
Abstract
Today, up to 88% of medical technology companies fail to deliver significant return to their investors. Clearly, the traditional stage-gate process employed in new product development is not dynamic enough, nor tactical enough, to provide a product’s success. The new product development process should address each stakeholder’s perspective (i.e. payers, patients, hospitals/healthcare systems, and governmental agencies) and generate data and corresponding messaging that speaks to them. Incorporating a global launch strategy, which is common today, amplifies the data burden when one considers each country’s constellation of stakeholder groups and regulatory requirements. Thus, launch strategies must map out total required stakeholder data needs before launch to capture efficiencies and lower total costs. This type of new product development process requires a unique team in place at the beginning of the product cycle. The Core Team must be an integrated, collaborative, flexible, cross-functional team that incorporates core strategic functions (Clinical, Regulatory, Legal, R&D, Reimbursement, Engineering, Sales and Marketing), but also has the ability to execute the tactical plans. The members’ differing perspectives inform the data-driven marketing and launch plans, claims matrices, key message development, competitive analysis, clinical publication strategy, and market conditioning plan. This article will address the gaps we have observed in the traditional stage-gate new product development process in the current healthcare landscape and will outline the marketing best practices we have used to bridge those gaps: creating an integrated customer engagement roadmap that fully aligns with a value-oriented global market and executing that roadmap with the cross-functional expertise of a Core Team.
Keywords
It has been our experience that the amount of data required to convince today’s stakeholders of a medical device’s value is exponentially greater than it was in the past. Previously, a company could launch and sustain a medical device rooted simply in a few regulatory-focused clinical endpoints, procedure-based billing, and marketing to a single stakeholder population (often clinicians); then, they could slowly generate clinical data and related messaging over time, if ever.
Today, the number of stakeholders participating in a product’s success has increased, and each stakeholder will determine a device’s value by data-supported messaging and claims that are specific and unique to each stakeholder’s perspective. Stakeholders may include patients, clinicians, government regulators, hospitals, and payers/reimbursement (i.e. private insurance, Medicare, Medicaid). Lastly, the data burden and complexity is further increased today because many get-to-market strategies are global, rather than restricted to the domestic market, and each country has its own constellation of stakeholders.
However, many products are developed using the linear stage-gate approach, 1 leaving gaps between the complexities of the external healthcare landscape and the often perfunctory and formulaic internal processes for new product development (NPD). It is our opinion that these gaps can be bridged by (1) creating value by early mapping of stakeholders’ messages/claims and the corresponding data needed to support them, and (2) early formation of a core cross-functional team that not only builds the messaging/claims matrix, but also leads downstream execution if the product moves forward. Early planning and capture of data desired by the various stakeholders can result in a value-differentiated product with a detailed plan on how to create that value during the product's lifecycle, in contrast to a product that launches with a simple clinical claim and a one-dimensional marketing message. Companies that plan for the components of a value-oriented product from the very beginning of the product cycle can be rewarded with an offering that (1) is attractive across multiple value-differentiated stakeholders, (2) has faster-to-market cycle times, (3) can deliver faster and more profitable growth, and (4) decrease costs to develop clinical data that go beyond regulatory claims.
Drawing on the authors’ collective 30+ years in the healthcare market, the article will examine the gaps in the traditional NPD process, and discuss an example of how to build and execute an integrated customer engagement roadmap that can guide product development and launch into a value-oriented global market.
Observed gaps in the traditional medical device NPD process
We have observed that, in general, the medical device NPD process can be characterized as: focused on a single stakeholder/customer, defined by a clinical benefit limited to regulatory endpoints, and developed with a linear stage-gate approach without a full lifecycle plan.
