
Abstract
Background:
Robot-assisted cystectomy (RAC) is well established in the management of muscle-invasive or high-grade non-muscle invasive bladder cancer, but its role in benign disease is less well described. This case series represents the largest published experience of RAC for radiation cystitis and the largest series using an intracorporeal urinary diversion technique in this context.
Objectives:
To evaluate perioperative outcomes and adverse events following RAC for benign indications, and to compare outcomes between patients with radiation cystitis and other benign conditions.
Design:
Single-centre, retrospective case series.
Methods:
Patients undergoing RAC for benign disease (2013–2024) were identified from a prospectively maintained database and electronic health records. Demographic, perioperative, and postoperative data were analysed using descriptive statistics. Comparative analyses were performed between patients undergoing cystectomy for radiation-related indications and those undergoing surgery for other benign indications using t tests, Fisher’s exact tests, and Mann–Whitney U tests in R.
Results:
Seventy patients (mean age 65 years; range 23–96) underwent RAC. Indications included radiation cystitis (n = 34; 48.6%), other cystitis (n = 14; 20%), premalignant changes (n = 9; 12.9%), refractory overactive bladder (n = 8; 11.4%), neurogenic bladder (n = 4; 5.7%), and Fowler’s syndrome (n = 1; 1.4%). Intracorporeal ileal conduit diversion was performed in 57 cases (81%). Mean operative time was 334 min (range 180–540). Mean blood loss was 326 ml (100–1250) in the radiation group and 300 ml (100–800) in other patients. Mean follow-up was 16 months (1–58). No significant decline in renal function was observed at 1 year in either group (p = 0.8). Complications occurred in 46 patients (66%) within 90 days, with 34% graded Clavien-Dindo III or higher. Fifteen patients (21%) were readmitted within 30 days, and 8 (11%) required further intervention. Limitations include the retrospective design.
Conclusion:
RAC is safe and feasible for benign disease with no observed differences in outcomes between radiation cystitis and other indications in our cohort. Outcomes and complication rates observed are within the published ranges for malignancy-associated radical cystectomy.
Trial registration:
Not applicable.
Plain language summary
We examined the outcomes of robot-assisted bladder removal surgery for non-cancerous conditions. Our findings show that this procedure is safe and has similar complication rates to those seen in bladder cancer surgeries. This suggests that robotic surgery is a viable option for patients with severe benign bladder disease.
Introduction
Radical cystectomy is an established management option in the treatment of muscle-invasive or high-grade non-muscle-invasive bladder cancer. ‘Simple’ (benign) cystectomy, however, is an end-stage treatment for a range of benign conditions and for those with intractable bleeding, for example, radiation cystitis, although the case mix is often far from ‘simple’. In the United States, it is estimated that up to 8% of cystectomies are carried out for benign indications. 1 In our centre robotic approach has become standard of care for patients requiring cystectomy except for those where this is technically not feasible.
Urinary diversion, with or without cystectomy, is recommended as a last-resort treatment option in the European Association of Urology (EAU) guidelines for refractory overactive bladder, interstitial cystitis/bladder pain syndrome and neurogenic lower urinary tract dysfunction.2–6 Other indications include urogenital fistulae, refractory cystitis, for example, radiation-induced, refractory incontinence and, keratinising squamous metaplasia. 7 Concomitant cystectomy is usually recommended at the time of urinary diversion to avoid pyocystitis. 8
Aftreth et al. reviewed the current landscape of benign cystectomy, focusing on the open approach. Early complications vary, with the largest case series reporting a complication rate of 67% – with 28% requiring blood transfusions and over 57% Clavien-Dindo Grade II or higher. 7 Population-level studies report slightly lower complication rates before discharge at 35% for those with cystectomy, and 31% for diversion alone. 7 Short-term postoperative infection rates were notably higher for benign cystectomy at 31% versus 25% for oncological cystectomies. However, long-term quality of life and functional improvements were positive across cases. Most patients maintain sexual function following surgery, except for men undergoing resection of the prostatic nerve plexus. Several techniques for urinary diversion are available, each with specific advantages and limitations depending on the condition being treated. Ensuring patients are well-informed about these options before surgery significantly lowers regret associated with their diversion choice.
