
Abstract
Hispanics have a lower burden of heart disease than would be predicted from their risk factors. Explanations for this phenomenon, the Hispanic paradox, focus on specific characteristics of the culture that affect stress appraisal and accumulation, including social connections. Features of culture evolve in the context of language, which influences the way emotions are appraised and expressed. The Spanish language, a unifying component defining Hispanic cultures, has unique features that may promote emotional expression, expand the emotional concepts implicated in the construction of emotion, and influence the appraisal of stress. Under chronic stress conditions, sustained responses can become maladaptive, leading to disease. Features of the Spanish language allow its speakers a wide range of emotion schemas by virtue of its emotion lexicon, the ability to easily minimize or exaggerate expressions, and ease in considering hypothetical situations with the use of the subjunctive. The hypothesis here proposes that the Spanish language is directly and indirectly (via culture) responsible for mitigating some of the effects of acute stress responses in Hispanics and, therefore, limits stress accumulation and is partly responsible for the Hispanic paradox.
The Hispanic paradox refers to the observation, first made more than 30 years ago (Markides & Coreil, 1986), that Hispanics/Latinos in the United States have lower mortality rates from cardiovascular disease (CVD) than their non-Hispanic White counterparts despite having a worse risk-factor profile. CVD refers to conditions of the heart and/or circulatory system and include but are not limited to coronary heart disease (CHD) and stroke. CVD has been the leading cause of death in the United States for more than a century (McClellan et al., 2019). Although the paradox has garnered considerable attention (Abraido-Lanza et al., 1999), the factors that explain it remain unclear. In this article, I argue that the Spanish language may be key to unraveling the paradox.
Current mortality data show a clear advantage for Hispanics/Latinos with respect to CVD, as well as more specific conditions under the CVD umbrella (Benjamin et al., 2017). The advantage has been reported to extend to all-cause mortality in Hispanics/Latinos compared with other racial/ethnic groups (Ruiz et al., 2013). Ruiz et al. estimated a weighted average effect size of .825, thus concluding that the mortality odds were 17.5% lower in Hispanics/Latinos relative to other racial/ethnic groups. The Hispanic/Latino advantage has also been observed in morbidity statistics. The American Heart Association reports the prevalence of heart disease for Hispanics/Latinos to be lower relative to non-Hispanic Whites (7.8% vs. 11.1%; Benjamin et al., 2017). Likewise, the prevalence for stroke is lower for Hispanics/Latinos than for non-Hispanic Whites (2.0% vs. 2.2% among men and 2.6% vs. 2.8% among women). Hypertension is also less prevalent in Hispanics/Latinos relative to non-Hispanic Whites (28.9% vs. 34.5% among men and 30.7% vs. 32.3% among women). This Hispanic/Latino CVD advantage is unexpected because obesity and diabetes, which are risk factors for CVD, are more prevalent in Hispanic/Latino men and women than in their non-Hispanic White counterparts (Benjamin et al., 2017). For example, with respect to diabetes, the National Health and Nutrition Examination 2011–2014 age-adjusted data for U.S. adults 20 years or older, the prevalence was 12.8% for Hispanics/Latinos but 7.6% for non-Hispanic Whites (Benjamin et al., 2017). The same pattern was true in obesity among men and women: The prevalence among men was 39.0% for Hispanics/Latinos but 33.6% for non-Hispanic Whites, and the prevalence among women was 45.7% for Hispanics/Latinos but 35.5% for non-Hispanic Whites.
The most comprehensive data on the health of Hispanics/Latinos comes from the Hispanic Community Health Study/Study of Latinos (HCHS/SOL; Sorlie et al., 2010), an epidemiological study of 16,400 Hispanics/Latinos 18 to 74 years old from four urban communities in the United States (Bronx, Chicago, Miami, and San Diego) and six background categories: Central American, Cuban, Dominican, Mexican-American, Puerto Rican, and South American. This study also reports a high prevalence of risk factors and low rates of CHD and stroke in Hispanics/Latinos. The prevalence of self-reported CHD among Hispanic/Latino men and women was 4.2% and 2.4%, respectively; the prevalence of self-reported stroke for Hispanic/Latino men and women was 2.0% and 1.2%, respectively (Daviglus et al., 2012). These estimates are lower than those seen in samples of U.S. non-Hispanic Whites (Benjamin et al., 2017).
I propose that the Spanish language, the greatest source of homogeneity across Hispanics/Latinos, offers clues to understanding the paradox. In support of this hypothesis, I reference disparate fields of study, including epidemiology, linguistics, cultural anthropology, psychology, cognitive neuroscience, and behavioral medicine. As a result, this review is broad but not exhaustive. The goal is to demonstrate the viability of the hypothesis by reviewing key ideas and existing evidence that support the links within and across these fields of study to motivate further work.
What May Explain the Hispanic Paradox?
