
Abstract
Dilated cardiomyopathy in pregnancy, whether diagnosed pre-conception, or occurring de novo during pregnancy, may be associated with significant maternal morbidity and mortality. Hypomagnesaemia is associated with ventricular arrhythmias and may be a risk factor for heart failure, coronary artery disease and atrial fibrillation in the general population. Pregnancy is associated with a progressive physiological fall in serum magnesium concentration. Intracellular magnesium deficiency may exist despite normal serum magnesium concentration. Three cases of dilated cardiomyopathy developing in the peripartum period with hypomagnesaemia are presented. The literature regarding associations between magnesium deficiency and dilated cardiomyopathy is reviewed. Potential future research examining magnesium deficiency as a potential contributor to dilated cardiomyopathy in pregnancy is proposed, and possible implications for management are discussed.
Keywords
Introduction
Distinguishing between peripartum cardiomyopathy (PPCM) and the development of heart failure precipitated by physiological cardiovascular changes in pregnancy superimposed on pre-existing dilated cardiomyopathy may be difficult. The aetiology of PPCM is not known. 1 Multiple mechanisms have been proposed, including viral and autoimmune myocarditis, toxicity of a 16-kilodalton fraction of prolactin, environmental factors, apoptosis and inflammation, electrolyte or micronutrient deficiencies, and a familial basis. 1 Hypomagnesaemia (hypoMg) and dilated cardiomyopathy are common features in several genetic and acquired conditions in the general population.2–4 In particular heterozygous variants in the RRAGD gene have recently been described in families with dilated cardiomyopathy and hypoMg.2,3 As a predominantly intracellular cation, tissue magnesium deficiency may exist despite normal serum magnesium concentrations. 5 Serum and tissue magnesium concentrations progressively fall during pregnancy due to increasing renal magnesium loss, as well as a transplacental gradient from mother to fetus.6,7 Cases of dilated cardiomyopathy and hypoMg presenting in the peripartum period in the setting of bacteraemia, preeclampsia, and previous chemotherapy are described. The possibility that Mg deficiency may be a factor in the development of dilated cardiomyopathy in pregnancy is explored.
Case 1 – dilated cardiomyopathy, hypomagnesaemia and preeclampsia
A 28-year-old woman presented at 38 weeks’ gestation in her first pregnancy with a 10-day history of palpitations and shortness of breath. Her pregnancy had been previously uncomplicated other than diet-controlled gestational diabetes mellitus (GDM). She denied any other past medical history, significant family history, or ingestion of medications, pregnancy supplements, alcohol, complementary therapy, illicit drugs or smoking. There was no history to suggest malabsorption or gastrointestinal losses of electrolytes. Examination revealed pulse 130/min regular, blood pressure 130/100 mmHg, a prominent third heart sound with gallop rhythm, and chest was clear. The body mass index was 28.2 kg/m2. NT-proBNP was 1940 ng/L (normal < 300), and serum Mg was 0.4 mmol/L (non-pregnant reference interval 0.7–1.1) (Table 1). High-sensitivity cardiac troponin I, ionised calcium, serum albumin and potassium were normal. Urine protein:creatinine ratio (uPCR) was 119 mg/mmol (normal <30) consistent with preeclampsia. One week earlier urine PCR and blood pressure had been normal, and serum Mg 0.5 mmol/L. Echocardiography revealed a severely reduced left ventricular systolic function globally [ejection fraction (LVEF) 20–25%], and normal right ventricular size and function. A screen for secondary causes of dilated cardiomyopathy was performed; thyroid function, thiamine, selenium, active B12, iron studies, plasma metanephrines and acylcarnitine profile were normal, and coeliac serology was negative. Spot urine Mg:creatinine (Mg:Cr) prior to infusion of Mg was 2.9 mmol/L, with a fractional excretion of Mg of 8.9% (non-pregnant normal 2–4%) consistent with inappropriate urine Mg losses. Urine calcium:Cr ratio (Ca:Cr) was 0.92 (non-pregnant normal 0.05–0.45). Intravenous magnesium, oral bisoprolol and furosemide were commenced, and vaginal delivery with epidural anaesthesia occurred uneventfully following induction of labour. Postpartum bromocriptine, ramipril, spironolactone, magnesium aspartate 1.5 g/day, enoxaparin and dapagliflozin were added to bisoprolol and furosemide. Six weeks postpartum the woman was asymptomatic with unchanged findings on echocardiography. Computerised tomography coronary angiography revealed widely patent epicardial coronary arteries with no atheroma or stenosis. Cardiac magnetic resonance imaging (cMRI) is pending. Urine Ca:Cr ratio had fallen to 0.23 mmol/mol. Whole genome screening for RRAGD mutations, a cardiomyopathy gene panel, and Bartter syndrome is pending.
Pathology result cases 1–3.
