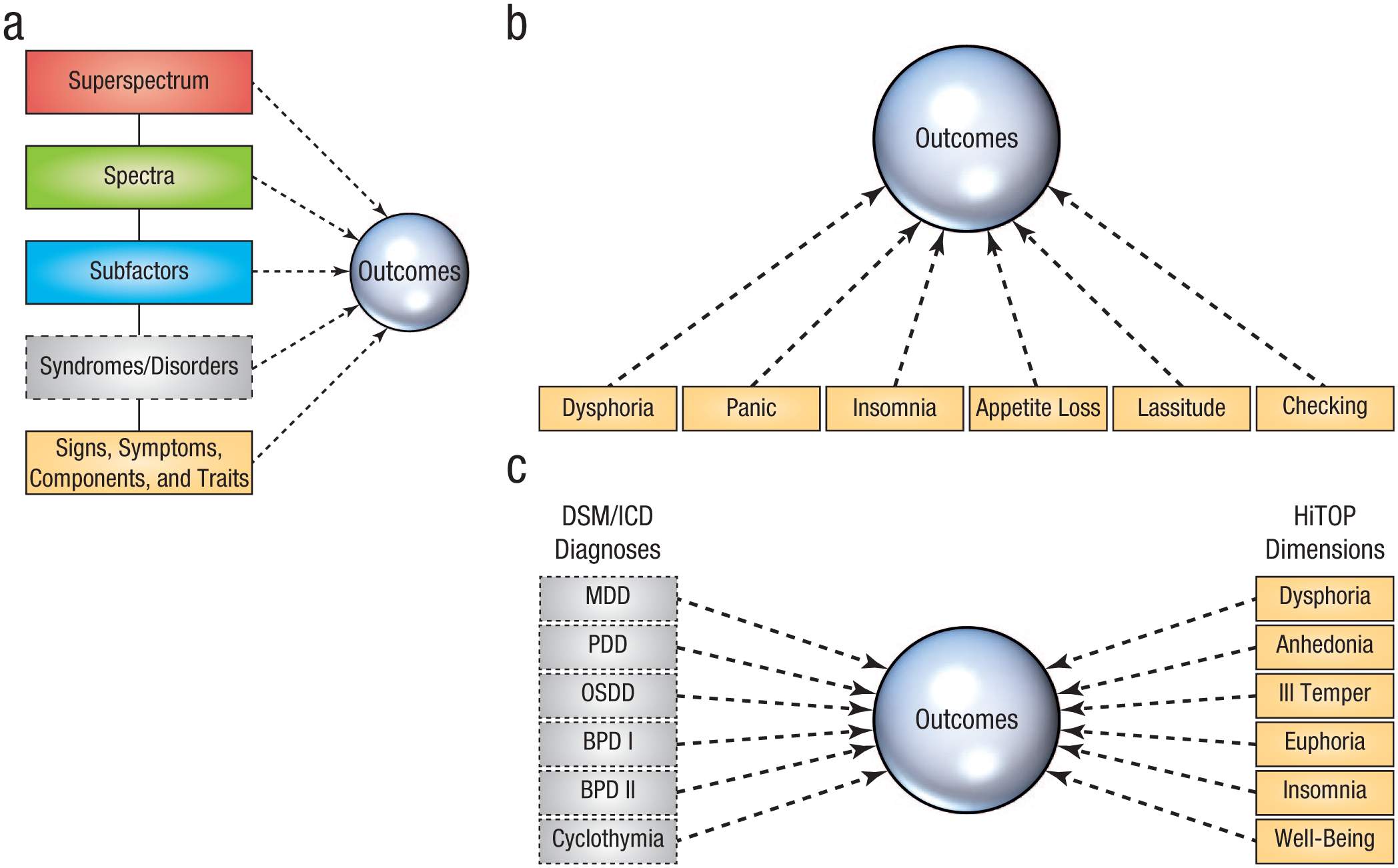
Conceptual diagrams of three possible HiTOP research designs. The diagrams show comparisons of the predictive validity (a) across HiTOP levels, (b) within HiTOP levels, and (c) of categorical diagnoses to HiTOP dimensions. BPD = bipolar disorder; DSM = Diagnostic and Statistical Manual of Mental Disorders; HiTOP = Hierarchical Taxonomy of Psychopathology; ICD = International Classification of Diseases; MDD = major depressive disorder; OSDD = other specified depressive disorder; PDD = persistent depressive disorder.
To illustrate these points, we now consider a more detailed example of putting HiTOP into practiceFig. 3). For ease of presentation, DSM diagnoses constitute the basic units of assessment. 2 A subset of HiTOP constructs are involved (listed in order of increasing granularity): the internalizing spectrum; fear, distress, and eating pathology subfactors; and their component syndromes (e.g., binge eating disorder, agoraphobia). These constructs serve as the predictor variables here.
