
Abstract
Pruritus is a common dermatologic complaint during pregnancy. Pruritus is reported by 23–38% of women during pregnancy, and 2% report severe pruritus. In addition to interfering with sleep and reducing overall quality of life during pregnancy, pruritus may be the first, or only, symptom of an underlying disorder that may impact maternal and fetal outcomes. It is therefore critical for all providers caring for pregnant women to be familiar with pregnancy-specific and non-specific conditions associated with pruritus to most effectively manage this unique population. In this review, we discuss clinical classification of pruritus, a practical approach to the differential diagnosis of pruritus in pregnancy, and focus on updates in the clinical features, diagnosis, management, and prognosis of pregnancy-specific causes of pruritus.
Introduction
Defined as “an unpleasant sensation that provokes the desire to scratch,” pruritus is a common dermatologic complaint. 1 As much as 16% of the general population reports chronic (lasting longer than six weeks) pruritus within the past year and 22% reports chronic pruritus over their lifetime.1,2 Interestingly, women are more likely to experience chronic pruritus in their lifetime, with 23–38% of women reporting pruritus during pregnancy, and 2% reporting severe pruritus.2–5
While the exact mechanisms are incompletely understood, physiologic mechanical, immunologic, and endocrinologic changes during pregnancy may exacerbate pruritus.5–7 Mechanical forces on the skin from abdominal growth and edema may stimulate pruritus in pregnancy.6,8 Modulation of the maternal T-helper type 1 (Th1) and T-helper type 2 (Th2) balance is thought to contribute to worsening of Th2-mediated diseases such as atopic dermatitis, and improvement in Th1-mediated skin diseases, such as psoriasis during pregnancy. 9 Increase in the quantity of, and effects of sex hormones on, mast cells, mediator release, and immunoglobulin E (IgE) production may also play a role.
In addition to pruritus interfering with sleep and reducing overall quality of life during pregnancy, it may indicate systemic disease. 5 During pregnancy, pruritus may be the first, or only, symptom of an underlying disorder that can impact maternal and fetal outcomes. It is therefore critical for all providers caring for pregnant women to be familiar with pregnancy-specific and non-specific conditions associated with pruritus to most effectively manage this unique population.
In this review, we discuss clinical classification of pruritus, a practical approach to the differential diagnosis of pruritus in pregnancy, and focus on updates in the clinical features, diagnosis, management, and prognosis of pregnancy-specific causes of pruritus.
Evaluation
An essential component of patient evaluation is the presence or absence of primary skin lesions (Table 1). Primary skin lesions originate from the causal disease and generally signify a dermatologic disorder. 10 In contrast, secondary lesions are reactive skin changes (i.e. excoriations, lichenification, hyperpigmentation) provoked by skin manipulation (i.e. scratching, rubbing) in response to pruritus. Pruritus in the absence of skin lesions, or with only secondary skin lesions, should raise suspicion for systemic, neurologic, or psychogenic causes of itch. 10 Other clinical characteristics such as location of pruritus or lesions (localised vs. generalised), lesion morphology, timing of onset relative to pregnancy, as well as aggravating and alleviating factors can assist in diagnosis. We propose a practical algorithmic approach to evaluation of the cause of pruritus in pregnancy (Figure 1).
Pruritus groups differentiated by presence or absence of primary skin lesions.
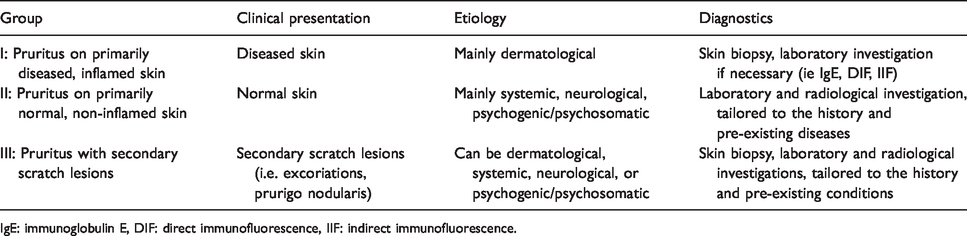
IgE: immunoglobulin E, DIF: direct immunofluorescence, IIF: indirect immunofluorescence.
