
Abstract
Antisynthetase syndrome (anti-SS) is an autoimmune condition characterised by autoantibodies against aminoacyl tRNA synthetases. Clinical features can include interstitial lung disease (ILD), myositis, Raynaud's phenomenon and arthritis. Described here is a 25-year-old pregnant woman with anti-SS with worsening ILD in the latter part of pregnancy, requiring emergency delivery at 36 weeks and 3 days of gestation.
Introduction
Antisynthetase syndrome (anti-SS) is an autoimmune condition characterised by autoantibodies against aminoacyl tRNA synthetases. Clinical features can include interstitial lung disease (ILD), myositis, Raynaud's phenomenon, skin changes and arthritis. There is a higher prevalence and increased severity of ILD in patients with anti-SS compared to dermatomyositis or polymyositis, and patients often require multi-modality immunosuppressive therapy. 1 Long-term care includes consideration of the effects of immunosuppression, such as malignancy and infection, and pulmonary sequelae of the disease, such as pulmonary hypertension and the need for lung transplantation. Few cases of pregnancy associated with anti-SS have been reported.
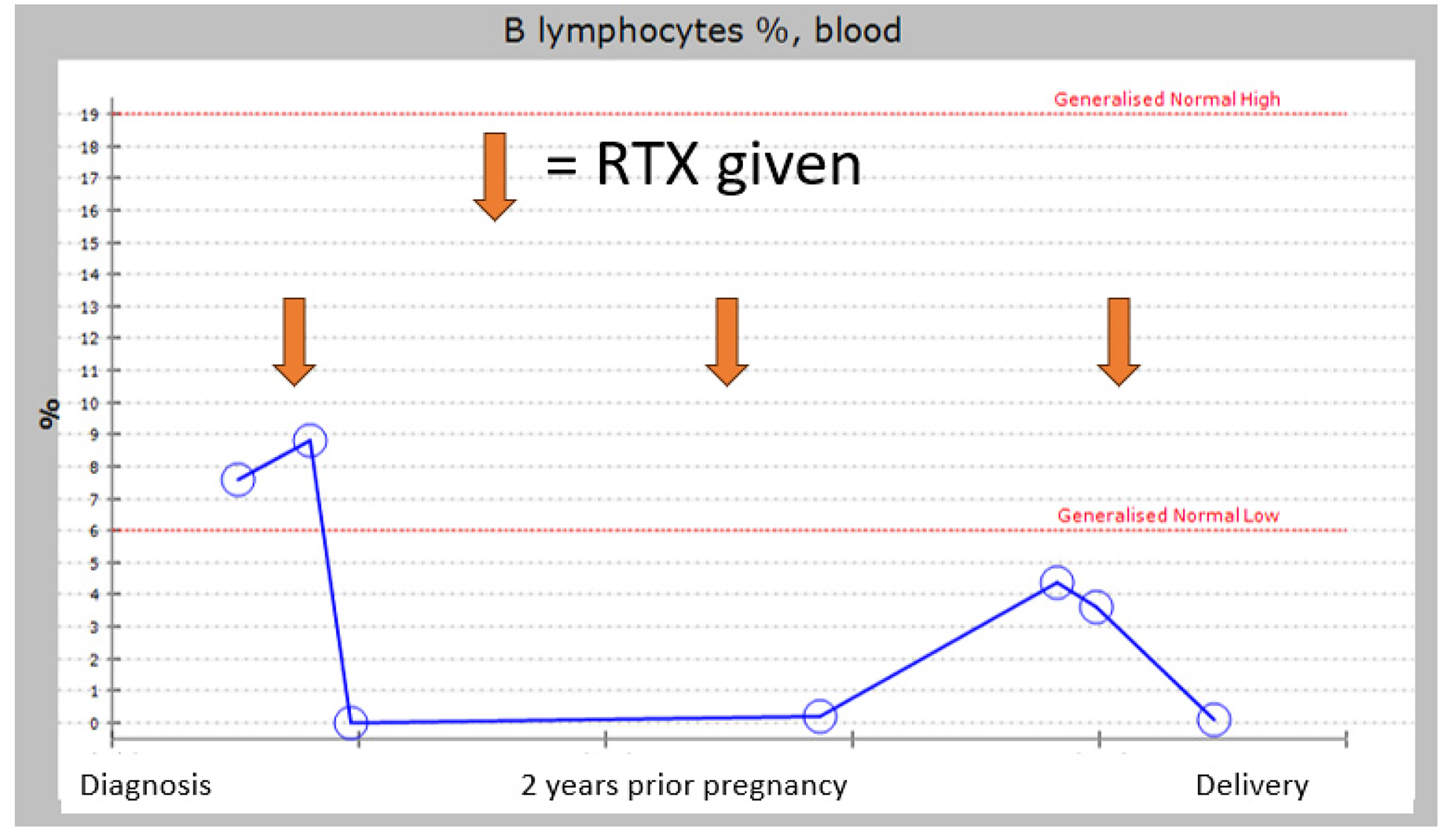
B lymphocyte % from diagnosis to delivery.
