
Abstract
Interstitial lung disease (ILD) presents rarely in pregnancy. Reports have associated disease activity with higher rates of preeclampsia, preterm births and fetal loss. This case report describes a patient presenting in her fifth pregnancy with worsening dyspnoea. She was treated with tacrolimus, prednisolone and post-partum methylprednisolone and ultimately had a successful outcome of childbirth.
Introduction
Interstitial lung disease (ILD) is a heterogeneous group of acute and chronic lung disorders characterised by varying degrees of inflammation and fibrosis of the pulmonary parenchyma that results in dyspnoea and impaired gas exchange. 1 Many require treatment with immunosuppressive therapy but this should be administered with careful consideration of effects on both the woman and her fetus. Here we describe a woman where tacrolimus and prednisolone were used for the treatment of ILD diagnosed during pregnancy, with successful outcome of childbirth.
History
A 32-year-old woman presented in her fifth pregnancy with worsening exertional dyspnoea since 6 weeks of gestation. She had four previous deliveries, including one stillbirth at 40 weeks in her third pregnancy, secondary to placental insufficiency. Her past medical history included mild childhood asthma and sickle cell trait. Her last admission to hospital with asthma was 11 years previous and medication at booking included beclometasone dipropionate and salbutamol inhalers. In her fourth pregnancy she was reviewed by respiratory physicians for shortness of breath which was attributed to a combination of asthma, anxiety and dysfunctional breathing. Postnatal follow-up was planned which she did not attend.
She was reviewed in the maternal medicine clinic at 25 weeks of gestation with severe shortness of breath on exertion, her exercise tolerance limited to 20 steps. She had attended a neighbouring hospital 10 days prior where she was investigated for this, with a V/Q scan that showed no pulmonary emboli and started on a fluticasone with salmeterol inhaler. In addition to her respiratory symptoms, she also described a rash over her arms and legs in summer but reported no muscle weakness or joint pains. There was no history of fever, cough, wheeze, chest pain, paroxysmal nocturnal dyspnoea, orthopnoea or oedema. She gave a history of childhood asthma but there was no history of exposure to asbestos, feathers or other potential precipitants. and she did not smoke. At this time on exertion her respiratory rate was 56/minute and her SpO2 decreased from 98% at rest to 92% on exertion. Her peak expiratory flow rate (PEFR) was 350 lpm (best 450 lpm) and pulse rate 120 bpm. Cardiovascular examination demonstrated an elevated jugular venous pressure. Heart sounds were normal. Respiratory examination showed reduced air entry at the lung bases. There was no gross muscle weakness and neurological examination was normal. She was admitted to hospital for further investigations and respiratory review. During her admission she was reviewed by the respiratory team and had various investigations including a CT pulmonary angiogram (CTPA), chest x-ray, ECG, arterial blood gas and echocardiogram. She was discharged two days later on treatment dose tinzaparin with a plan for outpatient respiratory and maternal medicine follow up and lung function tests.
Investigations revealed a mildly elevated creatinine kinase (439 U/L), positive ANA antibodies (titre >1/640) and positive Anti-Ku antibodies (SSc/PM/SLE overlap associated antibody). Transthoracic echocardiogram illustrated good left ventricular function in the context of a fast heart rate left ventricular ejection fraction (LVEF >60%), non-dilated right ventricle, biatrial dilatation and tricuspid regurgitation which was difficult to assess due to suboptimal colour doppler assessment with a fast heart rate (unable to assess pulmonary arterial systolic pressure).

CXR on admission showing diffuse bilateral mid and lower zone hazy opacification.