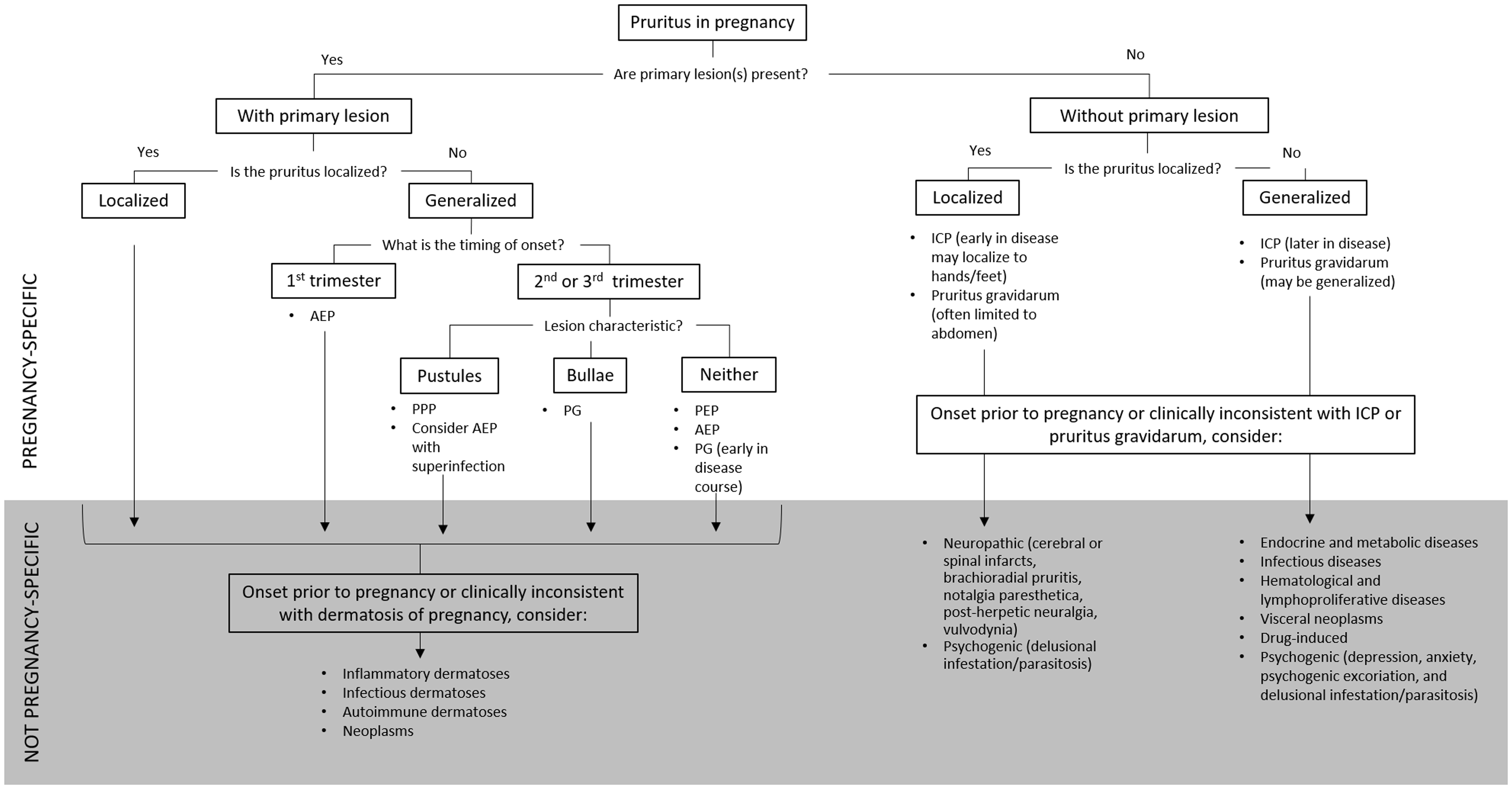
Algorithm for assessment of etiologies of pruritus in pregnancy. AEP: atopic eruption of pregnancy, PPP: pustular psoriasis of pregnancy, PG: pemphigoid gestationis, PEP polymorphic eruption of pregnancy, ICP: intrahepatic cholestasis of pregnancy.