Although these paradoxical patterns of lower-than-expected CVD as a function of Hispanic ethnicity have been consistently observed in the epidemiology literature, explanations for the paradox remain elusive. The focus has been on intrapersonal and interpersonal resources (Gallo & Matthews, 2003; Gallo et al., 2009; Myers, 2009) in the context of the reserve-capacity model. According to this model, resources such as social support and optimism may help to explain the resilience observed in Hispanics/Latinos in the face of socioeconomic and/or psychosocial stress (Gallo et al., 2009) by virtue of their role as moderators or buffers of stress. Although this model has received some support in explaining health disparities with respect to socioeconomic status in other minority populations such as non-Hispanic Blacks (Chen, 2007), it has received limited attention in Hispanics/Latinos. Because no current hypothesis has documented sufficient explanatory power to explain the paradox, there is a need to identify the specific cultural factors that are likely candidates—hence the language hypothesis presented in this article. Figure 1 displays the model of the proposed pathways linking Hispanic cultural aspects, including language and CVD.
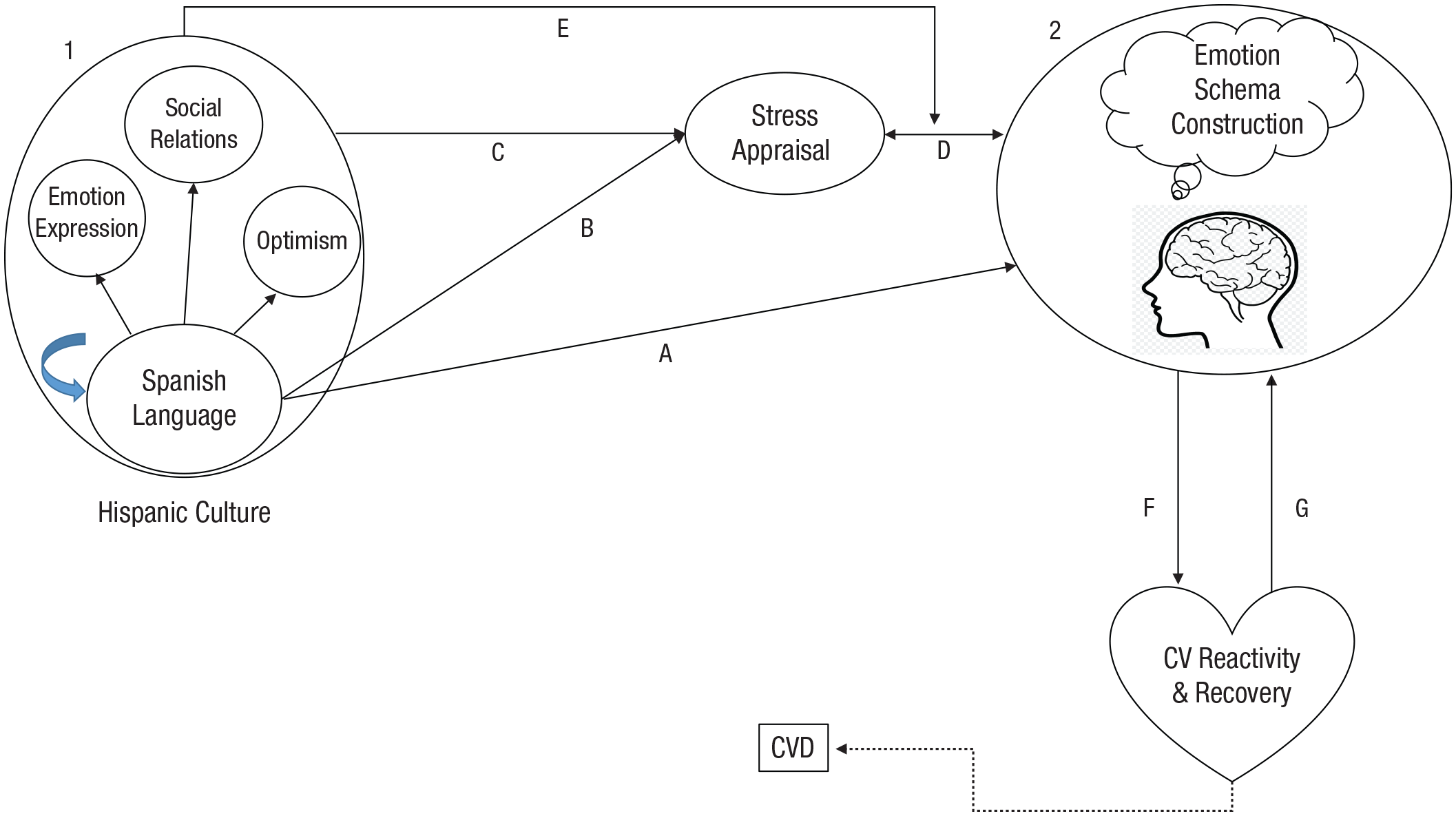
A model of how the Spanish language might explain the Hispanic paradox. In oval 1, language is depicted as a component of culture that influences the expression of emotion, social relations, and positive aspects such as optimism. The curved blue arrow shows culture as influencing language. Features of the Spanish language directly influence the appraisal of stress (path A) and the construction of emotion schemas (path B). In addition to language, other aspects of the Hispanic culture also influence the appraisal of stress (path C) and act to dampen the effects of stress on the emotional responses (path E). Path D shows the bidirectional association between stress appraisal and emotion. In oval 2, the process of emotion construction using schemas. This process results from the appraisal of internal or external stimuli as threatening. Brain systems interact with peripheral physiology in feedback loops (paths F and G) to maintain homeostasis. Cardiovascular responses to a specific stress appraisal can become maladaptive over time potentially leading to cardiovascular disease (CVD).
