
Abstract
Deep vein thrombosis (DVT) during pregnancy requires timely anticoagulation to prevent complications; however, the early postpartum period is associated with an inherently elevated risk of hemorrhage, creating competing management priorities. Herein, we describe the case of a woman with dichorionic diamniotic twin pregnancy who developed progressive femoral DVT despite therapeutic unfractionated heparin (UFH) and concurrent preeclampsia and acute kidney injury. Although postoperative hemostasis after caesarean delivery initially appeared stable, therapeutic UFH was restarted early as DVT continued to progress, requiring the resumption of standard treatment. Despite seemingly adequate early hemostasis, the woman developed a massive uterine wall hematoma that required uterine artery embolization. This case illustrates the complexity of balancing thrombotic urgency against fragile postpartum hemostasis and highlights the importance of individualized anticoagulation strategies for obstetricians, surgeons, anesthesiologists, and perioperative teams caring for high-risk patients.
Introduction
Venous thromboembolism (VTE) is a leading cause of maternal morbidity and mortality worldwide. 1 Pregnancy-associated deep vein thrombosis (DVT) requires prompt therapeutic anticoagulation; however, clinicians must consider the heightened risk of bleeding inherent to pregnancy and the early postpartum period. 1 Although international guidelines recommend low-molecular-weight heparin (LMWH) as first-line therapy,1,2 unfractionated heparin (UFH) is commonly used in Japan owing to insurance restrictions, 3 and the short half-life and full reversibility of UFH, which are advantageous when postoperative hemostasis may be unstable.1,2
Managing therapeutic anticoagulation following caesarean delivery is challenging, as surgical hemostasis often remains fragile for several days.4,5 Therefore, clinicians must weigh the competing risks of thrombus propagation and postpartum hemorrhage when determining when to restart anticoagulation.
Case report
A 34-year-old woman was pregnant for the first time, with a dichorionic diamniotic twin pregnancy conceived by frozen-thawed embryo transfer. She was admitted at 26 weeks and 4 days of gestation with threatened preterm labor. On admission, she complained of left inguinal pain, and lower-extremity ultrasonography revealed a thrombus in the left femoral vein. Therapeutic UFH infusion was initiated and titrated to maintain an activated partial thromboplastin time (APTT) of 1.5 to 2.5 times the control value.
A repeat ultrasound at 28 weeks and 6 days revealed no improvement in the thrombus, and further progression was confirmed at 31 weeks and 6 days. Although the woman's subjective symptoms remained unchanged, during this period she developed preeclampsia with worsening renal function, and serum creatinine levels reached 90.2 µmol/L (1.02 mg/dL) at 32 weeks and 4 days. As both fetuses were breech and the maternal condition was deteriorating, caesarean delivery was planned. Therefore, in anticipation of surgery, an additional ultrasound examination was performed to reassess the thrombus status and guide perioperative management, given the uncertainty regarding thrombus resolution.
A temporary inferior vena cava (IVC) filter was placed the day before surgery after reviewing previous reports of pulmonary embolism occurring intraoperatively in similar situations. 4
A caesarean delivery was performed at 32 + 4 weeks. Anticoagulation therapy was discontinued at 00:00 on the day of surgery, and the caesarean delivery was performed at 09:00. The uterine incision was closed in two layers using a continuous barbed suture (Stratafix™, size 0). No uterine pathology, such as fibroids, was noted intraoperatively. No intra-abdominal drain was placed. For uterine contraction, 5 units of oxytocin were administered intramyometrially after placental delivery, followed by an intravenous infusion of 10 units of oxytocin diluted in 500 mL of extracellular fluid. Tranexamic acid was not used.
The estimated blood loss was 2730 mL, and 900 mL of autologous blood was administered. The hemoglobin level was 11.0 g/dL postoperatively and 10.3 g/dL on postoperative day (POD) 1. The APTT was 41.9 s, lower than the target therapeutic range. Anti-Xa activity was not measured, as anticoagulation was monitored using APTT according to institutional practice. Transvaginal and transabdominal ultrasonography on POD1 revealed no uterine wall hematoma. As DVT had progressed antepartum, standard therapeutic anticoagulation needed to be resumed postpartum; consequently, therapeutic UFH was restarted 24 h postoperatively and titrated to maintain an APTT of 1.5–2.5 times the control value. On day 4 post-delivery, the woman suddenly developed lower abdominal pain, and her hemoglobin level decreased to 7.1 g/dL. Contrast-enhanced CT revealed a hematoma at the myometrial incision site, along with multiple sites of contrast medium extravasation within the uterine cavity (Figure 1). She was subsequently transferred to a tertiary center, where she received six units of red blood cells and underwent successful uterine artery embolization. The IVC filter was removed at the referral center on the first day after transfer (one day after the interventional radiology procedure). UFH was temporarily discontinued but restarted day 8 post-delivery. Subsequently, the woman was transitioned to an oral anticoagulant on day 16. Subsequently, the woman was transitioned to an oral anticoagulant on day 16, specifically edoxaban (Lixiana®) 30 mg once daily, and the woman did not breastfeed. Follow-up CT on POD36 showed a reduction of the hematoma to 10.7 cm, with no further bleeding.