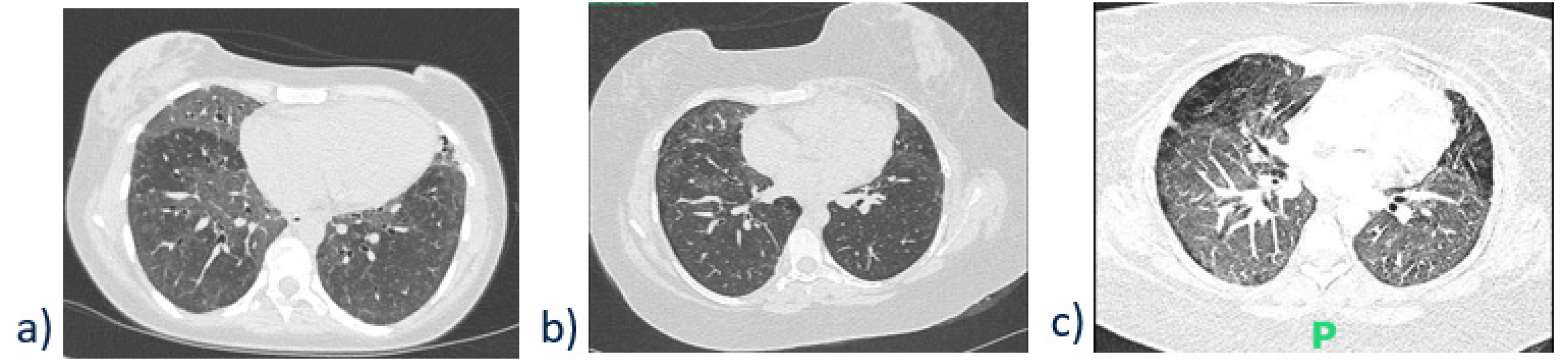
CT chest images: (a) at diagnosis, (b) at pre-pregnancy clinic and (c) on admission during which she delivered.
Case report
A 25-year-old woman was pregnant for the second time. Her first pregnancy was 4 years prior, and she underwent a surgical termination of pregnancy at 10 weeks around the time of her diagnosis of anti-PL7-positive anti-SS. She was ANA/dsDNA/anti-Ro/La/anti-Jo-1 negative. Her creatine kinase (CK) level was normal.
She had never smoked and had no occupational exposure to potential causative agents associated with ILD. There was no other significant past medical history apart from anaemia due to menorrhagia (corrected prior to pregnancy). She had no significant family history.
She initially presented during her first pregnancy with shortness of breath, generalised weakness, myalgia and 7 kg of unintended weight loss in 3 months. The diagnosis was made on the identification of the clinical constellation of symptoms, antibody positivity and high-resolution computed tomography (HRCT) findings. Her initial treatment was pulsed methylprednisolone followed by oral steroids. Mycophenolate mofetil (MMF) and hydroxychloroquine (HCQ) were added on shortly after due to residual symptoms. Six months later, she received rituximab (RTX), which led to a radiological improvement on HRCT (see Figure 2), and she weaned off steroid treatment. She received pre-pregnancy counselling and subsequently changed from MMF to azathioprine (AZA) 100 mg daily alongside folic acid 5 mg daily and aspirin 150 mg daily for prevention of pre-eclampsia, the latter advised from 12 weeks of any future pregnancy. She was advised to delay conception; however, she then conceived a month later.
