
Abstract
Aims
To describe the use of laser, endoscopic balloon dilatation with jet ventilation anaesthesia in the treatment of pregnant women with idiopathic subglottic stenosis.
Materials and methods
This is a case review of pregnant women with idiopathic subglottic stenosis, presenting to a tertiary referral centre with worsening breathlessness. Data were extracted from patient case notes.
Results
Four women underwent surgical management of subglottic stenosis in pregnancy. One patient required two procedures during the course of their pregnancy due to restenosis. All women had improvement in symptoms post-operatively and went on to deliver healthy babies at term.
Conclusion
Endoscopic balloon dilatation of idiopathic subglottic stenosis is a safe and viable treatment option in pregnancy and should be offered as first-line treatment in symptomatic women.
Introduction
Idiopathic subglottic stenosis (iSGS) is a rare condition characterised by mucosal inflammation and fibrosis of the subglottis, an area below the true vocal folds along the inner surface of the cricoid cartilage. This results in progressive airway obstruction which in advanced stages can present emergently with life threatening airway compromise. 1 Women present with progressive dyspnoea and cough, which can be mistaken for asthma and delay diagnosis.1,2 iSGS predominantly affects females, 1 but the incidence of pregnant women with iSGS is rare.
Pregnancy is associated with a number of physiological adaptations. In order to meet the increasing metabolic needs of the fetus, placenta and uterus, the respiratory system undergoes significant changes resulting in a progressive increase of oxygen consumption by 30–40%. In addition, high levels of oestrogen cause an increase in total body water and mucosal oedema of the vocal cords, larynx and trachea. Other physiological changes associated with pregnancy include a decreased functional residual capacity secondary to diaphragm elevation from a gravid uterus and decreased blood return to the right ventricle due to the weight of the fetus on the inferior vena cava.3,4 Consequently, about 70% of healthy pregnant women report shortness of breath which is also known as physiological breathlessness of pregnancy. 5
These changes make a diagnosis of iSGS especially challenging; symptoms may be attributed to pregnancy-related physiological adaptations.6,7 Therefore, in pregnant women presenting with airway symptoms such as stridor, wheezing or dyspnoea on exertion, iSGS should be considered because inadequate oxygenation can be associated with placental abruption, pre-eclampsia and intrauterine growth restriction. 5
A review of the literature shows a lack of high quality studies addressing the management of iSGS in the pregnant woman. With current evidence limited to case reports, there is no consensus or standardisation of managing iSGS in pregnancy.
Reported airway management approaches of iSGS in pregnancy range from surveillance, endoscopic surgery and tracheostomy.7–23 Endoscopic interventions are the predominant surgical technique reported in the literature,7–17 but some authors espouse the benefit of a surgical tracheostomy.18,19 The aim of the study is to describe the use of endoscopic balloon dilation with laser and jet ventilation in the management of iSGS in pregnancy and provide an overview of the current literature.
Materials and methods
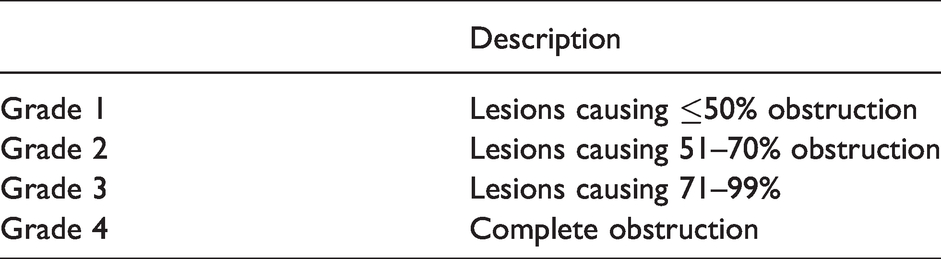
Records of all pregnant women with iSGS treated for airway compromise at a tertiary referral airway reconstruction centre were retrospectively reviewed. Information was obtained on patient demographics, clinical presentation, grade of stenosis and the treatment given. The degree of stenosis was graded using the Cotton–Myer grading scale 24 (Table 1). All women were managed using a standardised technique described below.
Myer–Cotton grading system for subglottic stenosis.
Ethical considerations
All data collection and analysis were carried out in accordance with our institution’s Clinical Information Governance regulations.