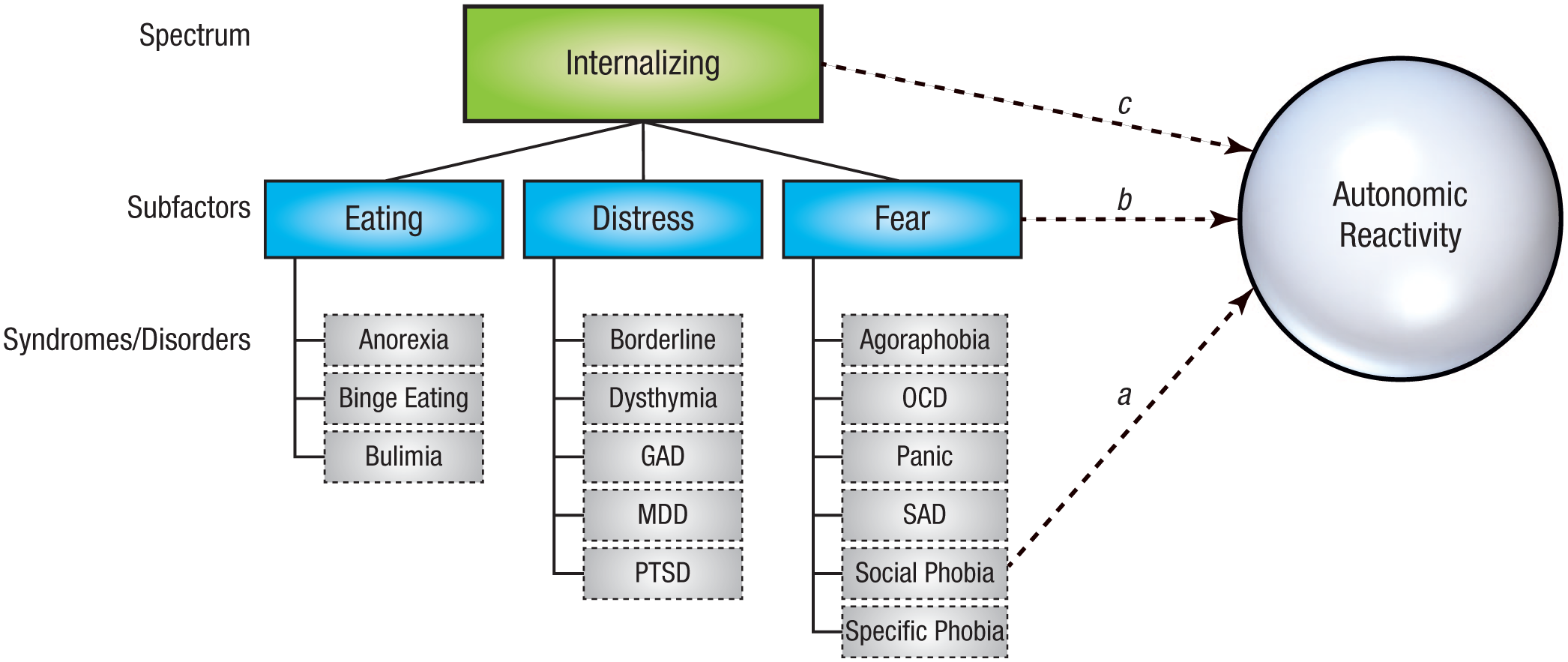
Heuristic model of the internalizing domain in relation to autonomic reactivity to a laboratory challenge. Paths a, b, and c represent regressions of the outcome on dimensions at different levels of the hierarchical model. GAD = generalized anxiety disorder; MDD = major depressive disorder; OCD = obsessive-compulsive disorder; PTSD = posttraumatic stress disorder; SAD = separation anxiety disorder.
For this example, we consider a test of an autonomic stress-reactivity theory of social phobia. The outcome of interest is skin-conductance level during an impromptu speech delivered to a group of impassive confederates. The researchers’ theory—which, like many others in psychopathology research, pertains to one particular categorical disorder—dictates that predictive path a in Figure 3 should eclipse the others: The social phobia diagnosis should be specifically associated with exaggerated autonomic reactivity in this evaluative social context. Alternatively, one could reasonably expect that excessive autonomic reactivity is a more general characteristic of fear disorders (e.g., social phobia, panic disorder, agoraphobia) compared with distress or eating pathology syndromes. In that case, path b should surpass the others in terms of variance explained. Finally, given evidence linking the full complement of anxiety and depressive disorders to stress responsivity, it is possible that reactivity is best captured at the spectrum level. In this last scenario, path c should predominate.
This heuristic illustrates that examining the validity of any DSM diagnosis in isolation—a conventional research strategy—is unnecessarily limiting. A zero-order association between a DSM diagnosis and some outcome could reflect one (or more) qualitatively distinct pathways (in our example, paths a, b, or c in Fig. 3). Hierarchical frameworks such as HiTOP provide a ready means of quantitatively comparing these alternatives. If, in our example, the effect for path a is comparatively small, the research team will know to revise the autonomic arousal theory of social phobia to encompass fear-based or internalizing disorders more generally.
We supplement this case study with a real-world example of theory building driven by HiTOP. The stress-generation theory posits that individuals with DSM-diagnosed major depressive disorder encounter more stressful life events—including ones they have had a role in creating (e.g., romantic relationship dissolution, school expulsion)—than nondepressed counterparts (Hammen, 1991). Indeed, there is evidence that depression prospectively predicts stress exposure. However, more recent work suggests that this effect is not specific to depression. In fact, stress generation appears to be a general feature of the internalizing disorders and dispositional negativity (Liu & Alloy, 2010). Research from Conway, Hammen, and Brennan (2012), who demonstrated that the internalizing spectrum, externalizing spectrum, and major depressive disorder all contributed to the prediction of future stress exposure when considered simultaneously, is consistent with this hypothesis (see Fig. 3; Conway et al., 2012). Note that panic disorder had an inverse effect on stress occurrence after adjusting for the transdiagnostic dimensions. The authors labeled this novel association a “stress-inhibition” effect.
These findings prompted a reformulation of stress-generation theory. First, stress-generation processes are now hypothesized to operate across a range of internalizing and externalizing syndromes, not just major depressive disorder. Second, the HiTOP-consistent analysis pointed to a role for depression-specific pathology in predicting stressful events above and beyond the effects of the internalizing spectrum (i.e., incremental validity). Theorists can use that result to consider the specific portions of major depressive disorder that increase the likelihood of encountering significant stressors. Third, this work highlights the need to understand more fully the stress-inhibiting consequences of panic symptoms, a signal that was not detectable when analyzing DSM diagnoses only.
Up to this point, we have considered how a hierarchical approach—that is, comparing pathways to and from dimensions at different levels of HiTOP—can advance our understanding of psychopathology. Although this approach has been the most common application of HiTOP, it is not the only one. Some researchers have used HiTOP to dissect DSM diagnoses into components and compare their criterion validity (e.g., Simms, Grös, Watson, & O’Hara, 2008; Fig. 2b). For example, panic disorder could be decomposed into physiological (e.g., tachycardia, choking sensations) and psychological (e.g., thoughts of dying or going crazy) symptoms. The predictive validity of these two symptom domains could then be compared in relation to a clinical outcome of interest (e.g., emergency-room visits). Other researchers have evaluated the joint predictive power of sets of HiTOP dimensions above and beyond the corresponding DSM–5 diagnosis (see Waszczuk, Kotov, Ruggero, Gamez, & Watson, 2017; Waszczuk, Zimmerman, et al., 2017). This approach explicitly compares the explanatory potential of dimensional versus categorical approaches to psychopathology (Fig. 2c).
