
Abstract
Amniotic fluid embolism (AFE) is a rare but potentially catastrophic pregnancy complication. This is a 10-year retrospective study on women with AFE from 2014 to 2023. Cases that met Clark's criteria or in whom a clinical diagnosis was made after exclusion of other causes were included. Information on clinical characteristics, treatment, complications and outcomes were collected and analysed. Four cases of AFE were identified. Two met Clark's criteria and presented with cardiac arrest requiring extracorporeal membrane oxygenation, of which one had cognitive and functional impairment. Two women had atypical AFE, one with disseminated intravascular coagulation (DIC)-type AFE who did not survive, and another who had paradoxical intracranial emboli from a patent foramen ovale, who had full recovery. All had coagulopathy and postpartum haemorrhage. Early recognition and initiation of cardiovascular support is crucial in AFE. DIC and haemorrhage should be treated aggressively. Survival and good outcomes of AFE are possible.
Background
Amniotic fluid embolism (AFE) is characterised by an acute cardiorespiratory collapse in a pregnant or postpartum woman associated with disseminated intravascular coagulation (DIC). While the incidence of AFE is low (1.9 to 6.1 cases per 100,000 deliveries 1 ), the mortality rate is high; aggregated data from nine population-based studies with over 17,000,000 live births from 1999 to 2016 found the overall AFE maternal mortality rate to be 20.4%. 2 Encouragingly, survival rates have improved in recent years. Data from the United States between 2000 and 2019 found the maternal mortality rate to be 17.7% with a significant decreasing trend over those years. 3
The pathogenesis of AFE is not entirely clear, but the hypothesised mechanism is the disruption in the maternal/fetal interface, causing entry of amniotic fluid into the maternal systemic circulation. This causes a complex sequence of events including (1) abnormal activation of humoral and immunological processes 4 (2) increased levels of pulmonary vasoconstrictors and mechanical obstruction from the amniotic fluid components and (3) activation of Factor VII and platelets with DIC. 5
The aim of this study is to (1) describe the critical care management and complications of AFE women in our centre, (2) report their outcomes and (3) review the literature on AFE management.
Methods
This is a 10-year retrospective study on women diagnosed with AFE from 2014 to 2023 in a tertiary hospital in Singapore. Inclusion criteria (identified through the hospital's registry) were cases that met the international diagnostic criteria for AFE, introduced by Clark et al.,
6
a working group of the Society for Maternal-Fetal Medicine and the AFE Foundation:
Acute cardiorespiratory arrest or both hypotension (systolic blood pressure (BP) less than 90mmHg) and respiratory compromise Overt disseminated intravascular coagulation (DIC) Clinical onset during labour or within 30 min of delivery of the placenta No fever (≥ 38.0°C) during labour.
We also included cases of atypical AFE, defined as women who did not strictly meet the above criteria but were believed to have AFE through the exclusion of other causes. It is hypothesised that the activation of the immune system and the coagulation cascade is closely intertwined in AFE.
7
Atypical AFE may reflect the varying involvement of these components.
8
Data on clinical characteristics, treatment, complications, and outcomes were collected and analysed. The SingHealth Institutional Review Board (IRB No. 2023/2567) waived the need for ethics approval and patient consent for the collection, analysis and publication of the retrospectively obtained and anonymised data for this non-interventional study.
Results
We identified two women with AFE meeting the Clark criteria and two with atypical AFE (Table 1).
Summary of AFE cases.