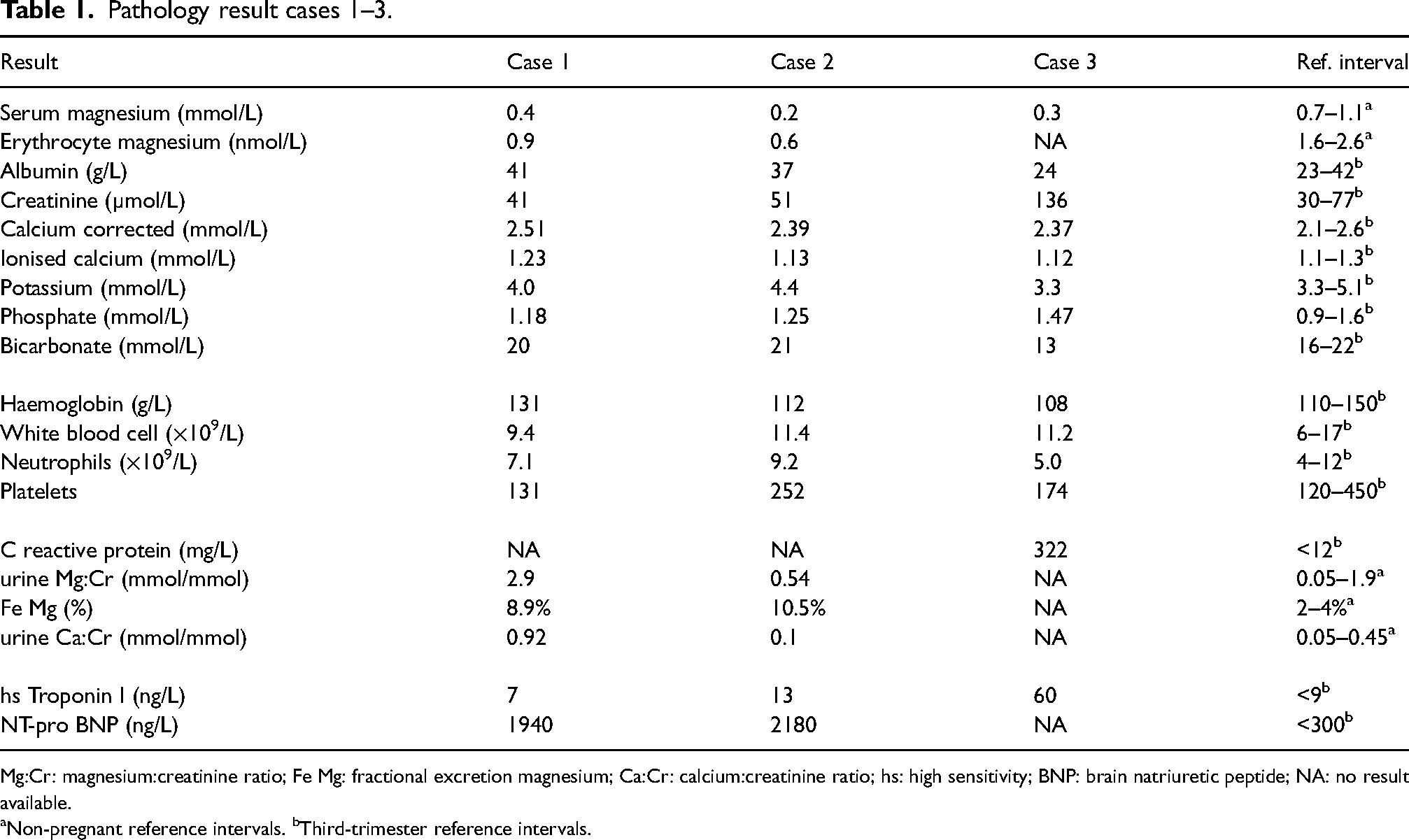
Mg:Cr: magnesium:creatinine ratio; Fe Mg: fractional excretion magnesium; Ca:Cr: calcium:creatinine ratio; hs: high sensitivity; BNP: brain natriuretic peptide; NA: no result available.
Non-pregnant reference intervals. bThird-trimester reference intervals.
Case 2 – dilated cardiomyopathy, hypomagnesaemia and prior doxorubicin/cisplatin
A 38-year-old woman in her third pregnancy was noted to have a serum Mg of 0.2 mmol/L clinic at 33 weeks’ gestation on a routine biochemistry panel in the setting of well-controlled insulin-treated GDM, and previous cisplatin/doxorubicin chemotherapy for osteosarcoma at age 19 years. The woman denied any other significant past medical or family history, ingestion of medications, alcohol, complementary therapies, pregnancy supplements or illicit substances, and was a non-smoker. There was no history to suggest malabsorption or gastrointestinal losses of electrolytes. She was not taking magnesium supplements. Ionised calcium, serum albumin and potassium were normal (Table 1).
Serum Mg prior to commencing chemotherapy 19 years earlier had been 0.63 mmol/L. Her first pregnancy at age 28 years had been complicated by preeclampsia at 35 weeks’ gestation, her second pregnancy at age 30 years was uncomplicated.