This characterization can apply to smaller companies where the development path for a new medical device often begins with a single product concept aimed at a handful of key stakeholders, usually a surgeon, implanting physician (if it is an implantable device), or a managing clinician. The value proposition of the device may not go beyond a primary clinical benefit (i.e. an implanted medical device that improves the cardiac output of a patient with heart failure). Any supporting marketing plans, claims, key messages, and/or publication plans are often centered on this primary clinical benefit and not much more. After launch, the product would likely settle into a niche category relatively quickly without much room to grow. Product development at smaller companies often follows a linear stage-gate approach: build prototype, do preclinical testing, proceed to human trial, get FDA approval, scale-up manufacturing, and so forth.
According to one report, 88% of medical technology companies fail to deliver significant return to their investors. 2 Focusing on traditional “phases” or “gates” may be one reason why these models are failing. Companies have become hyperfocused on regulatory approval milestones without planning at the outset how they will move beyond “safe and effective” in the most time-saving and cost-effective way possible.
Larger companies may have dedicated NPD teams, often bolstered by third party expert consultants, that develop new product plans. These teams usually incorporate a more robust consideration of the potential market, perhaps including general analyses of reimbursement, market size, and potential gaps in the market. However, the plan still relies on generic tech innovation/market need (i.e. push/pull) strategies and could be biased toward generally accepted perceptions of the market potential for a given product. Most importantly, the plans generated in this situation are often not tactical. Plans produced by dedicated NPD teams often do not detail the problem of “exactly what to do, exactly when to do it, and exactly who does it.” Thus, after leaving the NPD team, the product and plan may flounder in the unique functional areas of a large company, as these areas often lack cross-talk and are isolated by corporate silos. Without a detailed plan, each silo is left to problem solve and make decisions from the perspective of their own departmental culture and narrowly defined processes, not knowing those decisions’ downstream effects for the product.
Opportunity costs of the traditional medical device NPD process
A survey of over 200 medical device companies estimated a total cost of $31 million (USD) to bring a low- to moderate-risk device (i.e. FDA 510(k) product, or equivalent) from concept to market, whereas high-risk devices (i.e. FDA Class III Premarket Approval (PMA) products) averaged $94 million (USD), not including the cost of obtaining reimbursement approvals or sales and marketing-related activities. 3 In addition, it was found that only one in four venture capital (VC) funded-medtech start-ups ultimately find success. 3 Those investing money and resources to develop an expensive medical device concept—VC investors for start-ups and traditional institutional investors for large companies—will want to lower their risk, reduce the time to regulatory approval (which in the U.S. for an FDA PMA product can be as long as 54 months 3 ), and have the broadest possible market commercialization for the highest possible profit margin.
The high cost and risk of new medical device development may be due in part to the gaps in the traditional NPD process, which leaves (1) the process vulnerable to internal inefficiencies, confusion, and a changing external environment and (2) the product vulnerable to the limited value and marketing difficulties of a device that does not go beyond “safe and effective.”
If an organization has not thought through how their product’s value will be seen by different stakeholders (including how those values may change geographically in a global market), how will their product be differentiated in the market even if it is meeting its clinical goals? In the earlier example of an implanted medical device that improves the cardiac output of a patient with heart failure, potential avenues for creating that differentiation could include:
Can it also lower the overall cost of care in the heart failure population for a payer like Medicare? Can it reduce 30-day rehospitalization rates? Can it improve the efficiency of clinics managing heart failure patients? Can it improve the quality of life for the patient? Will it improve the clinicians’ practice and bottomline?
Anticipating these potential benefits of a product can move the product from “low value” (i.e. a single clinical benefit targeting a single stakeholder population) to one of “high value” (i.e. a diverse array of benefits targeting diverse stakeholder populations). Although it is the same product, the “low-value” scenario is risky because it depends on adoption by a single customer (clinicians), whereas the “high-value” scenario spreads its risk by appealing to not only clinicians, but also payers, hospitals, clinics, and patients. Anticipating these benefits enables a company to plan for and collect needed data for value creation earlier in the process rather than later, and frequently in parallel with regulatory required endpoints at a fraction of the cost.