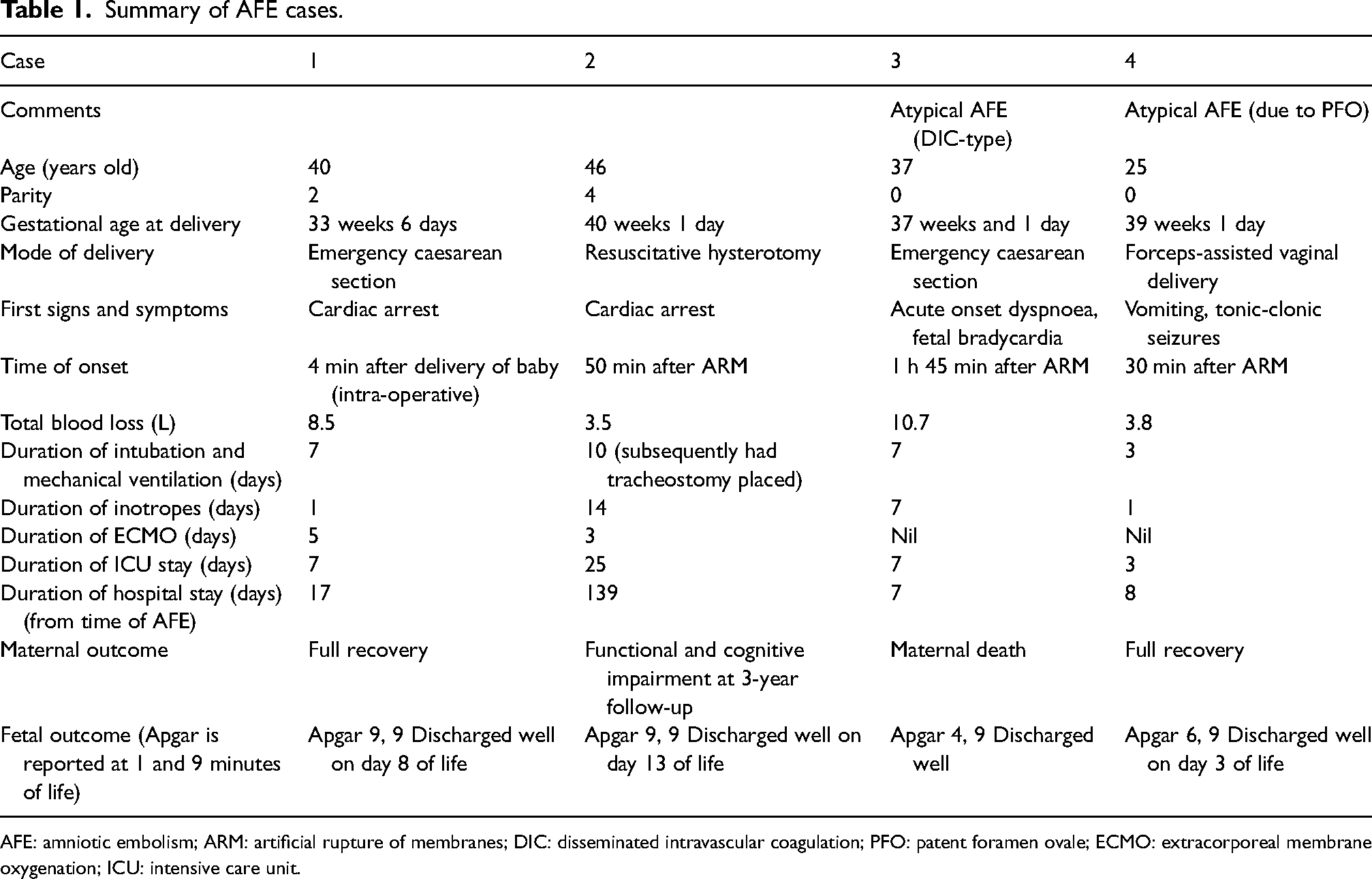
AFE: amniotic embolism; ARM: artificial rupture of membranes; DIC: disseminated intravascular coagulation; PFO: patent foramen ovale; ECMO: extracorporeal membrane oxygenation; ICU: intensive care unit.
Case 1
A 40-year-old Malay woman with two previous caesarean sections (CS) had gestational diabetes mellitus (GDM) on diet control and placenta previa. She had antepartum haemorrhage at 33 + 6 weeks of gestation. In view of a suspicious cardiotocograph (CTG), an emergency CS was performed under regional anaesthesia. Her baby required free-flow oxygen initially but was discharged well at 35 weeks corrected gestational age.