Hispanic Culture and Language
Despite vast individual and group differences in cultural practices within Hispanic/Latino communities, the Hispanic/Latino culture relative to mainstream U.S. culture has been described as collectivistic and emphasizing family and social interaction (Gallo et al., 2009; Ruiz et al., 2016). These interactions are supported by language, a key aspect of culture. In fact, the Spanish language is the one cultural component consistent across different Hispanic/Latino background groups (Oboler, 1995). Yet in Hispanic/Latino health research, language has received little attention beyond its use as a proxy for acculturation (Marin, 1992). Thus, exploring features of the Spanish language may be useful in understanding why these Hispanic/Latino groups display better-than-expected CVD outcomes.
In one of the few studies that considered language as a factor affecting social connections and health in Hispanics/Latinos, Mulvaney-Day et al. (2007) analyzed individual and community-level social connections in relation to self-reported health. Spanish-language proficiency and the language of thinking were significantly associated with self-rated physical health. Furthermore, the effect of family support on health disappeared once the effect of language was statistically controlled. The authors interpreted their language findings in terms of the role that Spanish-language proficiency may play in maintaining social connections, but an alternative interpretation is that specific features of the Spanish language themselves may be protective independent of those connections.
In another study, Daviglus et al. (2012) examined the prevalence of self-reported CHD and stroke from the HCHS/SOL as a function of whether participants chose to be interviewed in English or Spanish. The prevalence of stroke and CHD were 1.4% and 2.0%, respectively, for those who used English, and 0.8% and 1.3%, respectively, for those who used Spanish. Differences in language preference were interpreted in the context of acculturation rather than language per se but could easily be interpreted in the context of the impact of language type on CVD.
Language, Culture, and Relativity
The idea that language may shape our experiences has a long history. Formulations of the linguistic-relativity hypothesis, also known as the Sapir-Whorf hypothesis (Sapir, 1985; Whorf, 1956), have existed since the 18th century (Lucy, 1992; for review, see Lucy, 1997). The original strong, deterministic version asserted that the structure of a language determines thought. Yet, over time, weaker, more nuanced versions of the hypothesis—asserting that the language spoken merely influences the way people think—became more prominent. Influential early work by Brown and colleagues supported an association between the availability of lexically coded categories in a language and cognitive categorization (Brown & Lenneberg, 1954). This weaker version considers language as directing attention to environmental cues and modulating other cognitive processes, resulting in differential expressions of certain constructs observed among the speakers of different languages.
Although the deterministic version of the hypothesis is no longer considered viable, support for the weaker version is based on comparisons between speakers of different languages with distinctive structures on specific constructs. Typical studies compare speakers of languages that differ with respect to the conceptualization of geographic orientation or spatial direction (Boroditsky & Gaby, 2010), time (Boroditsky & Gaby, 2010), numerosity (Everett, 2013), or interpretations or memories of events, to name some salient domains. For example, Boroditsky and colleagues showed that English speakers relative to Spanish speakers ascribe blame to accidental events and remember the agents of those events more so than Spanish speakers (Fausey & Boroditsky, 2011). This, the authors explain, is because in Spanish, when describing an accidental event such as a vase breaking, one can say “the vase broke itself” without ascribing blame, whereas in English one is directed to say who broke the vase.
The number of experimental studies that test the linguistic-relativity hypothesis in the laboratory by manipulating the linguistic aspect of a stimulus, thus avoiding the cultural confound, have increased, although criticism of the methodology remains (Lucy, 2016). Examples are experiments by Franklin et al. (2008), who showed how learning a new color word actually modifies brain circuits, and Tan et al. (2008), who linked language to perceptual decisions. In a series of elegant experiments, Forder and Lupyan (2019) recently demonstrated that the words used as labels for colors facilitate the categorical perception of color. Thus, there seems to be accumulating empirical support, using sophisticated methodologies, for the hypothesis that language influences specific nonlanguage aspects of cognition and brain circuits and responses. To the extent that language influences aspects of how people relate to the world, it follows that language could play a role in our responses to the stressors around us and, therefore, our emotions.
