
Abstract
Aims:
Alongside the increasing prevalence of chronic health conditions such as cardiovascular disease and diabetes has been an increase in interventions to reverse these ill-health trends. The aim of this study was to examine the longitudinal impact of the Sheffield Hallam University Staff Wellness Service on health indicators over a five-year period.
Methods:
The Sheffield Hallam Staff Wellness Service was advertised to university employees. Of 2651 employees who have attended the service, 427 respondents (male = 162, female = 265) aged 49.86 ± 12.26 years attended for five years (4 years follow-up). Each year, participants were assessed on a range of health measures (i.e. cardio-respiratory fitness, body mass index, blood pressure, total cholesterol, high-density lipoproteins, lung function and percentage body fat). Participants also received lifestyle advice (based on motivational interviewing) as part of the intervention to either improve, or in some cases maintain, their current health behaviours (e.g. increased physical activity and diet change).
Results:
The wellness service improved staff health for those with an ‘at risk’ health profile from baseline. These improvements were maintained in subsequent follow-up assessments. Improvement from baseline to 1-year follow-up was observed for all health indicators as was the maintenance of this improvement in years 2, 3 and 4.
Conclusions:
The service demonstrates that a university-based wellness service using a combination of motivational interviewing and health screening to elicit behaviour change (and subsequent improvements in health-related outcomes) was successful in improving the health of employees with an ‘at risk’ profile.
Introduction
Most individuals, in particular men, spend two-thirds of their waking hours at work.1,2 There are many benefits of being employed such as improving identity, social status, health and economic wellbeing, and moreover, unemployment has significant and adverse health consequences.3,4 It is also recognised across international charters and declarations5–7 that the workplace is an appropriate setting for engendering health and wellbeing, which also contributes to the corporate social responsibility agenda as well as enhancing recruitment and retention of staff. The organisational culture of a workplace has been highlighted as a barrier to the adoption of healthy behaviours in the workplace. Efforts to intervene and increase employer responsibility for employees’ health have been observed. For example, in the United States, according to the Patient Protection and Affordable Care Act (ACA), 8 employers must, by law, invest in the health of their employees. To date, there is no such law in the United Kingdom which might be the reason for the paucity of workplace physical activity interventions compared with the United States. However, efforts to address this in the United Kingdom appear to be emerging. For example, the National Institute for Clinical Excellence (NICE) 9 recently released best practice guidelines for organisations to support healthy employee behaviour, as well as the NICE 10 guidelines for encouraging physical activity in the workplace.
Beyond this, there is considerable evidence of the link between employee health and enhanced work productivity and effectiveness.11–13 The healthiest quarter of the workforce is shown to be happier, less prone to illness and 18% more productive than the least healthy quarter. 14 Nevertheless, the health of the workforce (as a reflection of the UK population more generally) is in decline. This decline is largely being driven by an increase in non-communicable disease (e.g. cardiovascular disease, diabetes, obesity, arthritis, cancer and depression) underpinned by unhealthy lifestyle behaviours of which physical inactivity is a major cause.15,16
