
Abstract
The case presented details an uncommon case of subglottic tracheal stenosis exacerbated by pregnancy. We outine the multidisciplinary management involved and the outcomes for the pregnancy. The case serves as a reminder that shortness of breath in pregnancy has a broad differential diagnosis, and stridor is always abnormal.
Introduction
Subglottic stenosis (SGS) is a rare condition characterised by obstruction at the lower larynx and upper trachea. Airway compromise may be revealed or exacerbated during pregnancy, presenting a significant challenge for the pregnant woman and her treating team. Our case of a multigravida with idiopathic SGS highlights the necessity for careful multidisciplinary collaboration.
Case
A 31-year-old woman in her third pregnancy, had been troubled by stridor and dyspnoea during her second pregnancy. Persistent postnatal symptoms led to the diagnosis of SGS. A 75% (Cotton-Meyer grade 3) stenosis was diagnosed and managed with microlaryngoscopy, balloon dilatation and steroid injections prior to her third conception and she was otherwise well with a body mass index (BMI) of 27 kg/m2 at booking.
A referral to the local otolaryngology team was made at her first antenatal visit. The woman was seen in their clinic at 25 weeks’ gestation. Soft exertional stridor was noted at this time. Fibreoptic nasendoscopy demonstrated recurrence, with a 40% (Cotton–Meyer grade 1) stenosis. Surveillance was initiated, and when reviewed again at 31 weeks’ gestation she had deteriorated significantly, with progressive exertional dyspnoea, resting stridor and inability to speak in full sentences. Pulse oximetry revealed an oxygen saturation of 91% in room air and a 60% (Cotton–Meyer grade 2) stenosis was visualised on repeat endoscopy. The case was discussed at the local obstetric case review meeting with input from the otolaryngology and paediatric teams. It was agreed that delivery was not yet appropriate; however, administration of antenatal corticosteroids was advised to promote fetal lung maturity should preterm delivery become unavoidable. Semi-urgent microlaryngoscopy and dilatation were recommended for management of her progressive airway obstruction.
The woman was reviewed by an obstetric anaesthetist with otolaryngologists present. The risks of perioperative aspiration and airway compromise were discussed. It was noted that apnoeic ventilation was preferable for the operation and a plan for either Transnasal Humidified Rapid–Insufflation Ventilatory Exchange (THRIVE) or intermittent tracheal intubation was proposed. The woman was prophylactically commenced on a proton pump inhibitor 5 days prior to the procedure. The case was scheduled locally as our facility has capacity for 24-h obstetric and neonatal care from 31 weeks’ gestation.
Microlaryngoscopy, laser incision and balloon dilatation were performed under general anaesthesia using the THRIVE technique at 32 + 2 weeks’ gestation. The woman was preoxygenated to an end-tidal oxygen saturation of 95% prior to anaesthetic induction with propofol, remifentanil and rocuronium. High flow oxygen was then administered via nasal cannulae at a rate of 70 L/min. Following radial incision, the subglottis was twice dilated with a 5.5 cm balloon to 4 atmospheres (atm) for 6 seconds. Oxygen saturations were maintained above 99% throughout the procedure and the woman was then administered neostigmine and glycopyrrolate. Fetal heart auscultation pre- and postoperatively was reassuring with no intraoperative fetal monitoring utilised. Significant maternal improvement was immediately apparent. Prophylactic low-molecular weight heparin and thromboembolic disease stockings were administered during admission, with hospital discharge the following day.
The woman continued fortnightly review in the antenatal clinic with no recurrence of symptoms. She subsequently delivered a healthy male infant weighing 4350 g at 39 weeks and 1 day of gestation, via elective repeat caesarean under spinal anaesthesia. The woman had an uneventful recovery. Her husband was planning a vasectomy, and the couple declined bridging contraception.