Generalised pruritus with primary skin lesions
Pregnancy-specific etiologies
The dermatoses of pregnancy represent a heterogeneous group of poorly defined pruritic skin diseases unique to pregnancy. 11 They have been variably described and classified over the years, contributing to confusion in clinical care and research. Most recently, Ambros-Rudolph and colleagues classified the dermatoses of pregnancy into four distinct entities – three of which have primary skin lesions including polymorphic eruption of pregnancy (PEP), pemphigoid gestationis (PG), and atopic eruption of pregnancy (AEP; including previously separate entities of prurigo of pregnancy, pruritic folliculitis of pregnancy, and eczema in pregnancy). 11 Pustular psoriasis of pregnancy (PPP) has also variably been included among the dermatoses of pregnancy. Among pregnant women reporting pruritus, 11.8–76.4% are ultimately diagnosed with a specific dermatosis of pregnancy.4,5,11
Polymorphic eruption of pregnancy
Previously known as pruritic and urticarial papules and plaques of pregnancy (PUPPP), late-onset prurigo of pregnancy, erythema multiforme of pregnancy, and Bourne’s toxemic rash of pregnancy, PEP is a benign inflammatory disorder of the skin associated with pregnancy. It is among the most common dermatoses of pregnancy, with an incidence of 1:200–250 pregnancies.8,12 In 2006, Ambros-Rudolph and colleagues found that 21.6% of women presenting with pregnancy-onset generalised pruritus were diagnosed with PEP. 11 PEP more commonly affects women who are primigravida, have multiple gestations, or have obesity. PEP typically occurs in the third trimester or early postpartum period and most commonly presents with intensely pruritic erythematous and edematous urticarial papules and plaques.8,11 Approximately 50% of those affected, develop polymorphic features as the disease evolves, including widespread erythema, targetoid or annular lesions, vesicles, and eczematous plaques. Lesions classically present in striae distensae, spreading to the trunk and proximal thighs over the course of days. PEP generally spares the face, palms, soles, and the umbilicus (an important distinguishing feature between PEP and PG). 6 Diagnosis is based on clinical presentation and history. If biopsied, cutaneous histopathology shows nonspecific epidermal changes ranging from mild spongiosis to acanthosis with hyperkeratosis and parakeratosis, perivascular lymphocytic infiltrate, and/or dermal edema with variable neutrophilic and eosinophilic infiltrate. Direct immunofluorescence (DIF) and indirect immunofluorescence (IIF) are negative. Laboratory tests are unremarkable.6,8 Importantly, maternal and fetal prognoses are not affected by PEP. The rash typically resolves by four weeks postpartum and does not tend to recur with subsequent pregnancies. 8
Treatment is symptomatic, with low- to mid-potency topical steroids and emollients as first line therapy. Oral antihistamines may also be used. 6 For women who fail to respond to these initial therapies, intractable pruritus may be treated with short courses of systemic corticosteroids or narrowband ultraviolet B (UVB) phototherapy. 6
Atopic eruption of pregnancy
Coined in 2006 by Ambros-Rudolph and colleagues, the term AEP includes dermatoses historically termed: eczema in pregnancy, prurigo of pregnancy, pruritic folliculitis of pregnancy, papular dermatitis of pregnancy, and prurigo gestationis. 8 AEP is defined as an exacerbation or first occurrence of eczematous or papular lesions during pregnancy in women with a personal or family history of atopy. 8 It is the most common dermatosis of pregnancy; 43–49% of women who present with a pruritic rash during pregnancy are diagnosed with AEP.11,13 Among these women, roughly 20% experience an exacerbation of pre-existing atopic dermatitis and 80% develop an eczematous eruption for the first time or after extended remission. 11 AEP typically appears earlier than other pregnancy-related dermatoses, often during the first trimester, with 75% of affected women presenting before the third trimester. 11 Typical clinical presentations include eczematous eruptions over the face, eyelids, neck, and flexural aspects of the extremities (i.e. antecubital or popliteal fossae). This presentation is named eczematous type or “E” type. 11 However, up to 30% may present with either classic prurigo lesions or small erythematous papules or pustules over the trunk and extremities – a presentation named papular/prurigo type or “P” type. 11 Diagnosis is based on the woman’s clinical presentation and history, with specific features including onset before the third trimester, as well as personal or family history of atopy and/or elevated IgE (though this criterion is controversial). 