Much of the inactivity burden can be attributed to a technological revolution which, while bringing great benefit such as abundant modes of communication and transportation, has also resulted in a significant cost to society through a burden of non-communicable disease. 17 Within the workplace, the proliferation of computer-based technology means that many jobs require employees to be sedentary for prolonged periods of time. 18 For example, Thorp et al. 19 reported that office-based employees in industrialised countries such as the United Kingdom, the United States and Australia are sedentary for more than 75% of their working day (6–7 h). A total of 175 million working days, equating to 3.3% of total working time, are lost due to sickness absence per annum, which is reported to cost employers £14.4 billion. 20 Furthermore, poor health impairs economic productivity (presenteeism: that is, attending work while sick, effecting productivity) even when it does not lead to immediate absence, with the impact of presenteeism likely to be up to seven times greater than absenteeism. 20 It is unsurprising, therefore, that there have been calls for interventions that can reduce absence and improve productivity in the workplace, 21 the aim of which is often to either prevent disease onset or to diagnose and treat health concerns prior to experiencing complications (primary and secondary preventions, respectively).22,23
Like many occupations, the physical and psychological health of university employees requires attention given the increasing reports of ill health at work, often from work-related conditions (e.g. stress). 24 It has been reported that levels of psychological distress among academics in UK universities have remained consistent and continue to be greater in universities than other workforces and in comparison to the general level measured in the UK population. 25 Moreover, Kinman and Jones 26 reported that psychological distress among UK academics is higher compared with academics in other countries. There are gender differences for the causes of stress reported by UK university academics, for example, men have a higher level of vulnerability to stress caused by pay and benefits. 27 Stress related to pay and benefits may be relevant to university lecturers with previous reports that lecturers’ wages have increased by only 5% compared with 45% for the rest of the economy. 28
Nevertheless, it is encouraging that poor health at work can be managed and reduced, particularly via physical activity, 29 and the workplace is an ideal setting with an estimated 60% of the world’s population accessible directly or indirectly through the workplace. 21 Data from controlled and un-controlled studies reveal significant positive changes in alcohol consumption, nutrition, sleep, stress, body mass index (BMI), depression and perception of general health,12,29 including some long-term improvements in body mass, waist circumference, blood pressure and lipid profiles compared to controls. 30 Nevertheless, most interventions report that improvements dissipate after 12 months, 31 leaving a paucity of interventions that demonstrate a lasting effect. 32
A number of reasons exist for the ineffectiveness of programmes offered, including employer buy in, employee motivation and time due to the demands of the workplace.33,34 Thus, interventions that counter the pitfalls of previous ineffective interventions are required. The primary aim of this research was to develop and test a workplace health and wellbeing service in university staff to improve health indicators. In line with extant literature, 30 it was hypothesised that workplace health and wellbeing service would improve the health status of university employees.
Methods
Participants
Sheffield Hallam University (SHU) is a large UK University with 4,494 staff, employed in a range of occupations including administration, finance, hospitality, lecturer, maintenance, professional services, research and technical services. The level of staff attending the service varied in seniority. To support staff health and wellbeing, a service (SHU Wellness) was developed and has been delivered at the University for 8 years. For the past 5 years, data were collected on the SHU Wellness service. To recruit participants, the service was advertised via email, newsletter and attached flyers to staff pay slips across the university