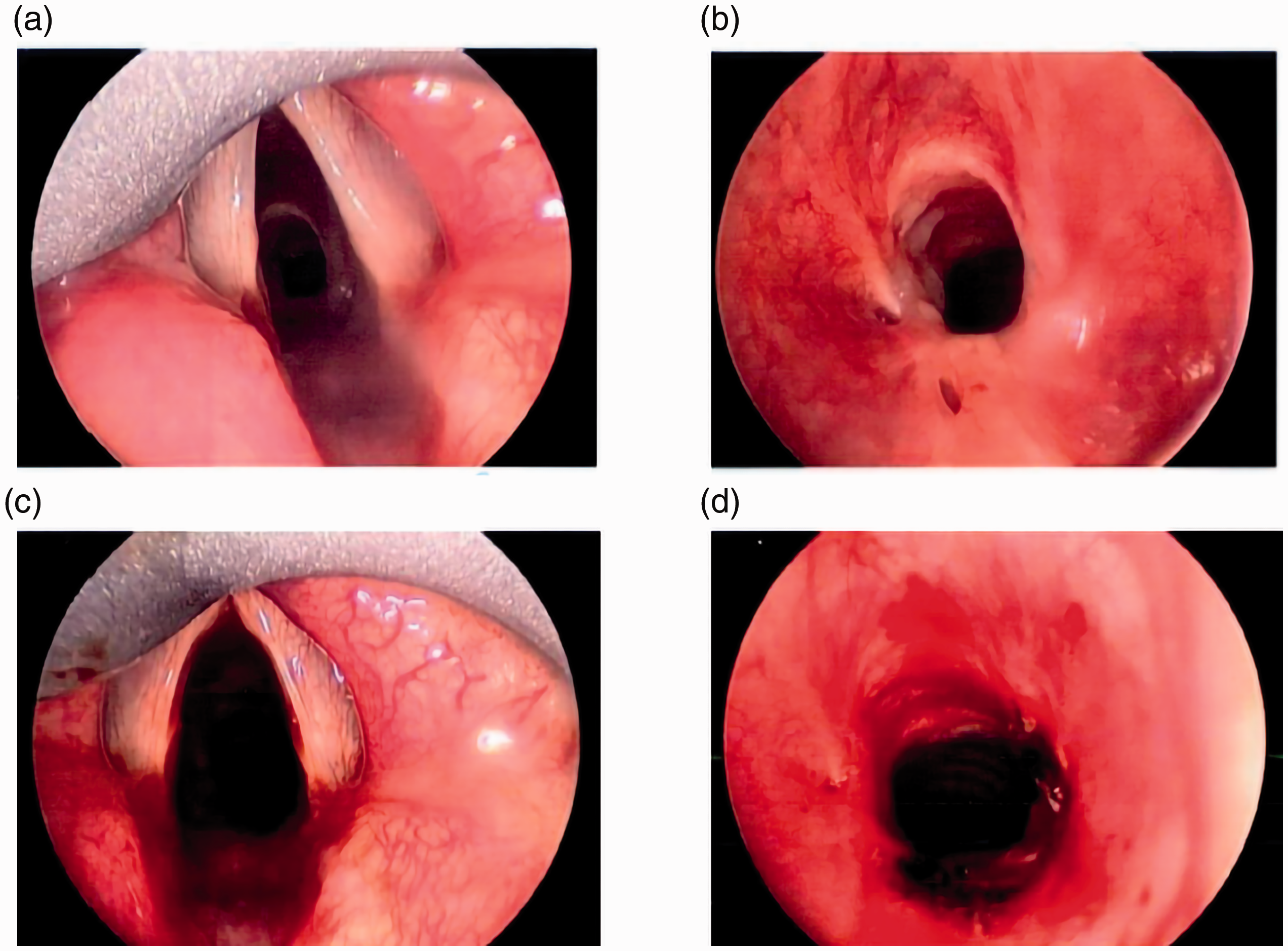
Images A and B immediately prior to intervention. Images C and D immediately following intervention.
Discussion
SGS may be congenital or acquired. Non-malignant causes include vasculitic conditions (granulomatosis with polyangitis, formerly known as Wegener’s granulomatosis, gastro-oesophageal reflux disease or airway trauma (e.g. iatrogenic injury from prolonged tracheal intubation). A history of previous anaesthesia or intensive care admission should be sought when SGS is suspected. Up to 30% of SGS is idiopathic, as in this case of a woman with no identified risk factors.
The physiological changes of gestation and parturition include: (i) a 25–50% increase in tidal volume and therefore minute ventilation to meet increased maternal oxygen demand,1,2 (ii) decreased functional residual capacity and expiratory reserve volume 2 and (iii) mucosal oedema and diaphragmatic splinting by the gravid uterus, resulting in a synchronous reduction in pulmonary compliance. As the subglottis is the narrowest point in the upper airway even a moderate degree of obstruction may manifest clinically during pregnancy, precipitating deterioration in an otherwise stable woman with SGS.
