
Abstract
Platelets play a vital role in haemostasis; therefore, an increase or decrease in levels or a disorder of platelet function can lead to symptoms such as easy bruising and excessive bleeding, particularly from mucocutaneous sites. Patients may also report symptoms associated with the underlying condition. Platelet disorders pose a particular challenge for primary care, due to the vast array of potential causes and clinical outcomes, ranging from little effect to life-threatening problems. Initial assessment in primary care should aim to identify those requiring urgent investigation or treatment, while also determining an underlying cause and potential complications.
Clinical case scenario
James is a 52-year-old male with a 30 pack-year smoking history. He presents with fatigue and loss of appetite. You request blood tests, including a full blood count and a chest X-ray as per the National Institute for Health and Care Excellence suspected lung cancer pathway. On review of the blood results, you note a raised platelet count (650 × 109/L). The chest X-ray, unfortunately, shows an abnormality that is suspicious for a malignancy. You call James into the surgery to discuss the results of the chest X-ray and arrange an urgent 2-week rule referral. James is understandably anxious and asks how long he will have to wait to be seen in hospital.
What are platelets?
Platelets are anucleated disc-shaped cells derived from megakaryocytes within the bone marrow. They are responsible for initiating haemostasis by responding to an injury to the vascular endothelium, which ultimately leads to the formation of a blood clot, and allows repair of the injury (Abrams, 2020). They have a lifespan of 5 to 7 days.
Towards the end of their lifespan, they are removed from blood vessels by macrophages and neutrophils, which transport them to the spleen to be removed from the body (Holinstat, 2017). Thrombopoietin is a platelet growth factor that is produced primarily in the liver. It amplifies the production rate of megakaryocytes and therefore platelets (Kuter, 2020).
Thrombocytopenia
Thrombocytopenia is defined as a circulating platelet count of less than 150 × 109/L and is a commonly encountered haematological abnormality. There is little variation in the platelet count of a healthy individual over time. Therefore, a reduction in an individual’s platelet count can be clinically concerning, even if it remains within normal range (Arnold and Cuker, 2020a). The main mechanisms responsible for the development of thrombocytopenia are; reduced platelet production; increased platelet destruction; and sequestration of platelets in the spleen (Geyer, 2018). Dilution by fluid resuscitation or consumption of platelets in thrombi can also lead to lowered count levels (Arnold and Cuker, 2020a).There are a vast array of causes of thrombocytopenia, some of which are summarised below.
Immunological conditions
Immune thrombocytopenia, also known as immune thrombocytopenic purpura (ITP) is an autoimmune haematological condition, whereby autoantibodies lead to the destruction of peripheral platelets. It is classified as either primary or secondary depending on whether an underlying associated medical condition is identified (Scully, 2019).
Primary ITP is further classified as acute or chronic. Acute ITP is most commonly seen in children following a viral illness. Approximately 90% of cases will completely recover; whereas, the remaining 10% will go on to develop chronic ITP. Chronic ITP is most common in young women and rarely undergoes spontaneous remission (National Institute for Health and Care Excellence (NICE), 2016).
Secondary ITP occurs due to an underlying condition, such as antiphospholipid syndrome, systematic lupus erythematous, human immunodeficiency virus (HIV), hepatitis C infection and chronic lymphocytic leukaemia (Arnold and Cuker, 2020b). In rheumatoid arthritis, thrombocytopenia is more likely to be related to splenomegaly, occurring in Felty’s syndrome or secondary to medication (Scully, 2019). Complaints of joint pain, morning stiffness and weight loss may suggest an underlying rheumatological condition (Arnold and Cuker, 2020a).
Drugs
Numerous medications can result in thrombocytopenia, but certain agents are more commonly implicated. Alcohol can cause direct toxicity to the bone marrow, associated liver disease or nutrient deficiencies (Arnold and Cuker, 2020a).