The robot-assisted approach has become popular in the oncological population, owing to lower blood loss, shorter hospital stays, and lower rates of venous thromboembolism compared to open cystectomy. 9 On the other hand, the robotic approach for benign cystectomy is less well researched, with only a handful case series published to date, mostly focusing on neurogenic bladder.10–20 Patients undergoing cystectomy for benign indications are often younger but may have more comorbidities or complex reconstructive needs. As a result, their complication profile may differ from that of patients undergoing radical cystectomy for malignancy, and outcomes observed in oncological series should not be directly extrapolated. This highlights the need to specifically study this heterogeneous benign population to better understand the safety and efficacy of robot-assisted approaches. Our study aims to expand the body of evidence on robot-assisted cystectomy (RAC) and provide valuable insights into its efficacy and safety for a range of benign indications.
Materials and methods
This study was a single-centre, retrospective case series which involved the review of a prospectively maintained database of over >1000 cystectomies and review of the institutional electronic health records where required. All patients undergoing RAC for benign pathology between April 2013 and February 2024 were included in the analysis, identifying 70 consecutive patients. All procedures were carried out at Guy’s and St Thomas NHS Foundation Trust, London, UK. Our centre performed 574 robot-assisted radical cystectomies in the study period. Six surgeons were involved. Our experience in part also reflects the learning curve of some surgeons. All procedures were carried out using a DaVinci robotic system (X or Xi), Intuitive Inc., USA. The introduction of robotic cystectomy at our centre followed a structured progression. All surgeons involved were experienced open pelvic and reconstructive surgeons and were already performing open cystectomy prior to undertaking robotic cases. Robotic training was undertaken using a stepwise approach with proctoring, initially performing less complex robotic reconstructive procedures such as colposuspension and ureteric reimplantation before progressing to more complex extirpative procedures including cystectomy and intracorporeal urinary diversion. This approach reflects real-world practice in functional urology, where formalised robotic training pathways are still evolving.
In all cases, a simple cystectomy was performed with a robotic approach, omitting the lymphadenectomy component of radical cystectomy in line with the established technique. 21 The patient is positioned in a low-lithotomy Trendelenburg position at 24° head down for cystectomy, which is reduced to about 10°–12° during urinary diversion to facilitate bowel anastomosis and ureteric reimplantation. In brief, our approach employs the Hasson method to create pneumoperitoneum and a 6-port technique (Figure 1). The ureters are identified at the iliac bifurcation and dissected to the detrusor, clipped and then divided. The left ureter is fed under the sigmoid to the right side and standard robotic cystectomy is performed. Fourteen of the 30 (46.7%) female patients had a hysterectomy either at the time of cystectomy, or as a prior operation. Thirty-two of the 40 (80%) male patients had prostatectomy either at the time of cystectomy, or as a prior operation.

Key operative steps: first row – six-trocar technique; second row – transposition of the left ureter using a stay suture beneath the sigmoid colon from left to right, and clipping the strings of both distal ureteric ends in the right iliac fossa to keep the ureters safe; third row – uretero-ileal anastomosis (Bricker technique) using two running semicircular sutures. A ureteral stent is inserted in each ureter prior to closing the cranial side of the anastomosis. The stents are tunnelled through the harvested ileal conduit which is exteriorised with the help of bedside assistant.