14 If biopsied, histopathology is nonspecific and varies by lesion stage. Epidermal changes include spongiosis, hyperkeratosis, parakeratosis, and erosions with a primary lymphocytic dermal infiltrate with admixed eosinophils and sterile follicular inflammation. DIF and IIF are negative. 8 Maternal and fetal prognoses are not altered in AEP. AEP resolves in the postpartum period; however, the eruption may recur in subsequent pregnancies.8,11
Treatment is directed at relieving pruritus and xerosis without increasing maternal or fetal risk. Women with AEP benefit from emollients applied directly after bathing with lukewarm water and using mild soaps/cleansers and detergents. When emollients alone are insufficient for symptom control, low- and mid-potency topical steroids are recommended. Antihistamines may also be used. In severe cases unresponsive to topical steroids, narrow-band UVB phototherapy may be helpful, or in recalcitrant and highly symptomatic cases, a short course of oral corticosteroids may be considered.6,8
Pemphigoid gestationis
Previously known as herpes gestationis, PG is a rare pregnancy-associated autoimmune skin disorder that is immunologically and clinically similar to the pemphigoid group of autoimmune blistering skin disorders. 15 It is estimated to occur in 1:50,000–60,000 pregnancies.6,15 Data from case series suggest that onset is most common in the second and third trimesters, but can begin in the first trimester and postpartum.11,13,15,16 PG initially presents with severe pruritus followed by inflammatory skin lesions, generally urticarial papules and annular plaques which progress to vesicles, and finally to large tense bullae on an erythematous background. 15 However, certain case series have reported vesicular lesions in only 65% of women diagnosed with PG. 17 Additionally, while PG was classically described to begin in the umbilical region (distinct from PEP) and spread to the rest of the abdomen, more recent case series have found the extremities to be the most common site of involvement.15,17 The eruption may involve the entire body, including palms and soles, sparing only the mucous membranes. 13 While PG is suspected based on clinical evaluation, biopsy is used to make the diagnosis. Histopathology shows papillary dermal edema and subepidermal bullae with eosinophil-rich infiltrate, with or without keratinocyte necrosis and perivascular infiltrate. DIF of perilesional skin demonstrates linear deposition of C3 and IgG autoantibodies at the dermoepidermal junction. 15 Recently, other diagnostic methods have been suggested to avoid biopsy – including IIF and enzyme-linked immunosorbent assay (ELISA) to detect circulating autoantibodies. 15 IIF detects IgG autoantibodies targeting the basement membrane of the skin in 30–100% of cases, while ELISA detects circulating IgG antibodies with specificity of 94–98% and sensitivity of 86–97% in women with PG. 15
The course of PG varies. It is typically self-limited and may spontaneously improve during late gestation or postpartum; however, 75% of women may experience flares at the time of delivery.15,18 While most women are symptom-free after six months postpartum, persistence over years has been described. In these cases, conversion from PG to bullous pemphigoid should be considered.15,19 Recurrence is common, occurring in 33–95% of subsequent pregnancies, generally with earlier onset and increased severity.15,19,20 PG may recur in association with menstruation or, in 25–50% of women, with oral contraceptives.15,16,19,21,22 PG is also associated with other maternal autoimmune disease, particularly a 10% risk of Graves’ disease. 20 Unlike PEP and AEP, PG is associated with fetal risks such as small-for-gestational-age and premature birth.15,16,19 Onset of PG before the third trimester and presence of blisters have been associated with adverse pregnancy outcomes.15,19,20 Approximately 10% of newborns may develop mild, self-limited urticarial or vesicular skin lesions, termed neonatal pemphigoid, due to passive placental transfer of antibodies, which resolve in days to weeks.16,17,19,20,22,23