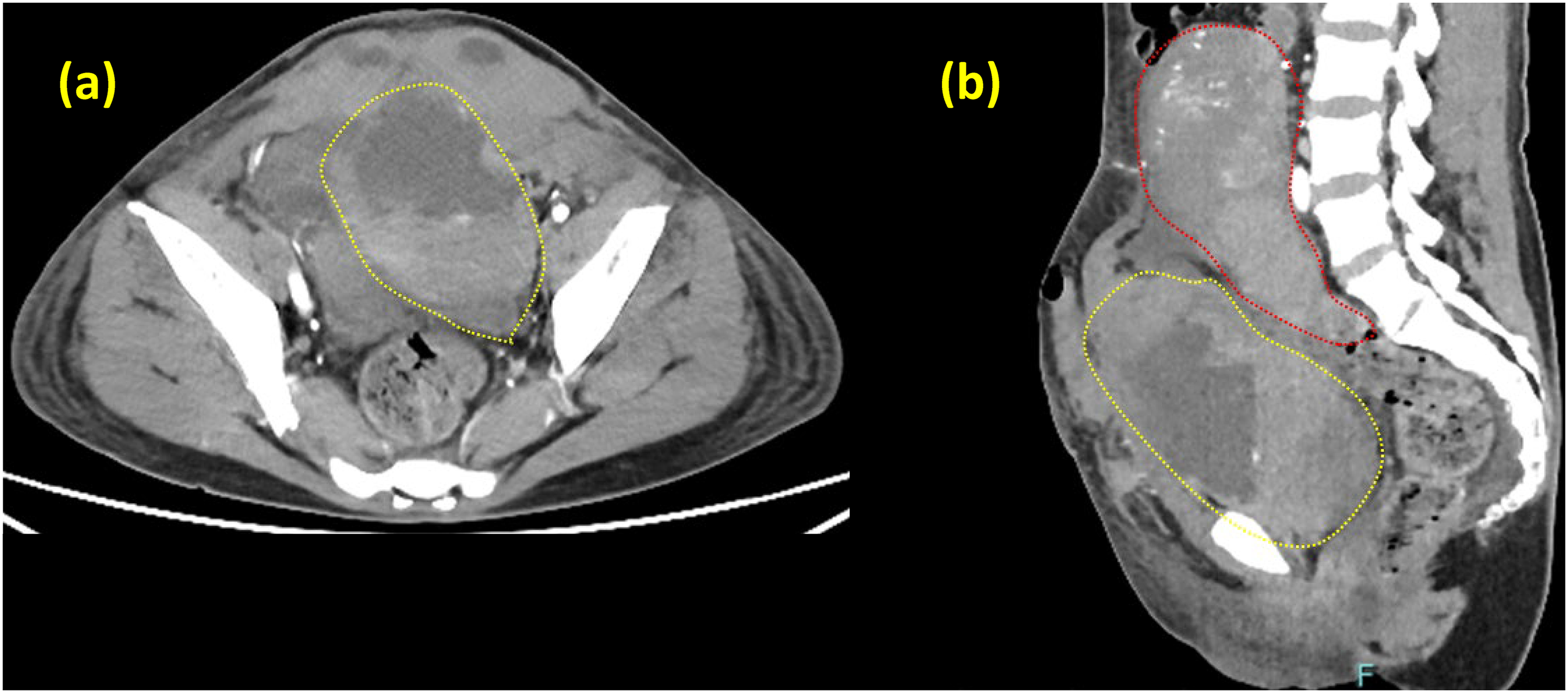
Computed tomography imaging of the uterine wall hematoma. (a, b) The area surrounded by a yellow dotted line shows the uterine wall hematoma of size 16 × 11 × 8 cm. The area surrounded by the red dotted line represents the uterus, and multiple sites of contrast medium extravasation can be identified.