Four minutes after delivery, the woman became acutely drowsy with sinus bradycardia (heart rate 40 beats per minute). Two doses of intravenous atropine 0.6 mg were administered but the woman went into cardiac arrest 6 min later. Cardiopulmonary resuscitation (CPR) was immediately commenced and she was intubated. Return of spontaneous circulation (ROSC) was achieved 6 min later. Massive transfusion protocol (MTP) was activated for ongoing heavy uterine bleeding and she was given one cycle (i.e. 4 units of red cell concentrate, 2 units of fresh frozen plasma (FFP), 1 unit of pool platelet concentrate). An emergency hysterectomy was also performed. Despite this, she remained hypotensive requiring continued adrenaline boluses. A bedside echocardiogram showed right ventricle (RV) strain with raised pulmonary pressures and cardiac failure. Extracorporeal membrane oxygenation (ECMO) was activated and right femoral veno-arterial (VA) ECMO cannulation was done.
Post-operatively, the woman developed tachycardia and abdominal distension with a high drain output. An ultrasound showed significant intraabdominal fluid. A relook laparotomy performed found bleeding from the right inferior epigastric artery, infundibulopelvic ligament, and ovarian serosa. Haemostatic sutures were placed and the abdomen was temporarily packed. The ECMO circuit was anticoagulation-free in view of DIC. Her coagulopathy was aggressively corrected and the abdomen was closed two days later when the drain outputs remained low and the haemoglobin trend was stable.
ECMO was explanted on postoperative day 5 as repeat echocardiograms showed improvement in the left ventricular ejection fraction (LVEF) during the weaning study. She however developed critical limb ischaemia from right common femoral artery thrombosis and underwent groin cutdown and embolectomy. Subsequently, she was started on therapeutic low-molecular-weight heparin and anticoagulated for three months.
The woman was extubated on post-operative day 7 and discharged well 10 days later. At her two-month postnatal review, she had full neurological function and no apparent cognitive deficits.
Case 2
A 46-year-old Chinese woman with a history of breast cancer post-surgery and chemoradiotherapy, was in her fifth ongoing pregnancy. She had an uneventful course and was induced with dinoprostone for a post-term pregnancy. An artificial rupture of membranes (ARM) was performed and she was started on a low dose of oxytocin (3 mL/hour). 50 min later, she collapsed with no pulse or recordable BP, with fetal bradycardia. CPR was commenced and a resuscitative hysterotomy was performed. Her baby girl was born at 3.25 kg. The baby required free-flow oxygen at birth and was discharged well.
Post-delivery, resuscitative efforts were continued with CPR, adrenaline boluses and MTP activation. As there was no sustained ROSC, ECMO was activated and initiated 1.5 h from collapse. In view of ongoing bleeding (4L estimated blood loss), persistent hypotension, severe anaemia and DIC despite aggressive resuscitation, a hysterectomy was performed 6 h from the time of collapse.
Post-operatively, she developed multiple organ-system complications in the intensive care unit (ICU). She required short-term dialysis support for severe acute kidney injury. A CT brain done in view of persistently low level of consciousness showed cerebral watershed infarcts from hypoperfusion, and inotropes were titrated to maintain cerebral perfusion pressures. MRI brain done for flaccid paralysis showed chronic haemorrhagic infarcts (possibly from small emboli). Electroencephalograms showed severe diffuse encephalopathy but neurological prognostication was indeterminate.
She also had acute respiratory distress syndrome complicated by pneumothorax which improved with the insertion of a chest drain. In view of the expected prolonged ventilation due to the poor neurorecovery, a tracheostomy was placed on postoperative day 10.
Two days after ECMO, the woman developed left lower limb compartment syndrome and underwent fasciotomy. This was complicated by necrotic muscle and wound infection requiring debridement, and fast atrial fibrillation (AF) post-ECMO decannulation requiring cardioversion. She had recurrent AF associated with infection and electrolyte derangements. Electrolytes were replaced accordingly and she was given amiodarone and bisoprolol. She developed a right upper limb deep vein thrombosis secondary to the peripherally inserted central catheter (PICC) line. The PICC was removed and she was started on an anticoagulant and continued indefinitely in view of AF.