Following the bladder removal, urinary diversion is fashioned. In our department, an ileal conduit is the default diversion technique; ureterostomy is reserved for challenging salvage cases, patients with significant comorbidities or limited life expectancy to minimise operative time, while orthotopic neobladder reconstruction is offered to young, fit, and well-motivated patients willing to accept a higher risk of complications. Early in the study period, we performed an extracorporeal ileal conduit but subsequently transitioned into a fully intracorporeal technique.22,23 A 15–25 cm segment of the distal ileum is harvested 20–25 cm away from the ileocecal junction, depending on the patient’s body habitus. Continuity of the bowel is restored using an endo-GIA 60 mm or 60 mm + 45 mm. Ureters are anastomosed to the ileal loop employing the Bricker technique using 4-0 continuous vicryl or PDS (in radiotherapy cases) suture over 6–7 Fr Bander stents. A catheter which acts as a sump drain is left in the ileal conduit which is removed along with the stents typically at days 10–14.
For an orthotopic bladder procedure, a longer segment (50 cm) of the intestine is reshaped into a Studer pouch with a 10 cm chimney to which the ureters are anastomosed. For cutaneous ureterostomy, a V-Y opening is made in the abdominal wall, and the ureters are fed through with the help of anchoring sutures. Ureters are then spatulated and a Wallace plate is fashioned, which is then sutured to the V-Y opening and ureteric stents are left in to facilitate drainage.
The bladder is extracted via a mini-Pfannenstiel incision or through extension of the camera port. In all cases, a pelvic drain is left in situ.
Postoperatively, patients typically spend a night in a high dependency unit before transferring to a surgical ward. Recovery includes stoma training, physiotherapy, and gradual oral intake as per the hospital’s protocols, in accordance with established Enhanced Recovery After Surgery (ERAS) guidelines. Discharge occurs once patients are mobile, eating normally, and managing their stoma. Stents are typically removed at the 2/3-week follow-up with antibiotic cover. A loopogram is routinely performed at 3 months and further upper tract imaging at a year, or earlier if there are any clinical concerns.
We recorded the baseline demographics, diagnosis, length of stay, renal function, follow-up imaging and adverse events. Patients were stratified into radiation-related and non-radiation-related indication groups for comparative analysis. Statistical analyses were performed on anonymised data using R (Bell Laboratories) Comparative analyses between radiation-related and non-radiation-related groups were conducted using t-test, Fisher’s exact test, and Mann–Whitney U test as appropriate. A threshold of p < 0.05 was used to denote statistical significance.
This study involved retrospective analysis of routinely collected clinical data. The UK Medical Research Council (MRC) decision tool (https://www.hra-decisiontools.org.uk/research/) was used to determine whether the project met the criteria for research requiring NHS Research Ethics Committee (REC) review. The tool confirmed that the study constituted service evaluation and therefore did not require REC review or formal research ethical approval under the UK Policy Framework for Health and Social Care Research 2017 (Supplemental Files). The study used fully anonymised routinely collected data and involved no change to patient care; accordingly, individual informed consent was not required. All data handling complied with institutional governance standards and the principles of the Declaration of Helsinki.
The study is reported in accordance with the PROCESS (Preferred Reporting of Case Series in Surgery) guideline, which is specifically designed for surgical case series. 24
Results
Patient demographics
Of the 70 patients (40 males, 30 females) undergoing RAC, radiation cystitis was the most common indication. Table 1 summarises key demographics and is sub-divided into groups according to the indication for cystectomy. Radiation cystitis patients were older (p = 0.005), with no significant differences in gender (p = 0.15).
Patient demographics and breakdown of indications.