Heparin can result in heparin-induced thrombocytopenia (HIT), whereby antibodies lead to platelet activation and a paradoxical increased risk of arterial and venous thrombosis. Although rare, it is an important differential, as it is a potentially life-threatening complication of heparin exposure. It typically occurs within 5 to 10 days of heparin administration, but should be considered in patients exposed to heparin within the previous 14 days (Arnold and Cuker, 2020a). This is increasingly relevant in primary care, as more patients are receiving thromboprophylaxis in the community (Bradbury and Murray, 2013).
Other commonly implicated medications include antibiotics (e.g. sulphonamides, ampicillin, piperacillin, vancomycin, rifampin), anti-epileptics (e.g. carbamazepine, phenytoin, valproate), quinine, gold and thiazides (Bradbury and Murray, 2013). Daily exposure to a new drug can result in thrombocytopenia developing over 1 to 2 weeks. However, if a patient has been previously exposed to the drug, it may occur within hours of exposure. Platelet levels should normalise 5 to 7 days after medication cessation (Arnold and Cuker, 2020a). Cytotoxic medications including chemotherapy and radiotherapy lead to myelosuppression and typically cause a pancytopenia.
Viral infections
Thrombocytopenia can occur following many viral infections (e.g. rubella, mumps, varicella, parvovirus) and will typically resolve after recovery from the illness.
However, hepatitis C can result in a chronically low platelet count. Any infection that causes acute hepatitis can lead to thrombocytopenia by affecting thrombopoetin production by the liver. In those with HIV infection, low platelets can occur via several mechanisms, including secondary ITP. It is important to note that an isolated thrombocytopenia may be the initial presentation of HIV infection (Arnold and Cuker, 2020a).
Bacterial infection and sepsis
Sepsis can lead to increased consumption and destruction of platelets or direct suppression of the bone marrow. Other infections such as leptospirosis, brucellosis and malaria can also lead to thrombocytopenia (Arnold and Cuker, 2020a).
Bone marrow disorders and malignancy
Thrombocytopenia can occur in several primary haematological disorders such as myelodysplastic syndrome and bone marrow failure syndromes, as well as bone marrow infiltration by a malignancy (e.g. leukaemia, lymphoma, myeloma and metastases). An isolated thrombocytopenia would be rare in these cases and the full blood count (FBC) test would typically show other cytopenias (Arnold and Cuker, 2020a; Patient, 2015a). Symptoms such as weight loss, fatigue, bone pain and night sweats may point towards a malignant cause.
Liver disease and hypersplenism
In patients with portal hypertension and hypersplenism, thrombocytopenia can occur via sequestration of platelets in the spleen. In those with severe liver disease, platelet production is affected via reduced production of thrombopoeitin in the liver (Bradbury and Murray, 2013).
Vitamin deficiencies
Vitamin B12, folate (Bradbury and Murray, 2013) and copper (Arnold and Cuker, 2020a) are required for haematopoeisis, and therefore, deficiencies of these vitamins can lead to thrombocytopenia or a mild pancytopenia. These patients can be asymptomatic or display signs and symptoms of the relevant deficiency.
Enquiring about dietary practices is therefore important. Vegetarianism and veganism may predispose to nutrient deficiencies and are increasingly common in today's society. Quinine consumption (e.g. tonic water) can produce an immune-mediated reaction leading to a profound thrombocytopenia (Bradbury and Murray, 2013).
Thrombotic microangiopathy
Haemolytic uraemic syndrome (HUS), Thrombotic thrombocytopenic purpura (TTP) and drug-induced thrombotic microangiopathy are rare in adults but should be considered in patients with a low platelet count and a microangiopathic anaemia (Arnold and Cuker, 2020a).