24-h urine Mg was 4.1 mmol/day with fractional excretion Mg of 10.5% consistent with renal Mg wasting, and 24-h urine calcium was 1.0 mmol/L (non-pregnant range 1.2–7.5). Urine amino acids were normal. Testing for HNF1-B mutation and 17q12 deletion was negative. The most likely diagnosis was an acquired tubulopathy secondary to previous cisplatin therapy, although the baseline hypoMg indicated a possible underlying tubulopathy or channelopathy. The woman was commenced on Mg aspartate orally 1.5 g per day orally. The woman proceeded to elective repeat caesarean delivery at 38 weeks’ gestation. Nine weeks postpartum the woman presented with shortness of breath and pleuritic chest pain. Echocardiography revealed severe global left ventricular systolic dysfunction with estimated LVEF of 10–15%, mild-moderate right ventricular systolic dysfunction, and multiple biventricular intracavitary thrombi. Computerised pulmonary angiography revealed extensive bilateral pulmonary emboli. The woman was treated with enoxaparin, intravenous magnesium, potassium and furosemide, and subsequently with bisoprolol, ramipril, spironolactone, warfarin and oral Mg. Five weeks later cMRI demonstrated normal left ventricular volume with severe global systolic impairment (LVEF 28%), normal right ventricular volume and moderate systolic impairment (RVEF 37%), moderate tricuspid regurgitation and septal flattening consistent with high right-sided pressures and volume loading, no myocardial or pericardial enhancement, and large biventricular thrombi. Four years postpartum LVEF was 45–50% while continuing to take bisoprolol, spironolactone, ramipril, warfarin and Mg supplements. Serum Mg has varied between 0.44 and 0.63 mmol/L. The woman has been referred for whole genome sequencing including RRAGD mutation, cardiomyopathy panel and Gitelman syndrome. Onset of anthracycline-associated cardiotoxicity more than five years following chemotherapy is extremely rare, suggesting the women had PPCM rather than doxorubicin-induced cardiomyopathy.
Case 3 – dilated cardiomyopathy, hypomagnesaemia and sepsis
A 26-year-old woman developed fever and malaise following an uncomplicated spontaneous vaginal delivery of her fourth child at 38 weeks’ gestation. The woman denied any other significant past medical or family history, ingestion of medications, alcohol, complementary therapies, pregnancy supplements or illicit substances, and was a non-smoker. There was no history to suggest malabsorption or gastrointestinal losses of electrolytes. Her symptoms were attributed to a viral illness, however on the third postpartum day she developed septic shock with acute kidney injury and pulmonary oedema. Serum creatinine was 136 µmol/L, serum Mg 0.3 mmol/L, serum albumin 24 g/L, high sensitivity cardiac TnI was 60 (normal < 9), and echocardiography revealed severe global systolic dysfunction (LVEF 25%) and moderately reduced right ventricular systolic function. Blood cultures grew Streptococcus pyogenes. The woman developed multi-organ failure requiring ventilatory support and dialysis for 30 days. Magnesium was replaced intravenously during her stay in the intensive care unit, but serum Mg subsequently became normal without requiring magnesium supplementation in the long term. LVEF remained at 25% when two months postpartum while receiving bisoprolol and enalapril, improving to 40% at 6 months postpartum, and 60% one year postpartum. The delayed recovery of LVEF in this case is atypical for sepsis-related cardiomyopathy and suggestive of the possibility of a co-existent PPCM.
Discussion
Assessing magnesium status
Mg is predominantly an intracellular cation and accurate assessment of tissue Mg status is difficult. The principal sites of distribution of Mg in humans are in bone (53%), muscle (27%), soft tissue (19%) and red blood cells (0.5%), with only 0.3% of total body Mg in serum.8–10 Of serum Mg, 30% is protein bound (predominantly to albumin), 50% is ionised and the remainder is complexed with anions including phosphate and citrate. 11 There is no simple, rapid and accurate laboratory test to determine total body magnesium status in humans. 5 Measurement of ionised Mg is possible, although difficult to automate, and susceptible to false results without very well-defined sample handling, and probably has little value in addition to serum Mg concentrations.12,13 Human and animal studies have consistently shown a poor correlation between serum and erythrocyte Mg (eMg) with skeletal muscle Mg concentrations.14–18 It is therefore possible to have significant depletion of Mg in tissues while demonstrating normal serum and eMg concentrations. 19 The correlation between lymphocyte Mg and skeletal muscle Mg stores has been inconsistent in studies, measurement is technically difficult, and has high intra-individual variation. 20 Intracellular Mg concentrations range from 5 to 20 mmol/L of which 1–5% is ionised. Mg loading/tolerance tests are a sensitive measure to detect Mg deficiency in individuals with normal renal function. 21 Intramuscular ionized Mg measured by phosphorous magnetic resonance spectroscopy was a better clinical measure of Mg status than total serum Mg and has the potential to non-invasively measure Mg content in cardiac muscle, as well as monitoring the effectiveness of Mg supplementation. 22 Haigney et al. demonstrated a strong correlation between intracellular Mg in sublingual epithelial cells obtained by scraping, and myocardial cells obtained by biopsy during cardiopulmonary bypass, while serum Mg correlated poorly with both tissue concentrations. 19
Spurious hypomagnesaemia may occur with severe hypoalbuminaemia. 11
Magnesium deficiency should be considered irrespective of serum Mg concentration wherever there are typical symptoms or associated electrolyte disorders, particularly in the setting of known acquired or inherited causes of magnesium deficiency. Symptoms of Mg deficiency include neuromuscular irritability (tetany, seizures, movement disorders, paraesthesias), muscle weakness and cramps, and cardiac arrhythmias. Electrolyte disorders associated with Mg deficiency include hypokalaemia, hypocalcaemia and hypophosphataemia, particularly where refractory to replacement therapy. Major risk factors for acquired Mg deficiency include alcohol excess, poorly controlled diabetes mellitus, diarrhoea and malabsorptive syndromes, and medications including proton pump inhibitors, diuretics, antibiotics affecting renal tubular function, calcineurin inhibitors, and platinum agents.