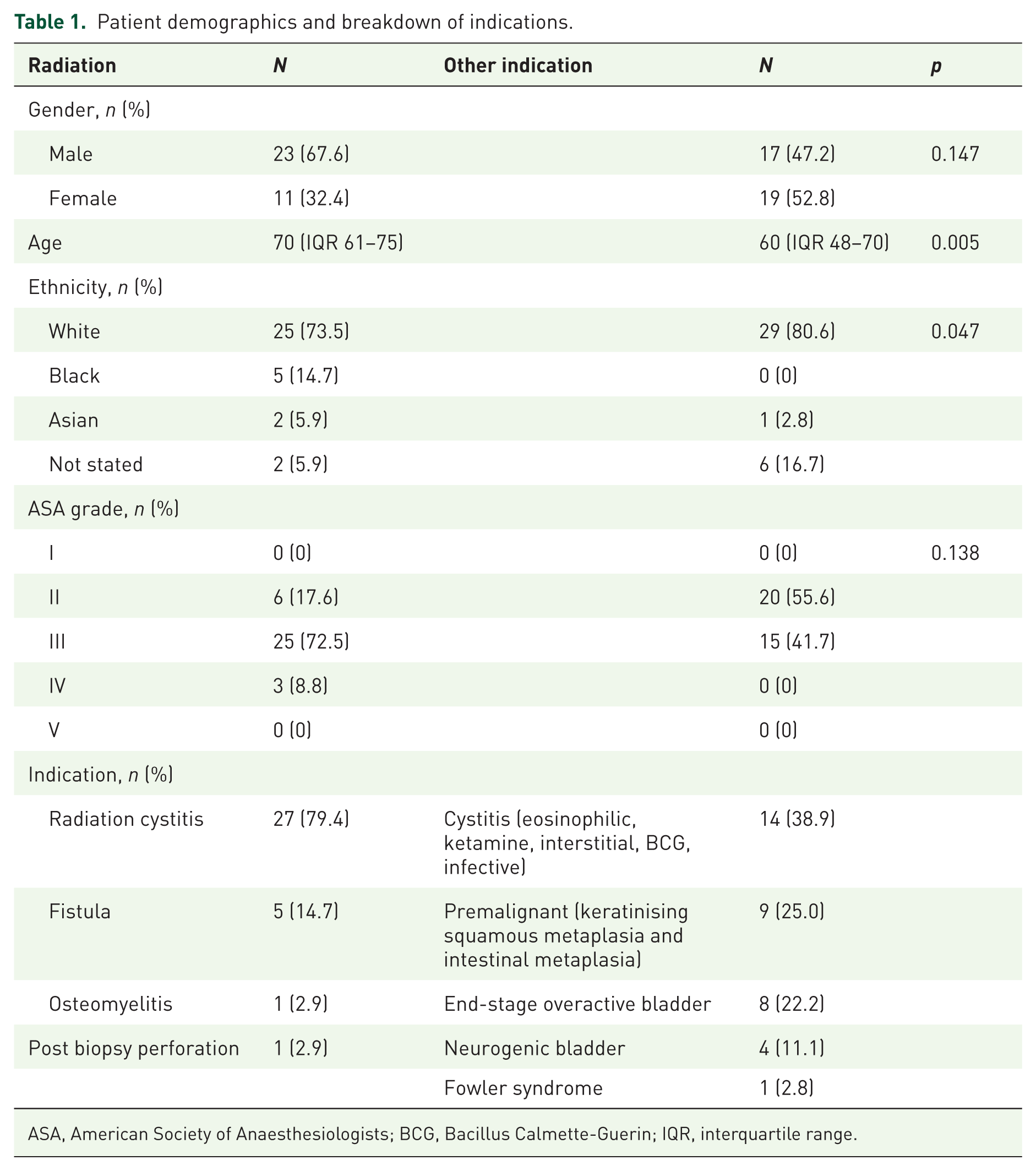
ASA, American Society of Anaesthesiologists; BCG, Bacillus Calmette-Guerin; IQR, interquartile range.
Thirty-five (50%) patients had previous radiotherapy. The most common indication for radiotherapy was treatment of prostate cancer (N = 22), followed by cervical cancer (N = 8). Of these, one patient did have radiotherapy; however, the indication for cystectomy was diffuse keratinising squamous metaplasia. Median Eastern Coooperative Oncology Group (ECOG) Performance Status was 1 in both radiotherapy and non-radiotherapy groups, while median American Society of Anaesthesiologists (ASA) grade was 3 in the radiotherapy and 2 in the non-radiotherapy group. Twelve patients had a nephrostomy or ureteric stent in situ for obstruction.
