
Abstract
We present the case of a postpartum woman presenting with acute dyspnoea and hypoxia. She was found to have liver enzyme derangement with evidence of synthetic dysfunction. Computed tomography of her chest showed ground-glass opacities. The causes of this phenomenon are discussed, including the difficulties in differentiating amniotic fluid embolism and acute fatty liver in pregnancy. Pulmonary fat embolism is also considered as a differential diagnosis.
Keywords
Introduction
The development of acute dyspnoea and hypoxia following delivery compels consideration of a range of aetiologies (Table 1). A case of acute respiratory deterioration associated with ground glass opacities on computed tomography (CT), together with hyper bilirubinaemia, elevated liver enzymes, and coagulopathy is presented. The main diagnoses considered, and the possible mechanism of respiratory compromise, are discussed.
Causes of acute peripartum hypoxia.
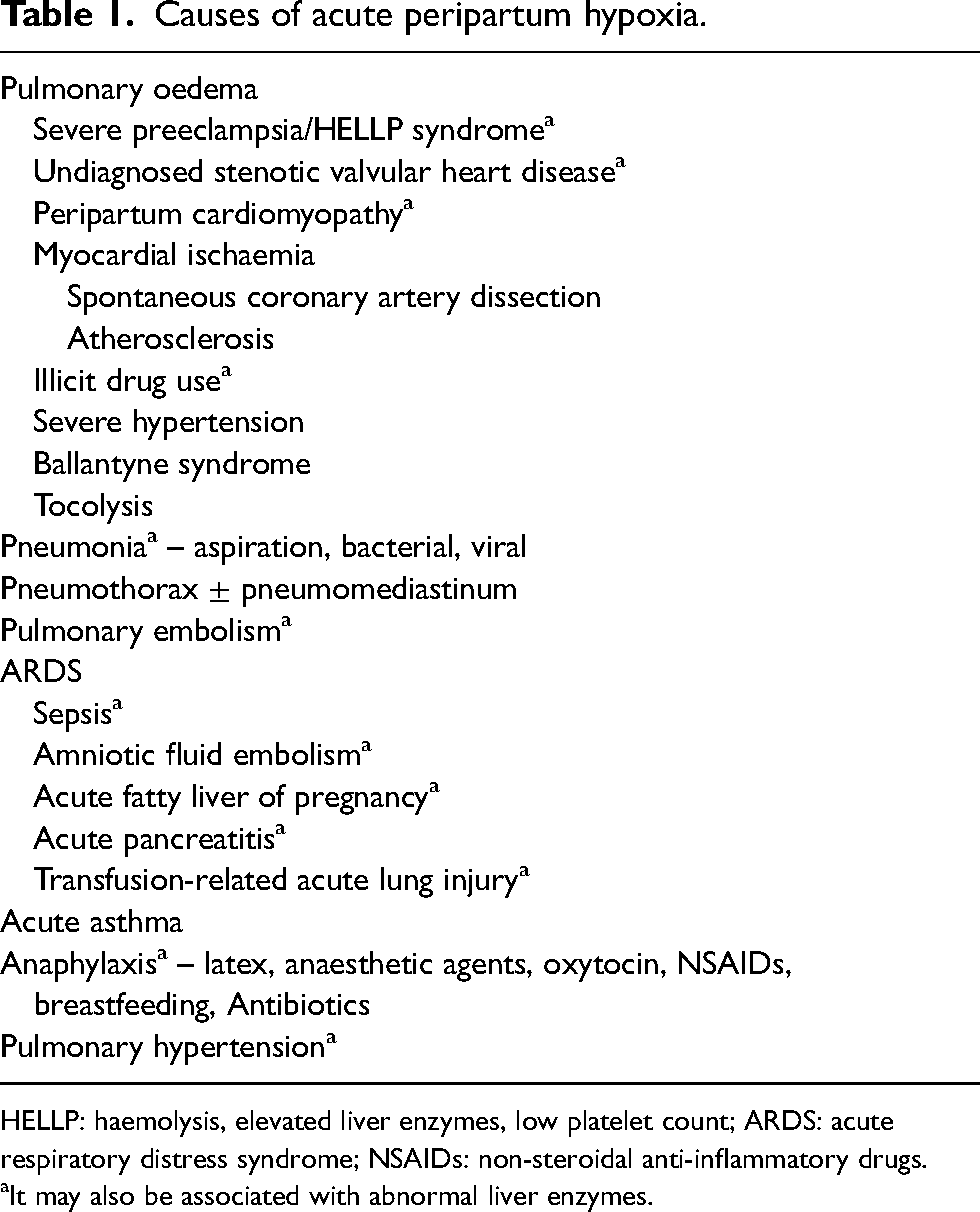
HELLP: haemolysis, elevated liver enzymes, low platelet count; ARDS: acute respiratory distress syndrome; NSAIDs: non-steroidal anti-inflammatory drugs.