She received a dose of RTX at 14 weeks of pregnancy after counselling about the risks of neonatal B-cell depletion and the benefit of disease control (see Figure 1). Despite this, she developed marked exertional desaturations at 13 weeks of pregnancy, and she was started on home oxygen 2 L/minute around that time. She used it sporadically, however, due to practical challenges like heavy weight of equipment. Table 1 illustrates her respiratory function over time.
The anomaly scan was normal, and an echocardiogram showed no evidence of pulmonary hypertension. Her CK level fluctuated but remained within the normal reference range. B lymphocyte count remained appropriately suppressed.
She received several courses of antibiotics during the second and third trimesters for presumed chest infection, usually with some improvement in symptoms reported. At 36 weeks’ gestation, she had an emergency admission due to worsening shortness of breath, generalised body ache, leg swelling, paroxysmal nocturnal dyspnoea and increasing oxygen requirement.
Investigation showed mildly elevated brain natriuretic peptide (176 pg/ml) and C-reactive protein (20 mg/L), normal white cell count, low procalcitonin, negative respiratory viral panel and depleted B cells (0.1%). Bedside echocardiogram showed normal biventricular function with no significant pulmonary hypertension. As Figure 2 shows, CT pulmonary angiogram showed no pulmonary embolism but bilateral increased ground glass changes.
Infection could not be excluded in the immunosuppressed patient, but exacerbation of ILD seemed more likely. Therefore, she was treated with both pulsed methylprednisolone for 3 days and antibiotics (piperacillin-tazobactam and erythromycin).
Caesarean delivery was performed at 36+3 weeks due to progressive shortness of breath and hypoxia (saturation of 80% on pulse oximeter at rest), after discussion about mode of delivery with the patient, with the hope that her respiratory function would improve with delivery of the fetus.
A male infant weighing 2660 g was delivered in good condition. The mother's respiratory function improved rapidly following the delivery (room air saturation 94%), and she went home on day 4 with a weaning of oral prednisolone.
Postnatal multidisciplinary team discussion concluded that whilst an initial infectious aetiology cannot be excluded, the acute presentation was more in keeping with a probable acute exacerbation of ILD, reinforced by the patient's treatment response. She was referred for consideration of antifibrotics (nintedanib) and lung transplant.
Discussion
Antisynthetase syndrome and antibodies
Anti-SS is an idiopathic inflammatory myopathy in the setting of a positive antisynthetase antibody and is thought to affect approximately 300,000 people worldwide. 2 Other clinical manifestations of anti-SS include fever, small joint arthritis, Raynaud's phenomenon, ‘mechanic's hands’ and rash. The mortality of the condition relates to muscle weakness and respiratory complications. Common antibodies associated with anti-SS include anti-Jo-1 (most common), anti-PL-7, anti-PL-12, anti-OJ and anti-EJ. 1 One study 3 described a case of postpartum IgA vasculitis associated with anti-PL-7 anti-SS, but renal involvement is rare. Varying clinical manifestation of the disease by the presence of antibody subtypes makes myositis and anti-SS autoantibody panel testing particularly relevant in the management of the illness.2,4 Less than 5% of patients with anti-SS are able to stop both steroid and cytotoxic drugs, and only 15% of patients achieve remission of anti-SS. 5
Antisynthetase syndrome and interstitial lung disease
Anti-SS behaves distinctively from other idiopathic inflammatory myopathy in that while its predominant clinical feature is myositis, there is often a concurrent ILD. While there may be some response to glucocorticoids, an additional immunosuppressant is often required.5–7 A proportion of patients with anti-SS also develop pulmonary arterial hypertension and, less frequently, obstructive bronchiolitis or acute respiratory failure. Clinical presentation of lung involvement can range from milder forms to a rapidly progressive disease which may lead to chronic lung damage if misdiagnosed and not properly treated. 8 The presence of ILD confers an excess 5-year mortality of over 40%, making it the defining clinical feature of the disease with respect to both morbidity and mortality.2,6
Antisynthetase syndrome and pregnancy
There is a limited but increasing body of evidence on anti-SS in pregnancy. To the best of our knowledge, seven cases of anti-SS have been reported in pregnancy so far, as summarised in Table 2.
Lung function pre- and during pregnancy.
