
Abstract
Objective
To assess clinical characteristics and outcomes of women who underwent concurrent valve replacement with caesarean section for severe rheumatic mitral valve disease with refractory heart failure.
Methods
All women admitted to a single centre from 2011 to 2020 with severe rheumatic mitral valve disease, having recurrent episodes of pulmonary edema on optimal medical therapy and contraindication to percutaneous balloon mitral valvotomy, who underwent concurrent valve replacement (for native valve disease) along with caesarean section, were included.
Results
Among 1300 pregnancies with rheumatic heart disease, six underwent the concurrent procedure. All had replacement of mitral valve except one who had both aortic and mitral valve replacements, between 33 and 39 weeks of gestation. There were no maternal deaths, and there was one neonatal loss from late-onset sepsis.
Conclusion
Pregnant women with severe rheumatic mitral valve disease with refractory heart failure, unsuitable for minimal access interventions, can be considered for a concurrent valve replacement with caesarean section.
Introduction
Rheumatic mitral valve disease remains the most common cardiac disease in pregnant women in emerging economies and is evolving to be a major contributor to indirect causes of maternal deaths.1–4 Hemodynamic changes in pregnancy increase the gradient across the stenosed valve, leading to the development of heart failure and arrhythmias. The burden of rheumatic heart disease (RHD) still remains high, especially in regions where access and affordability for interventions to optimise maternal condition remain out of reach for a greater proportion of the population.5–7 With the lack of pre-conceptional care and counselling, many presents in pregnancy with complications when the physiological changes pose a threat to the life of the mother and fetus.
Minimally invasive percutaneous balloon valvotomy has evolved as the procedure of choice for symptomatic mitral stenosis, even when diagnosed during pregnancy.8,9 Open cardiac surgeries under cardiopulmonary bypass (CPB) during pregnancy are possible but pose a significant challenge due to the hemodynamic effect on the mother and the fetus. 10 In situations where the mitral valve morphology is unfavourable for percutaneous valvotomy (subvalvular disease and severe valve calcification), associated with moderate to severe regurgitation and the presence of left atrial thrombus, valve replacement may be the preferred option.11,12 Cardiac surgery combined with the caesarean section may help to reduce the impact of additional circulatory changes during labour and delivery, thereby reducing the risk of maternal morbidity/mortality in such cases. 11 We aimed to assess the clinical characteristics and the outcome of concurrent valve replacements with caesarean sections for refractory heart failure in women with severe rheumatic valvular heart disease in late pregnancy from a tertiary centre in South India.
Methods
This study reports the outcome of women with symptomatic RHD who underwent concurrent valve replacement (for native valve disease) along with caesarean section during 10 years from 2011 to 2020. These patients were admitted to the Women and Children's Hospital, Jawaharlal Institute of Postgraduate Medical Education and Research (JIPMER), Puducherry, India, included from the database on RHD in the study. This centre caters primarily to the rural population of Puducherry and the neighbouring districts of Tamil Nadu. Pregnant women who underwent redo-valve replacement surgery for a stuck valve or prosthetic valve malfunction from thrombosis were excluded. Four out of six cases were part of a cohort of pregnant women with rheumatic valvular heart disease, which did not report on the details of the concurrent cardiac and obstetric surgery 1 ; and two of them were part of the ongoing cohort of RHD at the centre. This study is based on the information from the database of women with RHD from these 2 studies approved by the ethics committee. The protocol of the primary and ongoing study was approved by the Institute Ethics Committee (Human Studies), JIPMER, Puducherry, India (vide No. JIP/IEC/2016/1079 & JIP/IEC/2019/458).
