
Abstract
Kidney transplantation restores fertility in patients with end-stage renal disease, with many successful pregnancies after kidney transplantation being reported. However, there are little data regarding pregnancy in women transplanted under modern-era desensitisation protocols that utilise rituximab, plasma exchange and intravenous immunoglobulin, including ABO-incompatible transplants. Pregnancies in ABO-incompatible recipients can pose new challenges from an immunological perspective. Here, we report a case of successful pregnancy using in vitro fertilisation, in a renal transplant recipient who underwent desensitisation two years prior, that included use of rituximab and plasma exchange to receive an ABO-incompatible transplant from her husband and subsequent father of the baby. We believe this was the first case of successful pregnancy after ABO-incompatible kidney transplantation in Australia and New Zealand. This case also highlights the difficulties faced in conception following transplantation and demonstrates that in vitro fertilisation utilising ovulation induction can be successfully utilised for conception in this cohort. This recipient also had gestational diabetes, worsening renal function and preterm delivery which are important complications often seen in pregnancies of solid organ transplant recipients.
Introduction
End-stage renal failure (ESRD) in women impairs fertility. Transplantation restores fertility, providing opportunity for parenthood. Successful pregnancies have been reported in transplant recipients, with a live birth rate of over 70%. 1 – 8 However, there is reduced fertility and increased incidence of preterm delivery, intrauterine growth restriction, hypertension, pre-eclampsia, and gestational diabetes mellitus (GDM) compared to the general population. 3
Few pregnancies have been reported in women transplanted under modern-era desensitisation protocols, including ABO-incompatible (ABOi) kidney transplantation (KTx). 6 Pregnancies in ABOi transplant recipients pose new immunological challenges, above the standard risks for transplanted women. In vitro fertilisation (IVF) is rarely used in transplanted women but has successful outcomes. 9 We report a case of successful pregnancy after IVF in a woman with ABOi-KTx whose husband was donor and father of the baby. This case reflects the changing face of pregnancies post-transplantation.
Case report
A 29-year-old woman, with adult polycystic kidney disease, underwent living-donor KTx from her husband. The recipient HLA allele mismatches were 2, 1 and 2 at classes A, B and DR B1 respectively. Class C HLA was not tested. There were no recipient anti-Human Leukocyte antigens (HLA) antibodies when tested three months before undertaking transplantation (Luminex, Immucor-diagnostics-CT). Donor was blood-group A+ (subtype A2); and recipient O+ with anti-A2 titre 1:128. Pre-transplant desensitisation and immunosuppression are shown in Figure 1. Baseline creatinine was 1.2 mg/dL (105 µmol/L) with an estimated GFR of 76 mL/min/1.73 m2, with no rejection and normal protocol biopsy at six months. She had no proteinuria, hypertension or new-onset diabetes and therefore was not on an angiotensin-converting enzyme inhibitor.