Emotion Relativity
In addition to affecting basic processes of perception, language can shape emotion. Linguistic evidence suggests the absence of semantic emotion universals but rather a dependence on language and culture to assign specific meanings to emotions or emotion-related words (Wierzbicka, 1999). This empirical evidence has led to an affective version of the relativity hypothesis (Perlovsky, 2009). This hypothesis relies heavily on the work of linguist Anna Wierzbicka, who has argued that even the definition of emotion has a cultural bias (Wierzbicka, 1994) and that how we research emotion has been influenced by the English language’s conceptual vocabulary (Wierzbicka, 1998). According to Wierzbicka, culture determines attitudes toward emotions, which are reflected in the language’s emotion lexicon and grammar. The available emotion lexicon differs across languages and reflects a particular culture’s approach to emotional expression and social interactions (Wierzbicka, 1999). Recent empirical evidence from 2,474 spoken languages demonstrates cultural variation in emotion semantics (Jackson et al., 2019). As an illustration, the English language’s notion that emotions are to be “regulated” implies a preference for a standard or controlled emotional state and avoidance of extreme emotionality. The English language has been described as a cognitively focused language suitable for science and technology (Perlovsky, 2009). Conversely, the Spanish language has a wide array of emotion words that can be exaggerated or minimized through the use of suffixes, which are conducive to emotional expression. Whether the language reflects a culture’s view of emotion or influences that view may be impossible to parse. The effects are likely reciprocal and have evolved over time. Figure 1, oval 1, shows language influencing aspects of culture, which in turn influence language.
Cross-cultural studies have also indicated differences across cultures in the labeling of emotions (Gendron et al., 2014; Jack et al., 2012). Even within the English language, it has been suggested that focusing on six basic emotions (anger, disgust, fear, happiness, sadness, and surprise; Ekman, 1992) may be constraining. There may be greater variation in emotions than previously recognized (Cowen et al., 2019), which is important to what is being proposed here because emotional distinction (granularity) and emotional variation (diversity) may influence mental and physical health (Quoidbach et al., 2014; Smidt & Suvak, 2015).
Stress Appraisal
A critical link in the pathway between language and CVD is the construct of stress. Stress refers to any stimulus (internal or external) that taxes the organism’s capacity to respond. The psychological conceptualization of stress assumes that the appraisal of a stimulus as relevant to survival is a mediator to causing an emotional response (Cohen et al., 2016; Lazarus & Folkman, 1984). Yet the appraisal of a stressor’s personal relevance is not uniform. As a result, the same stimulus may evoke distinct physiological responses across individuals (Lovallo, 2005). It is generally presumed that differential coping responses result partly from differences in how the stimulus is appraised, with appraisal initiating the response cascade. Contextual factors, including language and culture, influence this appraisal (Fig. 1, paths B and C). In a model of stress, Cohen et al. (2016) posited that an environmental stressor may (or may not) be perceived (i.e., appraised) as threatening, which would determine whether a negative emotional response is elicited. Negative emotional responses elicit perturbations in peripheral physiological systems, such as the autonomic nervous system, immune system, and hypothalamic-pituitary-adrenal (HPA) axis. Over extended periods of time, sustained perturbations to these systems can contribute to the development of disease.
Language and Emotion: Constructionist View
An emerging body of research in cognitive neuroscience suggests that language may not simply play a role in how affective stimuli are appraised or communicated but how emotional experiences themselves are constructed. The constructionist theory of emotion (Barrett, 2006) posits that emotions are constructed by organizing internal body sensations and external perceptions around explicit conceptual knowledge (herein equated with schemas). This process of integrating current affective experience with conceptual knowledge to give rise to an emotional experience is supported by language (Lindquist, Satpute, & Gendron, 2015). Without the concept knowledge provided by language, internal sensations or external perceptions would be ambiguous (Lindquist, Satpute, et al., 2015). Thus, the concept knowledge, based on language, provides the context for the interpretation of the specific emotion. Schemas are units of conceptual knowledge, attitudes, and skills (Ghosh & Gilboa, 2014; Piaget, 1926) that are central to the formation, storage, and generalization of memories, including emotional memories (Heller, 2019). They serve to organize our understanding of the world and facilitate the interpretation of information. Schemas depend on and are supported by language. They are expressed in language (Dodge, & Lakoff, 2005). Figure 1, path A, indicates the influence of language (Fig. 1, oval 1) in emotion schema construction (Fig. 1, oval 2). When presented with a threatening stimulus these language-dependent existing schemas are accessed for their appraisal and for the construction of the emotional response (Fig. 1, path D).
Both experimental and meta-analytic studies are consistent with this constructionist view. For example, Lindquist and Barrett (2008) described how they manipulated the access to emotional language by having participants write a story about someone experiencing “anger” or “fear” or writing an emotion-neutral story. They also manipulated the participants’ body sensations with music, which was either highly arousing or unpleasant or neutral. Their results showed participants who wrote about fear and experienced the unpleasant music displayed behaviors more consistent with fear compared with participants in the other conditions. Their results support the notion that the interpretation of body states may depend on having access to the specific emotion language. Other studies have found that the perception of emotion from faces is impaired when experimenters disrupt participants’ access to linguistic emotion concepts (Gendron et al., 2012; Lindquist et al., 2006). Promising work relevant to the language hypothesis proposed here has shown that manipulating the access to emotion words during a stress-reactivity experiment influences cardiovascular reactivity responses (Kassam & Mendes, 2013). Last, meta-analyses from brain-imaging studies have found that patterns of brain activity during emotion processing (Lindquist et al., 2012) overlap with those involved in language (Binder et al., 2009).