Approaching a low platelet count
A finding of thrombocytopenia, especially if incidental or unexpected, should prompt three initial questions: Is it real? Is it new? Are there any other FBC abnormalities? (Arnold and Cuker, 2020a):
Is it real? ‘Pseudothrombocytopenia’ can occur due to the action of ethylenediaminetetraacetic acid (EDTA), which is an anticoagulant found in certain blood sample tubes. EDTA can cause ‘platelet clumping’ and a falsely low reading in up to 0.1% of the population. It may be necessary to repeat the FBC test using a citrate or heparin-coated tube in the first instance (Patient, 2015a) Is it new? Reviewing the trend of the platelet count is important. A new reduction would be more concerning than a mildly low or stable count. A drop in the platelet count of 50% would be particularly concerning Are there any other abnormalities on the FBC? Examples would include anaemia, leukopenia, leukocytosis. This would generally point towards a more serious diagnosis and may prompt a more urgent review
History and examination
Are they bleeding? The most common sites of bleeding in platelet disorders are mucocutaneous surfaces. The patient may report bleeding from the mouth and gums, nose, gastrointestinal and urinary tract, as well as heavy menstrual bleeding (Geyer, 2018). They may describe a history of easy bruising, excessive or frequent epistaxis or prolonged or excessive bleeding following tooth extractions or other procedures. Medication such as aspirin or non-steroidal anti-inflammatory drugs (NSAIDs) may exacerbate their bleeding symptoms (Patient, 2015a). Determining the onset of bleeding is also helpful. A recent history of bleeding or previously normal platelet counts would likely indicate an acquired disorder (Bradbury and Murray, 2013). Certain disorders that result in thrombocytopenia carry a risk of thrombosis, instead of, or in addition to, bleeding. Although rare, this is an important consideration. Examples include HIT, HUS, TTP, paroxysmal nocturnal haemaglobinuria and ITP associated with a thrombotic disorder (Arnold and Cuker, 2020a).
The history should then focus on determining the underlying cause by enquiring about signs and symptoms relating to the conditions described above. The patient’s demographics may be useful. For example, myelodysplasia is more common in older patients, whereas thrombocytopenia in a younger patient may point towards a congenital cause (Bradbury and Murray, 2013). A family history of bleeding problems may suggest a hereditary cause; however, it is important to remember that the absence of this does not exclude inherited disorders, as they often go undiagnosed.
The clinical examination should aim to identify signs of bleeding and an underlying condition. The patient may have petechiae and ecchymoses, which are generally small and superficial, but can be significant (Arnold and Cuker, 2020a).
Although very rare, it is important to note that central nervous system bleeding is the most common cause of death in severe thrombocytopenia. Fundoscopy should therefore be performed looking for retinal haemorrhage (North Devon Health, 2015), as well as an examination of the mouth, checking for bleeding at the back of the buccal mucosa, which is advancing forwards. Both are possible signs of impending intracranial haemorrhage and would therefore warrant emergency intervention (Geyer, 2018).
An examination of the liver, spleen and lymph node regions is essential.
Lymphadenopathy or hepatosplenomegaly should prompt investigation for lymphoproliferative disease, autoimmune disease, cancer, or infection. The remainder of the examination should then be directed by clinical findings. In an asymptomatic patient with isolated thrombocytopenia and no clinical signs, ITP is the most likely diagnosis (Bradbury and Murray, 2013).
Investigation
In addition to repeating the FBC test, a peripheral blood film is required in all cases. It can help to exclude pseudothrombocytopenia and may reveal characteristic morphological appearances leading to a diagnosis (Arnold and Cuker, 2020a; Bradbury and Murray, 2013). Other investigations that may be indicated include liver function tests, urea and electrolytes, lactate dehydrogenase, C-reactive protein, immunoglobulins, HIV, hepatitis C, clotting factors, vitamin B12 and folate (Bradbury and Murray, 2013).
Management of thrombocytopenia.