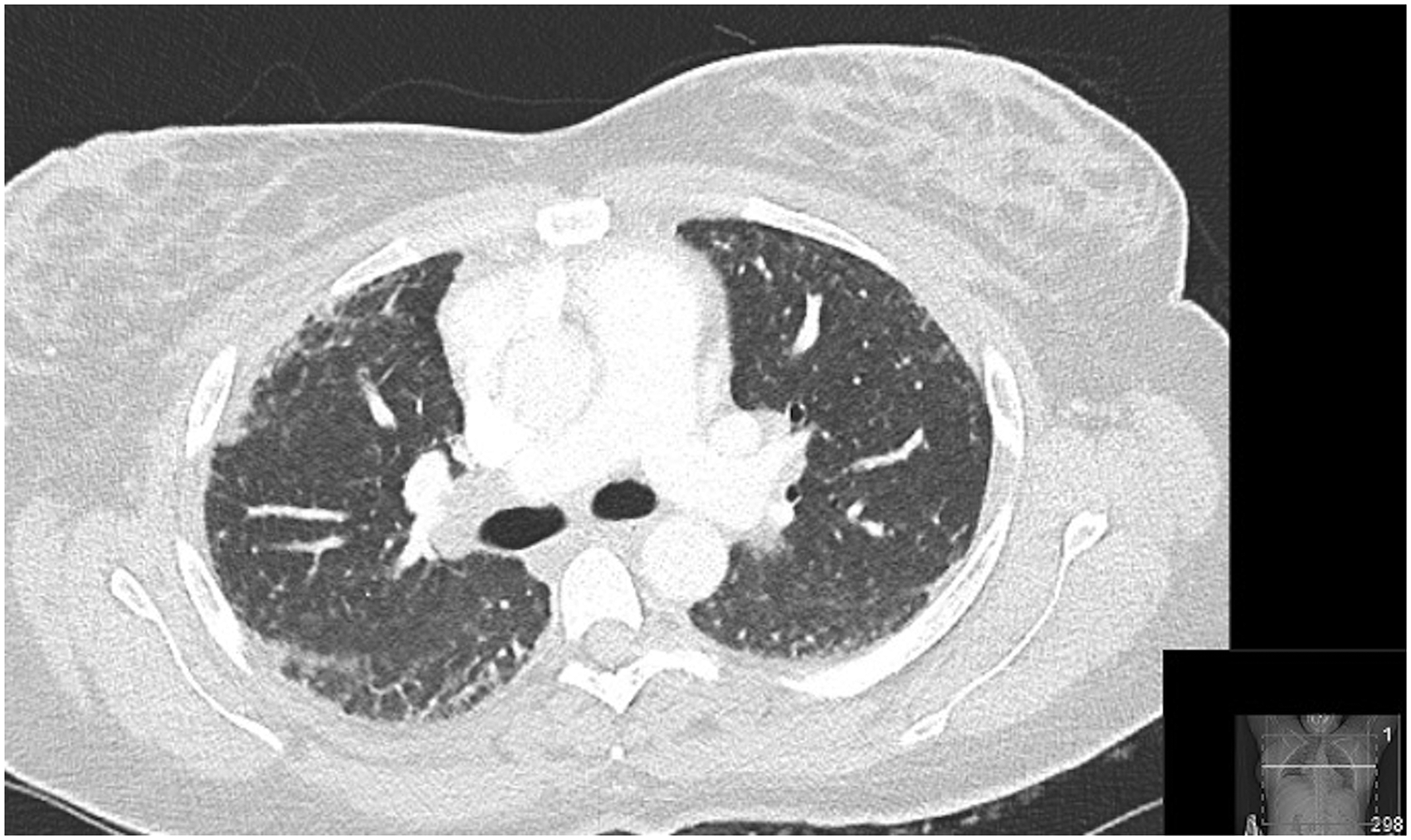
Computed tomography on admission showing subpleural ground glass opacification, early reticulation and traction dilatation at the bases, mediastinal lymphadenopathy, splenomegaly (16cm).