Creative thinking about potential stakeholders and getting detailed stakeholder input at the beginning of the NPD process will help avoid the costly rework of capturing missed data. A few expensive examples for our cardiac product could include:
Tracking down patients after a pivotal clinical trial has completed its follow-up phase because several large payers for reimbursement approval require data on a particular patient subgroup in the clinical effectiveness model. The additional expense may double what was already invested because once a patient has left a study, they are often hard to track down. Given that the cost for clinical investigation trials for high-risk device approval is estimated at $40 million (USD),
3
this data requirement could quickly escalate costs. In addition to the financial cost, there is the cost of lost time to market as data would need to be captured through a survey or some other form of clinical data gathering, which may take several months to compile and analyze. Funding a costly postapproval time and motion study with several managing clinics because the use of the medical device frustrates established clinical protocols. Adoption and referrals for the product have slowed because clinicians believe it is a bottleneck to handling or expanding their patient load.
Thus, early planning can save time and money by adding a few secondary data endpoints to a clinical study rather than funding numerous postmarket studies. By anticipating the needs of a diverse potential stakeholder population for a given device, companies can avoid developing products with limited value (“low-value” products) and may avoid costly downstream data collection activities. It is our opinion that the traditional NPD medical device process creates missed opportunities to develop the data to support fully differentiated, “high-value” products more efficiently and at a lower cost.
Understanding stakeholder populations and how they view “value”
A medical device’s potential value can be defined more broadly than the “safe and effective” bar set by governmental regulatory agencies if one considers the many stakeholders key to a device’s success in the marketplace. How differing stakeholder populations determine value for medical devices is a topic of intense research4–6 and is beyond the scope of this paper. However, to reach beyond the threshold of “safe and effective,” we will briefly discuss general value perspectives for patients, hospitals and integrated healthcare systems, payers (private and government run), and governmental healthcare agencies.
For patients, value may mean more choice, physical freedom, a lower out-of-pocket cost of device and related clinical services, and/or a better quality of life. Patients have become consumers, as they have online access to information (correct and incorrect) about procedures, prices, hospital quality ratings, and health outcomes data, as well as have an online platform to share product and provider reviews that can drive brand preferences.
7
More than ever, patients are price shopping and demanding higher levels of service—tactics which are usually reserved for the consumer goods industry—to reduce their out-of-pocket costs and make their lives easier
8
(Nextech Blog).
For payers (private and government run), value may mean lower product and service costs, better health outcomes for entire patient populations, and lower overall delivery costs per patient. For certain products, payers continue to need data to support if a product is “reasonable and necessary” and how it impacts long-term patient health.
For Governmental Healthcare Agencies, such as Medicare in the U.S. and the National Health Service in the U.K., value means balancing cost with improving health service delivery and outcomes at a national scale, using health economics data and strategies (alternative payments, formal value analysis, and efficiency tracking systems). NPD teams will need to anticipate the data requirements to support health economic claims.
What is common among stakeholders is the need for data to support messaging that addresses their needs. Thus, launch strategies must focus on securing data that supports stakeholders’ needs and outcomes-based reimbursement before launch; this requires that value propositions, clinical claims, marketing plans, and messages are rooted not only in regulatory clinical endpoints, but also broad population-based health outcomes, clinical and procedural efficiency, and patient quality of life improvements. These data are critical to building an integrated customer engagement roadmap that guides NPD through a process that “starts with the end in mind.”
Building an integrated customer engagement roadmap
An integrated customer engagement roadmap is data driven, specific, tactical, and unique to the company and the medical device in question. It is an early, clear vision for desired value propositions that are incorporated into the company’s and product’s marketing and launch plans. It captures and distills a device’s entire potential market through numerous stakeholders’ and/or customers’ needs. The process of building an integrated customer engagement roadmap will help identify opportunities early and help mitigate risk before resources have been spent.