Thus, the repertoire of linguistic concepts available may constrain the set and probability of emotional experiences. This construction of such a repertoire implicates multiple brain regions and their patterns and interactions. Cortical brain regions are involved in the integration of schemas with internal or external stimuli (Lindquist et al., 2012), and subcortical regions facilitate the coordination of emotion processes and peripheral physiology (Critchley, 2005). Patterns of responses among these regions may be key for understanding how emotions influence CVD (Kraynak et al., 2018). Neuroimaging studies have allowed the possibility of delineating these patterns in some detail. Heller (2019) explained, on the basis of the “engram theory of memory,” how cellular activity across these distal brain regions are synchronized in the formation and generalization of emotional memories or engrams (for reviews, see Gianaros and Jennings, 2018; Gianaros and Wager, 2015; Lane et al., 2009; for meta-analyses focusing on the role of language, see Brooks et al., 2017).
Emotions and Cardiovascular Health
Negative affect and health
Emotions, constructed and constrained through language, may then give rise to physiological bodily processes that, over time, become associated with health and disease. Extensive evidence, for example, has linked chronic negative emotion to CVD. Specifically, psychological conditions such as depression that are characterized by frequent and sustained negative emotion have been implicated in the development and progression of CVD. For example, major depression (Patten et al., 2009) as well as depressive symptoms more generally (Davidson et al., 2000) predict hypertension and an increased risk of mortality from heart failure (Kop et al., 2010). Likewise, meta-analyses of prospective studies have demonstrated links between depression and incident hypertension (Meng et al., 2012), depression and risk for CHD (Gan et al., 2014), anger/hostility and CHD (Chida & Steptoe, 2009), and anxiety and mortality in patients with coronary artery disease (Celano et al., 2015). Psychosocial stress, broadly defined, confers a risk of acute myocardial infarction comparable to traditional risk factors such as abdominal obesity and low socioeconomic status (Rosengren & Hawken, 2004).
Positive affect and health
Although less is known about the role positive emotion might have on health, there is increasing momentum in understanding the extent to which positive emotion influences health and the mechanisms that facilitate such influences. Evidence of interest in positive affect and health comes from several qualitative and quantitative reviews (Chida & Steptoe, 2008; Cohen & Pressman, 2006; Diener & Chan, 2011; Pressman & Cohen, 2005; Pressman et al., 2019). These reviews provide consistent evidence for an association between positive affect and longevity in older, particularly healthy adults.
The evidence linking positive affect and CVD morbidity is mixed. Boehm and Kubzansky (2012) concluded that measures of optimism were the most consistently related to CVD onset. There is also emerging evidence of relationships between positive affect and specific biomarkers of health (Cole et al, 2015; Fredrickson et al., 2015; Slavich & Cole, 2013; Steptoe et al., 2005; Uchida et al., 2018). This work suggests that trait aspects of well-being or positive emotion, although not relevant for all biomarkers, might be important with respect to immune function.
Pressman and Cohen (2005) specified trait positive affect as potentially dampening the effect of stress on health. This could happen because positive affect influences the appraisal of stress directly or indirectly by increasing social connections and the capacity to respond. To the extent that positive emotion builds capacity by increasing social connections, its accumulation may serve in a moderating role, buffering the effect of stress on body systems. A culture that values social connections may thus facilitate such a process (Fig. 1, path E).
Brain–Body Interaction
The mounting evidence associating stress, emotion, and CVD calls for a more nuanced understanding of how stressful events appraised as threatening trigger emotional responses that engender physiological reactions with implications for disease. Gianaros and colleagues (Gianaros & Jennings, 2018; Kraynak et al., 2018) contend that internal or external stimuli, when centrally appraised as threat (Fig. 1, path D), lead to the mobilization of brain-based predictions for peripheral systems to meet the situational demands of the threat (Fig. 1, path F). These appraisals also include expectations for the future. Such appraisals are interpreted and iteratively shaped by contextual factors and each individual’s own experiences. The contextual factors that construct the emotional experience include cultural norms and practices and language-based emotion schemas.
Thus, this perspective recognizes the bidirectional connection between the brain and the body in how the appraisal of stimuli as personally meaningful has consequences on the periphery, including the cardiovascular system. The bidirectional communication maintains autonomic homeostasis at set points conducive to the preservation of life. Efferent sympathetic and parasympathetic signals from the cortex affect peripheral organs with concomitant reciprocal signal flow from the periphery to the cerebral cortex (Fig. 1, path G) for integration with prior information and evaluation of predictions (Gianaros & Jennings, 2018).