She underwent multiple relook laparotomies and small bowel resection for ischaemia. There was sepsis secondary to enterocutaneous fistula (ECF) in the distal ileum contributed by the vacuum-assisted closure (VAC) dressing, for which she underwent laparotomy, closure of ECF with washout and reapplication of VAC dressing. She also developed an infected abdominal wound and left groin haematoma requiring multiple debridement and mesh repair of abdomen and left pedicled anterolateral thigh flap reconstruction, and ventilator-associated pneumonia. Simultaneously, the woman was on multiple culture-directed antimicrobials and eventually improved.
After four months, she was discharged to a community hospital for rehabilitation. She had significant functional decline due to prolonged hospitalisation and complications. Impairments included cognitive, right-sided weakness, bladder incontinence, physical deconditioning and foot drop. She had regular physiotherapy, occupational and speech therapy reviews. At the latest three-year follow-up, she was ambulating independently but was dependent on her activities of daily living (ADL). She denied urinary or faecal incontinence.
Case 3
A 37-year-old Malay woman with a pregnancy conceived via in-vitro fertilisation and with GDM on metformin. She was induced at 37 + 1 weeks as she had reduced fetal movements. The latest ultrasound was normal with no evidence of oligohydramnios or growth restriction.
After 12 h of dinoprostone, ARM was performed and an oxytocin infusion was started. Approximately 2 h later, she developed acute shortness of breath and tachycardia and CTG showed fetal bradycardia. An emergency CS was performed. There was blood-stained liquor but no evidence of placental abruption on clinical examination and histology. The woman developed severe postpartum haemorrhage and uterine atony requiring multiple uterotonics.
Postoperatively, she had persistent vaginal bleeding and a Bakri balloon was inserted. She then had pulseless electrical activity (PEA) collapse. CPR was started and she had ROSC. In view of persistent high Bakri drain output, anaemia requiring 2 cycles of MTP, and hypotension requiring inotropes, she underwent a hysterectomy. The uterus was atonic but the intraperitoneal survey was normal with no other sources of intraabdominal bleeding. She was maintained on triple inotropes and subsequent investigations showed overt DIC, severe metabolic acidosis and multi-organ failure with anuric kidney failure and transaminitis. A 2D echocardiogram performed showed a mildly reduced biventricular systolic function. She was referred for consideration of ECMO but was not deemed a suitable candidate.
The next day, she had another PEA collapse. ROSC was achieved 11 min after CPR and noradrenaline boluses. Continuous renal replacement therapy was started in view of acidosis and her coagulopathy was corrected. She developed abdominal distension with high abdominal drain output and underwent exploratory relook laparotomy, evacuation of haemoperitoneum, haemostasis and abdominal packing. She remained critically ill on triple inotropes. Ischaemic bowel was suspected in view of persistently high lactate despite dialysis. CT mesenteric angiogram showed ischaemic changes at the splenic flexure, liver and spleen. A CT pulmonary angiogram showed no evidence of pulmonary embolism. CT brain showed severe diffuse cerebral oedema with watershed infarcts and global hypoxic ischaemic encephalopathy. In view of her critically ill status with poor prognosis, the decision was made for terminal extubation and withdrawal of care. The cause of death by the coroner was multi-organ failure due to AFE.
Case 4
A 25-year-old primiparous Chinese woman with no medical history and an uncomplicated antenatal course was induced at 39 weeks and 1 day, with dinoprostone. ARM was done at 4 cm dilatation and she quickly progressed spontaneously to full dilatation 27 min later.
The woman then developed acute vomiting, followed by a tonic-clonic seizure, and became hypotensive and unresponsive. As delivery was imminent, a forceps-assisted delivery was expeditiously performed. Her baby required continuous positive airway pressure initially but was subsequently discharged well on day 3 of life.
Post-delivery, the woman was intubated, fluid resuscitated and monitored in the ICU. An echocardiogram showed a hyperdynamic preserved LVEF and normal RV. Her serum sodium level was normal (138mEq/L). Postpartum haemorrhage secondary to uterine atony and DIC ensued. This was initially managed with multiple uterotonics, Bakri balloon insertion and aggressive transfusion and correction of coagulopathy. However, as she had persistent bleeding on inotropic support, uterine artery embolisation was done.