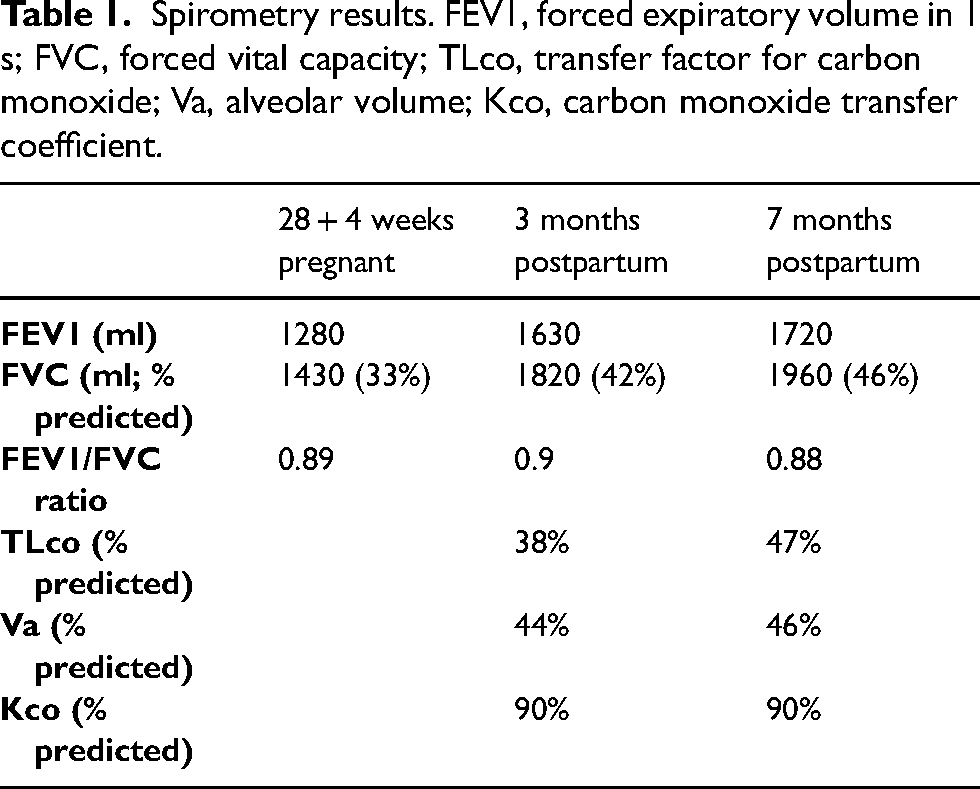
Spirometry was consistent with a restrictive deficit: FEV1 1280ml, FVC 1430ml (33% predicted), FEV1/FVC ratio = 0.9 (Table 1). A gas transfer measurement was not obtained as she was unable to achieve a minimal inspiratory lung volume of 1litre.
Spirometry results. FEV1, forced expiratory volume in 1 s; FVC, forced vital capacity; TLco, transfer factor for carbon monoxide; Va, alveolar volume; Kco, carbon monoxide transfer coefficient.
Treatment
She was seen in the maternal medicine clinic at 27 weeks with ongoing symptoms. An ILD screen was performed and referral made to the ILD team at our local tertiary centre for further input. A provisional diagnosis of connective tissue disease-associated interstitial lung disease (CTD ILD) was made and treatment with prednisolone, tacrolimus and ambulatory oxygen was initiated. Tacrolimus was offered as an option for robust immune suppression, in order to reduce the risk of progression to respiratory failure. The use of tacrolimus allowed for lower doses of corticosteroids, whilst being safe for the fetus. There were no features of infection prior to starting tacrolimus. She was also referred for rheumatology and neurology review. Despite neurological examination being normal it was felt that the degree of breathlessness was out of keeping with the degree of ILD and in view of this, and a mildly elevated CK and positive anti-Ku antibodies, there was a suspicion of an inflammatory myopathy with respiratory muscle involvement. A vastus lateralis muscle biopsy was therefore performed which showed no features of myositis.
Her dyspnoea improved after initiation of immune suppression and home oxygen therapy, however at 34 weeks she presented acutely with a deterioration in her breathing and a new productive cough. She was treated with antibiotics for a presumed lower respiratory tract infection and transferred from her local hospital to the tertiary centre in view of the possibility of needing delivery. Chest x-ray was unchanged from previous. A decision was made for induction of labour and she had an unassisted vaginal delivery of a live-born female weighing 1610g with normal Apgar scores. She was on 3 litres of oxygen during labour.
Following delivery she was initiated on methylprednisolone 1g/day for 3 days for possible myopathy contributing to her worsening dyspnoea. She also had a CTPA which showed no pulmonary emboli and stable background pulmonary changes. By three months following delivery, her symptoms had greatly improved and she could run upstairs and did not require home oxygen therapy. She has remained on tacrolimus and prednisolone. She has been reviewed by dermatology due to a history of rash which they did not feel was consistent with a diagnosis of dermatomyositis and has now been discharged from dermatology and neurology. Care under the ILD team is ongoing.
