
Abstract
The Bayesian-brain framework applied to placebo responses and other mind–body interactions suggests that the effects on the body result from the interaction between priors, such as expectations and learning, and likelihood, such as somatosensorial information. Significant research in this area focuses on the role of the priors, but the relevance of the likelihood has been surprisingly overlooked. One way of manipulating the relevance of the likelihood is by paying attention to sensorial information. We suggest that attention can influence both precision and position (i.e., the relative distance from the priors) of the likelihood by focusing on specific components of the somatosensorial information. Two forms of attention seem particularly relevant in this framework: mindful attention and selective attention. Attention has the potential to be considered a “major player” in placebo/nocebo research, together with expectations and learning. In terms of application, relying on attentional strategies as “amplifiers” or “silencers” of sensorial information could lead to an active involvement of individuals in shaping their care process and health. In this contribution, we discuss the theoretical implications of these intuitions with the aim to provide a comprehensive framework that includes Bayesian brain, placebo/nocebo effects, and the role of attention in mind–body interactions.
Keywords
The Bayesian interpretation of the human mind suggests that the brain does not perceive the world as it is, but as it is predicted to be (Friston, 2010). The brain uses probabilities, relying on previous expectations (i.e., “priors”), to infer the state of the world such that perception may be interpreted as a result of prediction rather than simply assimilating signals. These perceptions adjust following prediction and error processing, which is the brain’s ability to update models of the world and the body. Specifically, the encounter-confrontation of top-down processes (i.e., mental representations reflecting the working hypothesis of the state of the world and the body) and the bottom-up stream of sensory inputs generate a mismatch between predictions and inputs (i.e., prediction errors), which lead to a revision of the prior representations. In other words, the processed signals are essentially those that do not match prior expectations under this corrective-feedback process (Ongaro & Kaptchuk, 2019). Therefore, mental representations are updated when the brain receives new information that enables probabilistic representations (i.e., expectations) to be modified in a Bayes-optimal fashion. According to this model, the brain follows the “Bayes rule,” which states that the prior (e.g., an expectation) is integrated or updated with new information (i.e., the likelihood), resulting in an outcome (i.e., the posterior) that has a different distribution and location (see Fig. 1; Hohwy, 2013). The distribution of a certain prior (e.g., an expectation) or of new information (e.g., an observation) may be more or less precise based on the variance of its distribution (lower variance corresponds to a greater precision). Precision can be thought of as the confidence one has in a prior or the relevance one ascribes to the sensorial information. Graphically, higher precision results in a narrower distribution (in Fig. 1, the likelihood is more precise than the priors).
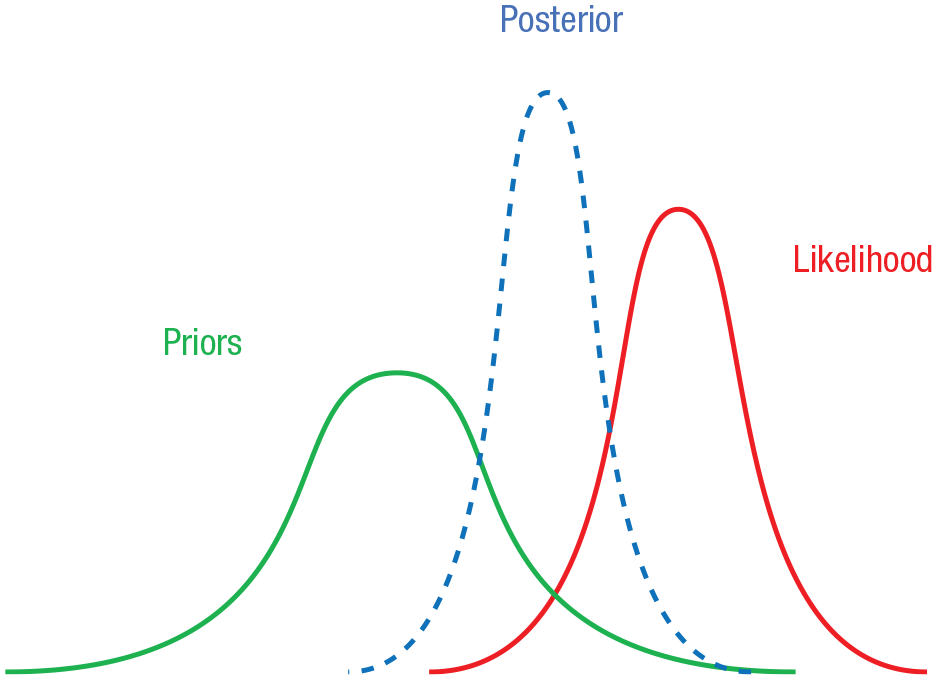
Bayesian model (priors – likelihood – posterior).
With the perception, which is this process of belief updating, the brain tries to reduce the “surprise” (i.e., the prediction error). To minimize surprise and create a more stable and foreseeable representation of the world (Holmes & Nolte, 2019), the brain can leverage two different strategies, depending on the “direction” of the belief-updating process. The first, “perceptual inference,” is the process of constantly updating the prior following prediction errors. The second mechanism is called “active inference,” which entails acting on the world (e.g., the body) to modify it so that sensory inputs are consistent with prior beliefs (e.g., homeostatic regulation). Overall, the world is actively sampled or organized to ensure that predictions become self-fulfilling prophecies and surprises are avoided (Friston, 2009).