All these patients underwent assessment and counselling by a multidisciplinary team including obstetricians, cardiologists, cardiothoracic surgeons, anaesthesiologists and neonatologists. After informed consent, a caesarean section was performed under general anaesthesia in the cardiothoracic operation theatre. After delivery of the baby, oxytocin infusion was started to maintain the tone of the uterus to reduce bleeding. The uterine incision was closed, and the abdominal wound was closed. Median sternotomy was performed, and full heparinisation with an activated clotting time > 450) was achieved. Aortic and bicaval cannulation was performed, and CPB was initiated. Valve replacement was performed using the standard technique, followed by weaning from CPB. Protamine was administered. After ascertaining complete haemostasis, chest closure was done. All patients were shifted to the cardiothoracic intensive care unit with minimal inotropic support, which was tapered off gradually, and they were extubated within 12–24 h. Uterotonic infusion was continued for 8 h after surgery, and heparin followed by anticoagulant were started following extubation, according to cardio-surgical protocols.
Records of these six patients were reviewed for the echocardiography findings, operative indications and the details of the surgical procedures. Neonatal outcomes and complications were also noted. Other details retrieved included cardiac diagnosis and prior interventions, maternal obstetric history and pregnancy course, medication following diagnosis, cardiovascular status prior to and after surgery, and final maternal outcome. Details of any complications till the time of discharge from the hospital and details of follow-up in the ‘Valve clinic’ under the Cardiothoracic surgery department were noted.
Results
During the time period there were 1300 pregnancies among women with RHD and six among them underwent valve replacement for native valve disease (stenosis or regurgitation) along with caesarean section. Clinical presentation at admission, management received and the operative details are shown in Table 1. All of them had severe mitral stenosis and pulmonary hypertension; one each had left atrial