Investigators are beginning to use these research strategies to reevaluate existing theories and findings through a HiTOP lens. In the sections that follow, we describe studies that have approached etiological and clinical outcome research from a HiTOP perspective as a way of selectively illustrating its utility.
Etiological Research From a HiTOP Perspective
Quantitative and molecular genetics
Twin studies find that HiTOP dimensions often are underpinned by distinct genetic liability factors, suggesting that the phenotypic and genetic structures of psychopathology may be closely aligned (e.g., Lahey, Krueger, Rathouz, Waldman, & Zald, 2017; Røysamb et al., 2011). For example, twin research has documented an overarching genetic liability factor that resembles a general factor of psychopathology (Pettersson, Larsson, & Lichtenstein, 2016). This general factor (see the top level of Fig. 1) was first described in phenotypic analyses (Lahey et al., 2012) and later was termed the “p factor” as a counterpart to the g factor in the intelligence literature (Caspi et al., 2014; Caspi & Moffitt, 2018). Consistent with the broad intercorrelations among higher order spectra in psychometric studies, there is growing evidence that common genetic vulnerabilities underlie a general (i.e., transdiagnostic) risk for psychopathology (Selzam, Coleman, Moffitt, Caspi, & Plomin, 2018; Waszczuk, 2018).
At a lower level of the hierarchy, genetic influences operating at the spectrum level have also been identified. For example, anxiety and depressive disorders seem to substantially share a common genetic diathesis, whereas antisocial behavior and substance-use conditions share a distinct substrate (Kendler & Myers, 2014). There is also a consistent but underdeveloped line of twin research that provides biometric support for the genetic coherence of the thought disorder and detachment spectra (Livesley, Jang, & Vernon, 1998; Tarbox & Pogue-Geile, 2011). Further attesting to the hierarchical structure of genetic risk, distinct genetic influences have been identified for the distress and fear subfactors of the internalizing spectrum (Waszczuk, Zavos, Gregory, & Eley, 2014). Finally, twin research shows that narrow psychiatric syndromes—and even certain symptom components within them—might possess unique genetic underpinnings alongside the genetic vulnerability shared with other psychiatric conditions more broadly (e.g., Kendler, Aggen, & Neale, 2013; Rosenström et al., 2017). Overall, although these specific genetic factors are often comparatively small, they provide etiological support for a hierarchical conceptualization of psychopathology. A key challenge for future researchers will be to evaluate more comprehensive versions of the HiTOP model in adequately powered, genetically informative samples (e.g., twin, genome-wide association studies, or GWASs).
Emerging cross-disorder molecular genetic studies also suggest that genetic influences operate across diagnostic boundaries (Smoller et al., 2018). For example, a recent meta-analysis of GWASs of DSM-diagnosed generalized anxiety disorder, panic, agoraphobia, social anxiety, and specific phobia identified common variants associated with a higher order anxiety factor, consistent with the HiTOP fear subfactor (Otowa et al., 2016). Other work reveals moderate (38%) single-nucleotide polymorphism (SNP)-based heritability of the p factor, indicating that common SNPs are associated with a general psychopathology factor in childhood (Neumann et al., 2016). Beyond these broader spectra, several molecular genetic studies have focused on constructs at the subordinate level of the HiTOP hierarchy, partly to reduce phenotypic heterogeneity and amplify genetic signals. For example, one GWAS investigated a narrowly defined phenotype of mood instability, which led to a discovery of four new genetic variants implicated in mood disorders (Ward et al., 2017). Together, these emerging results suggest that it will be possible to identify specific genetic variants at different levels of the HiTOP hierarchy, with some influencing nonspecific psychopathology risk and others conferring risk for individual spectra, subfactors, or even symptoms (e.g., anhedonia). In contrast, traditional case-control designs and even studies focused on pairs of disorders are incapable of untangling such hierarchical effects. In short, HiTOP promises to provide a more effective framework for discovering the genetic underpinnings of mental illness, although further empirical evidence and replications of any specific molecular genetic findings are, of course, needed.
Neurobiology
Paralleling the genetics literature, growing evidence shows that many measures of brain structure and function do not conform to the boundaries implied by traditional DSM/ICD diagnoses. There are no clear-cut depression or schizophrenia “centers” in the brain (e.g., Sprooten et al., 2017). Instead, associations between the brain and mental illness often show one-to-many or many-to-many relations (i.e., multifinality; Zald & Lahey, 2017). Heightened amygdala reactivity, for example, has been shown to confer risk for the future emergence of mood and anxiety symptoms, posttraumatic distress, and alcohol abuse (e.g., McLaughlin et al., 2014; Swartz, Knodt, Radtke, & Hariri, 2015). The internalizing and externalizing spectra are both associated with altered maturation of subcortical structures in late childhood (Muetzel et al., 2018). In some cases, these relations have been shown to reflect specific symptoms that cut across the categorical diagnoses outlined in the DSM. For instance, anhedonia is a central feature of both mood and thought disorders in the DSM, and dimensional measures of anhedonia have been linked to aberrant ventral striatum function (i.e., activity and functional connectivity) in several large-scale, mixed-diagnosis studies (Sharma et al., 2017; Stringaris et al., 2015).
Evidence of one-to-many relations is not limited to the neuroimaging literature. The P3 event-related potential, for example, has been linked to a variety of externalizing disorders and to dimensional measures of externalizing (Iacono, Malone, & McGue, 2003; Patrick et al., 2006). Cross-sectional and prospective studies have linked the error-related negativity to a variety of DSM-diagnosed anxiety disorders, to the development of internalizing symptoms, and to dimensional measures of anxiety (Cavanagh & Shackman, 2015; Meyer, 2017).