The Bayesian-brain model falls within the concept of predictive coding, which describes how belief updating rests on increasing prediction errors, which update prior expectations to form posterior beliefs. Crucially, this updating process depends on the precision afforded to prediction errors (Ainley et al., 2016; Brown et al., 2013; Clark, 2013; Feldman & Friston, 2010; Kok et al., 2012; Limanowski, 2017). In other words, if the precision is estimated to be high, sensory prediction errors have a greater influence on higher-level representations (i.e., prior expectations). Mathematically, this is related to the Kalman gain in Bayesian filtering (Kutschireiter et al., 2017); physiologically, this precision weighting is generally thought to reflect the excitability of neuronal populations reporting prediction errors—which depends on various neuromodulatory mechanisms. Finally, from a psychological perspective, increasing sensory precision may correspond to attentional mechanisms, that is, selecting those prediction errors that have privileged access to higher-level expectations (Feldman & Friston, 2010). Relatedly, in the context of active inference, attenuating sensory precision has been explored by several studies (Brown et al., 2013; Hohwy, 2020; Limanowski, 2017, 2022; Palmer et al., 2015, 2017; Pareés et al., 2014). Psychologically, this is often read as sensory attenuation (i.e., ignoring the consequences of self-generated actions). Perhaps the best example of this mechanism is saccadic suppression, which is the attenuation of optic flow signals during fast eye movements. It has been argued that failures of sensory attenuation and concomitant increase because sensory precision underlies many neuropsychiatric conditions, ranging from autism to nociception and functional medical symptoms (Ainley et al., 2016; Edwards et al., 2012; Fotopoulou & Tsakiris, 2017; Jardri et al., 2016; Krahé et al., 2013; Sterzer et al., 2018). Another way of attenuating sensory precision is through distraction (Edwards et al., 2012), which happens when attention is diverted away from the stimulus. Different studies suggest that distraction affects the precision of sensory stimuli, including appetite (Brunstrom & Mitchell, 2006) and pain (Bascour-Sandoval et al., 2019; Buhle et al., 2012).
In computational psychiatry, predictive coding has successfully provided models to explain phenomena, such as hallucinations, whose effect is mediated by strong prior beliefs, with a top-down effect that is particularly strong with voice hearers, and with an impaired belief-update process (bottom-up) in individuals with psychosis (Powers et al., 2017). However, the interaction between priors and the information received seems to differ depending on the sensor modalities and their integration, suggesting a hierarchical organization that still has to be fully explored (Sterzer et al., 2018). The Bayesian-brain hypothesis also provides a neurobiological account of functional-movement disorders (Edwards et al., 2012), once defined as “hysteria” or “conversion disorders.” Incorrect predictions about the consequences of one’s motor behavior might be the basis for the emergence of abnormal motor behaviors (Silveri et al., 2022). For example, the altered prediction about the sensorial consequences of a specific movement could result in a mismatch between the top-down expectation of the sensorial response and the actual response. In turn, this mismatch might be responsible for the altered motor programming; for example, the geste antagoniste in cervical dystonia might be seen as the movement that “works in anticipation of its sensory consequences” (Newby et al., 2016). Lack of a “sense of self-agency” during the movement is likely the most significant consequence of the mismatch between the expected and the actual sensory response (Maurer et al., 2016).
Placebo/Nocebo Responses as Active Inference Processes
The Bayesian-brain hypothesis is supported by growing evidence (Rohe et al., 2019) and has several potential implications for health and the relationship between mind and body. From a Bayesian perspective, for example, there is a particular “healthy body condition” hypothesis (Ongaro & Kaptchuk, 2019) whereby if the variation of somatic sensations (e.g., heart rate variability) is within the bound of a certain distribution, there is no percept of somatic change. A “symptom” is perceived when an “abnormal” somatic event (exceeding a subjective threshold of the healthy range of somatic-sensation variations) represents a prediction error. The Bayesian model offers a compelling explanation for placebo effects and other mind–body interactions (Kaptchuk, 2018). In this model, concepts such as expectation and learning, key components of the placebo effect (Barbiani & Benedetti, 2020), would represent the priors. When combined with sensory information (i.e., likelihood), including proprioceptive signals, an active inference process can explain physiological and functional changes. In other words, to reduce the prediction error, placebo responses would hijack perception not by revising the priors (which would be a perceptual inference) but by making sensory stimuli consistent with them, promoting physiological, functional, and biological changes (via active inference). The precision of priors and likelihood would eventually influence the physical outcome. For example, a less precise likelihood, such as perceived fluctuations of perceived pain, has been associated with increased placebo responses (Farrar et al., 2014).