Treatment during pregnancy is aimed at reducing pruritus and preventing development of new blisters. For mild cases, upper mid-strength topical steroids may be used; however, more severe cases often require systemic corticosteroids. Some recommend an initial daily dose of 0.5 mg/kg with subsequent tapering to a lower maintenance dose; however, refractory cases may require 1–2 mg/kg per day. Systemic steroids should not be tapered until new blister formation has been stabilised for at least two weeks, with final duration individualised according to the response.15,20 Oral antihistamines may be helpful adjunctive agents. In rare cases, more aggressive immunosuppressive therapy may be needed; there have been case reports of use of rituximab, intravenous immunoglobulin (IVIG) with and without cyclosporine, and in the postpartum, non-breastfeeding woman, azathioprine, minocycline or doxycycline with nicotinamide, or dapsone. 20 While these reports were from women who were not breastfeeding, azathioprine, short courses of minocycline or doxycycline, and even dapsone with appropriate newborn monitoring may be used in breastfeeding mothers while long courses of minocycline and doxycycline should be avoided. 24
Pustular psoriasis of pregnancy
Also known as impetigo herpetiformis, pustular psoriasis of pregnancy (PPP) is a rare variant of pustular psoriasis limited to pregnancy. PPP most commonly presents in the third trimester, but can occur in any trimester. 25 With fewer than 200 documented cases, there is debate as to whether PPP is a separate entity from generalised pustular psoriasis. While many women who develop biopsy-proven PPP have no personal or family history of psoriasis and are never symptomatic outside of pregnancy, some develop generalised pustular psoriasis later in life.25,26 Clinically, PPP initially presents with pustules studded on erythematous patches within intertriginous areas such as the groin, axillae, and inframammary folds. The pustules coalesce to form large dry plaques which may desquamate centrally as they enlarge, spreading centrifugally to the trunk and extremities symmetrically. The head, palms, and soles are spared, though oral and esophageal mucous membranes may be involved.26,27 Systemic symptoms may include fever, chills, diarrhea, lymphadenopathy, and malaise. Histologic findings are identical to pustular psoriasis, showing sterile spongiform pustules with neutrophilic invasion into the epidermis; both DIF and IIF are negative. Associated lab abnormalities may include leukocytosis, elevated erythrocyte sedimentation rate, hypocalcemia, hypophosphatemia, and low vitamin D due to hypoparathyroidism.25–28
PPP generally resolves after delivery, but often recurs in subsequent pregnancies, typically with earlier onset and greater severity. PPP has also been described to occur during menstrual cycles or oral contraceptive pill use. In severe cases, maternal risks include cardiac and renal failure, and fetal risks include placental insufficiency, low birth weight, stillbirth, and neonatal death.25–28
Systemic corticosteroids are generally first-line therapy, although topical steroids may be sufficient in mild cases. Most women respond to low-dose systemic corticosteroids (e.g. prednisone 15–30 mg/day). Severe cases, refractory to systemic steroids, have been treated with cyclosporine and infliximab and very resistant cases may require delivery. Importantly, fluid status and electrolytes should be closely monitored and corrected as severe hypocalcemia may lead to tetany or seizure.28–28
Etiologies not specific to pregnancy
When a woman presents with new or pre-existing pruritus with associated primary skin lesions in pregnancy, it is important to consider etiologies other than the dermatoses of pregnancy. These may include inflammatory and autoimmune lesions (atopic dermatitis, contact dermatitis, seborrheic dermatitis, stasis dermatitis, psoriasis, pityriasis rubra pilaris, lichen planus, urticaria, mastocytosis, drug eruptions, bullous diseases, eosinophilic folliculitis, dermatomyositis, lichen sclerosis), infestation or arthropod reaction (scabies, pediculosis, arthropod bite), infection (cutaneous bacterial, viral, fungal, or parasitic infections), neoplastic (cutaneous T-cell lymphomas, cutaneous B-cell lymphomas, and leukemic infiltrates of the skin), genetic, or genetic conditions (Darier’s disease, Hailey-Hailey disease, ichthyoses).