Studies examining differences in prevalence of hypoMg among populations are limited by significant variations in assays used and serum concentrations used to define hypoMg. 23 Two independent international groups designated 0.85 mmol/L as the low cut-off point defining hypoMg in non-pregnant individuals. 23
Magnesium physiology in pregnancy
Increased expression of the colonic and renal tubular magnesium transporter genes from 12 weeks’ gestation has been demonstrated compared with non-pregnant controls indicating an increased demand for Mg in pregnancy. 24 Serum Mg declines from a preconception mean of 0.93 mmol/L to a nadir mean of 0.63 mmol/L in the third trimester. 25 Similarly ionised and eMg, and intracellular free Mg in brain and muscle are lower in pregnancy than in non-pregnant controls when measured by NMR spectroscopy.26,27 After the fifth month of gestation, increasing amounts of Mg are transported from mother to fetus. 7 Fetal Mg concentrations are higher than maternal Mg concentrations consistent with a transplacental gradient. Little is known about the mechanism and regulation of placental Mg flux. 28 It has been postulated that maternal–fetal Mg gradient is due to an active transport mechanism, as the gradient is not due to differences in protein binding between mother and fetus. Urinary excretion of Mg rises by approximately 25% during pregnancy. 6 In the presence of hypoMg excretion of greater than 1 mmol/day is consistent with renal Mg wasting in non-pregnant individuals. 29 Mg excretion of less than 0.5 mmol/day is suggestive of Mg deficiency in non-pregnant individuals. 30
Conditions manifesting dilated cardiomyopathy and hypomagnesaemia
Conditions which have been reported to manifest hypoMg and dilated cardiomyopathy are summarised in Table 2. Improvement and/or normalization in left ventricular function with Mg therapy has been demonstrated in many of these conditions. The relative effects of hypoMg, hypocalcaemia, hypokalaemia and hypophosphataemia in contributing to LV systolic dysfunction in several of the conditions, however, is unclear.
Conditions associated with hypomagnesaemia and dilated cardiomyopathy.
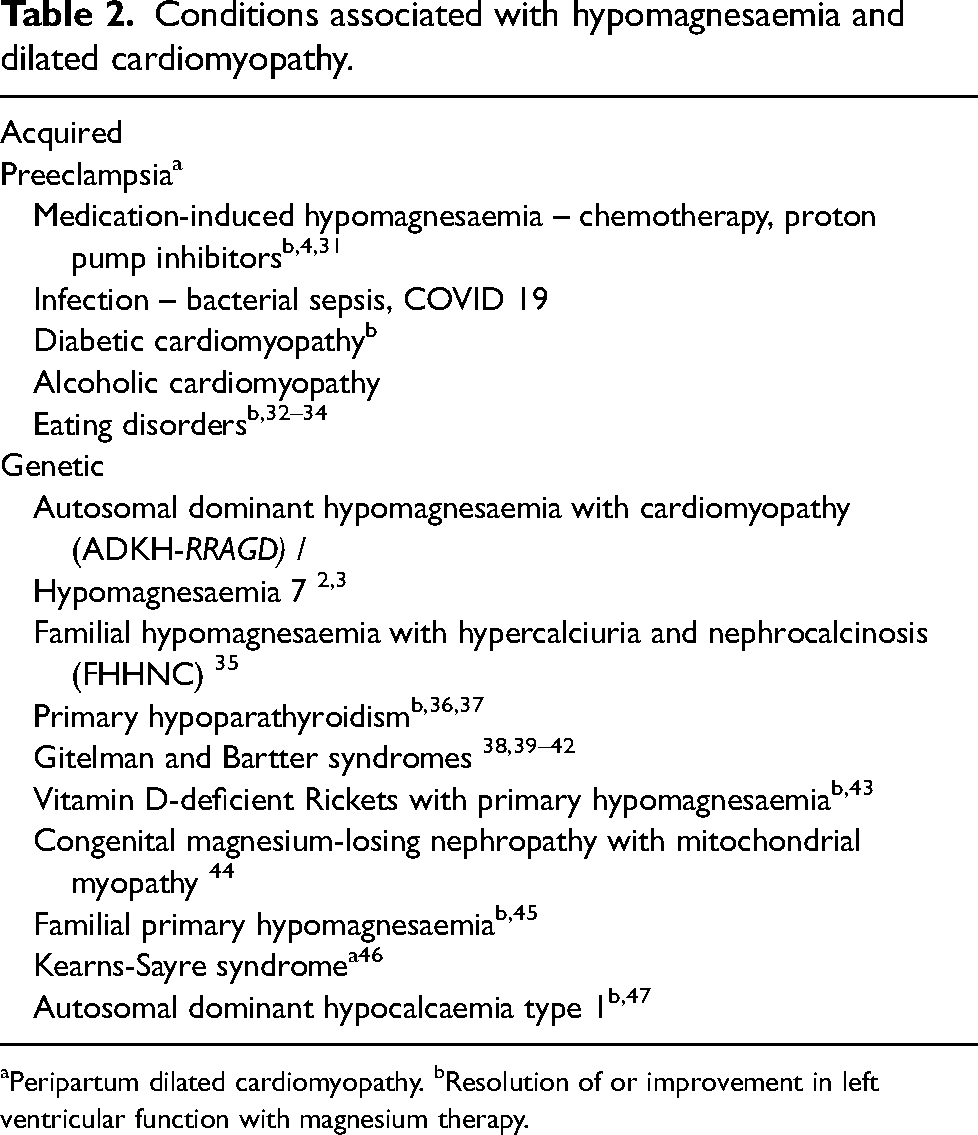
Peripartum dilated cardiomyopathy. bResolution of or improvement in left ventricular function with magnesium therapy.
Preeclampsia, hypomagnesaemia and cardiomyopathy
A systemic review and meta-analysis of 13 observational studies with 11 951 PPCM cases from seven countries found severe preeclampsia, preeclampsia, preeclampsia superimposed upon chronic hypertension, chronic hypertension and gestational hypertension were associated with odds ratios of 13.33, 4.73, 5.77, 4.73 and 3.13 for the development of PPCM. 48