Discussion
This case highlights the challenges associated with managing therapeutic anticoagulation during the early postpartum period. In cases where DVT progresses during pregnancy, delaying postoperative anticoagulation is not a viable option, even if postpartum hemostasis remains unstable. Although LMWH is recommended in international guidelines, its long half-life and limited reversibility complicate use in cases where rapid adjustments are needed.1,2 Conversely, UFH provides advantages such as flexible dosing, rapid titration, and complete reversibility, making it suitable for situations in which maternal clinical status may change rapidly or bleeding risk is elevated. 6 As the IVC filter—which was placed for intraoperative pulmonary embolism prophylaxis—cannot be left in place permanently, and because the patient's femoral DVT had already progressed despite antepartum anticoagulation, continued therapeutic UFH in the postpartum period was required to prevent pulmonary embolism and ensure adequate management of worsening thrombosis. Although the presence of an IVC filter may allow some flexibility in postoperative anticoagulation strategies, including the use of prophylactic-dose heparin, this approach may be insufficient in patients with progressive thrombosis. In the present case, the femoral DVT had demonstrated progression despite antepartum therapeutic anticoagulation, suggesting a high thrombotic burden. Furthermore, while an IVC filter can reduce the risk of pulmonary embolism, it does not prevent thrombus propagation in the lower extremities. Therefore, early resumption of therapeutic anticoagulation was considered necessary despite the increased risk of hemorrhage.
Our institution is the only tertiary perinatal center in the region capable of managing very low birth weight neonates. At 32 weeks and 4 days of gestation, the estimated fetal weights of the twins were 1168 and 2142 g. Postnatal management of the smaller twin was only feasible at our institution. Neonatal transport of very low birth weight infants carries major risks and is avoided whenever possible. Although interventional radiology was not immediately available at our institution, prompt transfer to a specialized center enabled successful management. These considerations reflect real-world constraints in regional perinatal care systems and the importance of system-level decision-making.
Although UFH offers advantages in terms of rapid titratability and complete reversibility, a previous study suggested that therapeutic UFH may be associated with a slightly higher risk of bleeding than LMWH, particularly when applied in the postoperative setting. 7 As such, it is possible that the choice of UFH, while clinically necessary in the present case, may have contributed to the development of the postpartum uterine wall hematoma.
This case highlights the clinical importance of preoperative counseling, including a discussion of the increased likelihood of postpartum hemorrhage and the potential need for interventions such as uterine artery embolization or even hysterectomy in cases of progressive femoral DVT during pregnancy.
The increasing prevalence of caesarean delivery, multifetal pregnancy, advanced maternal age, and assisted reproductive technologies has contributed to a recent rise in pregnancy-associated VTE.8,9 Consequently, situations involving high thrombotic risk and unstable postpartum hemostasis are likely to become more common. Individualized risk assessment and close multidisciplinary collaboration among obstetricians, surgeons, anesthesiologists, and perioperative nursing staff are essential in such cases.
In conclusion, therapeutic anticoagulation in the early postpartum period carries a substantial risk of hemorrhage, even when postoperative hemostasis initially appears stable. This case highlights the need for vigilant monitoring, individualized decision-making, and clear patient counseling in patients with thrombotic and bleeding risks. Although common in contemporary obstetric practice, this scenario underscores the following key considerations: (a) early reinstatement of therapeutic anticoagulation can precipitate major postpartum bleeding; (b) UFH, while advantageous for its rapid titratability and reversibility, carries an important hemorrhagic risk; and (c) optimal management of such cases requires coordinated multidisciplinary care involving obstetric, surgical, anesthetic, and perioperative teams.
Footnotes
Acknowledgments
Ethical considerations
This case report was conducted in accordance with the principles of the Declaration of Helsinki. Ethical approval was not required for reporting this individual case according to institutional guidelines. Written informed consent for publication of the clinical details and any accompanying images was obtained from the patient. All identifying information has been anonymized to protect patient privacy.
Informed consent
The patient provided written informed consent for the publication of this case report.
Consent to participate
Informed consent to participate was not required because this study is a case report.
Consent for publication
Written informed consent was obtained from the patient for the publication of anonymized clinical information and any accompanying images.
Authorship
All authors meet the International Committee of Medical Journal Editors (ICMJE) criteria for authorship. All authors made substantial contributions to the conception and design of the work, acquisition and interpretation of data, and drafting and critical revision of the manuscript. All authors approved the final version of the manuscript and agree to be accountable for all aspects of the work.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability
The data that support the findings of this study are available from the corresponding author upon reasonable request. The data are not publicly available due to their containing information that could compromise the privacy of research participants.
Guarantor
Dr Rei Sunami is the guarantor of this work and takes full responsibility for the integrity of the data and the accuracy of the data analysis.