to employees. Overall, 2651 employees of the university have attended the service in the last 5 years of which 427 respondents (male = 162, female = 265) aged 49.86 ± 12.26 years have attended follow-ups for four years (see Table 1). Employees were eligible to take part in the wellness service if they were contracted (full- or part-time). The health of the majority of staff at baseline was normal; however, there were participants who were overweight or obese, had borderline or high systolic blood pressure and diastolic blood pressure, borderline or undesirable levels of total cholesterol, and undesirable levels of high-density lipoprotein (HDL) (see Table 1).
Health indicators measured over four years among University employees aged 18–73 years in 2009–2013 (mean and standard deviation)
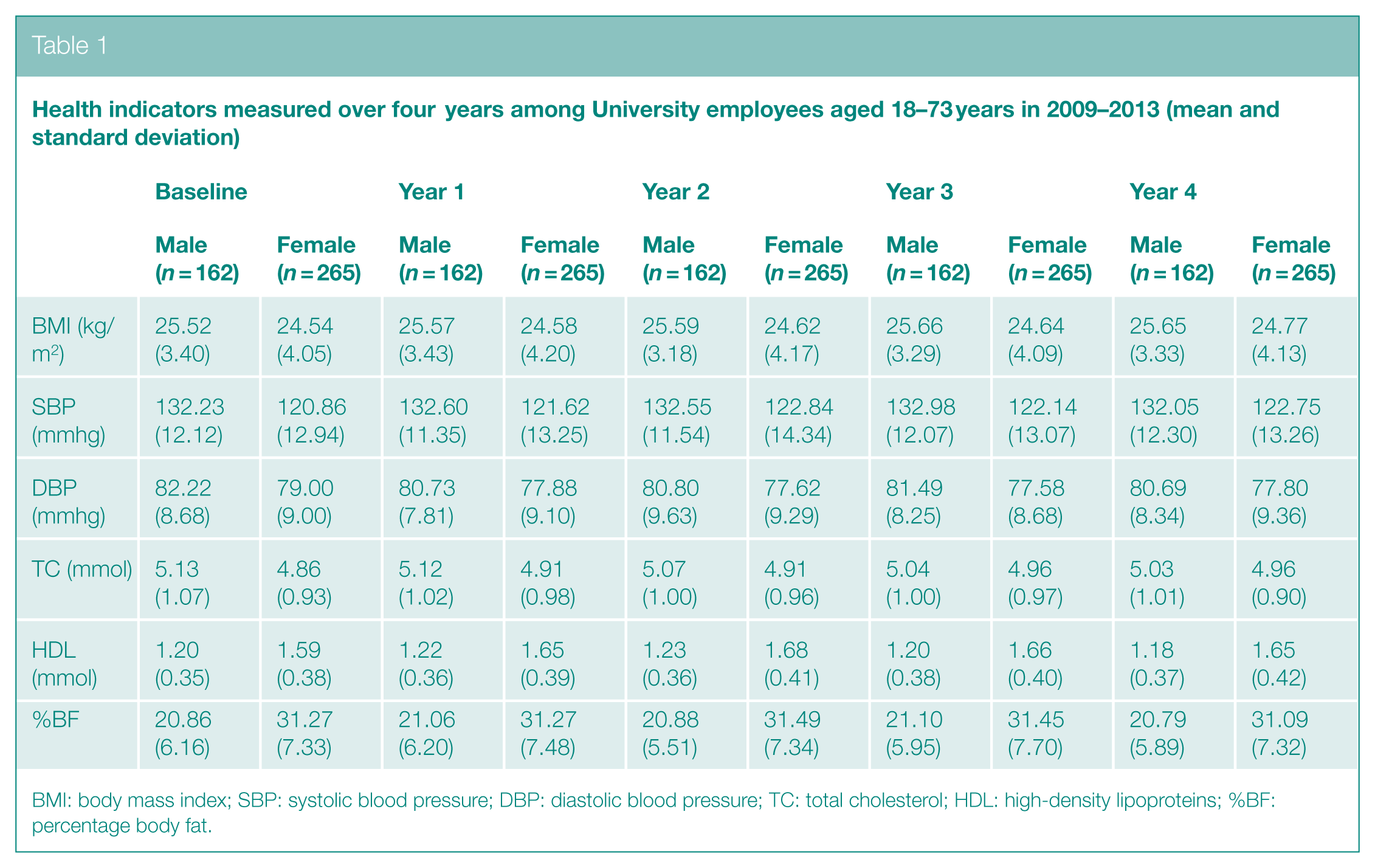
BMI: body mass index; SBP: systolic blood pressure; DBP: diastolic blood pressure; TC: total cholesterol; HDL: high-density lipoproteins; %BF: percentage body fat.
Measures and procedures
Following institutional ethics approval, all 427 attended and consented to participate in the service. After consenting to the study, participants were invited to attend the wellness service for a consultation. During the consultation, and every year for 4 years thereafter, participants were assessed on health screen measures: BMI was calculated as weight (kg)/height (m)2; blood pressure was measured using an automated sphygmomanometer; blood cholesterol (total cholesterol and HDL) and percentage body fat were measured using bioelectrical impedance. After assessment of the above health indicators, participants also received person-centred lifestyle advice (based on motivational interviewing) 35 to either improve or, where necessary, maintain their current health status to elicit and strengthen lifestyle modification. All advisors were trained in motivational interviewing to promote behaviour change with experience of delivering health assessments and lifestyle advice in a workplace health promotion setting. Advisors recorded their sessions and received feedback on the content and style of delivery by a member of the Motivational Interviewing Network of Trainers 36 to ensure treatment fidelity was maintained throughout the service.
In addition to the consultation, the service also included individualised health checks, lifestyle management advice and educational workshops on topics including physical activity, healthy eating, mental wellbeing and resilience. Employees were welcome to attend these workshops to supplement their understanding of health and wellbeing and had the option of reduced memberships for the university gym.
Data analysis
Repeated measures one-way analyses of variance (ANOVAs) with Bonferroni correction for confidence interval adjustment and follow-up post hoc tests with Scheffé correction were used to compare heath indicators across the 5 years of data collection. Alpha was set at .05 for all tests.
Results
On analysis of the 427 participants, irrespective of their initial health status (see Table 1), data suggested that the service had a beneficial impact in improving a range of health indicators (e.g. systolic blood pressure is on the cusp of significance). Despite this improvement, only diastolic blood pressure significantly improved from baseline to follow-up. Repeated measures ANOVA revealed that diastolic blood pressure was lower in all four follow-up assessments in comparison to the baseline measurement (F(4, 1,700) = 5.08, p < .01). No significant difference was found for BMI, systolic blood pressure, total cholesterol, HDL or percentage body fat across the five time points. An interaction effect was evident between cholesterol and gender, where male’s cholesterol decreased while female’s cholesterol increased (F(4, 1,700) = 3.22, p < .05). When participants who were initially measured as having a health status within the ideal ranges were not included, thus, the analysis only considered those in the non-ideal ranges (see Tables 2 and 3), and all of the health indicators improved significantly from baseline to follow-up 1.