4
First: To analyze early product concepts, a matrix is populated with device-specific claims and marketing messages that address each stakeholder’s needs
Second: Determine the resources needed to support each message, the potential benefit of each message, and identify possible challenges
Using the estimated costs and revenue/market share predictions, the messages and claims are evaluated and chosen for the most likely path to a successful launch and a product with maximized overall value. These “high value” messages and claims and their associated data/content requirements can be used to create a strategic plan (operations, budgets, timelines) and a tactical plan (for each functional area, a detailed action plan to generate or process the data or content needed to support the high value messages and claims). Using our previous example of a hypothetical cardiac product, Table 1 shows what a “high value” message and claim matrix may look like, organized by stakeholder needs. The same messages and claims matrix can be reorganized and visualized by data collection activity, showing which messages or claims will be supported by each preclinical, clinical, or bench study. Challenges for strategic and tactical plans may include lining up funding cycles with expensive clinical trials, incorporating the time needed to generate data, assessing the probability that a study will work, and obtaining access to competitors’ material for comparison studies.
Example of a medical device “high value” message and claims matrix produced by a cross-functional team during initial planning for product development

In practice, the process of creating an integrated customer engagement roadmap may take 10–20 people three months to complete, and an initial matrix of 20–40 messages and claims may be narrowed by 30–50% by the end of the process. Using the roadmap during NPD, the end product is a path for commercial success for a device whose true cost to achieve that success is clear. This is in contrast to the linear stage-gate approach, which often only defines the commercial opportunity for a device and its basic regulatory classification, leaving the actual details and decision-making up to other tactical functional areas in the company.
In terms of planning, if NPD were a road race, it is the difference between one team having a handwritten note with a list of cities to visit (traditional NPD process) versus another team with a map with details of route, destinations, potential hazards, driver rotation, and speed limits (integrated customer engagement roadmap). Which team will get to the finish line fastest?
Executing an integrated customer engagement roadmap: Role of the Core Team
Execution of the tactical action plan is where the true challenges are in NPD. In our approach, the cross-functional team that prepared the integrated customer engagement roadmap will be the same team that leads and executes the tactical plan through to product launch. Thus, each team member must be carefully chosen at the outset for both functional area of expertise and working style that includes both collaboration and leadership qualities. Many large organizations do not include experts from the tactical execution sides of their business when carrying out the NPD process, or in the case of smaller companies, may not have access to them in-house.
Team characteristics and responsibilities
The team should be an integrated, collaborative, flexible, cross-functional team that incorporates core strategic functions (i.e. Clinical, Regulatory, Legal, R&D, Reimbursement, Engineering, Sales and Marketing). Depending upon the device, additional or specialized functional areas may be needed, such as Software Engineering for an app-enabled smart device, or Patient Support/Technical Services if the device is consumer oriented and will require aftermarket care and support. Thus, this “Core Team” represents all key business functions that will touch the device and the expectation is that its members are responsible for, and dedicated to, the development of the new product; they are empowered and incentivized to drive toward success efficiently (Figure 1).