The placebo effect can be defined as a psychobiological phenomenon, which cannot be ascribed to the action of a pharmacological substance but rather to words, rituals, symbols, and meanings (Benedetti, 2020). Clinical benefit following placebo administration is achieved with the administration of an inert substance or device along with verbal suggestions of improvement. Verbal suggestions are crucial for inducing expectations, which are considered a key mechanism in placebo responsiveness. Beyond expectations of benefit or improvement, learning mechanisms, including classical and operant conditioning, and observational learning are crucial mediators of the placebo response (Colloca & Miller, 2011). Whereas the “placebo effect” refers to the positive outcome following the administration of an inert treatment along with explicit or implicit information of improvement, its negative counterpart (i.e., the nocebo effect) refers to a negative outcome following information of worsening. In the clinical setting, the nocebo effect may emerge when patients are informed about the possible side effects of a treatment and/or when they hold negative expectations about the treatment itself (Benedetti, 2020). Because the placebo effect is a psychosocial-context effect, there is now compelling evidence that different social stimuli, such as verbal suggestions and therapeutic rituals, may change the patient’s brain. These effects are similar to those induced by drugs (Benedetti, 2020). Ample evidence demonstrates there are many placebo effects, not one, with different mechanisms across different disorders and conditions (Benedetti, 2020). Some of the most fruitful models to understand the psychobiology of the placebo effect dealt with pain (Colloca, 2019), fatigue and physical performance (Shaibani et al., 2017), the gastrointestinal system (Elsenbruch & Enck, 2015), and the immune system (Smits et al., 2018). Across these and other domains, placebo administration significantly affects outcomes with remarkable changes in biochemical, neurophysiological, and behavioral parameters (Benedetti et al., 2016; Vits et al., 2011). Exposure to a negative psychosocial context (nocebo) may exacerbate symptoms and anxiety, eliciting symptoms or side effects that mirror the negative expectations about their onset (Colloca & Barsky, 2020; Pagnini et al., 2020). For example, among participants who received a nocebo believing it to be experimental endotoxin, physical symptoms correlated with state anxiety (Benson & Elsenbruch, 2019). Whereas anxiety and stress are some of the moderating factors for the nocebo response (Roderigo et al., 2017), individual characteristics such as optimism (Kern et al., 2020) and other personality traits (Frisaldi et al., 2018) are related to placebo effects (Frisaldi et al., 2018). However, further studies are required to define placebo responders and nonresponders. Placebo and nocebo effects may lend themselves to being considered through a Bayesian lens; the idea of applying a Bayesian explanatory framework for placebo mechanisms has been suggested by prominent scholars in the field (Kaptchuk et al., 2020) and successfully used to explain placebo hypoalgesia (Büchel et al., 2014). Complex psychological factors such as expectations and conditioning are at the very heart of placebo and nocebo effects and may play the role of priors and shape the process of reducing predictive errors from perceptual stimuli. One example focuses on symptom relief following placebo administration; this results in a revision of a maladaptive hypothesis (e.g., a chronic illness that clashes with interoceptive cues indicating improvement). Crucially, the process of interpreting these cues as signs of amelioration rather than “noise” can be activated by placebo usage that is nudging the brain to analyze small interoceptive changes in the body as a hallmark of the healing process (Ongaro & Kaptchuk, 2019).
There are other types of mind–body interactions in addition to a “classic” placebo response. For example, a study with people with type two diabetes (Park et al., 2016) manipulated participants’ perception of time, leading them to believe that more or less time had passed than the actual time. Remarkably, these patients’ blood-glucose levels followed perceived time rather than actual time. Although the chronological time was the same for everybody, participants who thought more time had passed had a significantly greater decrease in blood-glucose levels compared with participants who believed less time had passed. Another line of research found a strong association between the expectations of developing influenza-like symptoms and their actual development over the wintertime, even when accounting for previous influenzas or general health (Pagnini et al., 2020). These and other studies (e.g., Crum et al., 2011; Rahman et al., 2020) describe how illness expectations can become self-fulfilling prophecies (Crum & Phillips, 2015; Pagnini, 2019).
Neural Correlates of Placebo Effects in Bayesian Brain
The Bayesian-brain mechanism and placebo/nocebo responses also share some similarities in terms of neural correlates. A growing body of research has identified target areas in the brain that appear to be crucial for placebo responsiveness (Benedetti & Piedimonte, 2019; Carlino & Vase, 2018; Dodd et al., 2017). At the same time, a Bayesian-brain approach (Knill & Pouget, 2004) is rapidly taking hold in neuroscience and may help accommodate placebo phenomena. Recent models (Geuter et al., 2017; Lieberman et al., 2004) formulated to explain brain mechanisms underlying these effects identify the prefrontal cortex (PFC), insula, amygdala, hypothalamus, and periaqueductal gray (PAG) as critical brain regions in which dynamical and temporal changes occur before and after placebo administration. In this distributed network, the PFC has been identified as a pivotal structure in a Bayesian-brain model that implements probabilistic inference involved in the computation of predictions, the estimation of sensory discordance, and the continuous updating of priors to better predict the incoming sensory inputs and minimize error (Cao et al., 2019). This hypothesis is supported by neuroanatomical evidence demonstrating that the PFC is a convergence zone for multisensory information, receiving a widespread array of afferents from higher auditory and visual cortices and from association areas enabling a flexible strategy of sensory fusion (Romanski, 2012). In particular, the ventromedial prefrontal cortex (vmPFC) seems to play a key role in the generation of placebo responses. Research suggests that this brain area is involved in combining several streams of information (Roy et al., 2012), representing current states (Schuck et al., 2016) and structured relationships among notions, forming novel concepts (Barron et al., 2013), and conceptualizing future states of the self (Schacter et al., 2007). Therefore, the vmPFC provides a neural substrate for the expectations. Moreover, it has been proposed (Geuter et al., 2017) that relational maps of representations are located in vmPFC and constitute multidimensional priors that encode both the magnitude of predictions (the quantitative intensity) and the qualitative experience of the situation, including visceral correlates. These rich situational representations are integrated with sensory information processed from posterior brain regions to build percepts and direct motivated behavior. The integration of information in which top-down and bottom-up processes interact also involves the dorsolateral prefrontal cortex (dlPFC), lateral orbitofrontal cortex (lOFC), precuneus, and temporoparietal junction, regions associated with cognitive appraisals and attentional control (Ashar et al., 2017; Zunhammer et al., 2021). These dorsal frontoparietal and ventral attentional networks exert multiple effects on perception, emotion, and physiological responses via major descending projections to associative learning structures. Through these descending pathways, representations that generate predictions are projected from prefrontal regions to limbic brain areas, including the hypothalamus, amygdala, nucleus accumbens, and PAG, and downstream to effectors in the lower brain stem and spinal cord involved in nociceptive, autonomic, and immune regulatory systems (Geuter et al., 2017). Via descending pathways, cortical regulation may finally reach peripheral organs and determine complex psychobiological responses modulating hormone release and other transmitters into the blood. The engagement of a specific effector system depends on the nature of the placebo manipulation (Geuter et al., 2017). The involvement of these neural structures seems to further support the use of a Bayesian explanation for the mind–body phenomena (Shams & Beierholm, 2022), but neural coding and computation need to be further explored and defined.