Generalised pruritus without primary skin lesions
Pregnancy-specific etiologies
Intrahepatic cholestasis of pregnancy
Historically referred to as obstetric cholestasis, ICP is a reversible cholestasis, which affects genetically predisposed women during late pregnancy.6,8 Incidence of ICP varies widely and has been reported to affect between 0.3% and 5.6% of pregnancies depending upon geographic location and ethnic background. 29 ICP typically presents in the late second trimester or beyond. Initial pruritus characteristically affects the palms and soles, with a pattern of nocturnal worsening. ICP is characterised by the absence of primary cutaneous lesions; however, secondary lesions from scratching may develop, varying from subtle excoriations early on to lichenification and prurigo nodularis in women with pruritus of longer duration. 6 The extensor surfaces of the extremities are most commonly involved, though secondary lesions can also affect the buttocks and abdomen. 8 Jaundice may occur in 10% of cases and is associated with more severe disease and prolonged course. 8 Certain guidelines define ICP as pruritus in pregnancy accompanied by otherwise unexplained elevation in liver function tests or bile acid concentrations which resolve after delivery (Government of Western Australia Department of Health, Royal College of Obstetricians and Gynaecologists) while others only mention persistent pruritus that resolves with delivery and bile acids greater than 10 µmol/L (American College of Gastroenterology, European Association for the Study of the Liver, Society for Maternal and Fetal Medicine ((SMFM)). 29 An ICP diagnosis should be suspected based on clinical presentation and is supported by elevated total serum bile acids in the absence of other liver pathology.8,30 Liver function tests and serum bile acid levels should be drawn. 29 Viral hepatitis of any type should be considered when diagnosing ICP, particularly in the presence of jaundice, steatorrhea, dark urine, or history of illicit drug use. 29 Histologic findings in the skin and liver are nonspecific, and DIF of perilesional skin is negative. 25
Pruritus typically persists through delivery, with gradual resolution within two to three weeks postpartum. 8 Maternal prognosis is generally favorable; however, women who develop steatorrhea (often associated with jaundice) with malabsorption of fat-soluble vitamins, like vitamin K, have increased risk of bleeding. 25 ICP has been associated with increased risk of preeclampsia, gestational diabetes, gallstones, cholangitis, hepatitis C, and cirrhosis as well as future liver and biliary tree malignancy, immune-mediated diseases, and cardiovascular disease. 31 Importantly, recurrence rates range from 40% to 92% in subsequent pregnancies and there have been some reports of recurrence with oral contraceptive use.25,29 Concern is warranted regarding fetal prognosis in ICP. As maternal bile acid concentrations increase, so do risk of preterm delivery, intrapartum fetal distress (i.e. meconium, abnormal fetal heart rate), and stillbirth. Increased risk of stillbirth, as compared to the background rate of stillbirth in the general population, appears to be concentrated among women with bile acids of 100 µmol/L or greater.30,32
