
Abstract
Renal artery stenosis is rare in pregnancy. Patients generally present with hypertension and/or pre-eclampsia. Accompanying hypokalaemia is usually mild or absent. Our case demonstrates the unusual finding of severe and refractory hypokalaemia together with hypertension in a woman with renal artery stenosis in pregnancy. The differential diagnosis of hypokalaemia with hypertension in pregnancy is discussed.
Introduction
Renal artery stenosis (RAS) is rare in pregnancy. 1 Patients generally present with hypertension and/or pre-eclampsia.1–7 Our case demonstrates the unusual finding of severe and refractory hypokalaemia together with hypertension in a woman with RAS in pregnancy.
Case report
A 40-year-old woman presented to the emergency department of a regional hospital at 7 weeks' gestation with a short history of nausea, vomiting, and headache. Her past medical history included a normal pregnancy 22 years prior, three miscarriages, an ectopic pregnancy and depression. She had been taking ondansetron and escitalopram for the previous 3 days.
Significant hypokalaemia (potassium 2.4 mmol/L, normal range 3.5−5.0) was noted on initial blood tests and cardiac monitoring in the Emergency Department showed bigeminy and a prolonged QT interval. This deteriorated to Torsades de Pointes, quickly followed by cardiac arrest. She was resuscitated according to local protocol with rapid return of spontaneous circulation.
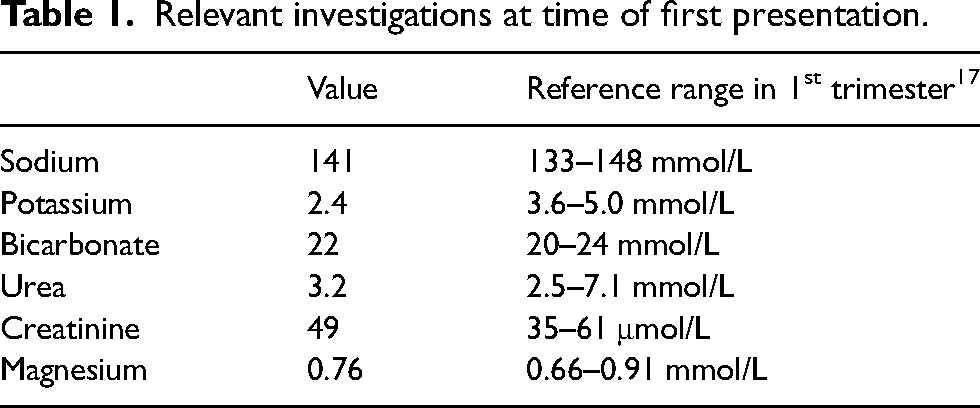
Following successful resuscitation, she was transferred to a tertiary hospital. ECG changes resolved with normalisation of potassium levels and cessation of potentially contributing medications (ondansetron and escitalopram). Further investigation on day 3 of admission revealed raised aldosterone and renin levels and a normal aldosterone:renin ratio (ARR). The patient had never been diagnosed with hypertension or hypokalaemia prior to pregnancy but there were no pre-pregnancy blood pressure or potassium measurements available to confirm (Tables 1 and 2).
Relevant investigations at time of first presentation.
Investigations performed after normalisation of potassium level.

Ultrasound renal Doppler demonstrated right renal artery stenosis, with subtle right renal atrophy (10.4 cm). The left kidney was 14.2 cm. Magnetic resonance angiography (MRA) without contrast showed a long segment of tightly stenosed right renal artery suggestive of intimal type fibromuscular dysplasia (FMD). There was no evidence of a reninoma on MRA and imaging of her carotid vessels did not show any FMD related cerebrovascular disease or atherosclerosis. Genetic testing for channelopathies was performed due to the severity of the hypokalaemia and initial presence of an abnormal QT but no pathogenic mutations were identified.
Over an 8-week inpatient stay, she was persistently hypertensive with refractory hypokalaemia requiring central line placement and high dose intravenous potassium replacement. After discussion at multiple multi-disciplinary meetings, termination was offered due to concerns about maternal wellbeing. This was declined by the patient. Spironolactone was commenced once non-invasive prenatal testing confirmed a female fetus. Blood pressure and potassium levels eventually stabilised on an oral medication regimen including potassium supplementation equivalent to 370 mEq KCl per day, spironolactone and amiloride. Additionally, she required labetalol and slow release nifedipine for blood pressure control to pregnancy target of <135/85 mmHg. Aspirin was started for preeclampsia prophylaxis and she was discharged at 15 weeks' gestation with regular antenatal follow-up.
Other pregnancy complications included diet-controlled gestational diabetes mellitus. She continued to have stable potassium readings and blood pressure. Surveillance ultrasounds showed normal fetal growth. Due to maternal and fetal stability, conservative management was continued. She delivered a healthy 3.16 kg female infant via elective caesarean section at 38 weeks' gestation.
After delivery, she was persistently hypertensive and underwent right renal artery angioplasty 5 months postpartum. After the procedure, she still required three antihypertensive agents including spironolactone to achieve good blood pressure control but was able to cease her potassium supplementation. Further postpartum testing to explore alternative causes of her persistent hypertension has not yet been performed.