A meta-analysis of 14 studies revealed women with pregnancy-induced hypertension had lower concentration of serum Mg, zinc and calcium than healthy pregnant women. 49 There is an overexpression for the gene SLC41A1, a Na/Mg exchanger, in placenta from women with preeclampsia (PET) compared with normal placentas, suggesting a change in Mg homeostasis may contribute to the development of PET. 50 A pilot study examining serum Mg in pregnant women at a University Teaching Hospital in Benin, West Africa, found that women with hypoMg had an Odds ratio of 22 for preeclampsia compared with normomagnesaemic women. 51 The presence of hypoMg in women with preeclampsia is associated with increased risks of complications of preeclampsia including posterior reversible encephalopathy syndrome and haemolysis, elevated liver enzymes and low platelet syndrome.52,53 Mean maternal cerebral and skeletal muscle Mg concentration measured by phosphorous magnetic resonance spectroscopy were lower in women with preeclampsia compared with healthy pregnant and non-pregnant controls.26,54 In women with preeclampsia, those with visual symptoms had lower cerebral Mg concentration than those without visual symptoms. 54
Major methodological difficulties in the interpretation of intervention studies into the role of Mg supplementation in prevention of hypertensive disorders of pregnancy include variations in dietary intake of Mg, and doses and the bioavailability of individual Mg preparations used. A 2014 review of the Cochrane Pregnancy and Childbirth Group's trial register found that Mg supplementation during pregnancy was not associated with a reduction in perinatal mortality, small for gestational age (SGA) or preeclampsia compared with a control group. 55 Of the ten randomised trials only two were judged to be of high quality overall, and there was a lack of consistency in the timing, dose and formula of Mg supplements used in individual studies. Additionally, the studies included were not in populations associated with a high prevalence of Mg deficiency. The Brazilian Magnesium trial found that supplementation with oral Mg citrate 150 mg twice a day from 12 to 20 weeks’ gestation was not associated with a reduction in preeclampsia. 56 A recent randomised controlled trial of low-risk pregnant women in Iran with serum Mg less than 0.78 mmol/L at 12–14 weeks’ gestation found that supplementation with an effervescent 200 mg Mg preparation for one month, together with a multi-mineral preparation containing 100 mg Mg until the end of pregnancy, was associated with lower risks of preeclampsia, intrauterine growth restriction, pre-term birth, and low birthweight. 57
Large, well-designed trials that are sufficiently powered addressing specific considerations including timing of commencement of supplementation, dosage and relevant maternal and neonatal/infant outcomes, in populations with a high incidence of Mg deficiency may be worthwhile.