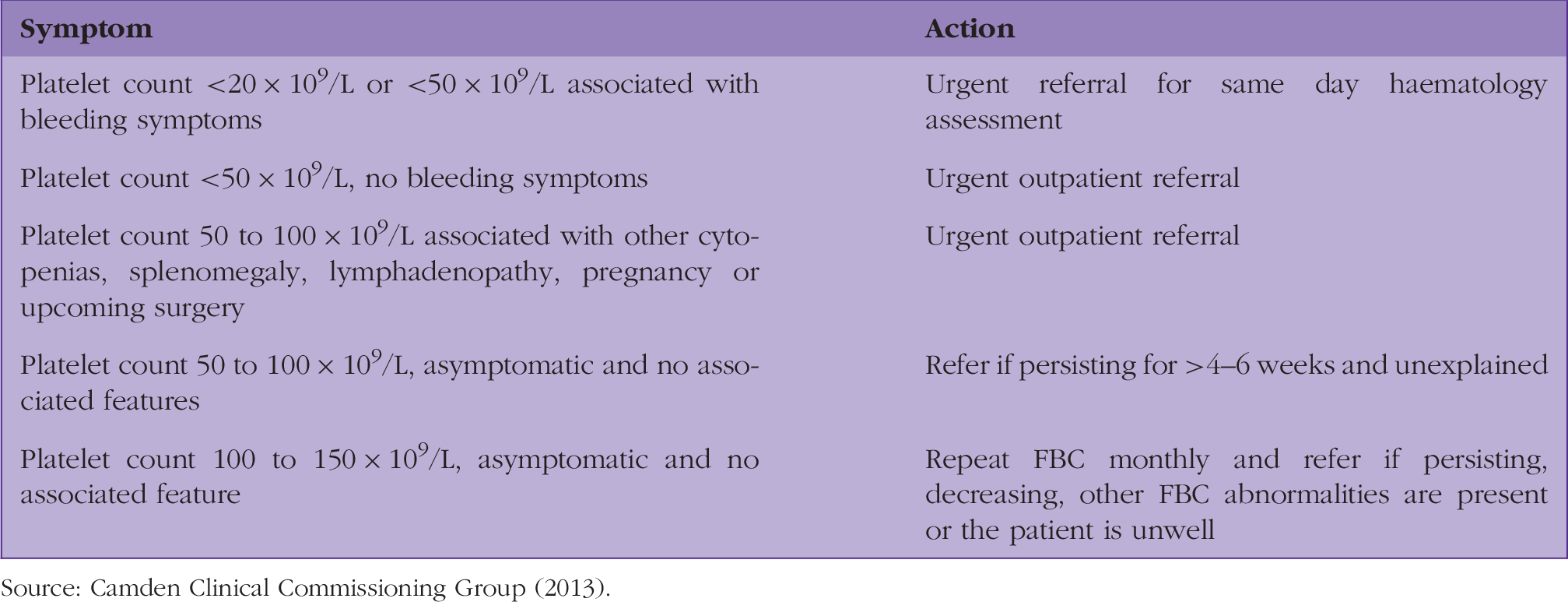
Important points:
A small percentage of patients with a mild thrombocytopenia (100 to 150 × 109/L) will normalise over 1 to 2 months (Arnold and Cuker, 2020a) Suspicion of certain conditions such as HIT, TTP, HUS, drug-induced thrombotic microangiopathy, acute leukaemia, aplastic anaemia and bone marrow failure syndromes should prompt immediate action (Arnold and Cuker, 2020a) Rarely, but significantly, an isolated thrombocytopenia can be the initial presentation of acute leukaemia, highlighting the importance of repeat testing (Bradbury and Murray, 2013) It is important to note that the categorisation of platelet levels is quite arbitrary, and the risk of bleeding is not based on the platelet count alone (Bradbury and Murray, 2013). If there are clinical concerns regarding bleeding or the underlying disorder, then appropriate referral or discussion with a haematologist should be arranged
Thrombocytopenia in pregnancy
Thrombocytopenia is the second-most-common haematological abnormality found during pregnancy (Rajasekhar et al., 2013). During normal pregnancy there is a physiological decrease in platelet levels, which can result in a mild thrombocytopenia that has no adverse effects to the mother or foetus. However, other conditions can have severe maternal and foetal consequences, and may require additional monitoring or treatment during pregnancy (Ciobanu et al., 2016).