Treatment of ICP is an active area of research with evolving recommendations.29,30 The goal is to reduce serum bile acid levels to ameliorate maternal pruritus, prolong pregnancy, and reduce fetal risk. Ursodeoxycholic acid (UDCA) was traditionally considered to lower bile acids, reduce maternal pruritus, and improve fetal prognosis; however, more recent meta-analysis and randomised controlled trial data suggest that there is no benefit to bile acid levels or fetal outcome and minimal, clinically insignificant effect on maternal pruritus.29,33 Still, all current guidelines recommend UCDA as first line treatment. 29 Oral antihistamines or aqueous creams with menthol may be helpful as adjunctive agents for pruritus. Antenatal testing in women with ICP has not been shown to predict pregnancies at risk of fetal death, and is currently recommended only by SMFM. 29 Optimal delivery timing given increased risk of stillbirth has not been well established and guidelines vary in their recommendations – with some recommending delivery at 38 weeks for severe disease and consideration of earlier delivery if bile acids are over 100 µmol/L and others advocating for delivery between 37 and 38 weeks or sooner with documented pulmonary maturity for all women with ICP. 29 Pruritus generally resolves within days to weeks after delivery. 8
Pruritus gravidarum
Pruritus gravidarum, or gestational pruritus, is defined as maternal pruritus without hepatic impairment or underlying dermatological disorder. Incidence varies from 3% to 14%. 34 Onset is typically in the last trimester of pregnancy, characterised by pruritus which may be focused over the abdomen or generalised. Importantly, primary skin lesions are absent and serum bile acids and liver function tests are normal. It typically appears in the last trimester and disappears soon after delivery, tending to recur in subsequent pregnancies. Treatment includes emollients, weak topical steroids, and systemic antihistamines. 34
Etiologies not specific to pregnancy
Generalised pruritus in the absence of primary skin lesions is typically caused by systemic disease (Table 1). It is important for the obstetric provider to recognise that etiologies unrelated to pregnancy may also affect pregnant women and to consider all potential causes of pruritus in pregnancy. These include a range of systemic diseases such as renal disease, liver disease (primary biliary cholangitis, sclerosing cholangitis, viral hepatitis, drug-induced cholestasis, obstructive jaundice), endocrine disease (thyrotoxicosis, Grave’s disease, hypothyroidism, diabetic neuropathy, and other disorders associated with poorly controlled diabetes), iron deficiency anemia, malignancy (most commonly Hodgkin lymphoma, non-Hodgkin lymphoma, mycosis fungoides, polycythemia vera, leukemias, plasma cell dyscrasias, bile duct carcinoma, and gastric carcinoid tumors), systemic infection (HIV), systemic rheumatic disease (dermatomyositis, systemic sclerosis, primary Sjogren’s syndrome), drug reactions (opioid analgesics are a particularly common culprit in the peripartum period), neurologic disorders (multiple sclerosis), and primary psychiatric disorders (psychogenic excoriation, delusional infestation, substance use disorders). Given the range of possible etiologies, it is important to perform a careful exam and history including history of thyroid disorders, liver disease, renal disease, HIV infection, malignancy, constitutional symptoms, medication use, travel, psychiatric and substance use history, and pruritus in other household members. Initial diagnostic testing should include complete blood count with differential, liver function tests including bilirubin, transaminases, and alkaline phosphatase, thyroid-stimulating hormone, and basic metabolic panel to assess blood urea nitrogen and creatinine. In pregnant women, this assessment should include bile acids. Additional lab testing should be based on the history and physical examination, and may include HIV testing, immunofluorescence studies, stool examination for ova and parasites, viral hepatitis serologies, and serum protein electrophoresis and immunoelectrophoresis.
Management is largely based on identification and appropriate treatment of the underlying disease. However, options for symptomatic control with oral antihistamines during pregnancy as outlined below are largely unchanged.