Intraoperative details and inpatient course
The average operating time was 334 min (range 180–540 min), with no differences between groups (p = 0.45). There were no unplanned conversions to open. Fifty-seven patients (81.43%) underwent intracorporeal ileal conduit formation, 7 (10%) had cutaneous ureterostomies, 5 (7.14%) had extracorporeal ileal conduit, and 1 (1.43%) had an orthotopic bladder substitution.
One intraoperative rectal injury (1.4%) occurred. This was a 1 cm rectal tear which was identified and repaired intraoperatively, with a defunctioning ileostomy performed. Another patient required hemicolectomy and defunctioning ileostomy as he was found to have ischaemic bowel following harvesting of the conduit.
Average blood loss was 326 ml (10–1250 ml), with no difference between groups (p = 0.46). A total of 14 patients (20%) required blood transfusion intra- or postoperatively; 10 of these were patients who had radiotherapy causing haematuria, with 4 in the non-radiotherapy group for anaemia from other causes. Median length of stay was 9 days (interquartile range (IQR) 8–17), with no significant difference between groups (p = 0.24). There were three outliers with a length of stay beyond 60 days.
Postoperative outcomes
There were 15 (21%) readmissions in the first 30 postoperative days (POD) – 7 patients presented with pelvic collections, 4 with sepsis without collection, 4 had acute kidney injury (AKI) and 1 presented with non-specific symptoms.
Mean follow-up was 16 months (range 1–58 months). There was no postoperative change in average glomerular filtration rate in either group (average change 1.37 ml/min/1.73 m2, range 36–43) at 1 year follow-up (Table 2). Follow-up imaging to rule out strictures was obtained for 59 (84.2%) patients within the first postoperative year – loopogram or computed tomography scan as appropriate. Of the 11 who did not have any imaging, 3 were deceased, 7 had cutaneous ureterostomies, and 1 was lost to follow-up.
Change in GFR.

GFR, glomerular filtration rate.
Complications
Postoperative 90-day complications were experienced by 46 patients (65.7%) as detailed in Table 3 according to the modified Clavien–Dindo classification. 25 There were no Clavien I; the majority (67%) were Clavien II, and we did not observe any bowel leaks in the study cohort.
Ninety-day postoperative complications according to Clavien–Dindo grading.

GA, general anaesthetic; LA, local anaesthetic; POD, postoperative day.
There were three Clavien V 90-day complications. These were high-risk (ASA3–4) patients who had salvage procedures for intractable bleeding due to radiation cystitis. No statistically significant differences were noted in complication rates between the two groups (p = 0.62).
Uretero-ileal stricture rate was 7% (five patients), requiring surgical management (robotic stricture excision and ureteric reimplantation) in two patients and long-term ureteric stenting in one. The remaining three patients were managed conservatively.
Six other patients underwent further surgical interventions during study follow-up. These include one conduit revision for stoma fistulation, one conversion from cutaneous ureterostomy to conduit, one exploration and washout of conduit. The remaining had procedures unrelated to their conduit (completion urethrectomy due to incidental malignant histology, nephrectomy for non-functioning kidney, prostate artery embolisation for ongoing bleeding from the prostatic remnant). All conduit revisions were performed within 12 months of the initial surgery.
Discussion
This study included 70 patients who underwent benign RAC, with radiation cystitis being the most common indication. Our case series adds to the body of evidence on the use of RAC for benign disease and, to our knowledge, is the largest published series on RAC for radiation cystitis, as well as the largest series where the intracorporeal approach was used for urinary diversion.
Benign RAC constituted just over 10% of the robot-assisted cystectomies carried out in the study period at our centre, in line with published figures from the United States. 1 Our complication rate was 66%, mostly Clavien <III, with similar results for the radiotherapy and non-radiotherapy groups. There were three deaths in high-risk patients who had salvage procedures for intractable bleeding secondary to radiation cystitis.