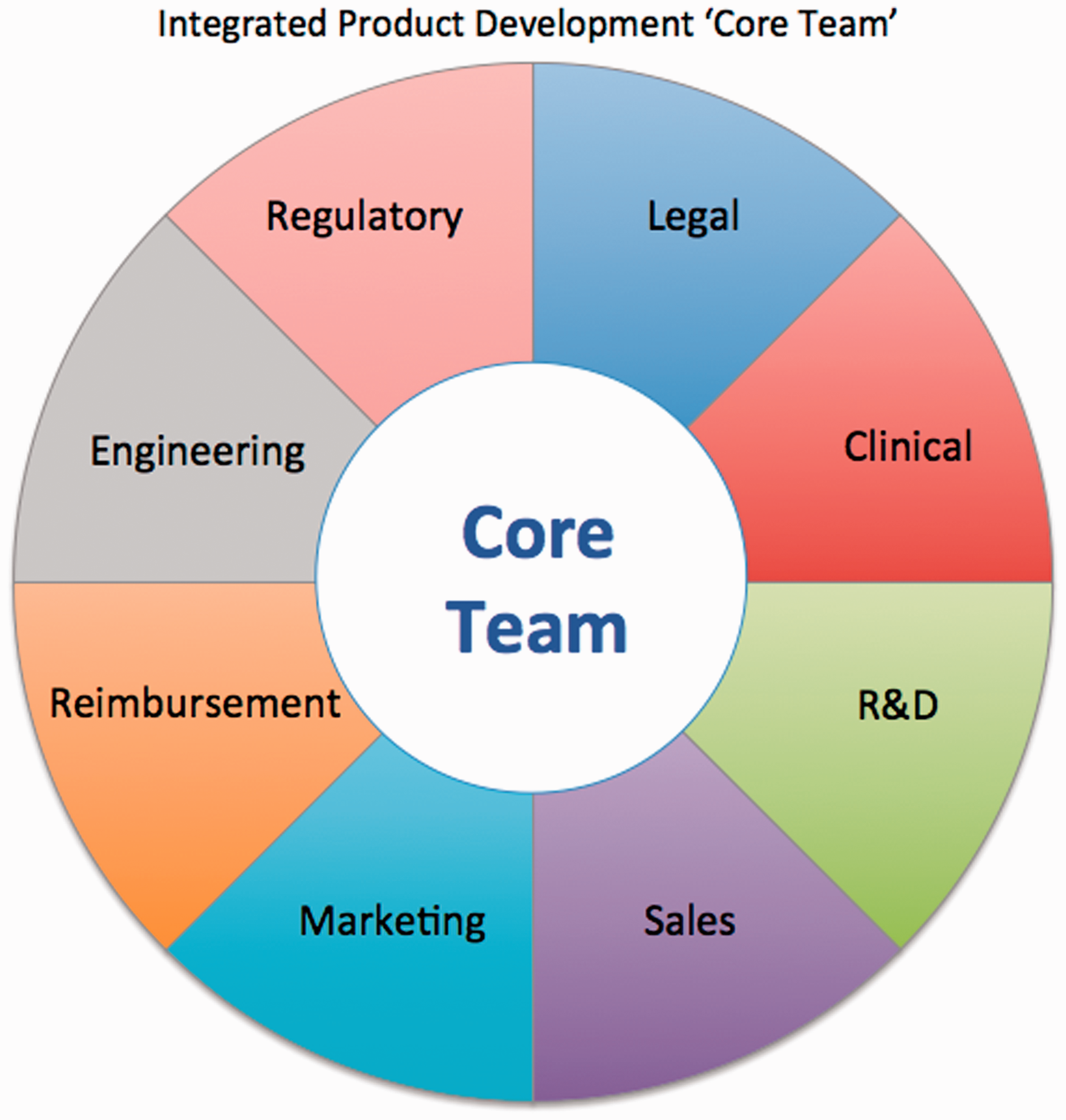
Integrated product development “Core Team.” Core Team members of a strategic model for medical device launch represent the key business functions needed during the entire product development cycle. Their input and planning at the initial stage of product development de-risk the endeavor and ultimately save time and money.
Members of the Core Team must be strategically oriented, creative and flexible individuals who can go beyond operations. They need to understand the whole commercialization lifecycle, even if they are not experts in all areas. A traditional operations person, while very good at their day-to-day job, may lack the cross-functional knowledge, creativity, and flexibility necessary to make an effective contribution in this approach. Some organizations may need to use strategic consultants who have a proven track record of execution to fill gaps in their Core Team, ensuring critical functional areas are not missed or a person with the desired working style is on the team. By the time that the Core Team has finished building the integrated customer engagement roadmap, they are in alignment with each other and each understands the “big picture” as well as the tactical details needed from their functional area of expertise. Each member has the expertise and authority to accelerate execution as the NPD process moves to operations.