Gestational thrombocytopenia accounts for 70–80% of all cases of thrombocytopenia in pregnancy. It most commonly occurs during the mid-second to third trimester and the platelet count will typically remain above 70 × 109/L. The exact mechanism of action is not known. However, it is thought to be related to haemodilution and accelerated clearance of platelets. It is a diagnosis of exclusion, and no specific management is required if the platelet count remains above 70 × 109/L. Gestational thrombocytopenia should resolve within 6 weeks of childbirth (Rajasekhar et al., 2013).
Hypertensive disorders account for approximately 20% of cases of thrombocytopenia in pregnancy (Ciobanu et al., 2016). There is significant overlap between these disorders, making it difficult, and sometimes impossible, to differentiate between them. They are classified as obstetric emergencies (Lee and Reau, 2020):
Severe pre-eclampsia: Pre-eclampsia is defined as the onset of new hypertension after 20 weeks of pregnancy in association with one or more new-onset conditions, including thrombocytopenia (NICE, 2018) HELLP syndrome (haemolysis, elevated liver enzymes and low platelets): This severe form of pre-eclampsia is characterised by haemolysis, elevated liver enzymes and low platelet counts. It is associated with high morbidity and mortality for mother and baby (NICE, 2018). Seventy percent of cases of HELLP syndrome occur in the late second or third trimester, with the remaining 30% of cases occurring postpartum (Rajasekhar et al., 2013) Acute fatty liver of pregnancy: This is a rare, but serious, condition characterised by maternal liver dysfunction, which may be associated with other laboratory abnormalities including thrombocytopenia (Lee and Reau, 2020)
ITP accounts for 3–4% of cases of thrombocytopenia during pregnancy; although the outcome is not worsened during pregnancy there may be adverse foetal and maternal consequences, and it is therefore important to be aware of its possible existence (Ciobanu et al., 2016). Notably, women with ITP are at increased risk of venous thromboembolism in the postpartum period (Rajasekhar et al., 2013).
Functional platelet disorders
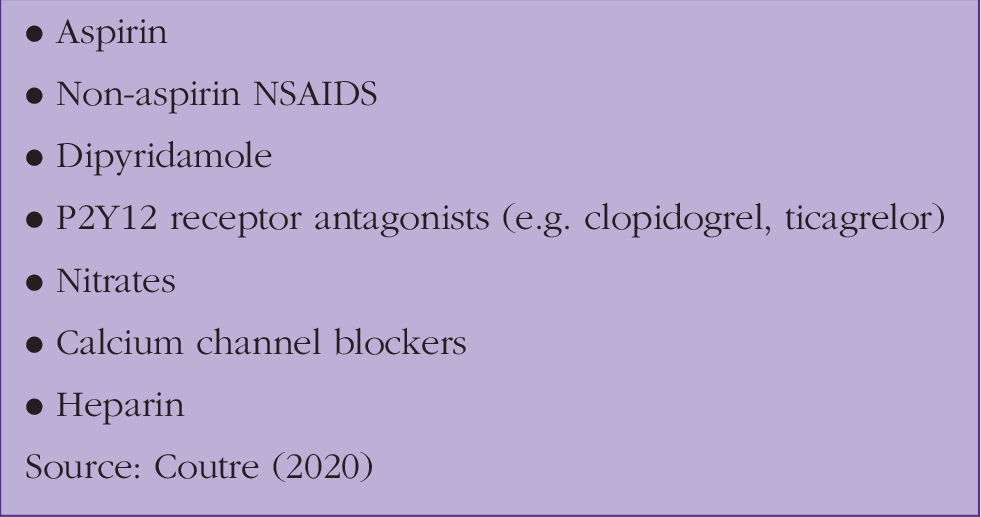
Medications causing disordered platelet function.
Von Willebrand disease.