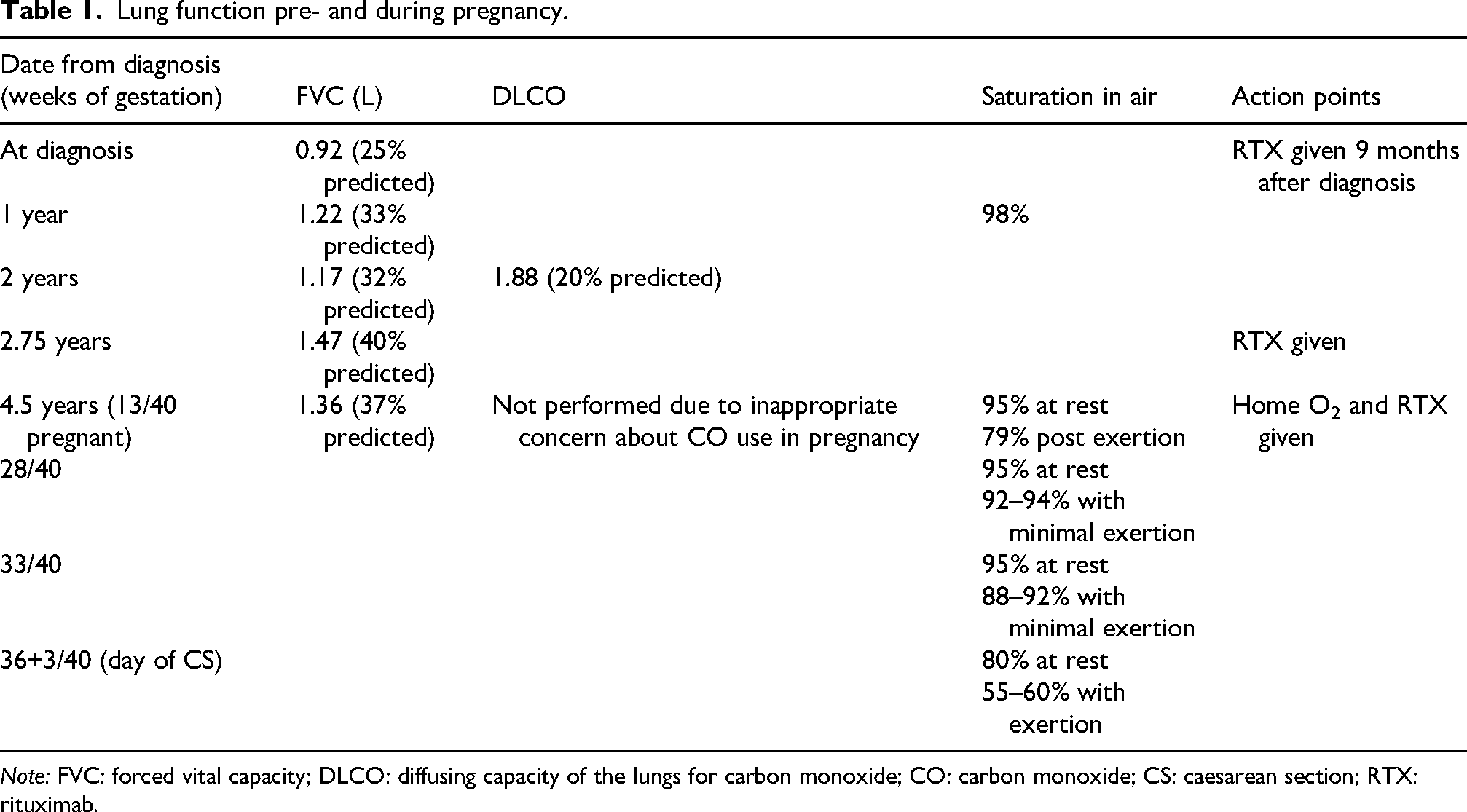
Note: FVC: forced vital capacity; DLCO: diffusing capacity of the lungs for carbon monoxide; CO: carbon monoxide; CS: caesarean section; RTX: rituximab.
Comparison of published cases of anti-SS in pregnancy and their outcomes.