Desensitisation protocol and immunosuppressive agents used.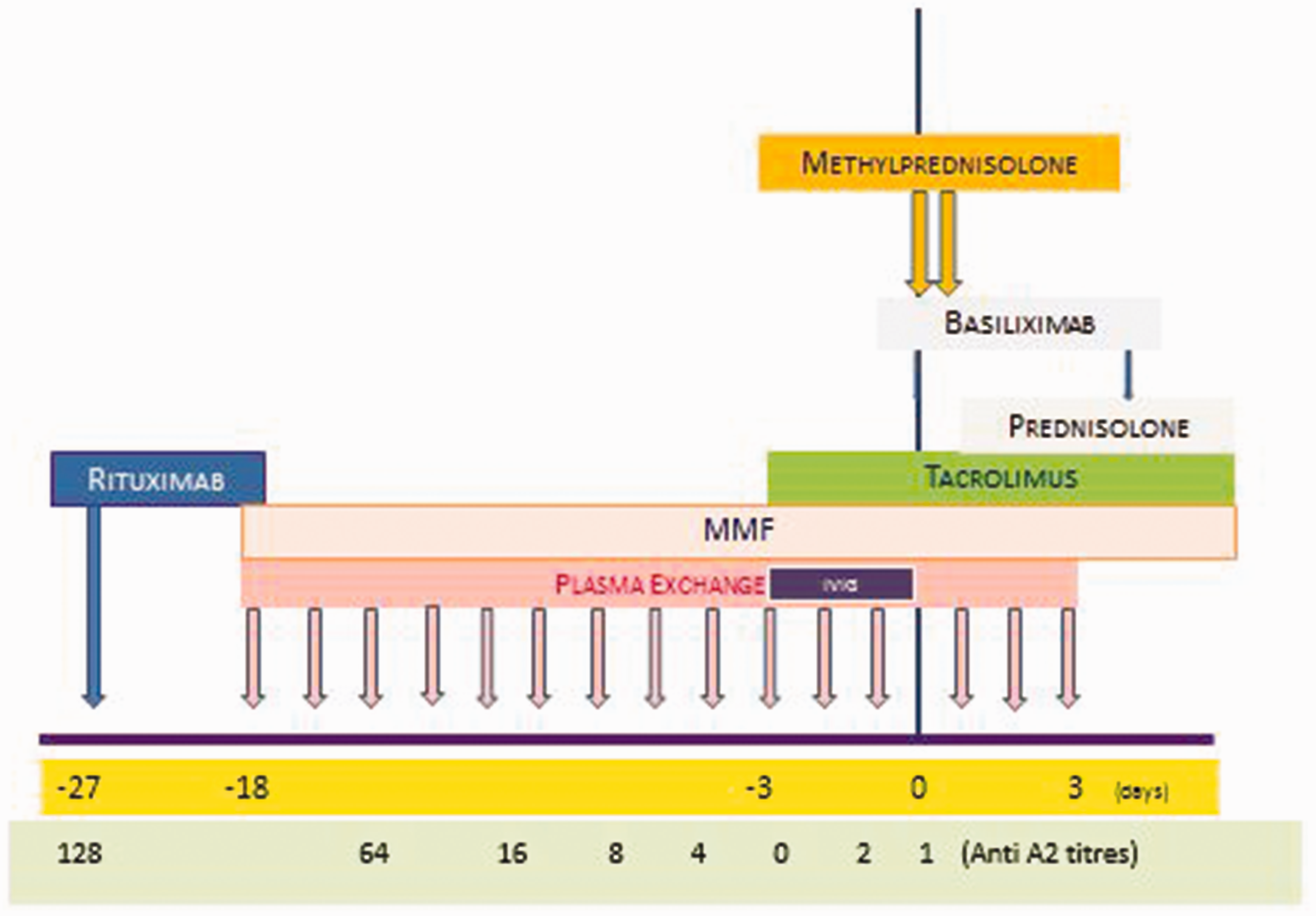
The recipient had no prior pregnancy. At one year post-transplant, she expressed a desire for pregnancy. Pre-pregnancy counselling was undertaken and risks including hypertension, pre-eclampsia, preterm delivery and its potential long-term sequelae for the baby, gestational diabetes, intrauterine growth restriction and loss of maternal renal function were explained to patient and family. Mycophenolate was switched to azathioprine. Tacrolimus and prednisolone were continued. Renal function was closely monitored following the switch for four months and remained stable. Donor-specific antibodies (DSAs) were not detected. Induction with goserelin followed by IVF with single-embryo transfer, resulted in conception two years post-transplant. She developed hypertension (blood pressure (BP) 140/90 mmHg) at 12 weeks of gestation and was commenced on methyldopa 500 mg twice daily. There was a progressive increase in requirement for tacrolimus to maintain levels over 5 ng/mL (peak dose 15 mg twice daily). Renal function remained at baseline levels without proteinuria. Anti-A2 titres were consistently less than 1 : 4 against donor red blood cells. BP was subsequently well controlled at 110/70 mmHg on methyldopa and serum creatinine remained stable at 1.2 mg/dL (105 µmol/L). Amniocentesis was not obstetrically indicated and fetal blood group was thus not determined.
At 30 weeks of gestation, serum creatinine was 1.7 mg/dL (149 µmol/L). Glucose tolerance test (GTT) revealed GDM. Anti-A2 titres remained low and no DSA was detected. Tacrolimus level remained stable between 5 and 6 ng/mL. Gestational diabetes was treated with dietary modification and protaphane insulin (twice-daily regimen). Ultrasound of the graft showed no abnormality. Markers for pre-eclampsia including liver function tests, platelets and blood film were unremarkable. There was no proteinuria. Ultrasound showed normal growth with an estimated fetal weight of 2050 g. Betamethasone (12 mg/dose × 2) was given to optimise fetal lung maturity. Delivery via caesarean section was undertaken at 34 weeks of gestation, because of worsening graft function (serum creatinine 2.1 mg/dL (184 µmol/L)). The female infant weighed 2350 g (50–75th centile), had no congenital abnormalities and was blood group O. Transplant biopsy undertaken at nine weeks postpartum showed focal thrombotic microangiopathy (TMA), despite no clinical features of pre-eclampsia. There was also moderate background scarring and tubular atrophy. However, there was no evidence of TMA in the blood film, with no rise in lactate dehydrogenase and normal serum haptoglobin. Post-partum anti-A2 titres were not elevated and DSA remained negative. At two months post-partum, she ceased breastfeeding and resumed mycophenolate mofetil. Repeat GTT was normal. At four months, creatinine was 2.1 mg/dL (184 µmol/L). Creatinine at two years was 2 mg/dL (176 µmol/L).