A consistent relationship between Mg deficiency, the risk of development of PET, and neurological complications of preeclampsia has been demonstrated. Parenteral Mg prevents seizures and placental abruption in women with PET, and the risk of recurrent seizures in women with eclampsia.58,59
To date, no association between Mg deficiency and dilated cardiomyopathy complicating PET has been confirmed.
Chemotherapy-induced dilated cardiomyopathy and hypomagnesaemia
Ninety-eight per cent of cases of anthracycline-induced cardiomyopathy occur in the first year following treatment, with only three case reports of onset of symptomatic heart failure described more than five years following treatment.60,61 A meta-analysis of pregnancies to women with doxorubicin exposure in childhood found 1.7% developed heart failure until 12 months postpartum. 62 The risk of PPCM was 55 times greater than the general pregnant population. Daunorubicin-induced cardiomyopathy in rabbits was associated with significant reductions in myocardial Mg and potassium and increased calcium. 63 These changes in myocardial elements were prevented in animals pre-treated with dexrazoxane, proven to prevent anthracycline-induced cardiomyopathy in humans. 64 Pre-treatment with Mg oxide nanoparticles also prevents doxorubicin-induced alterations in cardiac and apoptosis-related markers in animal studies. 65 In 26 cancer patients observed for seven days with daily clinical and electrocardiographic (ECG) evaluation following initial treatment with doxorubicin or epirubicin, 11 had a fall in eMg. 66 Seven of the 11 patients who developed low eMg manifested ECG changes, compared with only one of the 15 patients with normal eMg.
HypoMg due to urine Mg wasting occurs in 8–71% of individuals previously treated with cisplatin, typically with hypocalciuria. 67 Preloading with 8 mmol intravenous Mg significantly reduced cisplatin-induced nephrotoxicity in humans with an odds ratio of 0.234. 68 Dilated and Takotsubo cardiomyopathy have been described following treatment with cisplatin. 69
Sepsis, hypomagnesaemia and cardiomyopathy
Left ventricular systolic function is severely reduced on echocardiography (LVEF <40%) in 20–60% of non-pregnant individuals with septic shock, with resolution of cardiac dysfunction on echocardiography typically occurring within 7–10 days of presentation.70–72 In the third case cardiac dysfunction persisted for more than six months postpartum, atypical for sepsis as the sole aetiology, and suggestive of PPCM. HypoMg in patients admitted with sepsis to an intensive care unit (ICU) was associated with higher sequential organ failure assessment score, greater length of mean intensive care unit stay, and higher mortality rates (33% vs 4%) than normomagnesaemic septic patients. 73 Soliman et al. found a significantly higher prevalence of septic shock in individuals with low ionised Mg compared with normomagnesaemic individuals (57% vs 11%, p < 0.01) admitted to an ICU. 74 Patients who developed low ionised Mg during their ICU stay had higher Acute Physiology and Chronic Health Evaluation II and Sequential Organ Failure Assessment scores at admission, and may have been more likely to develop sepsis due to being more unwell than those with normal ionised Mg. A retrospective cohort study found the use of intravenous magnesium sulphate in patients admitted to an ICU with sepsis was associated with lower ICU and in-hospital mortality, and requirement for renal replacement therapy. 75 Magnesium therapy affords significant protection against lipopolysaccharide-induced cardiotoxicity and pyroptotic cell death. 76
HypoMg has been detected in 18–61% of individuals admitted to intensive care units, though it is unclear what proportion of these are spurious hypoMg due to hypoalbuminaemia, related to antimicrobial therapy, or represent an epiphenomenon. HypoMg is also associated with an increased risk of disseminated intravascular coagulation in septic patients. 77
RRAGD gene variants
In 2021 Schlingmann et al. described heterozygous variants in the RRAGD gene which induce a constitutive activation of mechanistic target of rapamycin resulting in tubulopathy associated with hypoMg due to renal Mg wasting, hypokalaemia, and renal salt wasting. 3 Hypercalciuria, hypochloraemia, nephrocalcinosis and polyuria were variable features. 3 Six of eight children from unrelated families with tubulopathy had early-onset severe dilated cardiomyopathy, three of whom underwent cardiac transplantation.
Trepiccione et al. subsequently identified 23 individuals from 11 families affected by gain-of-function variants of the RRAGD gene. 2 The renal phenotype for most of the variants (S76L, I221 K, P119R, P119L) typically manifests in the second decade of life occasionally preceded by dilated cardiomyopathy in childhood. Polyhydramnios and pre-term delivery were described for patients carrying the I221K- and S76L/W-RRAGD variants. The P88L variant, however, is associated with dilated cardiomyopathy and sudden cardiac death manifesting in adulthood. None of the four females with P88L variants presented with major complications during pregnancy. Standard potassium and magnesium supplements were effective in managing carpopedal spasm and tetany, though it is unclear as to whether this treatment had any impact on LV systolic function.