Health indicators measured over four years among university employees aged 18–73 years in 2009–2013 with an ‘at risk’ profile at baseline (mean and standard deviation)
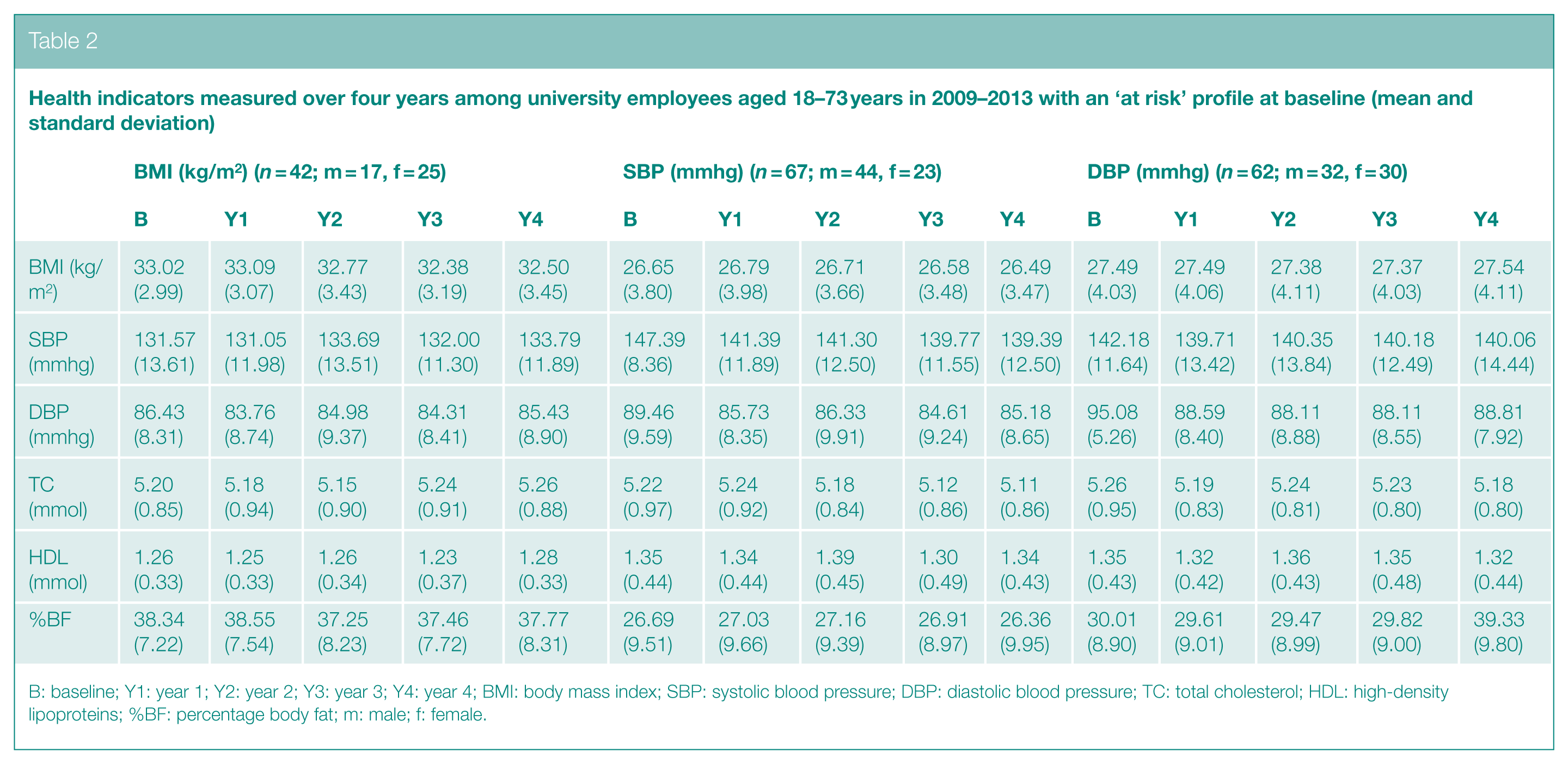
B: baseline; Y1: year 1; Y2: year 2; Y3: year 3; Y4: year 4; BMI: body mass index; SBP: systolic blood pressure; DBP: diastolic blood pressure; TC: total cholesterol; HDL: high-density lipoproteins; %BF: percentage body fat; m: male; f: female.