In this explanatory framework, such central-peripheral communication in the service of adaptive behavior is based on the hypothesis that the system is designed to identify and subsequently minimize prediction errors. In this context, prediction errors are defined as the difference between the demand of a stressor and the brain’s signaling of the magnitude of the mounted physiological response. Using autonomic nervous-system reactivity as the mechanism, Gianaros and Jennings (2018) describe how calibration can occur at multiple set points to align the brain’s predictions with actual demand. Failure in the feedback or adjustments can lead to patterns of reactivity that are detrimental to the organism in the long term.
My hypothesis, which maps onto this framework, is that when an individual appraises a stimulus as relevant for survival, language is used to construct the emotional response. To the extent that an individual has a greater number of heterogeneous emotion schemas available from which to draw, the degree of prediction error of the experience is lessened by providing opportunity to draw from a wider range of emotion schemas to minimize error. This is analogous to the statistical phenomenon of a decrease in the absolute magnitude of the prediction slope in a simple linear-regression model and a concomitant increase in the standard error of prediction when the range of values of a predictor is truncated. Conversely, when a wide range of predictor values is available, the standard error of prediction is decreased. In the extreme case, without the possibility of adjusting the prediction because only a single schema exists, then the same prediction error would occur over and over again, and no correction or adjustment would be possible. Of particular relevance is the pattern of reactivity associated with a slow recovery or slow return to homeostasis. Having a wide range of emotional responses available for adjustment may allow a more rapid return to homeostasis.
Cardiovascular reactivity to stress (Krantz & Manuck, 1984; Steptoe & Kivimäki, 2012) as well as delayed cardiovascular recovery from stress (Linden et al., 1997; Schwartz et al., 2003; Steptoe et al., 2002) have been hypothesized to confer risk for CVD. Exaggerated reactivity, delayed recovery, or other abnormal patterns could result from a failure in visceral sensory feedback but also from a failure to adjust appraisals (Ottaviani et al., 2016) to the demands of a given situation or context. To the extent that appraisals are limited by available language-based schemas, the adjustment process can fail, prediction errors are maintained, and recovery is delayed. Over repeated experiences, this pattern can contribute to hypertension, the progression of atherosclerosis, or other cardiovascular events, including death (Fig. 1, dotted path).
Other systems have been implicated in explanations of the observed links between stress and CVD. For example, Miller et al. (2009, 2011) gave the immune system a central role in a biological embedding model to explain how a traumatic or stressful experience in childhood can give rise to chronic disease, including CVD in adulthood. Prominent in their model is the notion that stress that occurs early in life influences immune-system cells, promotes unhealthy behaviors, and dysregulates the HPA axis and the sympathetic nervous system, leading to chronic inflammation and ultimately to disease. In a study that focused on the immune system, Mehl et al. (2017) reported associations between language volume and structure and conserved transcriptional response to adversity (CTRA). Specifically, using a sampling of natural language, they found that low total volume of speech, high use of adverbs, high use of impersonal or third-person singular pronouns, and low use of third-person plural pronouns were associated with increased CTRA. These associations were independent of self-reported negative affect or loneliness. This study is particularly relevant to what is proposed here because it points to a role for language, especially features that can be interpreted as indicative of inhibited self-expression (low total volume), a lack of outward social orientation (low use of third-person plural), or exaggerated emotionality (use of adverbs) that could have far-reaching consequences on the immune system.
Thus, threat appraisal leads to emotional responses that initiate a cascade of physiological processes that link our contextual lives to health and illness. The Hispanic paradox would suggest that early in that process, when emotions are encoded, Hispanics might have a source of resilience. This source could come from cultural practices influenced by language or directly from the Spanish language itself.
Features of the Spanish Language
What might be the unique characteristics of the Spanish language that contribute to the differential appraisal of stressful stimuli, allow the creation of a wide array of schemas in encoding emotion, promote emotional expression, or build capacity for social connections? Because the Hispanic paradox is in reference to discrepancies noted in the United States, the focus here is on contrasts between Spanish and English.
One way in which Spanish differs importantly from English is that the permanence of emotions can be specified in their label in Spanish but not English. This is because the verb “to be” has two forms in Spanish: ser, which conveys a permanent state, and estar, which conveys the present but with the possibility of change. In the context of expressing emotion, the estar version is used almost exclusively (e.g., estoy triste, “I am sad”; estoy enojada, “I am angry”), with the exception of happiness, which can take on the permanent form (soy feliz) or the temporary form (estoy feliz). This distinction with respect to permanence has important implications and applies not only to emotions but also to all situations, conditions, or characteristics. As an example, if I have obesity and am constructing a schema about it, in English I may think “I am fat,” whereas in Spanish I have the option to think soy gorda or estoy gorda, the latter giving me the idea that the condition, although present, can change.