Discussion
ILDs are a heterogeneous group of disorders, characterised by thickening of the interstitium, which may be a result of inflammation, scarring, or fluid build-up. Some forms of ILD may be complicated by pulmonary fibrosis and pulmonary hypertension.
There is very limited published data on potential outcomes or complications of pregnancy with the disease. ILDs may arise de novo in pregnancy or a previous known ILD may be exacerbated during pregnancy. 2 ILD may be idiopathic or secondary to drugs, sarcoidosis or connective tissue disease such as polymyositis. 1
A common presenting symptom in ILD is exertional dyspnoea, however this is also a typical symptom of normal pregnancy. Cough might help distinguish normal physiological changes of pregnancy from a new diagnosis of ILD. 3 Our patient presented with an interstitial pneumonia with autoimmune features; however her breathlessness was out of keeping with the degree of ILD, therefore a suspicion for inflammatory myopathy with respiratory muscle involvement was raised. Patients should always be asked about extrapulmonary symptoms that might help suggest a systemic condition.
Normal pregnancy results in a decrease in functional residual capacity as both expiratory reserve volume and residual volume are reduced. Large airway function is not usually impaired by pregnancy, and forced expiratory volumes and FEV1/FVC ratio is unaffected. Progesterone increases ventilation by increasing respiratory centre sensitivity to carbon dioxide as a result the tidal volume and minute ventilation is increased. The respiratory rate is not affected. This results in a decrease in arterial and alveolar carbon dioxide pressure. The respiratory alkalosis is compensated by an increase in excretion of bicarbonates by the kidneys, resulting in a normal pH. 4
On pulmonary function testing, the most common ventilatory defect seen in patients with parenchymal lung disease, a characteristic consequence of ILD, is a restrictive defect. Although spirometry does not change greatly through the course of a normal pregnancy, this may not be the case in restrictive lung disease where the increase in inspiratory capacity may be insufficient to compensate for the fall in expiratory reserve volume. 5 The improvement seen in lung function testing in this patient (Table 1) is therefore consistent with recovery from pregnancy and stabilisation of lung, and possibly muscle disease. The persistent restriction is likely related to a degree of pulmonary fibrosis and a BMI of 34 kg.m2.
The combined restrictive lung physiology of pregnancy and ILD can lead to severe pulmonary symptoms and hypoxemia. An ILD flare and venous thrombosis are also prime concerns in pregnancy. 3 There is a higher rate of miscarriage, premature delivery, and fetal growth restriction. 6 In patients with known ILD, pre-conception planning should include discussion of the possible increased risk of complications, stabilisation of pulmonary disease, and immune suppressive drugs contraindicated in pregnancy should be stopped. 2 Respiratory function should be assessed before conception as it is a major factor influencing maternal and neonatal outcome. 2
Treatment options for ILD during pregnancy include steroids, azathioprine, tacrolimus and oxygen supplementation. 7 Other drugs may be necessary in severe disease, based on a balance of risks. Labour and delivery should be managed according to obstetric indications, 3 however increased work and oxygen consumption during labour may not be tolerated well, resulting in an increased risk of respiratory failure requiring ventilatory support. 3 Authors of a recent retrospective study of 67 patients with ILD in pregnancy concluded ‘while adverse pregnancy outcomes are common in ILD pregnancies, especially in patients with more severe disease, overall maternal morbidity and mortality is low’. 8 As evidenced by this case, the management of ILD in pregnancy requires close monitoring and management by a multidisciplinary team to achieve a successful outcome.
Footnotes
Acknowledgements
None.
Contributorship
SP wrote the first draft of the manuscript. All authors reviewed and edited the manuscript and approved the final version of the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Whipps Cross University Hospital does not require ethical approval for reporting individual cases.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Written informed consent was obtained from the patient for their anonymised information to be published in this article
Guarantor
RA guarantees the manuscript's accuracy and the contributorship of all co-authors.