Although the neural bases of the p factor remain far from clear, recent neuroimaging research has begun to reveal some neural systems with conspicuously similar (i.e., transdiagnostic) features. In a recent meta-analysis, McTeague and colleagues (2017) identified a pattern of aberrant activation shared by the major mental disorders. When performing standard cognitive control tasks (e.g., go/no-go, Stroop), patients diagnosed with DSM-diagnosed anxiety disorders, bipolar disorder, depression, schizophrenia, or substance abuse all exhibited reduced activation in parts of the so-called salience network, including regions of the cingulate, insular, and prefrontal cortices. Applying a similar approach to voxel-by-voxel measures of brain structure, Goodkind and colleagues (2015) identified a neighboring set of regions in the midcingulate and insular cortices showing a common pattern of cortical atrophy across patients diagnosed with a range of DSM-diagnosed disorders (anxiety, bipolar disorder, depression, obsessive-compulsive, and schizophrenia). Few disorder-specific effects were detected in either of these large meta-analyses.
More recent imaging research has begun to adopt the kinds of analytic tools widely used in psychometric and genetic studies of psychopathology, enabling a direct comparison of different levels of HiTOP (see Fig. 2a) and new clues about the neural bases of the p factor. Using data acquired from the Philadelphia Neurodevelopmental Cohort, Shanmugan and colleagues (2016) identified the p factor and four nested subdimensions (antisocial behavior, distress, fear, and psychosis; see Fig. 1, subfactor level). Higher levels of the p factor were associated with reduced activation and aberrant multivoxel patterns of activity in the salience network (cingulate and insular cortices) during the performance of the n-back task, a widely used measure of working memory capacity and executive function. After accounting for the phenotypic variance explained by the p factor, the antisocial, distress, and psychosis dimensions were each associated with additional subfactor-specific alterations in task-evoked activation (e.g., psychosis was uniquely associated with hypoactivation of the dorsolateral prefrontal cortex). Using the same sample, Kaczkurkin et al. (2018) found an analogous pattern of results with measures of resting activity. These observations converge with the meta-analytic results discussed above (Goodkind et al., 2015; McTeague et al., 2017) and reinforce the idea that a circuit centered on the cingulate cortex underlies a range of common psychiatric symptoms and syndromes. Still, it is implausible that this circuit will completely explain a phenotype as broad as the p factor. Indeed, other correlates are rapidly emerging (Romer et al., 2018; Sato et al., 2016; Snyder, Hankin, Sandman, Head, & Davis, 2017).
Collectively, these results highlight the value of the HiTOP framework for organizing neuroscience and other kinds of biological research. Adopting a hierarchical, dimensional approach makes it possible to dissect brain structure and function quantitatively, facilitating the discovery of features that are common to many or all of the common mental disorders, those that are particular to specific spectra and syndromes, and those that underlie key transdiagnostic symptoms—a level of insight not afforded by RDoC or traditional diagnosis-centered nosologies.
Environmental risk
Stressful environments are intimately intertwined with risk for mental illness. For decades, researchers have proposed theories about the connections between stressors and specific diagnoses (e.g., loss, DSM-diagnosed major depressive disorder). Yet it is clear that most stressors are nonspecific and confer increased risk for diverse psychopathologies (McLaughlin, 2016). Socioeconomic adversity, discrimination, harsh parenting, bullying, and trauma all increase the likelihood of developing psychiatric illness (Caspi & Moffitt, 2018; Lehavot & Simoni, 2011; Wiggins, Mitchell, Hyde, & Monk, 2015). This lack of specificity raises the possibility that many stressors act on illness processes that are shared across entire subfactors (e.g., distress, antisocial behavior), spectra (e.g., internalizing), or even superspectra. Investigators can use HiTOP to identify the level or levels at which stressful environments exert their effects.
Childhood maltreatment represents an instructive case because it has potent and nonspecific relations with future psychopathology (Green et al., 2010). Several studies have used a hierarchical approach to assess the relative importance of higher order (i.e., transdiagnostic) versus diagnosis-specific pathways from early maltreatment to mental disorders in adulthood. Leveraging interview-based diagnoses and retrospective reports of childhood maltreatment collected as part of the National Epidemiological Survey on Alcohol and Related Conditions (NESARC; n > 34,000), Keyes et al. (2012) observed strong relations between childhood maltreatment and the internalizing and externalizing spectra (see path c in Fig. 3) but not specific diagnoses (see path a in Fig. 3). In other words, the marked impact of childhood maltreatment on adult psychopathology was fully mediated by the transdiagnostic spectra. Similar findings emerged in a community sample of more than 2,000 youth enriched for exposure to maltreatment (Vachon, Krueger, Rogosch, & Cicchetti, 2015; see also Conway, Raposa, Hammen, & Brennan, 2018; Lahey et al., 2012; Meyers et al., 2015; Sunderland et al., 2016).
The HiTOP framework has also been used to understand the influence of chronic stressors in adulthood (Snyder, Young, & Hankin, 2017). For instance, Rodriguez-Seijas, Stohl, Hasin, and Eaton (2015) recently showed that racial discrimination has strong associations with the internalizing and externalizing spectra (see path c in Fig. 3) in a nationally representative sample of more than 5,000 African Americans. For most disorders, the pathway from discrimination to particular DSM diagnoses (e.g., attention-deficit/hyperactivity disorder, social phobia) was largely explained by its impact on higher-order spectra. In a few cases, discrimination was directly associated with specific diagnoses (e.g., alcohol use disorder). These effects make it clear that multiple pathways from environmental adversity to psychopathology are possible—some centered on transdiagnostic spectra and others on more specific syndromes—with important implications for efforts to develop more effective and efficient strategies for preventing and treating mental illness.
Clinical Outcome Research From a HiTOP Perspective
Like etiological factors, clinical outcomes often reflect a mixture of specific and transdiagnostic effects and, as a result, are better aligned with HiTOP than traditional diagnostic systems such as DSM or ICD.
Prognosis
Clinicians and researchers often seek to forecast the onset or recurrence of psychological problems on the basis of diagnostic and symptom data (e.g., Morey et al., 2012). The HiTOP system has the potential to streamline this prognostic decision making. For instance, using data gleaned from the World Mental Health Surveys (N > 20,000), Kessler, Petukhova, and Zaslavsky (2011) examined the prognostic value of 18 disorders from the fourth edition of the DSM (DSM–IV; American Psychiatric Association, 1994) in predicting new onsets of subsequent diagnoses. They found that the vast majority of the development of categorical diagnoses arising at later time points was attributable to variation on internalizing and externalizing dimensions earlier in life (for similar results, see Eaton et al., 2013). This result suggests that higher-order dimensions can often provide a more efficient means of predicting the natural course of mental illness (see also Kotov, Perlman, Gámez, & Watson, 2015; Olino et al., 2018).