thrombus and atrial fibrillation. The multidisciplinary team (MDT), after discussion, decided on the combined procedure in view of recurrent episodes of pulmonary edema, not responding to medical therapy and New York Heart Association (NYHA) functional class III/IV. All were unsuitable for percutaneous balloon mitral valvotomy on assessment, either due to the presence of moderate to severe mitral regurgitation, sub-valve disease or with valve calcification as shown in Table 1.
The clinical features and medication at presentation with heart failure and the operative details of the women.
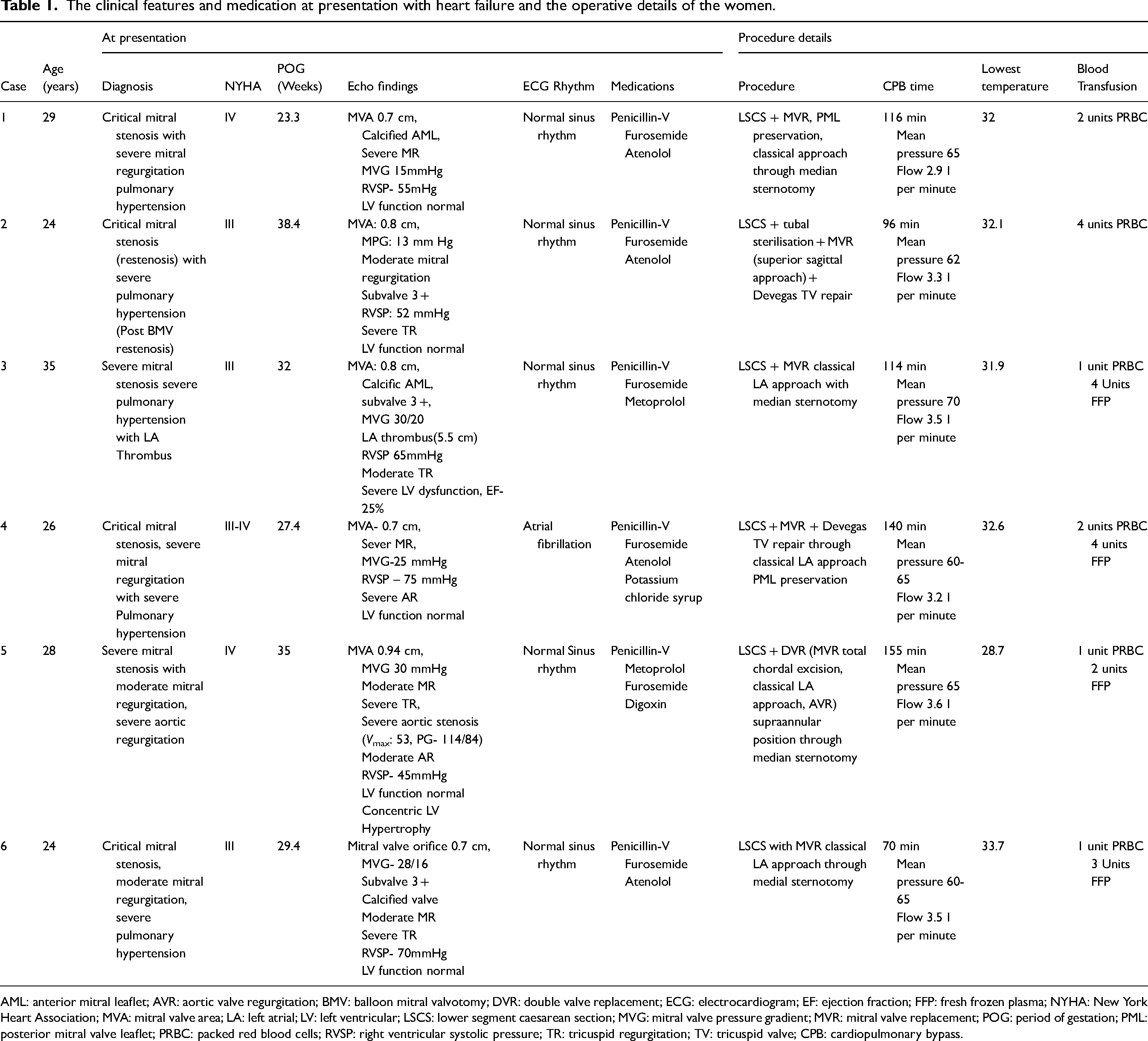
AML: anterior mitral leaflet; AVR: aortic valve regurgitation; BMV: balloon mitral valvotomy; DVR: double valve replacement; ECG: electrocardiogram; EF: ejection fraction; FFP: fresh frozen plasma; NYHA: New York Heart Association; MVA: mitral valve area; LA: left atrial; LV: left ventricular; LSCS: lower segment caesarean section; MVG: mitral valve pressure gradient; MVR: mitral valve replacement; POG: period of gestation; PML: posterior mitral valve leaflet; PRBC: packed red blood cells; RVSP: right ventricular systolic pressure; TR: tricuspid regurgitation; TV: tricuspid valve; CPB: cardiopulmonary bypass.
Caesarean section was performed prior to the valve replacement in all cases. All had valve replacement in mitral valve position except one who underwent replacement in both aortic and mitral valve position. Two underwent concomitant DeVega tricuspid annuloplasty for associated moderate to severe tricuspid regurgitation. CPB duration ranged from 70 to 155 min. All surgeries were performed under hypothermia (28.7–33.7 °C). Mean arterial pressure on bypass was maintained between 60 and 70 mmHg and the flow rate at 2.9–3.5 l/min.
There were no maternal deaths among these six women. Birthweight ranged from 1400 to 2800 g, with gestational age at delivery between 32.4 and 39 weeks. (Table 2) All babies were shifted to the neonatal intensive care unit as mothers were on elective ventilation. Five among the six newborns were low birth weight (< 2500 g) and one among them succumbed to neonatal sepsis on the fourth postnatal day.
The maternal and perinatal outcomes.