The weight of the infant was followed up for two years and remained normal.
Discussion
Pregnancy occurs more commonly after KTx than in dialysis cohorts.2,5 Pregnancy rate reported in Australia and New Zealand (ANZ) transplant recipients is 20/1000 person-years. 5 Live birth rate among ANZ transplant recipients has improved over time to 88%. 7 Despite this, pregnancies remain high risk due to increased rates of maternal and fetal complications, particularly pre-eclampsia (in 30%) and prematurity (over 50%).5,7
To our knowledge, this is the first case of pregnancy after ABOi-KTx reported in Australia and New Zealand. This case highlights the difficulties faced in conception following transplantation and demonstrates that IVF can be successfully utilised for conception. This patient also had GDM, worsening renal function, gestational hypertension and preterm delivery which are complications that are increased in transplant recipients.1,3,5
A major concern for KTx-recipients is worsening of renal function in pregnancy.5,10 In patients with pre-pregnancy serum creatinine >1.7 mg/dL (149 µmol/L), a trend towards increased post-pregnancy serum creatinine was identified. 10 In the case described here, pregnancy did result in permanent decline in the estimated glomerular filtration rate, despite the pre-pregnancy serum creatinine being less than 1.7 mg/dL.
In KTx recipients, 35–50% babies are born preterm and mean birth weight is below 2500 g in many reports.3,11,12 Preterm birth by caesarean section delivering a baby that is small for gestational age is common.13,14 Although most children attain normal growth after 48 months, 14 concern has been raised about possible hypertension and renal disease in adulthood due to reduced nephron mass. 15 This observation is consistent with the Barker Hypothesis of in utero programming of chronic disease. 16 The clinical significance of an isolated TMA in the renal graft in association with pregnancy is unknown.
Antibody-mediated rejection (AMR) after ABOi-KTx is common within the first 10 days post-transplantation, until accommodation is established. 17 These patients undergo desensitisation with aggressive immunosuppression to facilitate allograft acceptance. Pregnancies after ABOi-KTx have been reported in four cases, although outcomes in this rare group were not separately discussed. 6 There is little else in published literature regarding pregnancies in this group, and no data relating to the modern era of immunosuppression which utilises agents such as rituximab, plasma exchange and intravenous immunoglobulin. Maternal exposure to fetal cells normally promotes immunological tolerance to fetus. In pregnancies after ABOi-KTx, exposure to fetal blood when fetal and donor blood types are same, poses a second immunological challenge, acting as ‘double-allograft’. In our patient, fetal blood group was unknown until after birth. If the fetus had blood group A2, crossover of blood at maternal–fetal interface in placenta and at time of delivery could have re-exposed mother to A2 cells.
DSA and AMR after pregnancies have also been reported in the literature. 18 Our patient showed no anti-paternal DSA. Killer-immunoglobulin-like receptors (KIRs), expressed by uterine-NK cells, are in direct contact with the invading placenta. Trophoblasts express maternal and paternal HLA-C allotypes and can interact with KIRs. Allo-recognition of paternal HLA-C by maternal KIR can influence trophoblast invasion and vascular remodelling, with subsequent effects on placental development. However, donor and recipient HLA-C haplotypes were not specifically tested in this case. 19
Although transplantation restores fertility, this is consistently lower than in the general population.20,21 Small numbers of successful pregnancies using IVF after KTx have been reported in literature.22,23 The location of the transplant can be a potential problem for oocyte retrieval. Care should be taken to avoid ovarian hyperstimulation, with its resultant fluid and electrolyte disturbances. 24 It is also good clinical practice to transfer a single embryo to avoid risk of multiple pregnancies. 25
In conclusion, this report of a successful pregnancy in an ABOi-KTx recipient following IVF highlights the immunological complexities, where the donor fathered the child, in addition to the frequent complications seen in pregnancies of renal transplant recipients.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Written consent from the patient was obtained.
Guarantor
NR.
Contributorship
Nitesh Rao – Involved in patient care, preparation of manuscript Chris Wilkinson – Involved in patient care, preparation and suggestions to write the manuscript Mark Morton – drafting the article and critically revised the article Greg D Bennett – drafting and revision of the article Graeme Russ – drafting the article and critically revised the article Toby P Coates – Involved in patient care, drafting the article and critically revised the article Shilpa Jesudason – Involved in patient care, preparation of manuscript
Consent has been taken from all the authors before submission.