Health indicators measured over four years among university employees aged 18–73 years in 2009–2013 with an ‘at risk’ profile at baseline (mean and standard deviation)
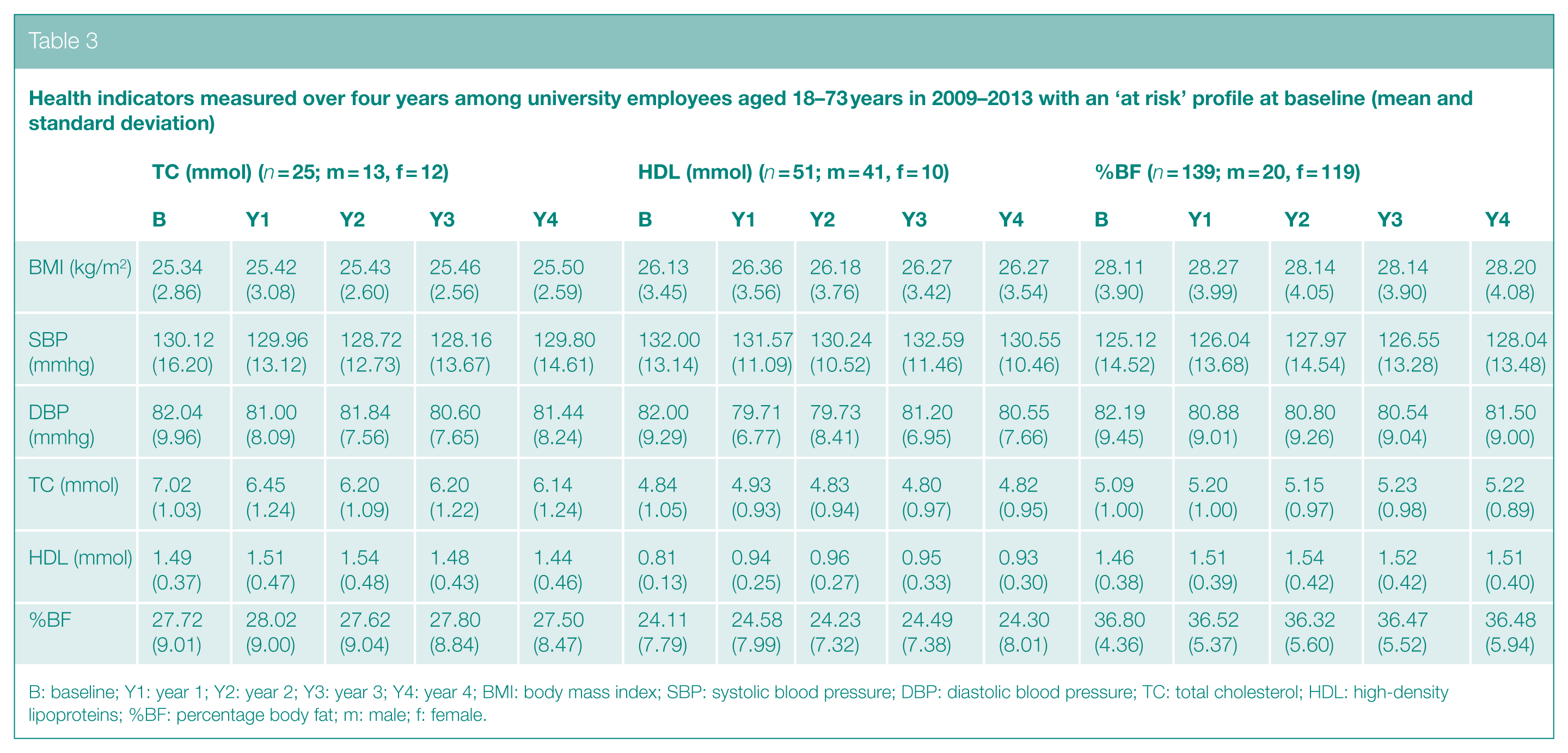
B: baseline; Y1: year 1; Y2: year 2; Y3: year 3; Y4: year 4; BMI: body mass index; SBP: systolic blood pressure; DBP: diastolic blood pressure; TC: total cholesterol; HDL: high-density lipoproteins; %BF: percentage body fat; m: male; f: female.