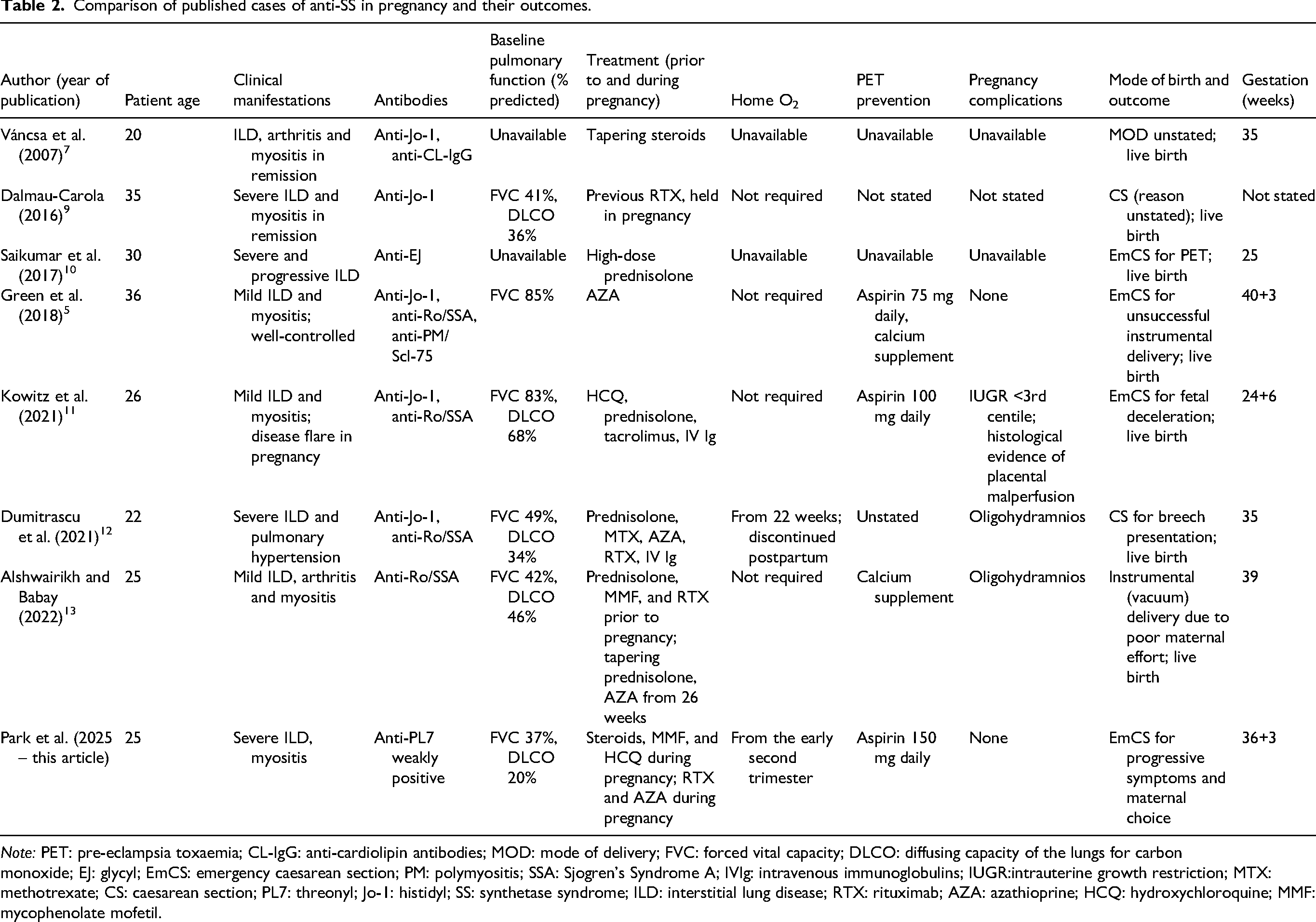
Note: PET: pre-eclampsia toxaemia; CL-IgG: anti-cardiolipin antibodies; MOD: mode of delivery; FVC: forced vital capacity; DLCO: diffusing capacity of the lungs for carbon monoxide; EJ: glycyl; EmCS: emergency caesarean section; PM: polymyositis; SSA: Sjogren's Syndrome A; IVIg: intravenous immunoglobulins; IUGR:intrauterine growth restriction; MTX: methotrexate; CS: caesarean section; PL7: threonyl; Jo-1: histidyl; SS: synthetase syndrome; ILD: interstitial lung disease; RTX: rituximab; AZA: azathioprine; HCQ: hydroxychloroquine; MMF: mycophenolate mofetil.