The Role of Attention in the Modification of the Likelihood
The scientific literature on the placebo effect points out the role of expectations (verbally induced) and learning (induced via repeated exposures to an active agent— i.e., conditioning paradigm; Colloca et al., 2010) as crucial priors (Barbiani & Benedetti, 2020; Benedetti, 2020). The role of verbal instructions and conditioning is also widely explored (Wolters et al., 2019) and has clinical implications, including how physicians can facilitate a placebo response through the relationship with their patients (Evers et al., 2021). Although assuming a mind–body Bayesian framework, researchers have given much less space to the likelihood and its manipulation. In fact, the weight assigned to the different sensorial information is not only determined by their intrinsic variability but may also be modified “top-down,” through cognitive strategies that can alter their relative influence. One of the most prominent examples of top-down modulation of information processing is endogenous attention (referred to hereafter as “attention”), which can be used to bias perceptual inference (Limanowski, 2022). Only a few studies have explored the mediating role that attention and perception can exert on the placebo effect (Geers et al., 2006; Rossettini et al., 2018). Available data suggest that focusing attention on the expected somatic response leads to an increase in the effect when the expectations are highly precise but hinders it when the expectations are less precise (Geers et al., 2006). The complex interaction between priors and likelihood still needs to be understood. Attention and perception are not independent of the priors; the Bayesian-brain model was initially developed to explain these two functions (Knill & Pouget, 2004). Expectations and learning could shape the perception of the somatic response, but that seems to depend on their precision levels. Understanding the role of attention and how it could be manipulated to promote desired clinical effect is a new frontier of mind–body research. We suggest that attention can lead to a shift in the position of the posterior distribution by acting on the precision of the somatosensorial information, or on its components, modifying the likelihood distribution. We identify two “attentional axes” referred to a specific target: One (y) represents the precision of the considered stimulus, and the other one (x) describes how far the target of selective attention is from the priors by sampling these stimuli differently (Fig. 2). In visual terms, this model enables identifying the precision of the likelihood (the position on the y-axis) and its relative distance from the prior (the position on the x-axis). In other words, given the distribution of the prior, it enables computing the expected value (i.e., the distance from the prior) and the precision of the likelihood distribution. Combined with the prior, this information enables estimation of the posterior.
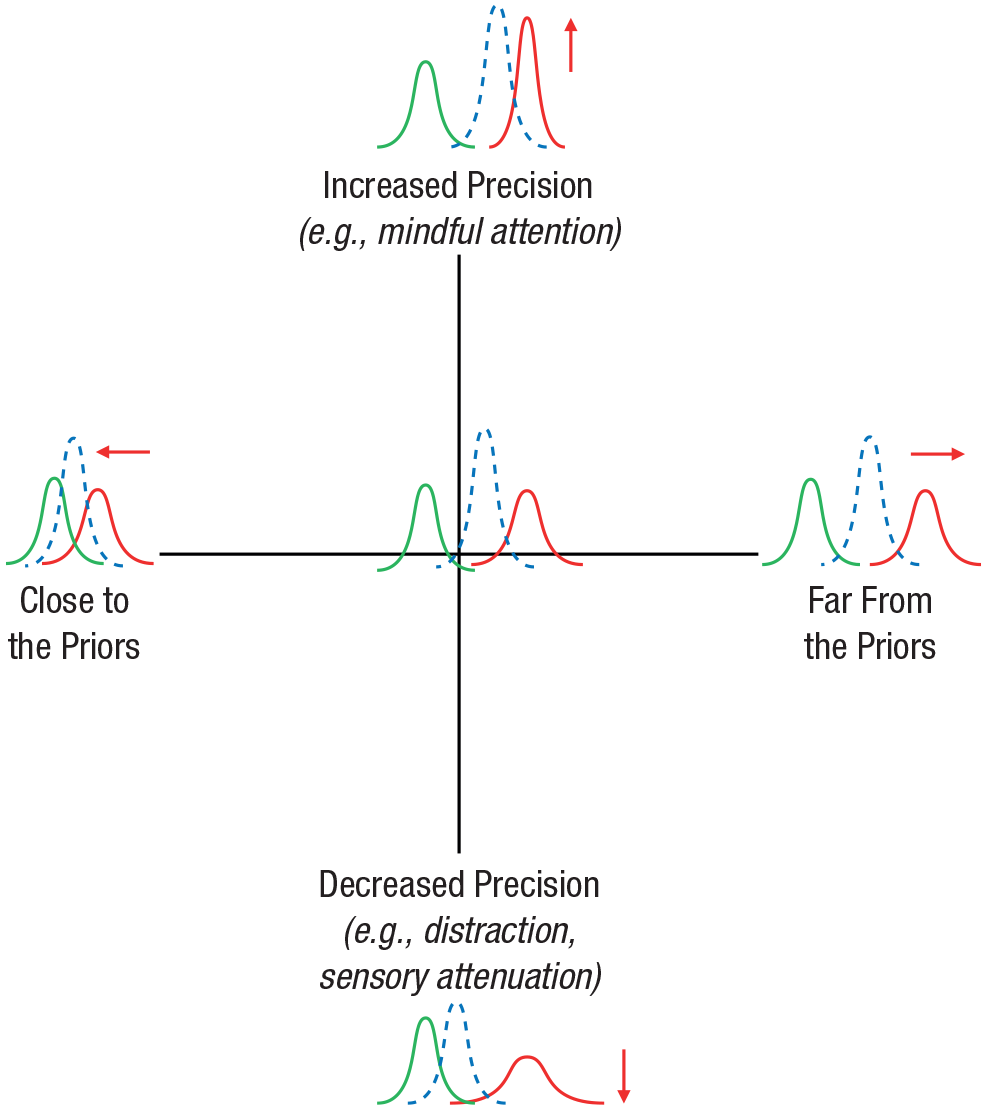
Attention-driven likelihood precision and relative distance from the prior. The y-axis goes from maximum precision (e.g., mindful attention) to lack of attention, such as sensory attenuation or distraction (minimal precision); the x-axis ranges from very close to the prior to its opposite. Priors are green, likelihood is red, and posteriors are blue.