In 2006 Ahmed et al. had described a case of a woman at 27 weeks’ gestation with newly diagnosed dilated cardiomyopathy, hypermagnesuric hypoMg, hypercalciuria and polyuria, who in retrospect may have a RRAGD gene variant. 78
Potential mechanisms in Mg deficiency contributing to dilated cardiomyopathy
Mg is involved in oxidative and inflammatory responses through neutralizing free radicals of oxygen and reducing inflammation by regulating the expression of nuclear factor kappa B.79,80 Mg deficiency leads to a pro-inflammatory state with excessive production of oxygen-derived free radicals, which may overwhelm tissue antioxidant capacity with subsequent oxidative tissue destruction. Cellular ATP is significantly reduced in low-Mg mouse hearts. Mishra demonstrated that Mg-deficient rats have fewer cardiac mitochondria than control rats. 81 Human studies have also described abnormalities of cardiac mitochondria with hypoMg. 44
HypoMg is associated with increased levels of catecholamines. Animals fed a Mg-deficient diet demonstrated a dramatic increase in myocardial injury following exposure to isoprenaline. 82 Isolated perfused rat hearts with low-Mg demonstrated a 20–37% reduction in coronary blood flow, a 25–50% reduction in cardiac output and stroke volume, 3- to 4-fold elevations in lactate production, and eventual irreversible cardiac failure. 83 Mg reduces catecholamine release from both adrenal medulla and peripheral adrenergic nerve terminals, and is a highly effective alpha-adrenergic antagonist and antiarrhythmic in the setting of high-dose epinephrine infusions. 84 Magnesium infusions have been shown to be effective in the perioperative management of phaeochromocytoma, as well as in reversing systolic dysfunction with both dilated and Takotsubo cardiomyopathy with phaeochromocytoma crisis.84–87
Hypomagnesaemia may be associated with hypokalaemia, hypocalcaemia and hypophosphataemia, which may affect cardiac function.
Mg deficiency and PPCM – geographical associations
Attempts to test for a possible relationship between incidences of hypoMg, dietary Mg intake, and PPCM among populations are significantly limited by a lack of data regarding prevalence of hypoMg globally, variations in assays and se Mg defining hypoMg, and heterogeneity of populations studied 23 (Table 3). A strong correlation, however, was found between incidence of PPCM and dietary Mg intake (r = 0.713).
Global incidences of PPCM, hypomagnesaemia, and dietary Mg intake – countries listed from highest to lowest incidence PPCM.
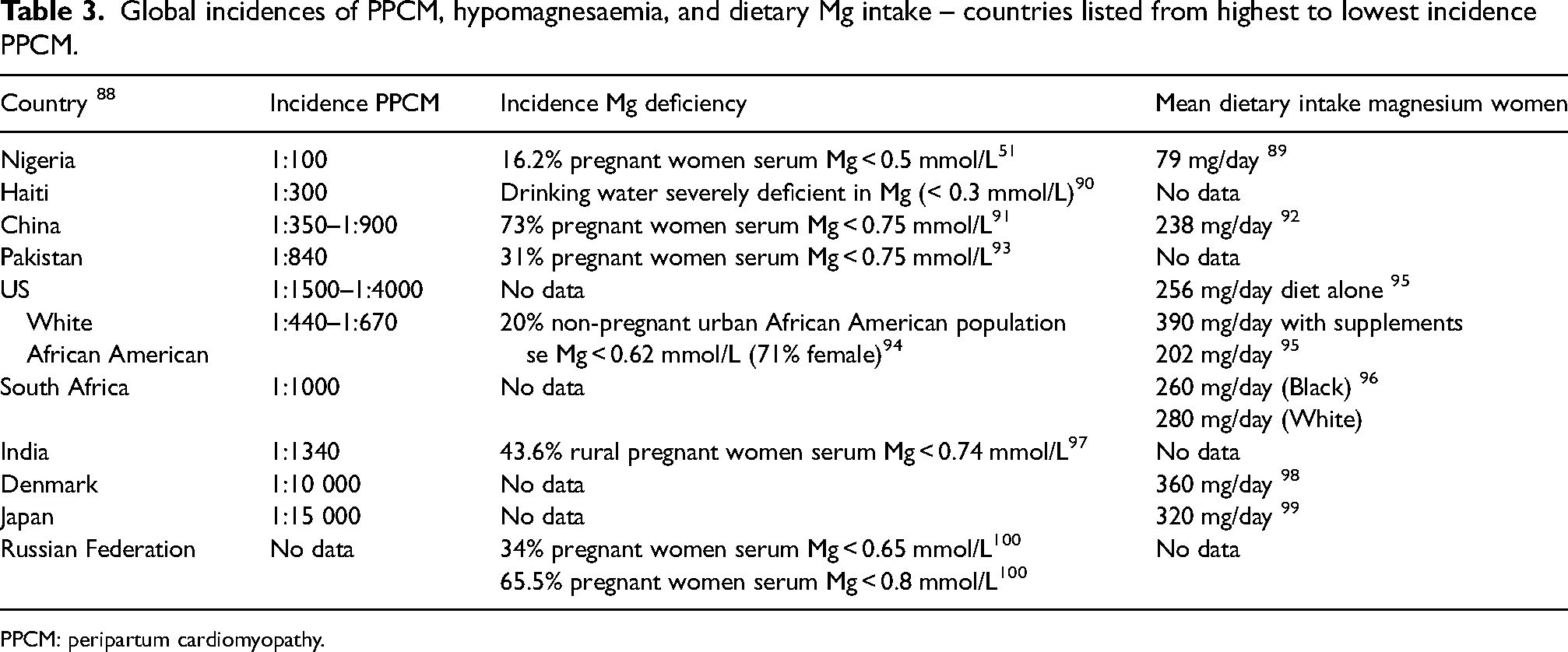
PPCM: peripartum cardiomyopathy.