It may also be associated with abnormal liver enzymes.
Case
A 33-year-old woman, gravida 11 para 6, was transferred from another hospital 24 h postpartum in the context of hypoxia with bilateral ground-glass opacities on CT, and elevated liver enzymes with evidence of impaired hepatic synthetic function.
The woman had presented with preterm labour at 35 weeks’ and 3 days’ gestation, delivering a 1900 g female infant by vaginal delivery, with estimated blood loss of 150 mL. The pregnancy had been complicated by fetal growth restriction, with the finding of large connatal and anterior temporal cysts on fetal ultrasound and magnetic resonance imaging. Single nucleotide polymorphism microarray on amniotic fluid detected a 850 kb deletion at 15q11.2. Parental studies did not detect a deletion. Her past medical history was significant for longstanding postural orthostatic tachycardia syndrome, and gastric bypass 1 year prior to conception, which resulted in a 45 kg weight loss and preconception body mass index of 18 kg/m2. The woman was not taking any medications, herbal or complementary medications, was a non-smoker and non-drinker, and denied illicit drug use.
Within 1 h of delivery, the woman noted shortness of breath but denied sputum production, haemoptysis or chest pain. Several episodes of maternal vomiting were noted. Physical examination revealed apyrexia, with oxygen saturations of 92% on room air, a pulse of 130 bpm regular and a blood pressure of 105/75 mmHg. Her chest was clear to auscultation with a non-elevated jugular venous pressure. Heart sounds were dual, and her abdomen was soft and non-tender. Arterial blood gases were not performed. Chest X-ray was unremarkable, and electrocardiogram showed sinus tachycardia only. CT pulmonary angiography showed bilateral ground glass appearance but no pulmonary emboli (Figure 1). Respiratory virus testing was negative for SARS-CoV-2, influenza A and B and respiratory syncytial virus. Further investigations revealed venous glucose 3.1 mmol/L, elevated liver enzymes, and low serum albumin and fibrinogen together with prothrombin time (PT) at the upper end of the pregnancy-specific reference range, suggestive of impaired hepatic synthetic function (Table 2). Liver enzymes had been normal at 32 weeks’ gestation. Her C-reactive protein was 83 mg/L (<6), brain natriuretic peptide, serum lipase, activated partial thromboplastin time (APTT), urine protein:creatinine ratio, and hepatic ultrasound were normal. The woman was commenced on oral azithromycin and intravenous ceftriaxone to presumptively treat community-acquired pneumonia. Although remaining afebrile, she was noted to have further deterioration of oxygen saturations to 86% on room air, 12 h postpartum, prior to transfer.