Suicide
The HiTOP framework has also proven useful for optimizing suicide prediction. Tools for forecasting suicide are often based on the presence or absence of specific diagnoses (e.g., bipolar disorder, borderline personality disorder). However, recent large-scale studies have consistently shown that the predictive power of DSM diagnoses pales in comparison to that of higher order dimensions. For instance, in the NESARC sample described earlier, the distress subfactor (Fig. 1) explained approximately 34% of the variance in suicide attempt history. In contrast, the top-performing DSM diagnoses accounted for only approximately 1% (Eaton et al., 2013; see also Naragon-Gainey & Watson, 2011; Sunderland & Slade, 2015). These kinds of observations indicate that suicide risk is better conceptualized at the level of spectra, not syndromes, contrary to standard research and clinical practices.
Impairment
Psychosocial impairment is typically a core feature of contemporary definitions of psychopathology, and it often persists long after acute symptoms have abated. Understanding impairment is important for prioritizing scarce resources. But is impairment better explained and, more importantly, predicted by DSM/ICD diagnoses or transdiagnostic dimensions? Using data from the Collaborative Longitudinal Personality Disorders Study (N = 668), Morey et al. (2012) found that maladaptive personality traits were twice as effective at predicting patients’ functional impairment across a decade-long follow-up compared with traditional diagnoses (see Fig. 2c). Likewise, Forbush et al. (2017) demonstrated that higher order dimensions explained 68% of the variance in impairment in a sample of patients with an eating disorder. In contrast, anxiety, depression, and eating disorder diagnoses collectively explained only 11%. In the area of psychosis, van Os and colleagues (1999) compared the predictive power of five dimensions versus eight DSM diagnoses in a large longitudinal sample across 20 distinct psychosocial outcomes (e.g., disability, unemployment, cognitive impairment, suicide). For every outcome with a clear difference in predictive validity, dimensions outperformed diagnoses.
Waszczuk, Kotov, et al. (2017) reported similar results in two samples evaluated with the Interview for Mood and Anxiety Symptoms (IMAS), which assesses the lower order components of emotional pathology (e.g., lassitude, obsessions). These dimensions explained nearly two times more variance in functional impairment than did DSM diagnoses. Moreover, DSM diagnoses did not show any incremental predictive power over the dimensional scores—a particularly striking result given that impairment is part of the DSM diagnostic criteria but not directly captured by IMAS scores (see Fig. 2c). In sum, this line of research suggests that transdiagnostic dimensions of the kinds embodied in HiTOP have superior prognostic value—both concurrently and prospectively—for psychosocial impairment (see also Jonas & Markon, 2013; Markon, 2010; South, Krueger, & Iacono, 2011).
Summary
Theoretical models of the causes and consequences of psychiatric problems have traditionally been framed around diagnoses. New research highlights the importance of extending this focus to encompass transdiagnostic dimensions, including both narrowly defined symptoms and traits (e.g., obsessions) and broader clusters of psychological conditions (e.g., internalizing spectrum). In contrast to other classification systems (e.g., DSM) and unlike RDoC, HiTOP provides a convenient framework for directly testing the relative importance of symptom components, syndromes, spectra, and superspectra (e.g., p factor) for the emergence and treatment of psychopathology (Fig. 1). The evidence reviewed here suggests that in many cases mental illness is better conceptualized in terms of transdiagnostic dimensions.
HiTOP: A Practical Guide
A primary objective of this review is to provide investigators with some practical recommendations for incorporating HiTOP into their research. Here we outline design, assessment, and analytic strategies that follow from the theory and available data underpinning HiTOP.
Design
The lion’s share of clinical research has historically been conducted using traditional case-control designs, in which participants meeting criteria for a particular diagnosis are compared with a group free of that disorder or perhaps any mental illness. This approach is generally inconsistent with a dimensional perspective on psychopathology. There is compelling evidence that mental illness is continuously distributed in the population, without the gaps or “zones of discontinuity” expected of categorical illnesses (Krueger et al., 2018; for a different perspective, see Borsboom et al., 2016). These observations indicate that artificially separating case subjects from non-case subjects leads to an appreciable loss of information (Markon et al., 2011), consistent with more general recommendations to avoid post hoc dichotomization (e.g., median splits) of continuous constructs (Preacher, Rucker, MacCallum, & Nicewander, 2005).
The case-control strategy also ignores the issue of diagnostic comorbidity. The ubiquitous co-occurrence of disorders makes it extremely difficult to establish discriminant validity for most categorical syndromes. In practical terms, any distinction between, say, patients with panic disorder and healthy controls in a particular study may not be a unique characteristic of panic disorder. It could instead reflect the influence of a higher order dimension, such as the HiTOP fear subfactor, that permeates multiple diagnoses (e.g., panic disorder, agoraphobia, social anxiety disorder, and specific phobia). By disregarding the symptom overlap among clusters of related conditions, the case-control design is bound to underestimate the breadth of psychopathology associated with a given clinical outcome.
From an efficiency standpoint, recruiting on the basis of particular diagnoses creates a fragmented scientific record. The traditional approach of studying one disorder in relation to one outcome has spawned many insular journals, societies, and scholarly subcommunities (“silos”). This convention belies the commonalities among disorders and has led to piecemeal progress. For example, the initial phases of psychiatric genetic research were oriented around specific diagnoses. There were separate studies focused on the molecular genetic origins of obsessive-compulsive disorder, generalized anxiety disorder, posttraumatic stress disorder, and so on. Analogously, the research on childhood maltreatment in relation to various individual syndromes is voluminous. These lines of research have consumed considerable resources but have revealed few (if any) replicable one-to-one associations between risks and disorders. A more parsimonious and efficient approach is to recruit participants on the basis of a particular psychopathological dimension (e.g., antisocial behavior, excitement seeking), either sampling to ensure adequate representation of all ranges of this dimension or recruiting at random from the population of interest (e.g., community, students, outpatients) to provide a representative sample. 3 Then, as was the case for our fictional study of autonomic disruptions in social phobia, the effects of both general and more specific dimensions of psychopathology can be compared empirically. Thinking broadly, such a strategy promises to facilitate more cumulative, rapid progress in developing etiological models for a wide range of psychological conditions.