In the linear stage-gate approach to NPD, both small and large companies have challenges in execution. In a small start-up, staff may wear multiple hats, such as a single person managing Clinical, Regulatory, and Quality. This can have the benefit of the person thinking cross-functionally about a product’s value to numerous stakeholders. But the downside during execution is that the person may be distracted by immediate needs (i.e. compliance and supplier audits) and cannot act proactively on parallel activities (i.e. clinical trial initiation). In larger, more established companies, functional areas are typically very established and separate, creating silos each with their own culture and language. Often these “siloed” functional areas hinder cross-talk and cooperation about a new product, often in an environment where staff are stretched thin. A clinical leader may be running seven or eight clinical studies simultaneously, or a regulatory leader may have a portfolio of 20+ products to keep in compliance around the world; their attention will not be focused on accelerating a new project’s launch.
With the Core Team approach, the new product has a champion within each functional area to shepherd it through obstacles or “translate” specific operational needs that are important within the broader context of the project. Thus, once the device enters the execution phase within each functional area, a Core Team member can make decisions that do not disrupt the “big picture.” This approach may require additional support resources, but the risk/benefit of a new product’s success overwhelmingly justifies this cost in the majority of cases.
Periodically, the original integrated customer engagement roadmap is reassessed by the Core Team to help guard against “alignment drift” within the team or the project. If needed, the roadmap can be proactively adjusted to align with new opportunities, new information discovered about stakeholders, or changes in the external/internal environment such as changes in Medicare rules or departmental budgets. Thus, when challenges arise, time is not lost and money can be saved because (1) the Core Team is responsive and (2) the roadmap tool captures the entire NPD process dynamically. Success in this era of complexity begs for a structured process for partnership across all departments and positions. It’s crucial that stakeholders are identified, goals are confirmed and requirements are agreed upon at kickoff. The expectation that teams work together early and often also must be established and accepted by everyone involved.
11
(MedCity News)
The benefits of using the integrated customer engagement roadmap approach
De-risks failure to launch
Because many aspects of the process to commercialize a medical device are independent of the company’s control (e.g. FDA approval), having a strategy to streamline and accelerate the controllable aspects of NPD will help de-risk the endeavor. Unlike the linear stage-gate approach, the roadmap approach de-risks and accelerates product development by understanding stakeholder needs and identifying and addressing challenges before design and data collection. The roadmap and its message/claims matrix provide enough data to be both strategic and tactical from the outset, allowing a dynamic accelerated approach versus a “Go/No Go” linear stage-gate approach. Development failure is further de-risked by the involvement of the Core Team, which can sense and respond to changes in the environment in a proactive manner throughout the NPD process. This is in contrast to the standard stage-gate approach where an NPD team may put the process in motion but is not actively engaged during execution, leaving what is often a single product manager to move a product’s development through each functional area in the company.
De-risks commercial vulnerability
The integrated customer engagement roadmap approach assumes the strategic goal of offering a fully differentiated product to the market. A simple clinical claims matrix used for commercialization (i.e. “safe and effective”) does not guarantee commercial success for a device, nor does it capture the true cost of generating data for sophisticated messaging; a device that enters the market as simply “safe and effective” is vulnerable to any competitor that can offer more value than modest clinical claims. Establishing a multistakeholder, value-driven plan for marketing and launch before clinical studies are even begun allows for de-risking during the development process, leading to a maximized return on investment.
Provides an efficient NPD process
While many investors hope to make a return on their investment in as little as 2–3 years, bringing a new medical device to market can take a decade or more. 12 The integrated customer engagement roadmap makes the NPD process more efficient by requiring members of the Core Team to make decisions and come into alignment at the beginning of the process. It allows proactive planning versus reactive scrambling at each challenge or milestone. For example, clinical trials can be designed to incorporate data collection for numerous and overlapping messages; early publication planning can condition the market before launch; and, while minding appropriate PMA promotional restrictions, engagement with KOLs and physician partners can generate early clinical adopters, accelerating market adoption at launch.