It is worth noting that our patient cohort, particularly the radiation group, poses significant surgical challenges: these patients often had intensive treatment for various malignancies including radiation with or without surgery and had undergone several other interventions for recurrent haematuria. 26 In this patient population, cystectomy is considered a last option. They are often treated semi-electively with salvage intent, often without adequate pre-operative optimisation due to time constraints. Intraoperatively, extensive adhesions, radiation-induced tissue changes, and dense scarring made dissection technically demanding.
Rectal injury is a recognised risk during cystectomy, particularly in patients with prior radiotherapy or multiple previous pelvic surgeries, where tissue planes are often obliterated. In our series, one rectal injury (1.4%) occurred, which was recognised intraoperatively and managed immediately. The authors believe that the robotic approach may offer some advantages in this setting due to improved visualisation, magnification, and precision during posterior dissection, particularly in a scarred pelvis. The enhanced visualisation provided by the robotic platform may facilitate identification of tissue planes and reduce traction-related injury. However, these cases remain technically challenging and rectal injury remains a recognised risk, particularly in salvage cystectomy; surgeons undertaking these procedures should be prepared to recognise and manage this complication intraoperatively.
Our results are comparable to the CORAL and iROC studies, two UK-based randomised clinical trials of radical cystectomy, regarding operative time, length of stay and complication rates – which were 334 min, 9 days and 66%. 27 The 90-day complication rate for the robotic arm of the CORAL trial was 55%, of which 63% were Clavien III or above, while the iROC trial reported complication rates of 62%, of which 27% were Clavien III or above. Mean operating time was 390 min for CORAL and not available for iROC, while the length of stay was 12 and 8 days, respectively. In our series, the robotic approach appeared to offer advantages similar to those reported in oncological series, including low intraoperative blood loss and rapid postoperative recovery, despite the complex nature of these benign cases.
An important consideration in this population is the choice of surgical approach. At our institution, the robotic approach has become the preferred technique for cystectomy, where technically feasible; however, careful patient selection remains essential. Factors influencing the decision between robotic and open cystectomy included prior radiotherapy, number of previous abdominal or pelvic surgeries, presence of fistulae, anticipated difficulty of pelvic dissection and need for concomitant procedures. In frail patients or those requiring a shorter operative time, a cutaneous ureterostomy was sometimes preferred over an ileal conduit, and in rare cases, an open approach may be considered.
In our series, all cases were completed robotically, reflecting both surgeon experience and institutional preference; however, this reflects careful case selection and should not be interpreted as suggesting that all benign cystectomies are suitable for a robotic approach. Patients with extensive prior surgery, very hostile abdomens, or where rapid access was required may be better suited to an open approach. Ultimately, the choice of approach should be individualised, accounting for patient factors, disease complexity, and surgeon experience.
Looking at comparable literature in the benign population, existing literature on cystectomy and urinary diversion for benign conditions is limited and summarised in Table 4. Although the robotic approach is commonly used for cystectomy in oncological cases, to our knowledge, only 11 papers have been published on robotic benign cystectomy. The most common indication for RAC was neurogenic bladder dysfunction in seven papers, radiation cystitis in two and interstitial cystitis and mixed urinary tract dysfunction in one report each. A series comparing open, laparoscopic, and robotic cystectomy for neurogenic bladder found similar rates of blood loss; our median operating time was lower, but the overall complication rate was marginally worse (60% vs 66%). 15
Summary of existing literature on benign RAC.

Complications are given for overall series of 252 patients undergoing cystectomy, of which the majority were for cancer and only 14 for benign indications.
Bold was used to highlight that our own report was in the table.
EC IC, extracorporeal ileal conduit; IC IC, intracorporeal ileal conduit; RAC, robot-assisted cystectomy.