Patient demographics
We identified four women presenting with iSGS in different stages of pregnancy. All four women were managed endoscopically using the technique described below. Table 2 shows the patient details and demographics.
Patient details and demographics.
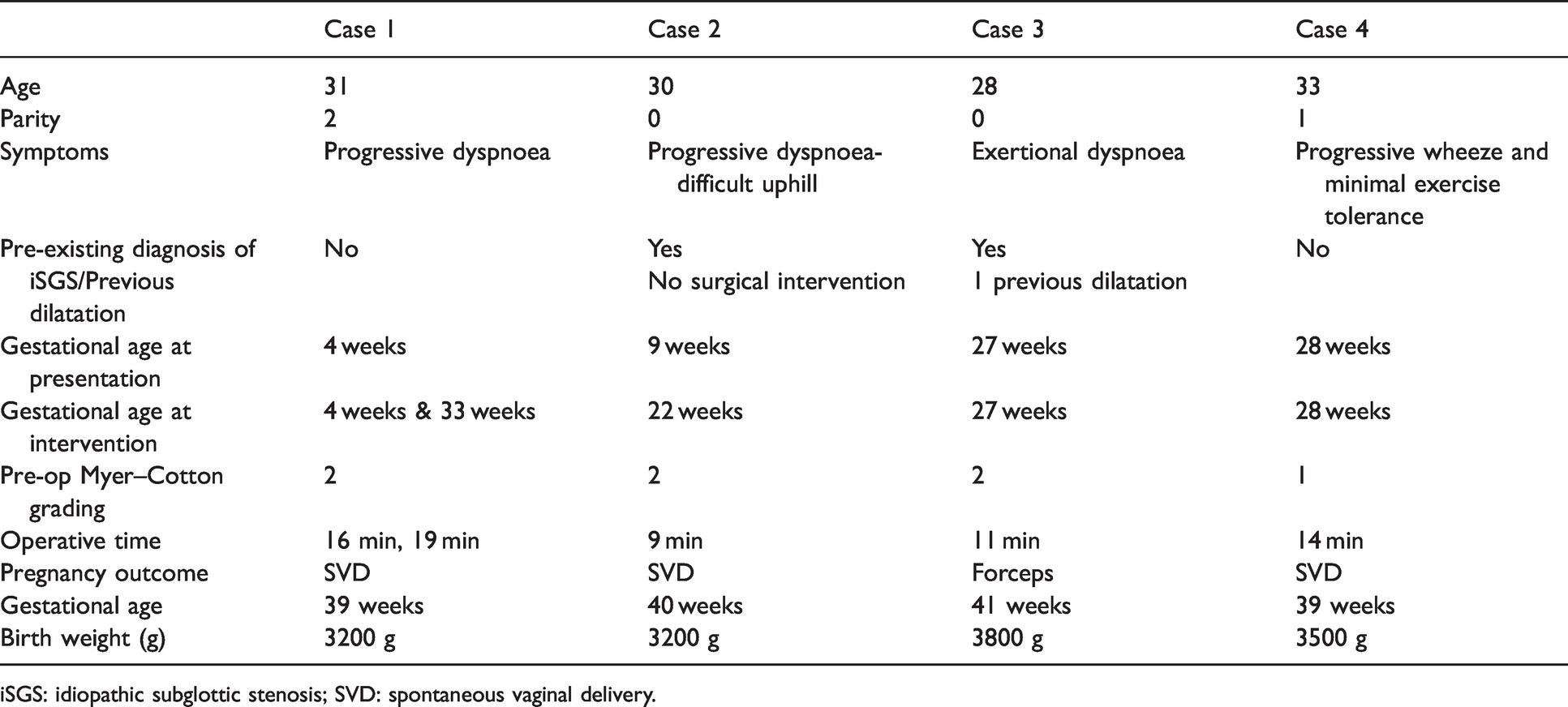
iSGS: idiopathic subglottic stenosis; SVD: spontaneous vaginal delivery.