History and examination
The bleeding manifestations associated with platelet disorders are the same as those in thrombocytopenia (described above). History and examination should focus on eliciting signs of bleeding while also looking for an underlying diagnosis. A thorough drug history is vital, including details of over-the-counter medications and herbal remedies. For example, the bleeding symptoms associated with aspirin are usually mild, however, anti-platelet therapy is often poorly tolerated in someone with an underlying disorder of platelet function and symptoms may worsen following initiation (Konkle, 2011).
Investigation
The initial evaluation of a patient with a suspected platelet disorder should include a FBC, peripheral blood film (Coutre, 2020) and clotting screen (Konkle, 2011). Further investigations should then be guided by clinical findings.
What are the next steps? If a medication is suspected as the cause, it may be appropriate to substitute this for another or to stop and observe for a period of time. Most patients will require referral to a haematologist for further investigation. The urgency of referral would depend on clinical findings and results of initial investigations (Ma, 2020).
Thrombocytosis
Thrombocytosis in adults is defined as a platelet count greater than 450 × 109/L. It is classified as either ‘primary’ (‘autonomous’) or ‘reactive’ (‘secondary’) (Tefferi, 2020). Approximately 1.5 to 2.2% of those over 40 years in age will have an incidental finding of thrombocytosis on a FBC, making it a common finding in primary care (Mathur et al., 2019).
Primary thrombocytosis occurs due to a failure of the mechanism by which platelets are produced. In adults this mostly occurs due to an acquired mutation of genes which regulate thrombopoeisis (Tefferi, 2020). Primary thrombocytosis is most characteristic of essential thrombocythaemia; however, it can also be seen in other myeloproliferative diseases including polycythaemia ruba vera, primary myelofibrosis, chronic myeloid leukaemia and some myelodysplastic syndromes (Mathur et al., 2019) and occasionally in acute myeloid leukaemia (Tefferi, 2020).
Reactive thrombocytosis is more common, and is considered to be a physiological response to a primary problem. The mechanism of action depends upon the underlying cause. However, it is largely driven by thrombopoeitic growth factors released in response to the underlying condition. These growth factors stimulate production and proliferation of the megakaryocyte, which in turn leads to platelet production. Platelet levels should normalise after resolution of the acute disease state. There are multiple causes of reactive thrombocytosis including acute blood loss, anaemia, malignancy, infections, acute and chronic inflammation, trauma and post-splenectomy patients or those with functional asplenia, e.g. sickle cell disease (Mathur et al. 2019;Tefferi, 2020).