There is evidence that the Spanish language may promote the use of “happy” words. In a study on the extent to which human language has a positive bias, Dodds et al. (2015) evaluated 100,000 words across 24 corpora in 10 languages. They developed an index of happy words and observed that human language displays a positive bias independent of word frequency. Furthermore, they noted variation in the distribution of happy words, with the three corpora in Spanish having distributions of the happy-word index with the highest central tendency. Their results suggest that the Spanish language, relative to other languages, may have a larger emotion lexicon, at least in terms of positive affect. The availability of emotional words and happy words in Spanish may promote optimism and allow greater variation in emotional schemas by extending the positive-valence emotions and increasing emodiversity. Emodiversity refers to the heterogeneity in the emotions experienced by people, in terms of both valence and arousal or any other potential dimensions that allow differentiation. Greater emodiversity has been associated with improved physical health (Quoidbach et al., 2014), and greater positive emodiversity has been related to lower systemic inflammation (Ong et al., 2018).
Whether emotions are positive or negative, the Spanish language may be conducive to a greater expression of emotion. In a study of reported affect, Guttfreund (1990) randomized bilingual college students to report on symptoms of depression and anxiety in either English or Spanish. Half of his participants had English as their first language; the other half had Spanish as their first language. Guttfreund hypothesized that English-first participants would report more symptoms if randomized to the English condition, whereas Spanish-first participants would report more symptoms if under the Spanish condition. Surprisingly, participants reported more symptoms of depression and anxiety in Spanish, regardless of whether it was their first or second language. Guttfreund concluded it was “the qualities of the language being used together with the role that language plays in the individual’s life” (p. 606) that will determine the emotional reporting. The results of this study suggest that the Spanish language may allow for a greater expression of emotion and less emotional suppression.
Emotional expression has been linked to health. For over the past 3 decades, a body of research has documented the immediate and long-term benefits of expressing emotions associated with traumas or major stressors. Such psychological and physical health benefits appear to accrue for everyone, regardless of gender, ethnicity, and level of education (Pennebaker, 1997), with a slight trend suggesting that longer intervals of verbal expression of emotion were associated with stronger effects (Smyth, 1998). It stands to reason that cultures that promote verbal expressions of emotion would see some of these benefits in their general population. Further, the set of emotion words in Spanish can be magnified or minimized easily with the use of suffixes. The common use of suffixes in the diminutive -ito or -ita and the superlative -ísimo or -ísima further provide a greater range of expansion of the emotion lexicon. With the simple addition of -ito or -ita, one can diminish the magnitude of a stressor.
Another relevant feature of Spanish relative to English is the more common use of the subjunctive form of verbs. The subjunctive refers to the mood of a verb or the probability or likelihood assigned by the user of the factuality of the action. The subjunctive is also used to express subjective ideas. Using the subjunctive allows for speculation and consideration of alternative positions. The subjunctive conjugation in a morphological language such as Spanish can add emotion to the infinitive form of any verb.
With the simple form of modifying the verb ending, the speaker can introduce doubt and move an event to another reality in which the person can speculate, avoid, and explore. It is said that the literary genre magical realism represented in the work of Gabriel García Márquez has its home in the subjunctive. “Without the subjunctive García Márquez would read like Hemingway. The subjunctive is more than a verb mode; it is a complete separate reality” (Keenan, 2015, p. 97). In Spanish, the subjunctive comes naturally and allows a person to easily speculate on experiences, with the mood added directly to the verb, providing a more nuanced meaning (Stadthagen-Gonzalez et al., 2017). The subjunctive mood is not frequently used in English (Turner, 1980), but it is widely used in Spanish and more commonly used in Spanish than in other Romance languages. Although there are other distinctions in terms of the type of information conveyed by verbs in English and Spanish (Slobin, 2003), the subjunctive has a close connection to the emotional aspect of the language and to the link between positive emotion and exploration.
Taken together, the features of the Spanish language presented here are consistent with the facility to express and encode a wide range of emotions. From the availability of an extensive emotion lexicon to the possibility of easy exaggeration, the Spanish language is conducive to emotional expression. Lazarus (2006) described the appraisal of stress as “a process of negotiation between the objective conditions and what people wish or fear (p. 5).” The common use of the subjunctive form of verbs in the Spanish language facilitates the introduction of hypotheticals, and the flexibility of permanence with two different forms of being provides individuals with more tools for negotiation.
Language Hypothesis
The definition of Hispanic is one who speaks the Spanish language or comes from a Spanish-speaking country. The language is the single distinguishing characteristic of this classification. The hypothesis put forth here is that the Spanish language, by virtue of its flexibility, use of the subjunctive, and abundance of its emotion lexicon, promotes the processing of emotion in a way that dampens the effect of stressful stimuli on cardiovascular reactivity and thereby promotes cardiovascular health. A corollary to the hypothesis is that the Spanish language may contribute to a culture that facilitates and promotes easy expression of emotion and a means of managing stressors by building social connections and promoting the exploration of hypotheticals. The values mentioned earlier that characterize the Hispanic/Latino culture all involve the use of language. Spanish may also contribute to a happy view. And these features may alter the pathways to cardiovascular health.