It is worth noting that some of these recommendations can be addressed after the fact. Many of the analyses that we have reviewed in earlier sections were carried out using data sets that were not assembled with HiTOP in mind. However, these projects have generally included a thorough assessment of psychopathology outcomes, which can serve as building blocks for quantitative investigations of symptom or syndrome co-occurrence via factor analysis or related techniques. For example, there have been several studies of the correlates (e.g., demographic features, environmental stressors) of higher order dimensions versus syndromes in epidemiological studies, such as the National Comorbidity Survey Replication and NESARC (e.g., Eaton et al., 2013; Keyes et al., 2012; Slade, 2007). Investigators have also taken advantage of comprehensive psychopathology assessments in longitudinal cohort studies—such as the Dunedin Multidisciplinary Health and Development Study and the Pittsburgh Girls Study—to examine the temporal course and longitudinal correlates of HiTOP dimensions (e.g., Krueger, Caspi, Moffitt, & Silva, 1998; Lahey et al., 2015; McElroy et al., 2018). These cohort studies are particularly valuable for theory building because they tend to have rich assessments of validators (etiological factors, clinical outcomes; e.g., Caspi et al., 2014).
Studies do not need to have especially large samples or wide-ranging assessment batteries (e.g., “big data”) to take advantage of the HiTOP framework. Often, dimensional measures of psychopathology can be integrated into typical (in terms of resources and sample size) study designs. Take, for example, the fictional study of autonomic reactivity described earlier. We described a scenario in which diagnoses were the basic units of mental illness and were used to infer standing on the next higher level dimensions (i.e., the subfactor and spectrum levels). However, analogous tests could be carried out if researchers administered a self-report questionnaire assessing both the broad and specific features of the internalizing domain, such as the Inventory of Depression and Anxiety Symptoms (Watson et al., 2012). For instance, the effect of lower order symptom components (e.g., lassitude, obsessions; see Fig. 3 path c) on autonomic reactivity could be compared with the effect of a higher level (e.g., spectrum) dimension (e.g., dysphoria; see Fig. 3 path a). We expect that, in most research situations, moderately sized samples would suffice to precisely gauge these effects. More generally, we expect that empirically derived dimensional measures of mental illness can be integrated effectively into most standard research designs. Along those lines, we plan to publish a series of “worked examples” on the HiTOP consortium website that illustrate the methodological and data-analytic steps—including relevant materials, data, and code—in typical studies that apply the HiTOP framework.
Assessment
Although assessing multiple syndromic or symptom constructs in the same study represents an improvement over “one disorder, one outcome” designs, this approach has limitations. DSM/ICD diagnoses and many symptom measures are notoriously heterogeneous, meaning they are composed of multiple lower order dimensions of psychopathology. For instance, many common depressive symptom scales include not only cognitive and vegetative symptoms, which arguably have separate etiologies and correlates, but also anxiety symptoms (e.g., Fried, 2017). Thus, a more optimal approach is to forego traditional diagnostic constructs in favor of assessing lower order dimensions of pathology (e.g., the symptom component level of Fig. 1). This strategy maximizes the precision of the dimensions that can be examined, improving our ability to “carve nature at its joints.”
Consequently, we recommend using assessment instruments that measure both higher and lower order dimensions of psychopathology. A number of such measures are reviewed in Kotov et al. (2017). No omnibus inventory yet exists that covers the entirety of the HiTOP framework, although our consortium is currently developing one. Instead, many existing measures assess specific aspects (e.g., component/trait, syndrome, and subfactor levels) of the HiTOP model (see https://psychology.unt.edu/hitop). Researchers can use these measures to perform a complete assessment of one spectrum (e.g., antagonistic externalizing) or several (e.g., antagonistic externalizing, disinhibited externalizing, thought disorder). The list of measures is expected to continue evolving, and researchers can refer to the HiTOP website to access the latest inventories, including a forthcoming comprehensive measure of the full HiTOP model as currently constituted. Most facets of the HiTOP structure can currently be assessed economically with questionnaire measures that are available in self- and informant-report versions. Structured and semistructured interview approaches can also be used, assuming they allow for dimensional scoring. Of course, for such assessments to be compatible with HiTOP, they may need to be modified to eliminate “skip rules” (e.g., if neither significant depressed mood or anhedonia is endorsed, some interview procedures automatically exit the major depression section) and hierarchical decision rules (e.g., DSM–IV stipulated that generalized anxiety disorder could not be diagnosed if it presented only in the context of a co-occurring depressive disorder) to collect all symptom data. Overriding these rules permits an assessment of the full clinical picture.
Analysis
There are several different ways for investigators to test the association of dimensional constructs with outcomes of interest. Expertise with latent variable modeling is not a prerequisite. Many popular measurement tools (e.g., the Child Behavior Checklist; Achenbach, 1991) include a combination of broad (e.g., externalizing) and narrow (e.g., aggression) dimensions. Connections of these scales with background characteristics or clinical outcomes could then be contrasted using standard regression approaches.
In the case of large samples, it is possible to use latent variable modeling to empirically extract the relevant dimensions. Exploratory factor analysis (EFA) is an atheoretical approach to determining the appropriate number and nature of latent dimensions undergirding psychological problems. In many common statistical packages, it is possible to perform an EFA and then extract factor scores—values that represent a person’s standing on a latent dimension—that can be used as variables in standard regression or analysis of variance procedures (although this procedure has some drawbacks; e.g., Devlieger, Mayer, & Rosseel, 2016). Confirmatory factor analysis, a hypothesis-driven approach in which the researcher specifies the relations of symptom or diagnostic constructs to latent dimensions, is another common approach. Finally, using a series of factor analyses to explicate a hierarchical factor structure by proceeding from higher (broader) to lower (narrower) levels of specificity (termed the “bass-ackwards” method) can be useful in extracting HiTOP dimensions from symptom- or diagnostic-level data (see Goldberg, 2006).