Discussion
RAS is an unusual cause of hypertension in pregnancy. RAS is estimated to affect less than 5% of women with hypertensive disorders of pregnancy, although the exact prevalence is unknown. 1 Based on available literature, accompanying hypokalaemia is usually mild or absent.1–7
Clinicians should consider investigating for RAS in cases of severe, early-onset or medication refractory hypertension during pregnancy.2,3 Non-invasive renal Doppler ultrasonography is a safe and readily available test but results are operator dependent and can be affected by obesity and overlying bowel gas.1,3 Magnetic resonance angiography is safe in pregnancy but can miss the distal arterial changes of FMD. 1 Renal artery contrast angiography is considered to be the gold standard investigation but there is often concern regarding fetal radiation exposure. Reassuringly, angiography can be performed with fetal radiation exposure around 10 mGy, significantly below the accepted safe upper limit of 50 mGy.1,3,4
Outcomes in cases of RAS are variable, with case reports documenting high rates of maternal hypertension, preeclampsia, fetal loss and preterm birth.1,5,6 Pregnancy-related complications were lower in a large retrospective registry cohort of FMD patients, although only 9 of 237 women were diagnosed prior to pregnancy and the median time from first pregnancy to diagnosis of FMD was 21 years. 8 Management centres around maternal blood pressure control with consideration of antepartum renal artery angioplasty. Intervention is indicated in the setting of early-onset hypertension that is unable to be controlled with medical management, deterioration in maternal renal function or where the benefit of intervention is felt to outweigh potential harms for the mother and fetus. 7 Given our patient was able to be managed conservatively during pregnancy, we did not pursue angiography or renal artery angioplasty until after delivery.
Our patient was commenced on potassium-sparing diuretics in addition to potassium supplementation for management of her refractory hypokalaemia. Data from animal studies suggests that spironolactone may cause feminisation of male fetuses at high doses, although this effect has not been clearly demonstrated in humans from the available case reports.
9
It was only commenced in our patient once a female fetus was confirmed via non-invasive prenatal testing. Eplerenone has also been used in a small number of pregnancies without adverse outcomes.
10
The severity of our patient's hypokalaemia was surprising and consideration was given to alternative or contributory diagnoses. She did not report ongoing nausea and vomiting of pregnancy to support gastrointestinal losses, was not polyuric and had a normal magnesium level. Ondansetron-associated hypokalaemia has been reported although this medication was ceased on admission and would not have contributed to the persistent hypokalaemia or hypertension seen.
11
She had no features to suggest an underlying eating disorder. She denied using any diuretics, laxatives or other supplements that could have contributed to hypokalaemia, although she did not have a diuretic screen performed at the time of presentation. Her normal bicarbonate excluded a concomitant renal tubular acidosis.
Normal pregnancy is a state of hyperreninaemic hyperaldosteronism. Elevated renin and aldosterone levels are seen from early pregnancy and pregnancy specific reference ranges should be used when interpreting ARR ratios in this setting. 12 Medications may also impact ARR results. At the time of testing, our patient was on labetalol which may increase cause a reduction in renin levels. 12 Taking this into account, our patient's ARR results were not suggestive of Liddle syndrome, syndrome of apparent mineralocorticoid excess or Cushing syndrome which are all associated with hyporeninaemic hyperaldosteronism. Her 24-hour urinary cortisol was elevated but in keeping with normal changes in pregnancy. 12
Geller syndrome, increased mineralocorticoid activity secondary to progesterone and a gain of function mutation in the mineralocorticoid receptor, can cause hypokalaemia isolated to pregnancy but is usually associated with suppressed aldosterone levels.13,14 A diagnosis of primary hyperaldosteronism was less likely in our case, as most pregnant patients with this condition will have a ARR >40 and/or direct renin level of <20 mU/L. 15
Genetic testing for potassium-wasting channelopathies was negative. This indicated that an underlying genetic disorder causing hypokalaemia, such as Liddle, Bartter or Gitelman syndrome was less likely although genetic testing for Gitelman and Bartter syndromes can have variable clinical sensitivity. 16 She did not have an assessment of urinary calcium performed.
Some of our patient's hypokalaemia may be attributable to pregnancy-related changes. In normal pregnancy, progesterone is known to have an antagonistic effect on the mineralocorticoid receptor in the distal convoluted tubule, attenuating the effects of aldosterone and reducing the occurrence of hypokalaemia. 10 However, the clinical course in pregnant women with underlying hyperaldosteronism (such as RAS or primary hyperaldosteronism) is variable with some experiencing significant hypokalaemia. 10
As our patient has remained hypertensive despite treated RAS, and spironolactone use may mask ongoing postpartum hypokalaemia, repeat testing for alternative causes is being arranged. This is particularly relevant for primary aldosteronism, given the prevalence of this condition is increased among patients with concomitant RAS and the ARR mya be falsely normal in 38% to 50% of patients with both disorders. 16
The investigation of hypertension with hypokalaemia in pregnancy can be challenging. There is a broad range of differential diagnoses and results need to be interpreted with appropriate adjustment for gestation. The possibility of secondary causes of hypertension should be carefully considered, particularly for patients with severe presentations.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Not applicable. Our institutions do not require ethical approval for reporting individual cases.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Written informed consent was obtained from the patient for their anonymized information to be published in this article.
Guarantor
Jessica Phillips.
Contributorship
II wrote the first draft of the case report. JP wrote the first draft of the discussion. All authors reviewed and edited the manuscript and approved the final version of the manuscript.