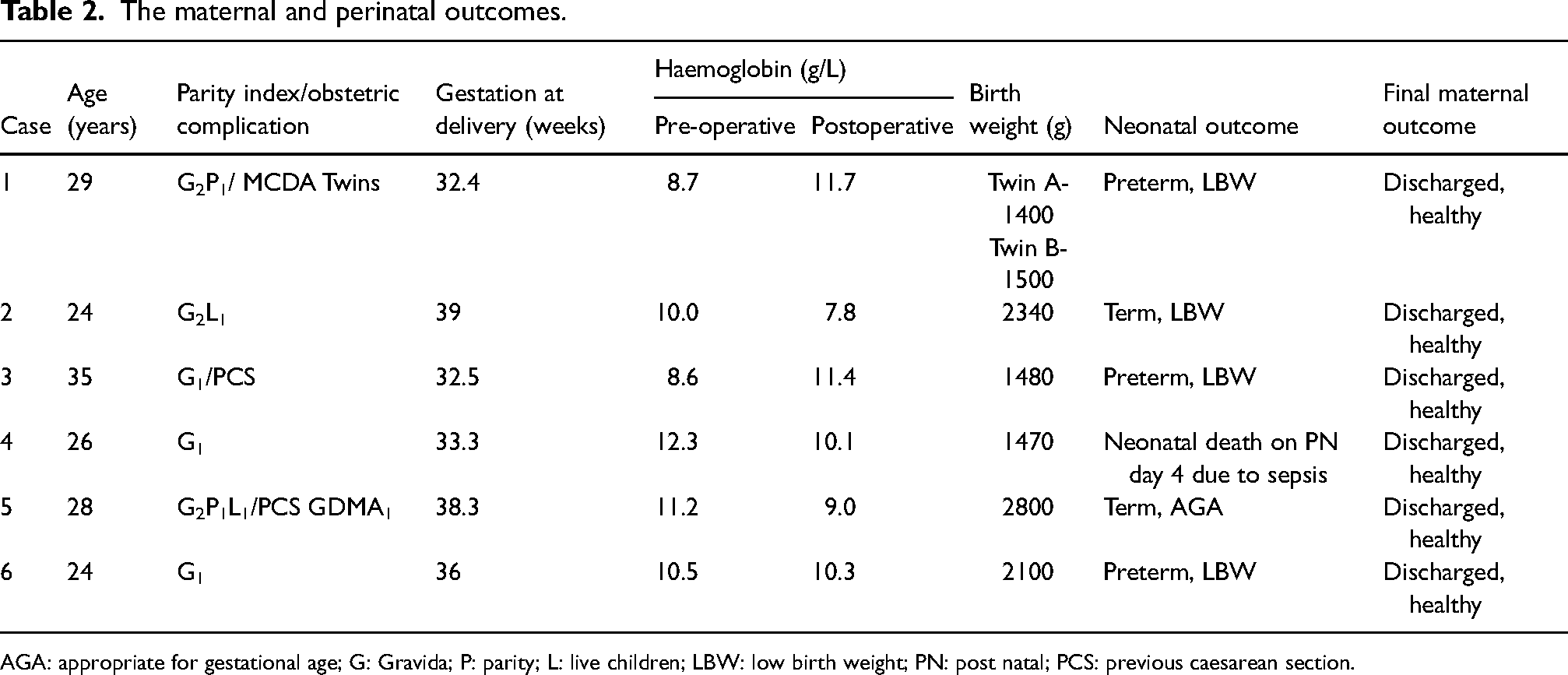
AGA: appropriate for gestational age; G: Gravida; P: parity; L: live children; LBW: low birth weight; PN: post natal; PCS: previous caesarean section.
On follow-up of these women in the Valve clinic (duration varying from 6 months to 2.5 years), all women were continued on therapeutic anticoagulation without any adverse cardiac events or complications. On their review, the prosthetic valve was functioning well.
Discussion
Pregnant women presenting with symptomatic severe mitral valve disease pose a challenge to the treating team due to increased maternal morbidity or mortality risk. Circulatory changes such as an increase in stroke volume and heart rate, along with the additional increase occurring during labour and delivery, make them vulnerable to life-threatening complications such as heart failure and arrhythmias. The risk increases when they are diagnosed for the first time during pregnancy without optimising their condition with medical therapy. In symptomatic patients unresponsive to medical treatment, with situations unfavourable to minimally invasive interventions such as percutaneous balloon mitral valvotomy (PBMV), near-term, open cardiac surgery may be the preferred option to reduce maternal morbidity and mortality.
There are very few reports of cardiac surgery performed during pregnancy on CPB, but maternal mortality rates varying from 3% to 15%.11–13 These rates are similar to those of the nonpregnant population when it is a planned procedure under the supervision of an MDT. Due to concerns about the adverse haemodynamic and physiological effects of the CPB on the mother and fetus in some of the earlier reports, the strategy of the caesarean section followed by the valve replacement was followed, as is done in this series.11,12,14–16 This strategy helps to avoid the risk of reduction in the uteroplacental circulation during bypass, which can lead to hypoxia and in utero fetal death. This resulted in no procedure-related pregnancy losses. One preterm infant died on the fourth post-natal day due to late-onset neonatal sepsis.