SGS may also directly complicate fetal well-being. An association exists between impaired forced expiratory volumes in asthmatic women with a trend towards lower birth weight 3 and higher rates of preterm birth. 4 This association is unlikely to ever be validated in SGS given the rarity of this condition, but should be considered by antenatal care providers.
There is no consensus regarding the timing or optimum method of intervention for SGS in pregnancy, with the literature restricted to a small cohort of case reports.5–12 Some authors report the use of prolonged systemic corticosteroids to alleviate symptoms, and at least one case of conservative management has been described. 13
Both endoscopic and open procedures for SGS have been described. 14 Interventional endoscopy using laser, balloon dilatation and stenting are generally temporising, with high rates of recurrence (as reflected in this case), but may be sufficient to support women pregnancy and birth. In severe cases, the use of tracheostomy may also be considered as a bridging measure to definitive management, e.g. with laryngotracheal reconstruction.
The risks of intervention, namely ventilatory failure, aspiration pneumonitis and an emergent need for preterm delivery, must be balanced against the unpredictable risk of progression to critical airway obstruction in a gravid woman. The timing of intervention must weigh these risks against the benefits of advanced fetal maturity. Subspecialist expertise in obstetric anaesthesia is essential. The need for paralysis and apnoeic ventilation, unimpeded airway access for surgical manipulation and the increased risks of airway compromise and aspiration in pregnancy can present significant challenges.
Apnoeic ventilation in the pregnant population is of particular interest due to increased maternal oxygen demand and decreased functional residual capacity. A faster rate of oxygen desaturation in the pregnant woman presents challenges for anaesthetic safety and potentially limits operating time for proceduralists. It is unlikely that a large-scale randomised-controlled trial examining apnoeic ventilation techniques in this population can be achieved; however, computer modelling has supported the use of apnoeic oxygen delivery via high-flow nasal cannulae, proposing up to 53 min in additional time to desaturation below 90% in the average pregnant woman. 15
The THRIVE technique16,17 as yet unvalidated in pregnancy, was successfully used in this case and has been reported elsewhere under similar circumstances. 6 This technique utilises high-flow nasal oxygen in an apnoeic woman to support oxygenation, but exposes both the woman and her fetus to the dual risks of aspiration and respiratory acidaemia from maternal accumulation of carbon dioxide. The alternative (intermittent oxygenation with bag-mask ventilation or repeated tracheal intubation) is technically challenging in pregnancy and hinders endoscopic access. Jet insufflation has also been successfully used in pregnant women undergoing balloon dilatation for SGS 18 with good results. The availability of extracorporeal membrane oxygenation (ECMO) should be considered in extreme examples at high risk of airway collapse.
Obstetrically, these women require close antenatal coordination of multiple disciplines including otolaryngology, anaesthetics, obstetrics, midwifery and neonatology. Postnatal contraceptive counselling is essential to ensure optimal timing of any future pregnancy in meeting the biological and psychosocial needs of the woman and her family.
The greatest risk appears to be for undiagnosed SGS, with case reports of latent upper airway obstruction being unmasked during pregnancy, even at the time of general anaesthesia for emergent caesarean section. 19 While shortness of breath and exertional dyspnoea are relatively common symptoms for pregnant women, stridor is always abnormal and warrants prompt investigation. The obstetric clinician should consider the possibility of unrecognised airway obstruction in the differential diagnosis of these symptoms, and remain alert to the potential for significant compromise with advancing gestation.
Conclusion
Progressive SGS is a rare but potentially severe complication of pregnancy and warrants consideration in all pregnant women reporting stridor or worsening dyspnoea. Endoscopic management with balloon dilatation appears to be a safe and effective first-line approach. Management requires close collaboration between otolaryngologic, anaesthetic, obstetric, midwifery and neonatal teams to optimise maternal and fetal outcomes.
Footnotes
Acknowledgements
None.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Written consent for anonymised publication of patient information has been obtained.
Informed consent
Written consent was obtained from the patient(s) for their anonymised information to be published in this article.
Guarantor
Obstetric case management by EH. Manuscript prepared by EM and EH. Consent for publication and images sought by EM.