For example, if a person receives a decaffeinated coffee disguised as caffeinated, the activated priors will likely depict the psychophysiological effects of caffeine. Depending on their rigidity and combined with the somatosensorial information received, they will create a posterior, which will, in turn, influence the placebo response (e.g., being stimulated). This model suggests that if people focus on the somatosensorial information that confirms these priors (i.e., how energized they feel) or ones that would disconfirm them (i.e., how tired they feel), the position of the likelihood would also change accordingly. Furthermore, focusing attention on the information in an unbiased way or, on the opposite side of the precision spectrum, not being aware of these data at all would shape their precision level, again providing a different likelihood, to be combined with the priors.
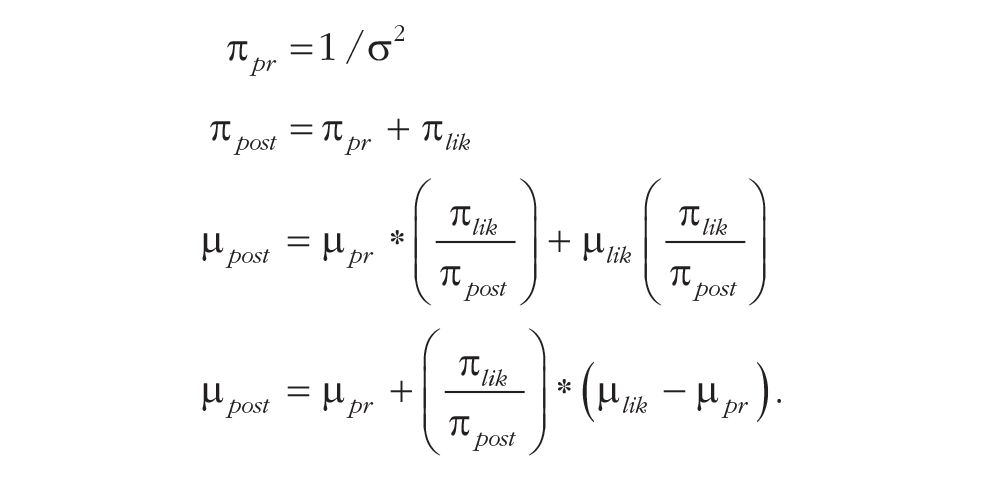
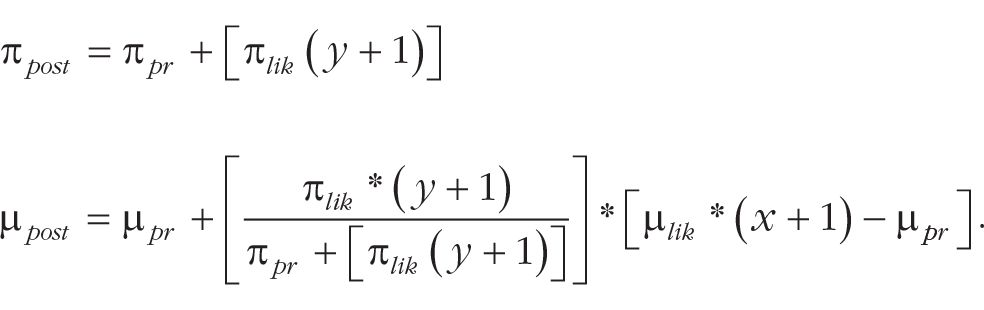
Mathematically, below are the equations to compute expected values and precision of the posterior distribution (see e.g., Sterzer et al., 2018), where π is the precision, µ is the expected value, pr refers to the priors, post refers to the posterior, and lik refers to the likelihood.