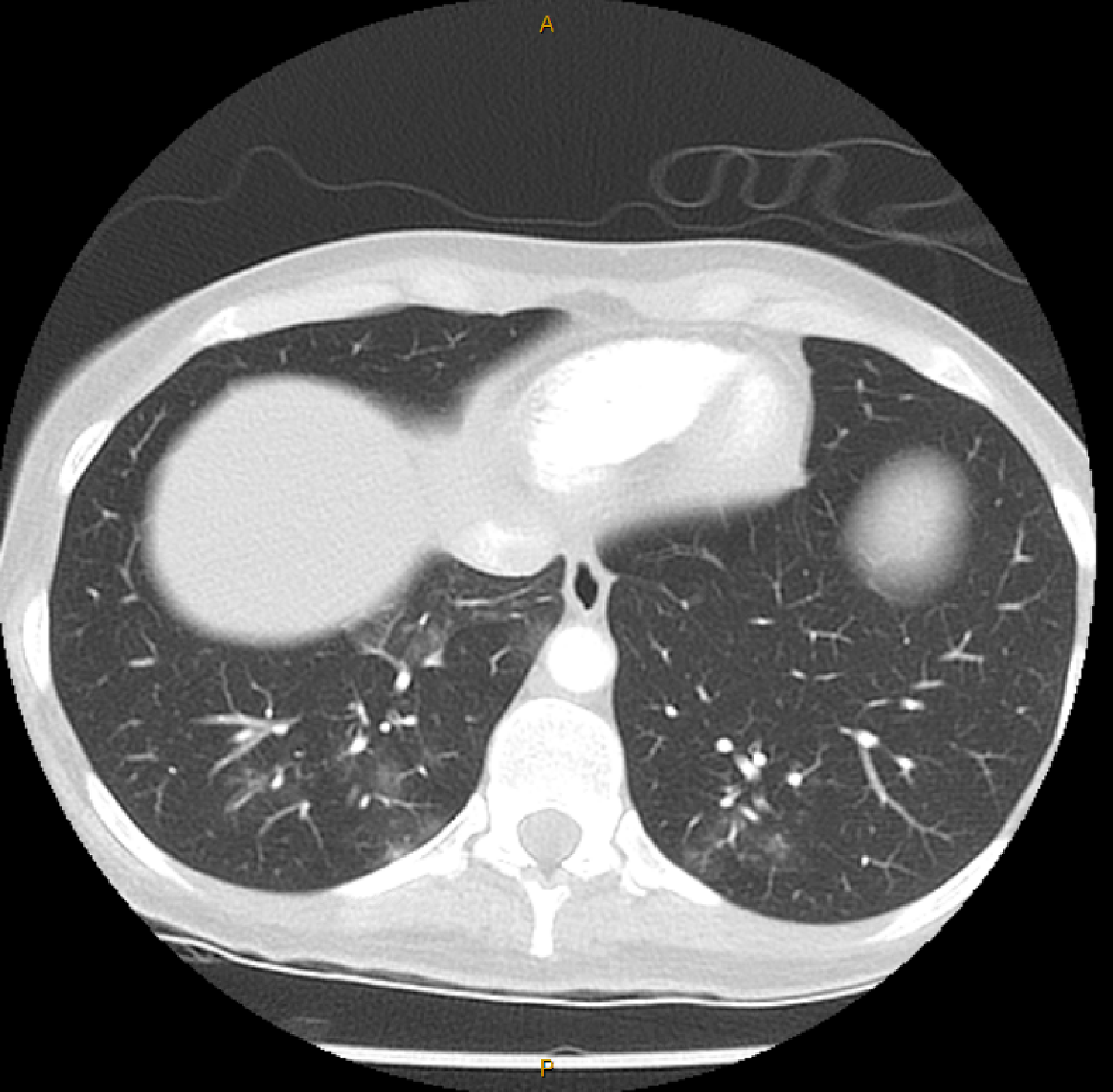
CT lungs showing ground glass opacities.
Laboratory values.

pp: postpartum; ALT: alanine transaminase; AST: aspartate aminotransferase; GGT: gamma-glutamyl transferase; PT: prothrombin time; APTT: activated partial thromboplastin time; Hb: haemoglobin; WBC: white blood cells; Plt: platelets.
Upon arrival at the receiving hospital, she had a 2 L oxygen requirement to maintain oxygen saturations above 95%. She was haemodynamically stable, aprexyial, and her chest was clear. No rash was found, and she was not encephalopathic. Repeat blood tests showed a rise in PT to 17.4 s, which did not correct on Echis time, or with vitamin K administration. Serum cholesterol was low at 2.9 mmol/L, and antithrombin III was 31% (80–120). The woman was diagnosed with acute hypoxaemic respiratory failure secondary to either acute fatty liver of pregnancy (AFLP) or amniotic fluid embolism (AFE). Antibiotics were ceased 48 h postpartum, the woman remaining afebrile. The woman's gas exchange, abnormal liver enzymes and hepatic synthetic function gradually improved over the ensuing 4 days. Further investigations excluded viral and autoimmune hepatitis, Wilson's disease and alpha-1 antitrypsin deficiency. A nutritional screen revealed the woman to be deficient in vitamins A and D, as well as selenium and zinc. Testing for long-chain hydroxyacyl-CoA dehydrogenase deficiency (LCHAD) revealed the common pathogenic hydroxyacyl-CoA dehydrogenase/3-ketoacyl-CoA thiolase/enoyl-CoA hydratase, c.1528>C (p.Glu510Gin) was not detected in mother or daughter.