BMI
Significant differences were identified for participants with a BMI of 30 kg/m2 or greater at baseline, in relation to body fat percentage (F(4, 164) = 2.57, p < .01). No differences were identified between follow-up time points (p > .05).
Hypertension (systolic blood pressure)
Significant differences were identified for participants with systolic blood pressure of >140 mmhg at baseline, in relation to systolic blood pressure and diastolic blood pressure (F(4, 264) = 9.22, p < .01, F(4, 552) = 7.45, p < .01, respectively). Follow-up tests identified significant differences between baseline and all four years of follow-up, where systolic blood pressure and diastolic blood pressure improved between baseline and follow-up 1 (p < .01 respectively). Improved systolic and diastolic blood pressure was maintained from follow-up 1 to 1up 2, 3 and 4 with no differences identified between follow-up time points (p > .05).
Hypertension (diastolic blood pressure)
A significant main effect was identified for participants with diastolic blood pressure of >90 mmhg at baseline, on measures of diastolic blood pressure (F(4, 244) = 19.14, p < .01). Follow-up tests identified significant differences between baseline and all four years of follow-up, where diastolic blood pressure improved (p < .01 respectively). No significant differences were identified between follow-up 1 and follow-up 2, 3 and 4 for diastolic blood pressure, suggesting participants maintained their improved status over time (p < .05).
Cholesterol (total cholesterol)
Significant differences were identified for participants with total cholesterol of >6.5 mmol/L at baseline, in relation to total cholesterol and HDL (F(4, 96) = 7.69, p < .01, respectively). Follow-up tests identified significant differences between baseline and all four years of follow-up (p < .05). Total cholesterol improved from baseline to follow-up 1 and was maintained with no differences identified between follow-up 1 and follow-up 2, 3 and 4 (p > .05).
Cholesterol (HDL)
Significant differences were identified for participants with HDL of <1 mmol/L at baseline, in relation to HDL (F(4, 200) = 5.94, p < .01). Follow-up tests identified significant differences between baseline and all 4 years of follow-up, where HDL improved from baseline to follow-up 1 and was maintained with no differences between follow-up 1 and follow-up 2, 3 and 4. While a main effect was identified for systolic blood pressure, follow-up tests revealed no differences between time points (p > .05).
Percentage body fat
Significant differences were identified for participants with a percentage body fat in the poor range for males or females in line with Jackson and Pollock (1978) at baseline,37 in relation to systolic blood pressure and HDL (F(4, 552) = 3.38, p < 01, F(4, 552) = 2.96, p < .05 respectively). Despite these main effects, follow-up tests revealed no significant differences systolic blood pressure (p > .05). Follow-up tests revealed that HDL improved from baseline to follow-up 2 (p < .05).
Discussion
Similar to previous research, 38 the findings of the service suggest that the SHU Wellness service has had a significant impact in improving health indicators over a five-year period. Initial data analysis suggests that while trends towards significance are evident, staff health is not improved over time. Nevertheless, while re-examining the data, it became evident that many of the participants had a profile within the ideal range for the health indicators measured. For many participants, their current health status was maintained rather than improved. Consequently, secondary data analysis including only participants with health indicators in the ‘at risk’ ranges for the health indicators was examined. Beneficial impacts of the service were observed where a number of health indicators improved from baseline to follow-up 1 and were maintained between follow-up 1 and follow-up 2, 3 and 4. Importantly, the service demonstrates that not only is the service beneficial in improving staff health in the short term (i.e. over a 12-month period), but that participants maintained their improved health status. Thus, the data suggest that the SHU Wellness service has a long-term impact on staff health.