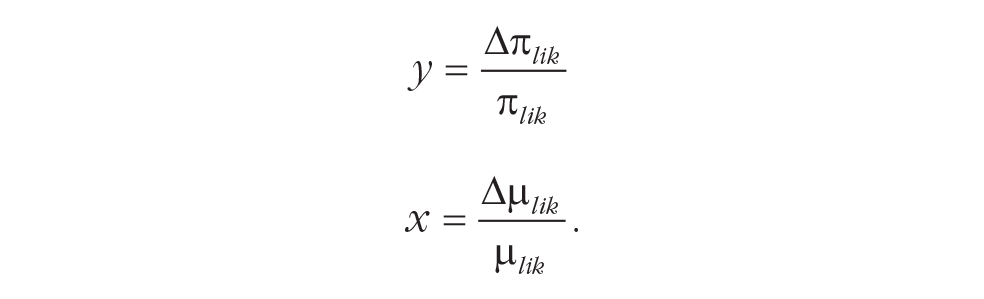
The attention coefficients y and x can be added, where y represents the change in attention-related precision (computed as the difference between precisions in time or compared with “neutral” attention) and x corresponds to the difference in precision between a relatively unbiased expected mean and the one obtained by focusing the attention of specific characteristics of the stimulus:
Therefore, accounting for these attention coefficients, the equations to compute precision and the expected value of the posterior will be modified as follows:
Increasing somatosensorial precision: from mindful attention to distraction/sensory attenuation
The precision of the somatosensorial data can be improved by pointing an unbiased (or, at least, less biased—i.e., with less rigid priors) attention toward the proprioceptive/interoceptive information that one is receiving, as it happens with mindful attention (Papies et al., 2015). Mindful attention is a specific form of attention in which a person is aware of thoughts and experiences and can observe them as transient mental events (Papies et al., 2015). It requires decentering or the insight that experiences are impermanent mental events rather than permanent states reflecting an objective reality (Keesman et al., 2020). Mindful attention is an essential component of mindfulness, which is defined here as the process of actively noticing new things as a way to be in the present (Pagnini & Philips, 2015). Mindfulness also includes or incorporates the awareness of somatosensory attention (Khoury et al., 2017). It has been suggested that mindfulness, as well as meta-awareness, facilitates an “opacification” of mental states (Limanowski, 2017; Limanowski & Friston, 2018; Lutz et al., 2019), promoting awareness of their processes and, eventually, fostering their de-reification (Lutz et al., 2015). Its opposite is defined as “mindlessness,” in which one’s perspectives and expectations rely on aprioristic knowledge and automatic thought processes, judgments, and behavior (Langer, 1989). Priors are mindless insofar as they shape experience on the basis of previous schemas without regard to current contextual cues. In a mindful-attention state, the individual focuses on the present moment, decentered from previous schemas. Thus, these schemas have a limited impact in predicting current experience. In Bayesian terms, the precision of the priors reduces while the salience of the likelihood increases. Simultaneously, unbiased (or less biased) attention toward the information received increases the salience and the precision of the likelihood. As a result of these processes, the posterior will be closer to the likelihood. Previous studies have suggested that mindful attention can reduce automatic reactions and behaviors (Papies et al., 2015), including salivation and automatic food biases (Baquedano et al., 2017).
Mindfulness-based interventions and mindfulness disposition often resulted in association with somatic changes (Riva et al., 2021). For example, dispositional-mindfulness levels predict different disease progressions in people with amyotrophic lateral sclerosis (Pagnini et al., 2015). They are also longitudinally associated with lower levels of fatigue in people with multiple sclerosis (Pagnini et al., 2019). Mindfulness-based interventions seem to reduce physical symptoms in various chronic conditions, including multiple sclerosis (Carletto et al., 2020), cancer (Cillessen et al., 2019), and chronic pain (Hilton et al., 2017). These associations suggest a protective role of mindfulness against adverse physical outcomes. One possible explanation, which requires more specific investigation, is that mindful attention can mitigate the effects of negative priors, resulting, compared with people with lower dispositional mindfulness, in an improvement of physical outcomes. By referring to the illness-expectations model (Pagnini, 2019), which aims to explore how expectations can influence the course of chronic illnesses, we believe this would be conceptualized as a reduction of cognitive rigidity over one’s expectations. In this sense, the influence of negative expectations on the course of an illness can be reduced by mindfulness because it increases cognitive flexibility (Pagnini & Langer, 2015). The rigidity of a schema, in the Bayesian framework, corresponds to the precision of a prior. A rigid schema/precise prior requires more discordant observations to be modified than a flexible prior. Despite many desirable results associated with mindfulness and mindful attention, however, we note that a more precise likelihood is not intrinsically positive or negative because it depends on the context. In the case of a placebo induction, mindful attention is supposed to hinder the effect, because the likelihood increases its precision, while the priors (in this case, the placebo effect) become less precise. Moreover, as suggested by Stephan and colleagues (2016), for example, an exaggerated likelihood precision may lead to an overdrive of efforts to restore allostasis, possibly prompting fatigue and depression. However, an increase in likelihood precision following mindful attention is also paired with a reduction of the priors, reducing the efforts required to reconcile them into a posterior.
On the other side of the precision spectrum, distraction and sensory attenuation are two examples of mechanisms that hinder attention on specific targets or tasks. When one is distracted, the precision of a stimulus is reduced, increasing its uncertainty. In fact, a lower level of precision corresponds to a broader distribution that encodes a particular degree of uncertainty about a particular cause (Feldman & Friston, 2010). Mathematically, this uncertainty is the average (expected) surprise over all possibilities and can be measured by the width of variance of the distribution (i.e., precision). From a Bayesian perspective, when the variance of the likelihood distribution decreases (i.e., becomes more precise), the influence of the prior is reduced, making it less likely for priors to update, forming a different posterior. Likewise, sensory attenuation allows to “switch off” sensory precision, abolishing belief updates during self-generated movements (Petzschner et al., 2017).