Future Challenges
There are clear and compelling scientific reasons to adopt HiTOP-style approaches to understanding psychopathology, but it is equally clear that additional work will be required to refine this framework and determine its optimal role in mental illness research. Uncertainties regarding several architectural elements of HiTOP remain. Additional research is needed to incorporate psychiatric problems not currently included in HiTOP (e.g., autism spectrum disorder and other neurodevelopmental conditions) and to validate the placement of domains of psychopathology that have received limited attention in structural studies (e.g., lower order dimensions of mania as components of internalizing versus thought disorder). At the spectrum level, data are particularly limited for HiTOP’s somatoform and detachment dimensions. Further, continued research is needed on possible latent taxa, as opposed to dimensions, involved in mental illness. Taxometric research has favored dimensions over categories for every HiTOP construct that has been examined to date; however, in theory, zones of discontinuity could emerge and would therefore merit inclusion in the HiTOP model. For example, deviation on multiple dimensions may yield discontinuous cutoffs (cf. Kim & Eaton, 2017). In short, the HiTOP framework is a work in progress, and researchers are encouraged to consult the consortium website for updates or to apply for membership in the consortium and contribute to improving the model.
Moving forward, we also need to carefully examine the use and interpretation of factor analysis with respect to HiTOP. There are questions about whether the theoretical constructs outlined in HiTOP satisfy assumptions of the common factor model (e.g., van Bork, Epskamp, Rhemtulla, Borsboom, & van der Maas, 2017; see also Borsboom, Mellenbergh, & Van Heerden, 2003). For instance, are the factors (e.g., fear, detachment) naturally occurring phenomena that directly cause variation in their indicators (e.g., panic, social phobia)? Or are the HiTOP factors simply useful—and, to some extent, artificial—summaries of symptom covariation (see Jonas & Markon, 2016)? We note that although factor analysis has proved to be a useful tool in this area of research, HiTOP outcomes need not be represented by latent variables; it is possible to operationalize them directly using questionnaire and interview measures of the types mentioned earlier, although every specific measure has strengths, weakness, and a particular range of applicability, so it will be important not to equate measures with constructs.
Additional work will also be required to better understand the degree to which HiTOP is compatible with network models and the RDoC framework (e.g., Clark et al., 2017; Fried & Cramer, 2017). Network models conventionally assume that psychopathology does not reflect latent traits; psychological syndromes instead arise from a chain reaction of symptoms activating one another (e.g., Cramer, Waldorp, van der Maas, & Borsboom, 2010). A common example is that a constellation of depression symptoms might coalesce not because of the guiding influence of an unobserved, unitary depression dimension but rather because of a snowballing sequence of symptom development (e.g., insomnia → fatigue, fatigue → concentration problems). The purpose of the network model is to discern these hypothesized causal pathways among symptoms. In contrast, HiTOP aims to identify replicable clusters of symptoms that have shared risk factors and outcomes. Both perspectives can be useful for understanding the nature of psychopathology and are not necessarily mutually exclusive (e.g., Fried & Cramer, 2017).
Like HiTOP, the National Institute of Mental Health’s RDoC initiative deconstructs psychopathology into more basic units that cut across traditional diagnoses (Table 1). However, its primary focus is on fundamental biobehavioral processes (e.g., reward, anxiety), especially those conserved across species, that are disrupted in mental illness (Clark et al., 2017). This approach has gained traction in biological psychology and psychiatry as an alternative to DSM diagnoses, but its utility for other areas of research may be more limited because RDoC does not specifically model the observable signs and symptoms of mental illness that are the subject of most theories of psychopathology. That is, it does not include detailed representations of clinical phenotypes (e.g., aggression, narcissism, emotional lability) that are common targets in research on organizations, close relationships, social groups, aging, psychotherapy, and many other fields wherein the prevailing theoretical models have little (or no) biological emphasis.
Prominent Mental Illness Frameworks
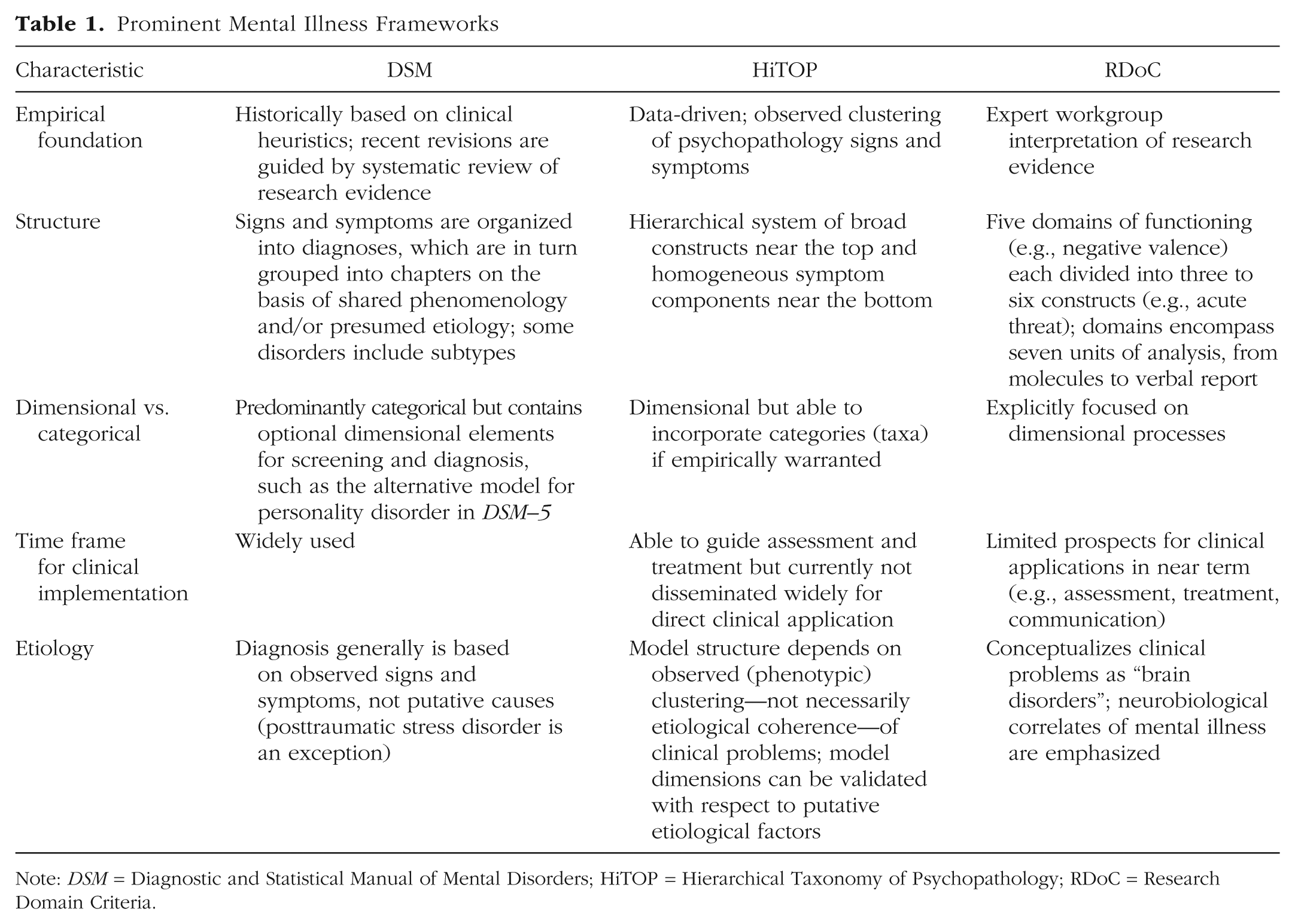
Note: DSM = Diagnostic and Statistical Manual of Mental Disorders; HiTOP = Hierarchical Taxonomy of Psychopathology; RDoC = Research Domain Criteria.