Localised pruritus without primary skin lesions
Pregnancy-specific etiologies
Localised pruritus without primary skin lesions generally suggests neuropathic or psychogenic itch; however, in the setting of pregnancy, if pruritus is localised to the hands and feet, ICP must also be considered as detailed above.
Etiologies not specific to pregnancy
There are a limited number of diagnoses characterised by localised pruritus without primary skin lesions. These include brachioradial pruritus, notalgia paresthestica, postherpetic neuralgia, cerebral or spinal infarcts, and vulvodynia.
Pregnancy-related considerations for common pruritus therapies
Topical corticosteroids
Several large population-based studies and a Cochrane review have failed to demonstrate an increased risk of congenital malformations, including oral cleft lip/palate or preterm delivery with use of topical corticosteroids.35–38 Because high-potency steroids have been associated with fetal growth restriction and are known to cause skin thinning, increasing propensity for striae gravidarum, mild- to moderate-potency topical steroids are recommended as first-line agents.35–38 However, if high-potency steroids are required, the duration of treatment should be limited and areas of thin skin (genitals, axillae, eyelids, skin flexures) should be avoided.
Systemic corticosteroids
While systemic steroids carry greater risk in pregnancy than topical steroids, they are an important therapeutic option. Placental metabolism and transplacental passage are variable among different systemic corticosteroids. Non-fluorinated corticosteroids like prednisone or its metabolite prednisolone are largely inactivated by placental 11-beta hydroxysteroid dehydrogenase, thereby limiting passage to the fetus.35,39 While some studies suggest increased risk of orofacial clefts or decreased birth weight among fetuses exposed to systemic corticosteroids in the first trimester, evidence is conflicting, and likely impacted by maternal dose, duration of exposure, and indication for use.40–42 More recently, larger population-based studies have shown no increased risk of orofacial clefts or other congenital anomalies.35,36 Yet prolonged steroid exposure may have other important fetal and maternal implications such as fetal or maternal hypothalamus-pituitary-adrenal axis suppression, as well as maternal insulin resistance, weight gain, hypertension, psychiatric disease, infection, and decreased bone density. When systemic corticosteroids are necessary for dermatologic indications, the lowest effective dose should be used, and prolonged courses should be avoided. If prolonged courses are necessary, women should be monitored for hyperglycemia, supplemented with vitamin D and calcium, and stress-dose steroids around delivery should be considered. 6
Antihistamines
Generally, most pregnant women who require antihistamines may be appropriately treated with a second-generation agent as these drugs are less sedating and have fewer cholinergic side effects compared with first-generation agents. Traditionally, the sedating first-generation antihistamines (i.e. chlorpheniramine, tripelennamine, diphenhydramine) were preferred in the first trimester due to less available data on newer, second-generation agents (i.e. cetirizine, loratadine, fexofenadine). 35 However, more current safety data suggests that first- and second-generation antihistamine use during pregnancy with respect to birth defects is generally reassuring, with no definite teratogenic effects.35,43–45 Among first-generation agents, the American College of Obstetrics and Gynecology and the American College of Allergy Asthma and Immunology have recommended chlorpheniramine and tripelennamine as antihistamines of choice during pregnancy, while among the second-generation agents cetirizine and loratadine are preferred. 46
Conclusion
Pruritus is common during pregnancy. While it may be the result of physiologic changes of pregnancy or pregnancy-specific pathologies, it may instead indicate an underlying disease process unrelated to pregnancy. As each of these etiologies have different prognoses, implications for fetal monitoring, and treatments, it is essential that obstetric providers are aware of these possibilities and take a systematic approach to evaluation to allow for timely diagnosis and intervention.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Ethical approval
Not applicable
Informed consent
Not applicable
Guarantor
MR is the guarantor of the present work.
Contributorship
MR, RT, and EL researched relevant literature. MR wrote the first draft of the manuscript. EF assisted with reviewing and editing. All authors reviewed and edited the manuscript and approved the final version of the manuscript.