It is recommended that pregnancy should be planned for when the disease is quiescent and medication has been optimised through pre-pregnancy counselling.5,11 Multidisciplinary team input, involving but not limited to obstetrics, obstetric medicine, respiratory, anaesthetics, rheumatology, fetal medicine and midwifery, would be paramount to securing a good outcome for mother and baby.
We note that patients in previously reported cases5,9,11–13 had a better baseline pulmonary function profile prior to conception compared to our patient. While data is lacking to draw firm conclusions, impaired lung function and poorly controlled ILD in our patient may have contributed to rapid decline of respiratory function and flare-up of ILD during her pregnancy. Pregnancy leads to increased oxygen consumption, decreased lung volumes and increased minute ventilation, which is most pronounced in the third trimester. 11 These factors may have contributed to her pronounced deterioration towards the third trimester. It is interesting to note that she did not develop ventilatory failure (hypercapnoea) despite significant deterioration, while some women with restrictive lung disease do because of their inability to maintain the physiological increase in minute ventilation. 14 It is believed that ILD is generally well tolerated in pregnancy, even in women with severe disease. 15 However, total lung capacity <65% predicted increased likelihood of requiring oxygen at delivery. 16
There is no evidence to favour a particular mode of delivery in anti-SS. Current recommendation is that mode of delivery advice is not altered by this condition, and caesarean delivery would be advised for the obstetric indications. 5 Of note, at least five of the seven previously reported pregnancies with anti-SS required caesarean delivery; the majority of these were for obstetric indications. Whilst caesarean delivery was not mandated in the patient described here, she was concerned about managing the stress of labour given her declining respiratory function. However, current evidence suggests that delivery does not always improve maternal respiratory status.17,18
Of ongoing interest is the risk of pre-eclampsia with anti-SS. Women with connective tissue disorders are at increased risk of placental insufficiency resulting in fetal growth restriction, hypertension and rarer complications such as placental abruption and hemolysis, elevated liver enzymes and low platelets syndrome. 5 Therefore, additional growth scans should be considered. Aspirin (75–150 mg daily) from 12 weeks’ gestation is recommended in the UK national guidelines for all women with connective tissue diseases. 19 Calcium supplements are recommended by the World Health Organisation for women at risk of low-calcium diets to reduce the risk of hypertensive disorders and preterm birth. 20 The risk of pre-eclampsia is not well quantified due to the rarity of anti-SS in women of childbearing age.
Key learning points
Anti-SS is rare in pregnancy, and therefore improving clinician familiarity with the condition is important. The presence of ILD and diagnosis during pregnancy appear to be associated with poorer maternal and fetal outcomes. Lung function tests, echocardiography, regular monitoring of CK levels and regular clinical review are required during pregnancy to facilitate the early detection of deterioration. Diagnostic vigilance is required to ensure an exacerbation of the underlying condition is not mistakenly attributed to acute illness such as infection as prompt treatment would affect prognosis.
Fetal risks of connective tissue diseases have been well summarised in previous studies; this small case series detected three out of eight pregnancies associated with anti-SS which had evidence of placental malperfusion (oligohydramnios or intrauterine growth restriction (IUGR)).
Vaginal delivery is not contraindicated, but caesarean delivery may be required for obstetric indications or severe maternal illness. However, delivery does not always improve maternal oxygenation or ventilation.
Pre-pregnancy optimisation, regular monitoring and a multidisciplinary approach involving respiratory physicians, rheumatologists, obstetric physicians, obstetricians and anaesthetists are essential.
Footnotes
Acknowledgements
We would like to thank the patient for giving us permission to publish this report.
Ethical approval
Imperial College Healthcare NHS Trust does not require ethical approval for reporting individual anonymised cases or case series.
Informed consent
Written consent from the patient was obtained.
Contributorship
This article was conceived by CJF and written by EP. The final draft of the article was approved by all authors.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Note
Esther Park is currently employed by Buckinghamshire Healthcare NHS Trust.
Guarantor
CJF.