A complementary nosological framework is needed to link the basic science discoveries spurred by RDoC—and similar National Institutes of Health initiatives, such as the National Institute of Alcohol Abuse and Alcoholism’s Addictions Neuroclinical Assessment and the National Institute of Drug Abuse’s Phenotyping Assessments Battery—to the signs and symptoms that lead people to seek treatment. HiTOP, which provides a clear and comprehensive system of clinical phenotypes, offers such a bridge. Research that integrates these dimensional frameworks has the potential to make RDoC clinically relevant and to provide important insights into the biological bases of the dimensions embodied in the HiTOP framework.
Whereas RDoC proponents acknowledge that it is unlikely to have much applied clinical value in the near term, HiTOP is poised for clinical implementation. HiTOP encapsulates clinical problems that practitioners are familiar with and routinely encounter. Existing questionnaire and interview measures that capture HiTOP dimensions can be administered to patients or other informants (Kotov et al., 2017). Normative data are available for many measures and will continue to accrue (e.g., Stasik-O’Brien et al., 2018). Clinicians can use dimensional scores to compare patients’ scores to clinical cutoffs or other norms to inform decisions about prognosis and treatment (see Ruggero, 2018). Moreover, dimensional measures are more useful for monitoring treatment progress than are categorical diagnoses because they tend to be more sensitive to change while also yielding more reliable change indices (e.g., Kraemer, Noda, & O’Hara, 2004). One of the most important challenges for the future will be to gather appropriate normative data for more instruments and refine their use in clinical assessment and treatment planning.
The hierarchical structure of HiTOP implies that targeting higher order dimensions such as the internalizing spectrum may cause therapeutic effects to percolate across multiple DSM conditions, augmenting the efficiency of psychological treatment. For example, the Unified Protocol for Transdiagnostic Treatment of Emotional Disorders (Barlow, Sauer-Zavala, Carl, Bullis, & Ellard, 2014) was developed to act on common temperamental processes theorized to lie at the core of internalizing problems. Rather than using separate protocols to treat individual diagnoses, such as major depression and generalized anxiety disorder, the Unified Protocol uses cognitive-behavioral strategies to reduce negative emotionality and increase positive emotionality, traits thought to maintain anxiety and depression over time, and emerging evidence shows that such transdiagnostic psychotherapies can be as effective as traditional (i.e., diagnosis-specific) treatments (Barlow, Farchione, Bullis, Gallagher, & Cassiello-Robbins, 2017). Practitioners can apply the Unified Protocol to a diverse set of anxiety and depressive conditions, streamlining the training process and minimizing barriers to dissemination, compared with standard training models that involve learning a separate treatment framework for each disorder (Steele et al., 2018). The policy of using one psychological treatment for various conditions is analogous to standard prescription practices for psychiatric medications, which often work across—and in many cases have regulatory approval for treatment of—multiple diagnoses.
The most important avenue for future empirical work, in our view, is continued validation research into the utility (for research and theory building) of the dimensions that make up the HiTOP model. In particular, validation studies to date have been mostly limited to the spectrum level (e.g., correlates of internalizing, disinhibited externalizing), and criterion-validity research is needed at other levels of the hierarchy. In addition, existing research has largely relied on snapshots of symptoms and syndromes without modeling illness course. Longitudinal studies that are designed to examine the correlates and structure of HiTOP dimensions in diverse samples across the life span are a pressing priority (cf. Lahey et al., 2015; Wright, Hopwood, Skodol, & Morey, 2016), as is research on the short-term dynamics of psychopathology symptoms (e.g., Wright & Simms, 2016). Although research has supported the invariance of the internalizing and externalizing spectra across gender, developmental stages, and various racial, ethnic, and cultural groups (see Rodriguez-Seijas et al., 2015), investigating other HiTOP dimensions with regard to aging, culture, context, and so forth will be important.
Conclusion
There is compelling evidence that the nature of psychopathology is dimensional and hierarchical, with many studies indicating that genes, neurobiology, and clinical outcomes align with this new conceptualization. We recommend a shift in mental-health research practices to match the HiTOP model. This emerging system has the potential to (a) expand existing theories and generate new hypotheses, (b) unify unnecessarily fragmented empirical studies, (c) increase the utility of classification systems for both basic and applied research, and (d) establish novel phenotypes that explain the etiology of psychological problems and serve as more efficient assessment and treatment targets. Although many important challenges remain, HiTOP has the potential to transform research practices for the better and accelerate theory development across diverse areas of psychological science.
Footnotes
Acknowledgements
Action Editor
June Gruber served as action editor and interim editor-in-chief for this article.
Declaration of Conflicting Interests
The author(s) declared that there were no conflicts of interest with respect to the authorship or the publication of this article.