Calls for workplace wellness programmes have been evident for decades, and this has increased alongside the prevalence of physical and mental health concerns.18,32 The effectiveness of these interventions to improve health has been mixed with many ineffective interventions attributed to factors such as insufficient time and a lack of employer buy in.29,30 Furthermore, the benefits observed previously have been relatively short term, and thus, long-term maintenance of improved health status has been lacking. The findings, however, show promise, with participants maintaining their improved health status. These findings demonstrating improvements in health indicators are similar to the conclusions drawn by Plotnikoff et al. 32 and Tytherleigh et al. 24 that behaviour change interventions targeting tertiary education staff can be effective and may provide an ideal platform for innovative programmes. Thus, as Haines et al. 39 suggested, innovative interventions such as the SHU Wellness service that stimulate physical activity and wellness offer one method of improving employee health and wellbeing, and may consequently increase return on investment through reduction of presenteeism and absenteeism for the employer and healthcare costs for the individual.
The overall findings of the service may be relatively unsurprising, as the health status of individuals working in universities might be expected to be better than the national average, and that of National Health Service (NHS) staff, due to greater flexibility due to their line of work and the opportunities to engage in healthy behaviours. Additionally, the university environment, while likely to target many employees due to the large-scale nature of this business, may not reflect that of other workplaces. The values and ethos of a university environment, which promotes healthy living and has a more flexible approach, may not therefore be replicated in other businesses, and therefore, the maintenance of improved health as observed in the service may not be observed outside of this context. Nevertheless, the secondary analysis including only employees with a health status that might better reflect that of other workforces provides promising findings to suggest that the SHU Wellness service may be effective in non-university settings. Thus, the initial improvement and maintenance of health indicator scores within an improved range is noteworthy and may have implications for other workplace settings. Blake and Lloyd 30 discuss the need for socially responsible organisations to take the lead on workplace wellness services that target unhealthy lifestyle choices and that these services may be a useful starting point for interventions in the NHS where reports of ill health among staff have increased. Thus, the SHU Wellness service represents an attempt at accepting organisational responsibility for workplace wellness. Future examination of the benefits of implementing the SHU Wellness service in other settings such as healthcare will identify whether the service is setting specific, or whether the promising findings translate to the other settings.
It is pertinent to note the potential limitations of this study. First, while the study findings provide indications of the impact of the wellness scheme, further analysis examining the most at risk participants based on baseline scores of health indicator scores means that the sample size is reduced. Nevertheless, the findings indicate the positive effects of the wellness scheme and thus the potential improvement for employees. Additionally, while over half of the total staff at the university have attended the SHU Wellness service, the proportion that have attended for 5 years and thus are included in this article is small in comparison. It is anticipated that over time, the impact of the service across a greater proportion of the staff in the workplace will be evident with current initiatives in place such as agreements for staff to attend and participate in the service while in work, rather than in breaks or after work. Furthermore, there has been greater publicity of the service through university emails, pay sheets and newsletters. Consequently, an increased employee engagement with the service has been observed over time. Second, while the findings are positive with improvements in participants’ health indicators, we are unable to conclude comprehensively whether the improvements were due to the combined impact of the service or specific elements. For example, the improvements may be due to the combined, motivational interviewing or awareness raising elements of the service. Thus, future work in this area should examine the impact of motivational interviewing in enhancing lifestyle behaviour change. Third, while prescribed medication was recorded, this was not included in the analysis and might have influenced the findings (i.e. health indicator changes might have been due to medication). Finally, the sampling strategy employed in this service may have led to bias in those recruited, where those sampled may already have had a strong desire to improve their health or engaged in behaviours commensurate with health improvement. Thus, this may have impacted the success observed in improving some of the health indicators measured. It might be likely, therefore, that university staff and thus those recruited for this study might be biased due to the healthy worker effect. 40
Conclusion
In conclusion, this service demonstrates the beneficial impact of the SHU Wellness service in improving and maintaining staff health for employees whose health indicators are in the high-risk categories. The findings suggest that SHU Wellness supports the maintenance of good health and is most beneficial to individuals in the ‘at risk’ range for the health indicators measured. This primary prevention workplace wellness scheme based on assessment of health indicators and advice using motivational interviewing to elicit behaviour change has been successful and, unlike many previous interventions, has led to maintenance of improved health status.
Practical implications
The SHU Wellness service is effective in improving health indicators.
The findings add to a growing area of research that is warranted given the increasing prevalence of health conditions linked to physical inactivity.
The findings contribute to a growing appreciation of the role that the workplace can have in improving the health of employees.
Footnotes
Acknowledgements
We would like to acknowledge the efforts of Simon Till, Hanna Leahy and Lindsey Reece in supporting the service.
Conflict of interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.