History and examination
Symptoms associated with thrombocytosis
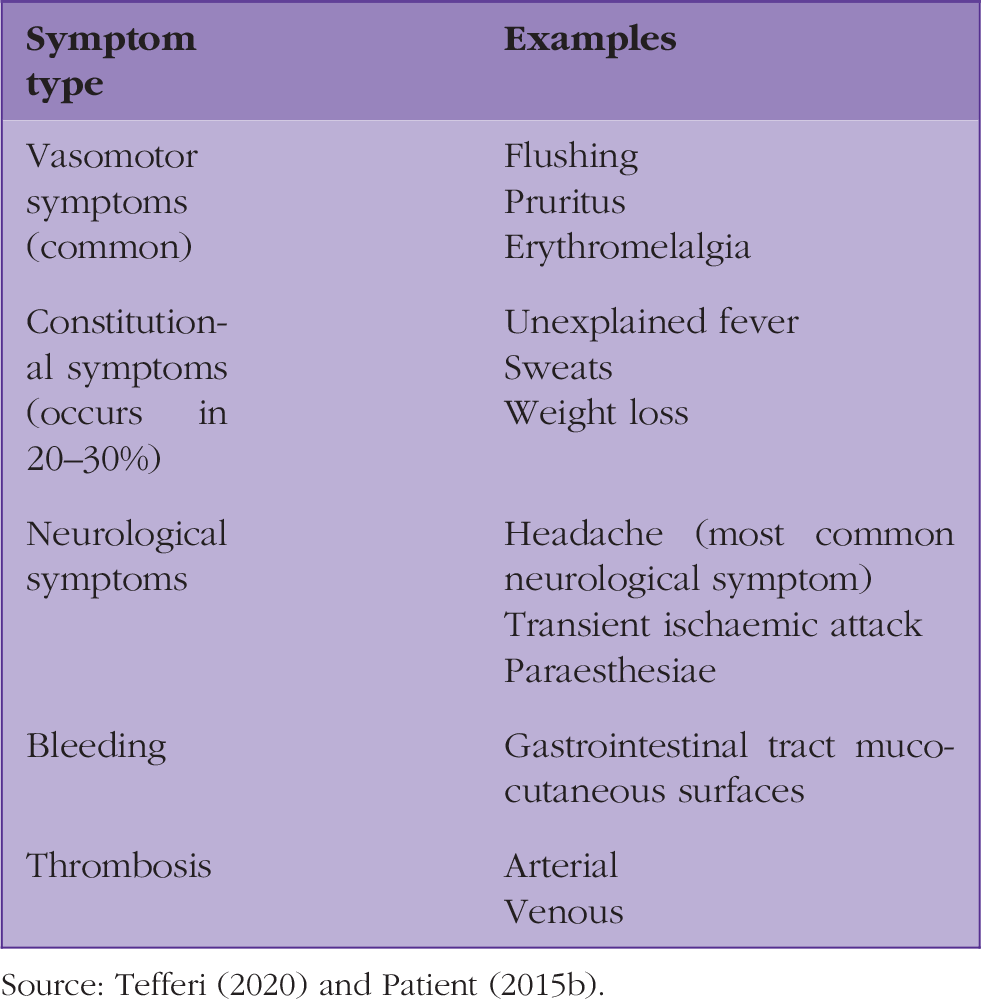
Source: Tefferi (2020) and Patient (2015b).
Paradoxically, these patients are at an increased risk of bleeding and thrombosis. Bleeding primarily occurs in the gastrointestinal tract, although this is unusual unless the platelet count exceeds 1000 × 109/L. There is a risk of arterial and venous thrombosis. Arterial thrombosis may occur in the cardiac, renal or lower limb arteries or may lead to neurological complications such as transient ischaemic attack and stroke. Venous thrombosis may occur in the splenic, hepatic, leg or pelvic veins. Pulmonary hypertension can occur due to thromboembolism. Thrombosis occurring at unusual or multiple sites in younger patients (e.g. aged under 45 years) should prompt evaluation for an underlying myeloproliferative disorder (Patient, 2015b). Hepatosplenomegaly is more likely to point towards a diagnosis of primary thrombocytosis (Patient, 2015b). At the time of presentation, 40-50% of those with primary thrombocytosis have splenomegaly and 20% have hepatomegaly (Mathur et al., 2019).
The BMJ Best Practice has suggested an algorithm for the investigation of thrombocytosis, which is shown in Fig. 1 (Mathur et al., 2019). It is important to note that thrombocytosis has been integrated into the NICE suspected cancer guidelines (NICE, 2015). The results of a study published in the British Journal of General Practice in 2017 found that thrombocytosis is a risk marker for cancer in adults, particularly lung and colorectal cancer (Bailey et al., 2017).
Algorithm for the investigation of thrombocytosis.
KEY POINTS
There are a vast array of causes of thrombocytopenia, thrombocytosis and disordered platelet function Mucocutaneous surfaces are the most common site of bleeding in platelet disorders Urgent investigation is warranted if the platelet count is less than 20 × 109/L or less than 50 × 109/L associated with bleeding or other abnormalities or certain conditions are suspected ITP is not worsened during pregnancy, however, it may have adverse foetal and maternal consequences and therefore requires increased monitoring VWD is the most common bleeding disorder and often results in mild symptoms; however, bleeding can be severe Thrombocytosis is a risk marker for certain types of cancer in adults, especially lung and colorectal cancer