Discussion
This case highlights diagnostic possibilities in the setting of combined respiratory compromise and liver injury in the early postpartum period (Table 1). Pulmonary and hepatic congestion due to cardiomyopathy, sepsis, and pulmonary embolism with right heart failure were felt to be excluded from clinical features and investigations. Major causes of acute symptomatic hypoxia with ground-glass opacities on CT include infectious and aspiration pneumonia, pulmonary oedema, pulmonary haemorrhage, hypersensitivity pneumonitis and diffuse alveolar damage with acute respiratory distress syndrome (ARDS).1,2 The most likely diagnosis, in this case, was thought to be acute hypoxaemic respiratory failure with AFLP, with AFE being less likely.
The woman fulfilled seven of the Swansea criteria consistent with the diagnosis of AFLP. The combination of prolonged PT, severely depressed antithrombin III, low cholesterol and low fibrinogen in the absence of other causes of acute liver injury are also consistent with AFLP. 3 Negative testing for LCHAD deficiency has been reported previously in women with typical features of AFLP fulfilling the Swansea criteria.4–6
The prevalence of respiratory involvement in AFLP is not known. Zhang et al. reported pulmonary infection in 21% and pulmonary oedema in 13% of 56 cases of AFLP. 7 Dwivedi et al. reported ARDS in three of seven (42.8%) women with AFLP. 8
Another potential mechanism for hypoxia in AFLP with ground glass on CT may be fat embolism. At least 20 autopsy studies have described non-traumatic pulmonary fat embolism in both acute and chronic fatty liver in non-pregnant individuals.9–12 Jones described a woman who had progressive deterioration postpartum due to AFLP, culminating in maternal death 5 days after delivery. 13 At autopsy, widespread fat emboli were identified in the microcirculation of the lungs, renal glomeruli, brain and spleen, with extensive microvesicular fatty deposits in the liver. Unfortunately, other autopsy studies of women with AFLP have not described lung histology. The absence of neurological abnormalities and petechial rash, present in approximately 59% and 33% of cases of fat embolism, respectively, may be against this as a cause of hypoxia in the woman described in this case.
The incidence of AFE is estimated to be one case in 8000–30,000 pregnancies. The American Society for Maternal-Fetal Medicine criteria for the diagnosis of AFE require:
14
Sudden cardiopulmonary collapse, or hypotension (systolic BP <90 mm Hg) with hypoxia (SpO2 <90%). Disseminated intravascular coagulation (DIC). Symptomatology either during labour or up to 30 min following delivery. Absence of fever.
AFE is the cause of 7.5%–10% of maternal deaths in the United States.
15
Recent population-based studies have reported a case fatality rate of 13%–44%.
16
Lung histology from autopsies following AFE shows pulmonary oedema, amniotic component emboli, and alveolar haemorrhage. Women who survive AFE may have complications of renal failure, ARDS, myocardial infarction, cardiomyopathy, liver failure, seizures, prolonged coagulopathy and anoxic encephalopathy.
It may be difficult to distinguish DIC from the coagulopathy of liver disease in the pregnant population, especially when considering AFE. The physiological rise in fibrinogen, and slight fall in PT, APTT and platelets in pregnancy need to be considered in the diagnosis of DIC. DIC may also complicate acute and chronic liver injury, including 50% of women with AFLP. 17 Some authors have suggested factor VIII levels are decreased with DIC, and normal or elevated in coagulopathy of liver disease; however, this has not been a consistent finding.18–20 While the woman's low fibrinogen, PT difference, and low platelets fulfil the International Society for Thrombosis and Hemostasis criteria for the diagnosis of DIC in pregnancy, the transient minimally decreased platelet value and normal APTT were atypical for this diagnosis. 21 Additionally, the woman did not manifest sudden cardiopulmonary collapse or significant hypotension.
Conclusion
In conclusion, a case of postpartum hypoxia with elevated liver enzymes and evidence of hepatic synthetic dysfunction, most likely due to AFLP is described. The differential diagnosis of peripartum hypoxia with elevated liver enzymes is broad, and careful assessment and investigation is required to make the correct diagnosis, guide acute management, as well as inform the risk of recurrence in future pregnancies.
Footnotes
Acknowledgments
None.
Contributorship
UP, CA and AM provided clinical care to the patient, and researched, wrote and reviewed the manuscript.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Ethical approval was provided by the Mater Health Human Research and Ethics Committee (EXMT/MML/105596).
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Guarantor
AM.
Informed consent
The patient provided written consent for their information to be included in this report.
Trial registration
Not applicable.