Getting closer or moving farther away from the priors: selective attention
Whereas mindful attention tries to “escape” from biases (i.e., higher- and lower-level priors), other forms of attention are, purposefully or not, biased. As mentioned, attention can bias perceptual inference by sampling somatosensorial information differently, increasing the precision of specific characteristics. In hierarchical-generative models, hierarchies of probabilistic representations that predict somatosensorial information can be systematically altered by modifying the relative influence of sensorial cues (Limanowski, 2022). Thus, a direct focus on specific and selective components of the sensory information (likelihood) will emphasize their salience and shape the posterior in different ways. For example, when someone listens to a symphony, the sensorial information can be a compendium of auditory stimuli resulting from the orchestra playing. However, one can focus attention on a specific instrument (e.g., violins), changing the precision of the different components of the information and, eventually, reshaping the sensorial experience. This selective attention emphasizes specific parts of the sensorial information in which perceptual systems must triangulate different sensory signals, assigning greater or lesser precision to specific prediction errors, resulting in a different experience. Paying selective attention to specific somatic perceptions could result in an increased magnitude of these perceptions (Rossettini et al., 2018). The few studies that explored this modulating effect of selective attention did not manipulate its target. It is not yet known what will happen when attention is oriented (following placebo administration or some other mind–body trigger) toward either the characteristics of the sensorial information that confirm the priors or the opposite direction. Furthermore, this effect may be particularly relevant when the priors are less precise because the likelihood would be less constrained by the priors’ influence and thus be more strongly modulated by attention. This could result in an increased salience of the likelihood, which, in turn, will dominate the priors in determining the effects on the posterior. Because selective attention focuses on specific components of the received sensorial information, it can be argued that the integration of multiple information channels, such as different senses, can further increase the overall precision of that specific part of the likelihood. For example, hearing fire cracking, smelling smoke, and observing a flame is a more precise experience of fire than just one of these components (Riva et al., 2021).
In the context of this model, selective attention is particularly relevant when directed toward stimuli that are consistent or inconsistent with the priors. In the first case, selective attention is directed toward the confirmation of the anticipated mind–body effect. For example, after receiving a placebo for pain reduction, the focus will be on how much pain relief one is experiencing. In the second case, selective attention deals with the opposite direction of the anticipated effect. In the analgesic-placebo example, the focus will be on the perceived pain. When directed toward prior-consistent stimuli, attention reduces prediction errors, and when directed in the opposite direction, it increases prediction errors.
Incorporating Attention and Sensorial Information in a Mind–Body Placebo Framework
Individual characteristics and previous experiences can spontaneously modify attention, for example, through premature cognitive commitments (Chanowitz & Langer, 1981) or attention bias (Smith et al., 2006). In the mind–body framework, for example, previous painful experiences may hijack attention toward pain-relevant cues, increasing the salience of sensory information confirming pain (Villemure & Bushnell, 2002). In turn, this spontaneously shifted attention may affect how one approaches incoming sensory stimuli (i.e., the likelihood), influencing their levels of precision and, in turn, changing the posterior. Introducing a complex role of attention, influenced by past experiences, individual characteristics, and current priors, may help explain a controverted phenomenon (reported in one study involving patients with Parkinson’s disease [PD]; Lidstone et al., 2010). In this study, PD patients were told different probabilities (0%, 25%, 50%, 75%, 100%) of receiving an active medication versus placebo, but in fact, they all received a fake treatment. Remarkably, only those patients who were informed of a 75% probability of receiving the drug showed a significant increase in dopamine release in the striatum, whereas no improvements were observed in patients who were given a 100% probability. In other words, the placebo response manifested only under a condition of mild (75% probability) and not complete (100% probability) certainty of receiving the drug. Although this may sound counterintuitive, because it challenges the notion that placebo effects are more likely to occur when priors have a higher degree of certainty or precision, this conundrum may be solved by introducing the role of attention: The lesser degree of certainty (i.e., lower precision) of the placebo-induced expectations could have heightened patients’ attention toward bodily sensations that were consistent with the anticipated effects of the drug, thus making it more likely for these same effects to occur, including those at a neurobiological level (i.e., dopamine release). This is consistent with evidence that placebo effects are stronger when one closely attends to expectation-relevant somatic sensations (Geers et al., 2006; Rossettini et al., 2018). Contrarily, complete confidence (100% probability) of receiving the drug could have made patients less actively engaged in the detection of its anticipated effects, decreasing their level of somatic focus (i.e., attention toward the body) and, in turn, the magnitude of the placebo effect.
Any placebo/nocebo procedure engenders expectations, which may be influenced by higher-level priors (e.g., trust in medicine, previous experience with this treatment). These higher-level priors may themselves affect the likelihood (or its specific sensorial components), through attentional mechanisms, beyond any “active” placebo or attention manipulation. The effects of a placebo procedure are therefore somewhat “contaminated” by and built on top of this substrate of higher-level priors. The combination of these effects would inevitably lead to a more “hybrid” form of attention (i.e., not only the one activated by the ongoing placebo/nocebo procedure). This hybrid attention then may affect the way information is captured and processed (i.e., the likelihood) and, in turn, the effect that is experienced (i.e., the posterior, Figure 3). In the aforementioned coffee example, one’s previous experiences with coffee, suggestibility, and energy levels will contribute to shaping the placebo-related priors (e.g., increase in stimulation) but may also influence the way one pays attention to the somatosensorial information.