In the immediate postpartum period, anticoagulation with heparin to maintain the CPB and the various anaesthetic agents may increase the risk of major postpartum haemorrhage, which may even necessitate a lifesaving hysterectomy. Timely use of continuous oxytocic infusion and other agents such as misoprostol to maintain the uterine tone is the key to reducing this risk, as is the meticulous haemostasis following caesarean section.10,11,15,17
Most earlier series reported had heterogeneous study populations i.e. those with prosthetic heart valve dysfunction and native valve disease, in whom a concurrent valve replacement and caesarean section was performed.11,18–20 In the present series, we focussed on a cohort of pregnant women in the third trimester who had contraindication for a PBMV, where the options were (a) to allow progression to labour/caesarean section without an intervention with resultant increased risk of mortality or (b) to perform the concurrent valve replacement with the caesarean section with risk of the procedure and postpartum haemorrhage. In an earlier published cohort from the same centre, the majority of maternal mortality (10/12 deaths) was due to mitral valve disease with refractory heart failure and unfavourable valve morphology, following which MDT discussion initiated the open surgical approach to reduce the morbidity/mortality. 1 The timing of the surgery needs to consider the maternal condition and available neonatal support to balance the risk of the maternal complication and neonatal complications of prematurity. In the present series, the severity of the maternal condition (especially in cases 1, 3, and 5) necessitated delivery before 34 weeks, after discussion with the MDT. The study is limited by its small sample size, being a series from a single centre. Undertaking a randomised controlled study to safety in this vulnerable subset of patients may not be ethically appropriate. This points toward the need for developing registries of cardiac disease in low-to-middle income countries (LMIC), where the settings differ from those in high-income countries.
Gender disparity, especially in the rural region in LMIC, for access to education and care has led to more adolescent/young women getting diagnosed in advanced stages of their cardiac disease.5–7 Lack of access due to socio-economic constraints and availability of expertise limited to regional centres lead to a higher time lag between the diagnosis/decision to cardiac surgery in these regions. 7 Performing a concurrent valve replacement with caesarean section in selected cases unsuitable for interventions such as PBMV offers the dual advantage of the reduction in the impact of circulatory changes in labour/delivery and also helps to circumvent the long waiting list for surgery. This strategy can aid in reducing maternal as well as perinatal mortality/morbidity and improve the quality of life among these women.
Conclusion
With the improvement in the safety of open cardiac surgery, the strategy of the concurrent caesarean section followed by valve replacement may be considered for pregnant women with symptomatic valvular heart disease presenting in advanced pregnancy, unsuitable for minimal access interventions. Further reports from cardio-obstetric registries or multicentric observational studies are required to confirm the findings, which can aid in reducing maternal mortality and morbidity in such cases.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
All procedures performed in this study were done with the ethical standards set by the Institute Scientific Advisory and Ethical committee (Human Studies), in accordance with the 1964 Helsinki declaration and its later amendments. This study is based on the information from the database of women with rheumatic heart disease form these two studies approved ethics committee Protocol of the study and waiver of consent for the collection of the details of the women from records, admitted from 2011 to 2015, was approved by the Institute Ethics Committee (Human Studies), JIPMER, Puducherry, India. (vide No. JIP/IEC/2016/1079 and JIP/IEC/2019/458).
Informed consent
Written informed consent was obtained from all women recruited from 2015 to 2021.
Guarantor
Anish Keepanasseril
Author Contributions
AK and AAP conceived the study. All authors contributed to the design. JB, YJ carried out the data collection and guarantees data integrity. AK performed statistical analyses. AAP, NM and PK reviewed the analysis and AK and JB wrote the first draft. All authors contributed to revising and finalisation of the manuscript. AK (corresponding author) guarantees all aspects of the reliability and freedom from bias of the data presented and their discussed interpretation.