An MRI brain was performed in view of left-sided weakness. This demonstrated multiple intracranial emboli in the right middle cerebral artery (MCA) territory, corresponding to the right hemispheric syndrome. In view of the clinical suspicion of a right-to-left cardiac shunt, a transthoracic echocardiogram was done. Over 50 microemboli were demonstrated in the MCA on moderate Valsalva; consistent with a significant right-to-left atrial septal defect.
The woman was extubated and recovered and discharged well. She underwent closure of the patent foramen ovale (PFO) a year later. At her latest outpatient follow-up, she had no cognitive or neurological deficits.
Discussion
AFE is a clinical diagnosis that should be considered in the differential diagnosis of acute cardiorespiratory compromise in pregnant or postpartum women. Our first two patients presented with the classic triad of abrupt cardiovascular collapse around the time of delivery, associated with coagulopathy. The last two patients with atypical AFE had a more heterogenous presentation. Case 3 had DIC-type of AFE, 9 distinguished by uterine atony and DIC prior to cardiopulmonary failure, instead of acute cardiovascular collapse as the first presentation. Paradoxical AFE (Case 4) can occur in the presence of an intracardiac shunt between venous and arterial circulations in the form of a PFO or an atrial or ventricular septal defect. Although the exact mechanism is unknown, possibilities include paradoxical embolism of fetal material with local complement activation in the brain or formation of venous thrombus (potentially in the context of DIC) and paradoxical thrombotic emboli that cross the intracardiac shunt and enters the cerebral circulation resulting in neurological manifestations. 10
Early recognition and timely initiation of cardiovascular supportive therapies are crucial in cases of maternal cardiac arrest. CPR with effective chest compressions and lateral displacement of the gravid uterus should be initiated immediately. If the gestational age is above 20 weeks and if spontaneous circulation has not returned within 4 min of maternal cardiorespiratory collapse, resuscitative hysterotomy should be performed to relieve aortocaval compression and facilitate ROSC.11,12
Echocardiography is an invaluable tool in differentiating life-threatening causes of hypotension and cardiac arrest, and is being increasingly incorporated in obstetric resuscitation. A focused transthoracic echocardiogram can provide quick detection of gross abnormalities in systolic biventricular function, volume status, pericardial fluid, and valvular function. 13 This may narrow the differential diagnosis in obstetric shock, reduce the diagnostic ambiguity of AFE cases and triage patients who may require more advanced haemodynamic support.
Echocardiographic RV dysfunction is a common finding in AFE and is associated with a high risk of cardiac arrest. 14 This RV dysfunction is thought to be due acute pulmonary vasospasm and increased pulmonary vascular resistance. Early commencement of RV support therapies, e.g. inotropes, vasopressors, ECMO and expediting delivery therefore enables quicker achievement of haemodynamic stability and may reduce further cardiac morbidity.
ECMO was vital in supporting circulation and end-organ perfusion in the women in cases 1 and 2 who had refractory AFE. Obstetric patients are often young with minimal co-morbidities, which are ideal factors for ECMO candidacy, and ECMO has been successfully used in pregnant and postpartum women for various indications. 15 In cases of AFE, VA-ECMO is beneficial in women with cardiac failure and stunned myocardium caused by cardiac arrest 16 and early initiation suggests a mortality benefit.17–19
Newer reports have proposed extracorporeal CPR (ECPR), where VA-ECMO is rapidly initiated during CPR in patients with no spontaneous cardiac activity. 20 ECPR can optimise oxygenation and improve end-organ perfusion compared to conventional CPR, which provides only 25–30% of cardiac output. 21 This may help reduce morbidity from prolonged collapse, such as in Case 2, who had to be treated for multi-system complications due to challenges with sustaining circulation despite conventional CPR.