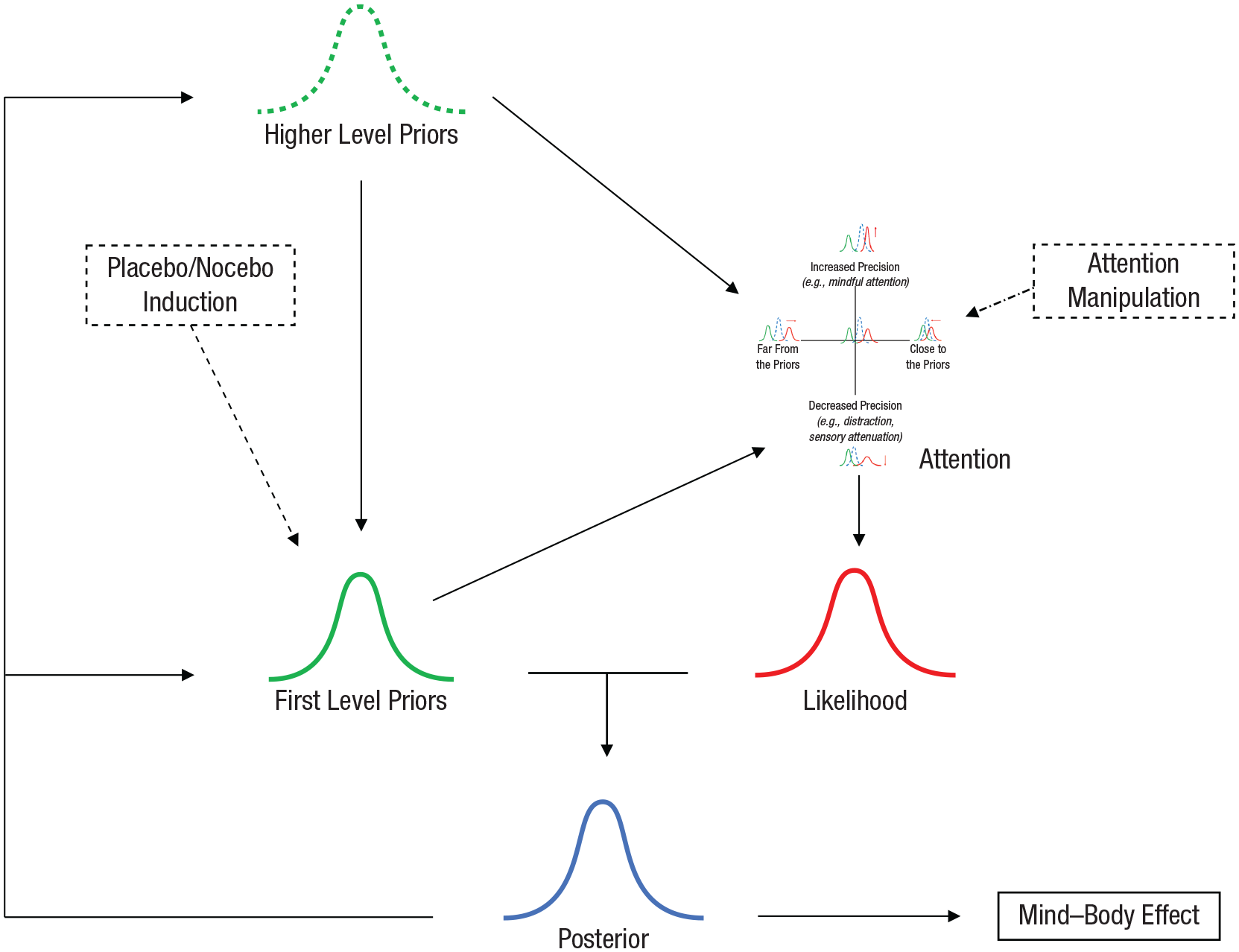
Interactions between priors, attention, and the likelihood in mind–body effects. A placebo/nocebo induction shapes specific expectations (first-level priors) that combine with somatosensorial data (likelihood) and may be updated into a posterior. This posterior can be the source of the mind–body effect, through an active inference principle. As depicted in Figure 2, attention can be oriented toward an improved/worsening precision and toward specific characteristics of the data. These attentive processes can be manipulated (e.g., in an experimental context) and, in turn, influence the likelihood. However, attentive processes may be influenced by previous experiences, individual characteristics, and beliefs (higher-level priors) and from the placebo/nocebo-generated priors. The process is characterized by a circularity because the posterior modifies the priors in a continuing updating procedure.
The role of the higher-order priors can be substantial for the promotion of placebo–nocebo effects, but a detailed review of their characteristics goes beyond the scope of this article. Previous studies have largely explored the role of expectations and described different individual characteristics and previous learning experiences related to these higher-level priors; however, limited information is available regarding the potential of attention manipulations in promoting different mind–body effects.
Conclusions
Over the past several decades, the scientific community investigating placebo/nocebo responses and other mind–body effects has contributed to outlining the impact of the priors (e.g., expectations and learning) on these phenomena. However, evidence focusing on the likelihood (i.e., sensory information) and the role of attention as a potential mediator of these effects remains largely unexplored. The hypothesis defined in this article suggests that particular ways of directing attention may shape these effects by either strengthening or downplaying them. Similar to exploring the role of predictive coding in the explanation of psychotic symptoms (e.g., Powers et al., 2017), empirical data to test the validity of this model are required. An empirical confirmation of the model, or potentially just the main hypothesis, entails that attention earn a spot among the main mechanisms (mostly referred to as the priors modification) that have already demonstrated effectiveness in shaping placebo/nocebo effects and other mind–body phenomena. Improved knowledge of the role of likelihood and attention will allow for better management and “control” of placebo/nocebo effects and mind–body phenomena, enhancing or minimizing them depending on the circumstances (e.g., reducing the impact of negative expectations about side effects or negative diagnosis). Furthermore, the focus on attention emphasizes the role of the individuals, who become actively engaged in the process of shaping their health and is no longer purely at the mercy of external circumstances.
Footnotes
Transparency
Action Editor: Timothy J. Pleskac
Editor: Klaus Fiedler
Author Contributions
The theoretical framework was developed by F. Pagnini, with the support of D. Barbiani and D. Phillips. All other authors collaborated on the development of specific parts of the idea, based on their expertise. All of the authors approved the final manuscript for submission.