There is considerable variability in the reported complication rates across studies evaluating benign RAC, likely reflecting the diverse and often complex patient populations included, and overall, fewer patients. The major complication rate (Clavien III or above) ranges from 0% to 37%. Similarly, overall 90-day complication rates are highly heterogeneous, with our study reporting a complication rate at the higher end of this spectrum (67%), which may be attributed to the challenging nature of the cases included. The persistence of high-grade complications in this benign cohort likely reflects the complexity of the cases, including extensive prior radiation, adhesions, tissue fragility, and the salvage nature of many procedures. Rates of conversion to open are overall low due to careful case selection and surgeon experience.
Readmission and reintervention rates, where reported, were comparable to our findings. Piazza et al. noted a 30-day readmission rate of 22% and a reintervention rate of 15%, while our study reported similar readmission (21%) and reintervention (11%) rates, primarily due to AKI and sepsis. Overall, the relatively small cohort sizes in most studies, with several reporting fewer than 50 patients, limit the ability to draw definitive conclusions and highlight the need for larger, multicentre, prospective studies to better characterise outcomes. In addition to patient-related factors, surgeon experience and the learning curve associated with robotic cystectomy may also influence outcomes and should be considered when interpreting these results.
The involvement of multiple surgeons at different stages of their robotic learning curve represents a potential limitation of this study but also reflects real-world practice in a high-volume functional urology unit. Importantly, all surgeons were already experienced open pelvic surgeons and were familiar with cystectomy and urinary diversion prior to transitioning to a robotic approach. The learning curve, therefore, is related primarily to the robotic platform rather than to the procedure itself. At our institution, robotic experience was developed in a stepwise manner under proctorship, and for the non-cancer surgeons beginning with less complex reconstructive procedures such as colposuspension and ureteric reimplantation before progressing to cystectomy and intracorporeal diversion. This structured transition likely mitigated the impact of the robotic learning curve on perioperative outcomes.
Although we did not formally analyse outcomes by surgeon experience or case sequence, we did not observe an obvious increase in complications in early cases, and overall outcomes remained comparable to published oncological robotic cystectomy series. These findings suggest that, in centres with established open cystectomy experience and a structured transition to robotics, benign robotic cystectomy can be introduced safely. However, these cases remain technically demanding, particularly in previously operated patients, and should be undertaken in high-volume centres with appropriate robotic and reconstructive expertise.
Strengths of this study include our setting as a high-volume centre with extensive expertise of RAC for oncological indications, and the availability of detailed patient records from a prospectively maintained database. Limitations include the heterogeneity of our patient population, with low numbers for individual indications, and a relatively limited length of follow-up. Additionally, we note its single-centre, retrospective nature and involvement of several surgeons at differing levels of their learning curve (although this will often reflect real-world practice in a busy urology unit). We also acknowledge the potential for selection bias in patient inclusion and the limitations inherent to single-centre studies, which may affect generalisability of our findings.
Conclusion
Robot-assisted approach is a good alternative to open cystectomy for benign bladder disease, as it offers the advantages of minimally invasive surgery in this complex group of patients. The data would suggest outcomes and adverse events are comparable to the literature in malignant disease. Previous radiotherapy did not seem to impact outcomes.
Management of these cases is very resource-intensive and usually requires multi-disciplinary input and a high level of surgical expertise, and therefore, best managed in high-volume centres. Further, larger, prospective, multicentre studies are needed.
Supplemental Material
sj-docx-1-tau-10.1177_17562872261451298 – Supplemental material for Robot-assisted simple cystectomy for benign disease with medium-term follow-up: a case series
Supplemental material, sj-docx-1-tau-10.1177_17562872261451298 for Robot-assisted simple cystectomy for benign disease with medium-term follow-up: a case series by Martina Spazzapan, Jonathan Kam, Ellen Benn, Basil Lutfi, Samuel Folkard, Marc Alain Furrer, Sachin Malde, Ramesh Thurairaja, Rajesh Nair, Prokar Dasgupta, Arun Sahai and Muhammad Shamim Khan in Therapeutic Advances in Urology
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.