Technique
Anaesthesia
Procedures were performed under general anaesthesia (GA) with both our specialist otolaryngology airway and obstetric anaesthetists present. Women were positioned in a 30° reverse Trendelenburg position with a 15° left lateral tilt to relieve aorto-caval compression. Preoxygenation was performed by mask ventilation with 100% oxygen. Anaesthesia was induced with a bolus of propofol (3 mg/kg) and fentanyl citrate (100 mcg). Women were temporarily paralysed with atracurium besilate muscle relaxant. The airway was initially secured with a laryngeal mask airway (LMA; Intavent, Orthofix, UK) before commencing intermittent positive pressure ventilation. In the operating room, the LMA was replaced with a suspended surgical laryngoscope positioned to visualise the vocal cords, subglottis and proximal trachea. High-frequency supraglottic jet ventilation was started. Total intravenous anaesthesia, using an infusion of propofol and alfentanil hydrochloride was used for the procedures. The surgical laryngoscope was replaced with the LMA at the end of the procedure. Paralysis was reversed using neostigmine and glycopyrolate and the women were ventilated until spontaneous breathing commenced.
Surgical approach
Suspension laryngoscopy with a Dedo-Pilling laryngoscope (Teleflex, Morrisville, NC, USA) was performed under GA. The airway was visualised with a combination of a defogged 4 mm Karl-Storz 0° airway endoscope (Karl Storz GmbH & Co KG, Tuttlingen, Germany) and an operating microscope. To begin the procedure, the endoscope was advanced through the laryngoscope to inspect and photo-document the larynx and trachea. The severity of the subglottic stenosis was graded using the Cotton–Myer grading scale as previously described. The lesions were infiltrated with 60–80 mg of methylprednisolone acetate. Thereafter, radial incisions were made at the edge of the stenosis using carbon dioxide (CO2) laser delivered via a surgical microscope and micromanipulator device, leaving intact islands of tissue between the incisions. Balloon dilatation of the stenotic segments was performed using CRETM Pulmonary Balloon dilator (Boston Scientific, Natick, MA, USA) to 16.5 mm, for up to 60 s duration. Figures 1 and 2 demonstrate pre and post dilatation images from case 1.
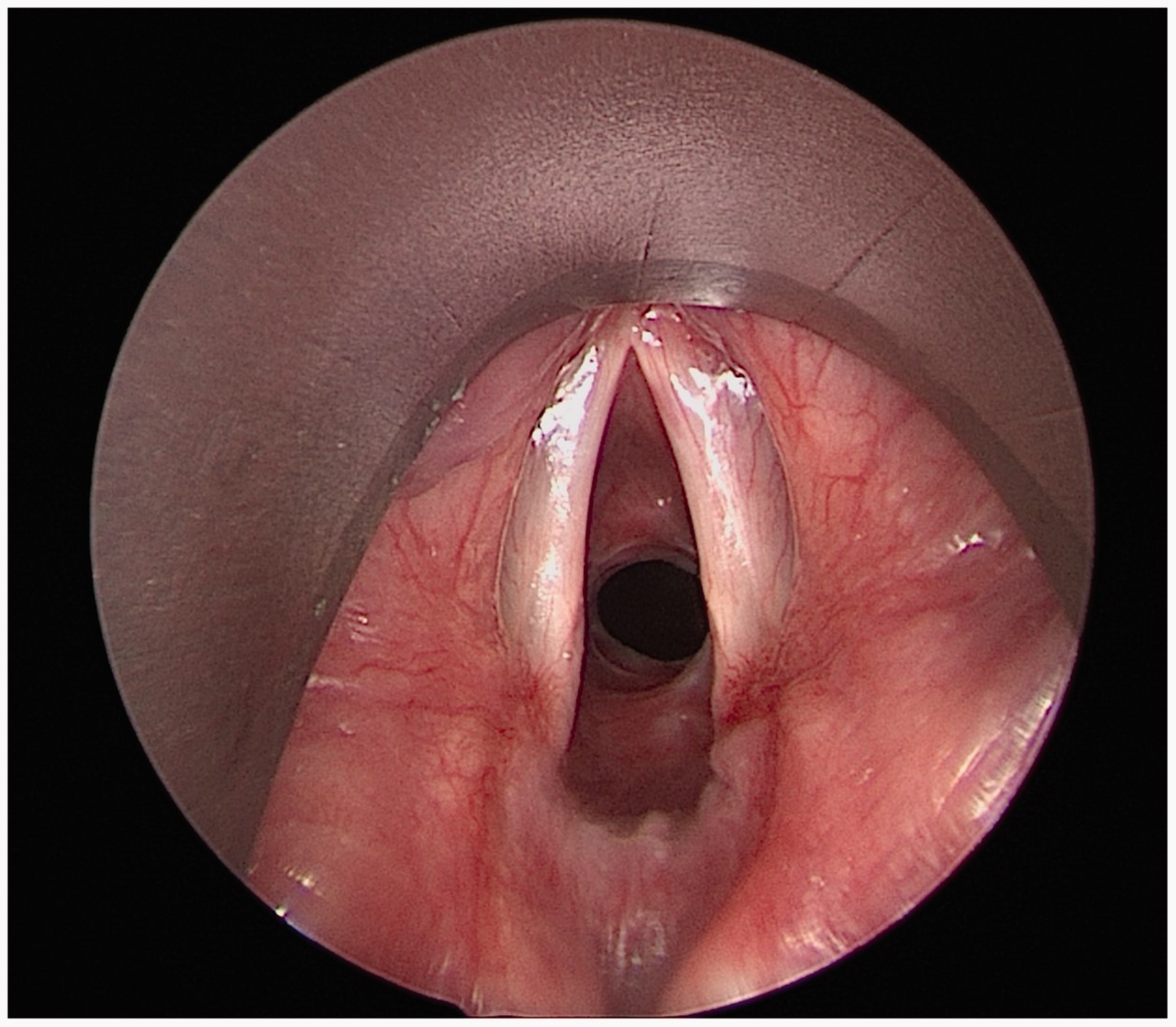
Intraoperative endoscopic view of the larynx showing grade 2 Myer–Cotton subglottic stenosis.
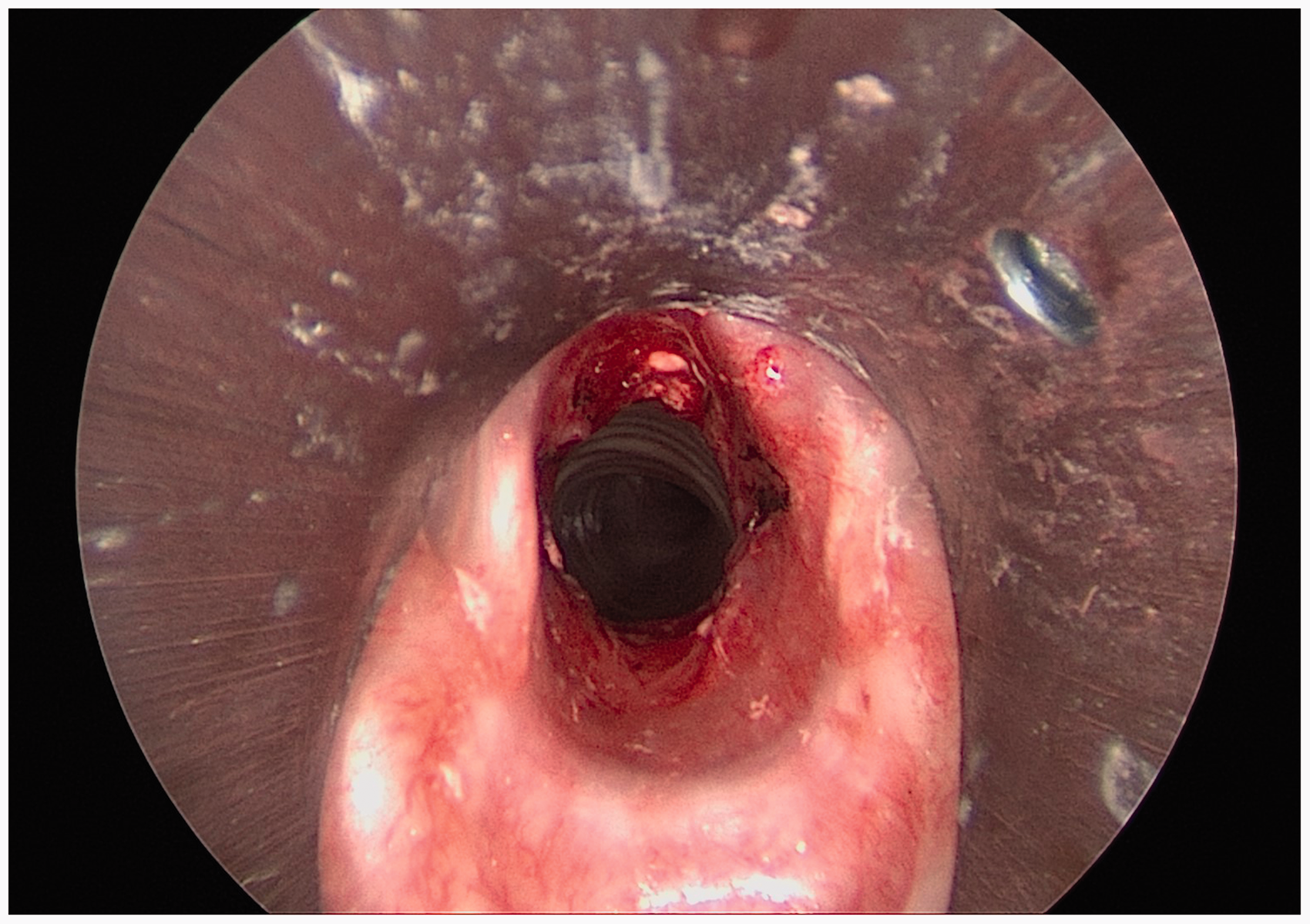
Endoscopic view of the subglottis and trachea following balloon dilatation and laser.