There may be more than one pathway by which Spanish language to leads to improved cardiovascular health, despite higher risk profiles (the Hispanic paradox; see Fig. 1). One possibility is that the language directly influences the construction of emotion schemas, and this path extends beyond the language’s effect on the culture. This path relies on the proposition that the Spanish language is conducive to emodiversity. In the presence of emodiversity, a wide range of emotion schemas are available for use in the appraisal of a stressful or threatening stimulus and in the minimization process of prediction errors central to attaining homeostasis. Thus, along this path, the Spanish language assists in the construction of capacity to respond to stress and buffers the effect of stress on body systems, allowing for quicker recovery. The second pathway is based on the proposition that the Spanish language reflects or influences (or both) cultural practices that promote social connectedness, expression of emotion, optimism, and the exploration of hypothetical situations that could have positive outcomes. In doing so, the Hispanic culture also assists in building capacity that influences the appraisal of stressful stimuli and dampens their effect on cardiovascular physiology. These propositions are consistent with the conceptual models proposed by Pressman and Cohen (2005) and Fredrickson (2013) in the context of positive emotion. They are also consistent with theories of stress and coping.
Future Directions
As with any novel hypothesis, much more work is needed to test its viability and limitations. The selection of features in the Spanish language were identified ad hoc. Specific domains such as emotion lexicon, use of the subjunctive, ease of exaggeration, and distinction between transient and permanent states were highlighted because they have some face validity in terms of their potential link to emotion processing. This domain-based approach is not conducive to integration and generalization to other languages. Rather than handpicking these domains, a structured-centered analysis that systematically compares languages along predetermined dimensions could provide a starting point for the selection of features to be tested empirically. Experimental work could then use a behavioral approach in which these features are manipulated to assess their effects on proximal and distal outcomes. Outcomes to consider include stress appraisals, emotion encoding, neural responses, and cardiovascular reactivity and recovery.
Although anecdotal evidence suggests greater emotional expression in Spanish compared with English, it would be useful to better characterize the emotion lexicon in English and Spanish as well as to compare the use of emotion words in general populations. Paralleling the recent work of Cowen et al. (2019), the high-dimensional taxonomy of emotions could be compared between English and Spanish to determine whether the number and composition of emotion dimensions differ as a function of language.
Any study that compares English and Spanish speakers must confront the decision of how to deal with the confounding of culture and language, as the samples of primary interest would be English and Spanish monolingual speakers. Attention would need to be given to other sociodemographic characteristics, including identification with one’s culture. One of the ways in which culture has been controlled is with the use of bilingual samples, in which an ordering of the languages is taken into consideration, as was done in the design used by Guttfreund (1990), in which both English/Spanish and Spanish/English bilingual participants were assessed. Working with bilingual participants introduces additional issues such as comparability in proficiency, language dominance, and exposure to cultural content. Bilingual persons have been reported to present different personalities in different languages, a phenomenon that may be related to the level of language proficiency in that language (Degner et al., 2012). The extent to which language proficiency plays a role in emotion construction and expression and, in turn, sympathetic arousal would be an important consideration.
Additional questions raised by the language hypothesis include whether there are individual differences in language use among Spanish speakers from different countries and the extent to which differences in the use of specific features (e.g., the subjunctive) may be associated with differences in disease. Considering the generalizability of the language hypothesis, another question is whether the difference in CVD prevalence is present in speakers of Spanish compared with speakers of other languages outside of the United States. Along with tests of the language hypothesis, further work is needed to address these ancillary questions.
Conclusion
This article reviewed evidence in support of the notion that the Spanish language plays a role in explaining the Hispanic paradox by virtue of how language influences the appraisal of a stressor and the encoding of the emotional response in language-based schemas, which leads to the regulation of autonomic and other (i.e., neuroendocrine and immune) systems in the body. The Spanish language indirectly reinforces a culture open to the expression of emotion and the exploration of hypothetical considerations in the presence of stress. This review is not exhaustive and spans distinct disciplines, including epidemiology, psychological linguistics, anthropology, and behavioral and cognitive neuroscience. Although not all of the links in the pathway from language to disease are fully supported by empirical evidence, there is sufficient theory, logic, and evidence to entertain the plausibility of this hypothesis. Linguistic and neuroimaging evidence converge to suggest an important and direct role for language in emotion encoding and expression. Further work combining linguistics, cultural anthropology, psychology, and neuroimaging is needed to strengthen the evidence of the links along the proposed pathways. The goal of this work should not only be to better understand the role of language in disease and unravel the paradox but also to identify practices that would improve cardiovascular health in a population.
Footnotes
Acknowledgements
I thank my colleagues Aaron Heller, Patrice Saab, and Richard Sloan for their feedback on an earlier version of this article. I also acknowledge the important suggestions of an anonymous reviewer and the editor.
Transparency
Action Editor: Laura A. King
Editor: Laura A. King