Potential implications for management
A single-centre, randomised placebo-controlled double-blind study of 79 non-pregnant patients with severe congestive heart failure (NYHA IV) receiving optimal medical therapy found the use of magnesium orotate as adjuvant therapy improved survival, clinical symptoms, and patient quality of life. 101
Mineralocorticoid receptor antagonists are not effective in increasing se Mg concentration. Amiloride and sodium-glucose transporter 2 inhibitors (SGLT2i) increase serum Mg by reducing renal Mg loss, through increasing reabsorption in the distal nephron. 102 Amiloride was shown to increase lymphocyte intracellular free Mg in patients treated with furosemide compared with furosemide alone. 103 SGLT2i reduces mortality, rehospitalisation, and adverse cardiac outcomes in individuals with heart failure with reduced ejection fraction. 104 No studies have specifically examined the use of SGTL2i or amiloride in PPCM or the efficacy of amiloride in cardiac failure.
A study examining improvements in intracellular tissue Mg with intravenous Mg therapy demonstrated greater improvement with doses of Mg larger than 40 mmol/24 h. 19 Up to 160 mmol of intravenous Mg may be required over five days to correct deficiency. 105
Animal studies have not demonstrated teratogenicity with amiloride. Amiloride use has been described in only ten human pregnancies in the management of Gitelman, Liddle and Geller syndromes, and primary aldosteronism, without adverse maternal or fetal outcomes.106–109 SGTL2i have been shown to cross the placental barrier in ex-vivo human placental perfusion models with a maximal fetal to maternal concentration of 0.38–0.67. 110 The adjusted risk for any and cardiac major congenital malformation following periconception use of SGLT2i referenced against insulin use were 1.13 and 0.98 respectively. 111
Women with PPCM may be treated with dopamine agonists, or be advised against breastfeeding, although a study demonstrated that lactation was not associated with lower rates of myocardial recovery with PPCM. 112 Only one human case report has described the use of amiloride during breastfeeding, without adverse neonatal effects. While SGLT2i are ∼ 90% protein bound in plasma, and therefore unlikely to pass into breastmilk in clinically significant amounts, there is no published information to date regarding the safe use of SGTL2i with breastfeeding.
Future research possibilities
Retrospective studies of databases of individuals with PPCM or idiopathic dilated cardiomyopathy in pregnancy examining serum Mg, and myocardial Mg from autopsy or myocardial biopsy specimens may be helpful. Retrospective studies of women with preeclampsia complicated by PPCM comparing outcomes with and without parenteral Mg therapy may be informative. Prospective studies involving non-invasive measurement of myocardial or skeletal muscle Mg using phosphorous magnetic resonance spectroscopy (MRS), or alternatively measurement of sublingual epithelial cell Mg by energy-dispersive x-ray analysis, may provide information regarding tissue Mg concentration in PPCM and dilated cardiomyopathy in pregnancy. Prospective randomised double-blinded trials of intravenous Mg at a dose of at least 40 mmol/day for up to five days comparing outcomes in treatment groups and placebo control may be worthwhile. Genetic testing for RRAGD variations from retrospective databases as well as in future cases of dilated cardiomyopathy and PPCM may also be informative.
Conclusion
It is unclear whether Mg deficiency may be related to the development of pregnancy-related dilated cardiomyopathy, whether hypoMg and PPCM may co-exist due to common risk factors such as African ancestry, hypertensive disorders of pregnancy and diabetes mellitus, or may be an epiphenomenon. The reduction in tissue Mg as a result of physiological increased renal loss and transplacental transfer of Mg during pregnancy may predispose to PPCM or dilated cardiomyopathy in pregnancy. Further research in this area may be useful in determining whether magnesium therapy, and/or medications such as amiloride and SGLT2i, which may reduce renal Mg loss and stabilise or increase myocardial Mg may be useful in both the prevention and acute treatment of dilated cardiomyopathy in pregnancy.
Footnotes
Contributorship
AM researched, wrote and reviewed the manuscript.
Declaration of conflicting interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Ethical approval was provided by Mater Health Human Research and Ethics Committee QACR/MML/115905 (V2).
Funding
The author received no financial support for the research, authorship, and/or publication of this article.
Guarantor
AM.
Informed consent
Written informed consent was obtained from each patient for the inclusion of their anonymised information in this publication.
Trial registration
Not applicable.