Obstetrics
All women had routine antenatal care. A joint anaesthetic, obstetric and ENT consultation was carried out prior to the surgery. Corticosteroids were considered and given to women over 26 weeks’ gestation for fetal lung maturity. All women received ranitidine and metoclopramide antacid prophylaxis. Women in the third trimester were admitted the day before surgery to the antenatal ward. One patient was only 22 weeks’ gestation and fetal heart rate was auscultated before, during and after the procedures. The other three cases had continuous fetal monitoring in the operating theatre and in the recovery area. The obstetric team including an obstetrician, midwife and an obstetric anaesthetist were available in the operating theatre and participated in the WHO time out and sign in. The neonatologists were informed of the case and a neonatal resusitaire was made available in the operating theatre in case of an emergency delivery for prolonged fetal bradycardia. After a period in recovery the patient returned to the antenatal ward and was monitored overnight.
Discussion
Subglottic stenosis can be congenital or acquired. Tracheal trauma and systemic conditions like granulomatosis with polyangiitis are recognised causes of the acquired form.1,8 The absence of an identifiable cause leads to a diagnosis of iSGS, a disease that almost exclusively affects Caucasian women. 1 Direct endoscopic examination of the airway confirms the diagnosis.
Both endoscopic and open techniques are used for the management of iSGS in the non-pregnant patient.1,25,26 Endoscopic techniques include a combination of balloon and rigid dilatation with or without laser; primary laser excision; and rarely stents.1,25 The use of intralesional mitomycin C and glucocorticoid injections has also been reported in combination with other techniques. 27 At our tertiary referral centre, intralesional methylprednisolone is used rather than mytomycin C, due to the limited evidence of benefit as well as potential carcinogenicity. 28 Resection of the stenotic segment via cricotracheal resection, or in some cases a laryngotracheal reconstruction with rib graft, are more definitive open surgical techniques.1,26
Surgery and GA in a pregnant patient are challenging with a perceived increased risk of miscarriage in the first trimester29,30 and an increased risk of premature delivery. 31 However, with respect to ENT, planned surgery in pregnant women who are otherwise well, is generally safe and has good pregnancy outcomes. 32
Pregnancy results in considerable changes in cardiopulmonary and metabolic physiology. A combination of a diminished functional residual capacity, and an increase in maternal and fetal oxygen requirements, leave both mother and fetus at risk of hypoxia. 29 Furthermore, as pregnancy progresses, the gravid uterus compresses the major vessels and causes an increase in intra-abdominal pressure. Gastro-oesophageal reflux occurs in over 80% of women in the second trimester of pregnancy, as a direct result of progesterone decreasing lower oesophageal sphincter tone, and the gravid uterus pushing the stomach into a horizontal position. This, in concert with hypotonia of the lower oesophageal sphincter, predisposes the pregnant patient to aspiration. 30 Thus in pregnancy, minor airway and physiological derangements can have devastating consequences for both mother and fetus. Subglottic stenosis is challenging for both anaesthetist and surgeon; even if tracheal intubation is possible, it can be traumatic, and surgery requires a tubeless field. 33 The risk of a pregnant woman aspirating during GA can be minimised using rapid sequence induction/intubation (RSI). 4 However, RSI was not used in our series; instead we utilised an open airway anaesthetic technique similar to that we use in all our non-pregnant iSGS women. Damrose et al. reported using a similar anaesthetic technique in their series describing the management of pregnant women with iSGS. 8
Women with iSGS in pregnancy are complex and require input from a multidisciplinary team (MDT) consisting of an otolaryngologist, anaesthetist and obstetrician. Early diagnosis is critical, and the value of a shared airway management plan between the patient and the MDT cannot be overstated.