Uncovers unique opportunities in the market
The integrated customer engagement roadmap provides an unbiased evaluation of the potential marketplace by (1) challenging an integrated Core Team to creatively consider numerous stakeholders’ needs specific to the product, and (2) quantifying each message with the cost of data to support the message balanced by the potential market benefit. The process to create the integrated customer engagement roadmap is reproducible across product types, but each roadmap is unique and specific to the product, the company, and the marketplace.
Challenges and perceived pitfalls of using the integrated customer engagement roadmap approach
The main challenge of the integrated customer engagement roadmap approach is the need for funding early in the process to collect data needed to support marketing messaging. However, budget allocation for marketing studies is not typically available until after the product is developed and on a regulatory approval trajectory. The integrated customer engagement roadmap approach could potentially disturb an organization’s established business practices, such as annual budgeting and internal product review boards. These are significant internal barriers for the Core Team to address, which is why team members need to be seasoned, strategically oriented, and have formal authority and real power to make decisions.
In VC-supported companies, the funding cycles are also misaligned with the integrated customer engagement roadmap approach. Most start-up companies rely on discrete phases of capital that drive a very specific activity, such as an animal study or a human clinical trial. Thus, at the beginning of the NPD process a start-up may need to communicate with their VC investor partners that the integrated customer engagement roadmap approach will de-risk their investment, but it will also require a larger percentage of the investment upfront.
Another challenge to the integrated customer engagement roadmap approach is the perception that it is slowing things down or losing focus by building a fully integrated roadmap before the device is fully developed. This may be because companies often begin a marketing roadmap process late in the product development cycle and without an established Core Team, resulting in a disorganized and inefficient experience. When implemented correctly, the upfront investment of money and time is balanced out by a fully differentiated and high value device, downstream cost savings, and the ability to accelerate to launch.
Lastly, a fully developed integrated customer engagement roadmap at the beginning of the NPD process may be seen as restrictive or limiting as compared to the linear stage-gate approach. However, the Core Team continually modifies and adjusts the roadmap as conditions require. They can easily and quickly modify the plan because they are the ones who built it, understand it, and will execute it. In addition, by early integration, the Core Team can be sensitive to, and proactively address, environmental changes that can slow or derail a product’s development, such as unexpected clinical trial results, regulatory rule changes, new laws requiring changes for payers and hospitals, or changes in the competitive landscape. Thus, early changes can be made if necessary to handle future challenges for the device.
Conclusion
In our experience, we have seen the linear stage-gate approach to NPD result in product development derailment or more often, launch of a “safe and effective” product that is soon a “me too” undifferentiated product in the competitive landscape. This failure often stems from the very initial steps during NPD: (1) the early message marketing matrix was limited to a single stakeholder’s value (regulatory clinical claims), or (2) although an initial differentiated product plan was developed, the tactical execution person or team did not have the integrated cross-functional expertise to effectively or efficiently manage challenges or make decisions within the context of the “big picture.”
The integrated customer engagement roadmap, when built at the beginning of the NPD process and executed by a cross-functional, integrated Core Team, will:
Identify all stakeholders and the device-specific marketing messages that would address their unique views of “value” to create a differentiated product in the marketplace. Contain enough information so that an unbiased list of “high value” marketing messages (not just clinical claims) can be used to create strategic and tactical plans for NPD, including a budget and timeline for data studies (e.g. preclinical, clinical, health economic), and communications and marketing (e.g. publication plan, KOL engagement strategies, marketing strategies). Empower members of the Core Team to become the champions of the device’s NPD process within each functional area, while working collaboratively to sense and respond to internal and external challenges.
We have seen this approach lead to successful medical device launches from idea to 510(k) approval and commercialization in as little as nine months. We believe that research and testing of the outcomes of our integrated approach, along with traditional NPD methods, is warranted.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.