Peripheral access through the femoral vein and artery is the most commonly used modality for VA-ECMO initiation. However, limb ischaemia is a risk (due to vessel occlusion from retrograde arterial cannulation) and this complication unfortunately occurred in two of our patients. A prophylactic use of a distal perfusion cannula is associated with a reduction in this complication and should be considered in high-risk patients. 22
ECMO patients require anticoagulation to prevent complications such as systemic thromboembolism and circuit thrombosis. 23 This is challenging in AFE, which is often complicated by DIC and ongoing haemorrhage. 24 Thus, an anticoagulation-free ECMO strategy may be considered. 25 This method was employed in Case 2 as there was DIC and ongoing bleeding. Avoidance of anticoagulation mandates high-flow VA-ECMO, and anticoagulation should be started as soon as the bleeding risk subsides. Close collaboration between the obstetrician, haematologist and ECMO team is necessary to aggressively correct coagulopathy, secure haemostasis and titrate ECMO flow rates while reducing the risks of ECMO-related thrombosis. 33
DIC is a complication of AFE that results in life-threatening haemorrhage. MTP activation will allow aggressive transfusion of packed RBC to maintain tissue oxygenation and reverse coagulopathy. ‘Haemostatic resuscitation’ with transfusion of packed RBC, FFP and platelets in a 1:1:1 ratio is associated with improved outcomes in obstetric haemorrhage. 26
All of our patients had significant bleeding due to DIC, and required transfusion and intervention to secure haemostasis via hysterectomy or uterine embolisation. Hysterectomy should be considered early in patients with persistent uterine haemorrhage and DIC. If there is persistent intraabdominal bleeding after hysterectomy, temporary abdominal packing is a useful option to control life-threatening bleeding 27 while awaiting correction of coagulopathy.
Specific laboratory coagulation abnormalities may be treated with FFP, platelets, and/or cryoprecipitate transfusion. Cryoprecipitate contains fibrinogen, factor VIII, factor XIII, and von Willebrand factor. It can replenish clotting factors in lieu of FFP 28 and correct obstetric DIC which is typically associated with low fibrinogen. Hyperfibrinolysis is a contributing factor of AFE-associated coagulopathy.29,30 Early use of tranexamic acid in hyperfibrinolysis-predominant DIC has shown some benefits and may be associated with improved maternal outcomes in these cases of AFE. 31 Several studies have also reported supportive management with the use of C1 esterase inhibitor 32 and atropine, ondansetron, ketorolac therapies33,34 with successful outcomes.
In our study, three women survived, two with good functional and neurological recovery and one who required ADL-assistance. Although the AFE case fatality rates have fallen over the years, the survivors have significant morbidity. Persisting neurological impairment have been reported in 6–61% of women who survived AFE.35,36
Women with severe obstetric adverse events are also at a greater risk of long-term physical and mental health problems. 37 Physical problems (e.g. muscle weakness, chronic fatigue, and pain) can significantly impact daily activities, work, or caring for their child even years after discharge. 19 Patient-centred rehabilitation programmes are important to help improve long-term postpartum health-related quality of life for AFE survivors. 38
Due to the morbidity and psychological trauma associated with AFE, these women may refrain from further child-bearing. Studies have reported successful pregnancies and outcomes after AFE, with no recurrence,39–44 suggesting that AFE is a sporadic event. Although AFE may be an immune-mediated phenomenon, a low risk of recurrence might be expected as each fetus may be antigenically different. 40
Many obstetricians may have limited prior experience in managing AFE cases due to its rarity. Ongoing education and simulation training, ideally in a multidisciplinary setting, allows one to be better prepared in the recognition and management of AFE. In our institution, each case was reviewed and debriefed by the department to identify areas for improvement and modify processes as needed. A dedicated AFE pathway has also been proposed to facilitate streamlined care 45 and this implementation can be considered.
Conclusion
The management of AFE is primarily resuscitative and directed towards maintaining oxygenation, cardiac output and BP, and correction of the coagulopathy. With prompt recognition and treatment of AFE involving a multidisciplinary team, survival and good outcomes are possible.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
The SingHealth Institutional Review Board (IRB No. 2023/2567) waived the need for ethics approval and patient consent for the collection, analysis and publication of the retrospectively obtained and anonymised data for this non-interventional study.
Guarantor
Dr Liying` Yang.
Contributorship
SLJB and LY collected the data and wrote the first draft of the manuscript. WCT, DK, TTY, RN, and LKT edited the manuscript.