However, advance planning is not always possible, and women can present with life-threatening airway compromise especially where iSGS is undiagnosed. As well as being traumatic for the patient, management of acute airway compromise in pregnancy can be challenging from an anaesthetic and surgical standpoint. Some authors have reported cases of failed intubation and traumatic intubation dealing with women with undiagnosed iSGS in pregnancy. 20
Historically, surgical tracheostomy under local anaesthesia (LA) has been widely accepted as the optimum method for securing a severely compromised airway that is not amenable to any other intervention. However, this technique is also risky and requires a compliant patient capable of lying flat and tolerant of tracheal manipulation. 32 This is not a straightforward undertaking in pregnancy, given the challenges of lying in the supine position as outlined above. Parsa et al. described an emergency tracheostomy in the last trimester of pregnancy in a woman with subglottic and tracheal stenosis after previous cricotracheal separation. 19
Some clinicians have advocated for elective surgical tracheostomy in pregnant women with iSGS. They argue that a surgical tracheostomy under LA is the safest temporising method of securing the airway in pregnancy as it minimises the risk of hypoxaemia and hypocarbia to the fetus. The airway is then managed definitively in the postpartum period.19,20 We also believe that institutional factors such as a lack of equipment or surgeons with endoscopic airway skills may also influence the decision to perform a surgical tracheostomy.
A variety of endoscopic techniques have been reported in the literature. Rumbark et al. reported their experience of using electrocautery to make longitudinal incisions into the stenotic segment followed by balloon dilatation in two women in the third trimester of pregnancy. One of these cases was managed under LA and sedation while the other had GA. 10 A combination of radial incisions into the stenotic segment with potassium titanyl phosphate laser and balloon dilatation has also been described in the third trimester of pregnancy.11,12 Successful use of carbon dioxide laser and balloon dilatation under GA in the last trimester has been reported with excellent results.8,14
Our preference is to use endoscopic balloon dilatation with steroids and laser as adjuncts, a technique we have used extensively in the non-pregnant patient with iSGS. We firmly believe that this is a favourable alternative in pregnancy where the prospect of a tracheostomy and its aftercare are burdensome for women. This endoscopic technique carries less immediate surgical risks and fewer long-term risks than tracheostomy. Reported complications with the endoscopic technique include cough, bleeding, tracheitis, and rarely, tracheal perforation and surgical emphysema. 34 Women may have a cough and some blood stained secretions in the immediate post-operative period but these tend to be self-limiting. More serious complications such as tracheal perforation will need an urgent ENT review. Typically, all our non-pregnant women with iSGS are discharged on the same day of surgery after 6 h of routine monitoring. They are given humidified oxygen and saline nebulisers in the post-operative period. However, all pregnant women in our series were kept in hospital for one night for routine monitoring and were discharged the next day.
A key consideration in pregnancy is that the endoscopic technique is not curative and as such, the patient may require another procedure as was the case for some of our women. These considerations and the risks associated with other surgical techniques need to be discussed with the patient to facilitate an informed decision.
Conclusion
Management of iSGS in pregnancy is challenging and requires a MDT approach. While best evidence on management of iSGS in pregnancy is limited to case reports, there is a trend towards endoscopic airway techniques. Based on our experience and that of others we believe that endoscopic balloon dilatation is a safe and efficacious option in managing the pregnant patient with iSGS.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Aintree University Hospital does not require ethical approval for reporting individual cases or case series.
Informed consent
Written informed consent was obtained from the patient for their anonymised information to be published in this article.
Guarantor
TK guarantees the integrity, accuracy and contributorship of the manuscript.
Contributorship
TK wrote the first draft of the manuscript. All authors reviewed the literature and edited the manuscript and approved the final version of the manuscript.
Acknowledgements
None.