
Abstract
Introduction
The purpose of this review was to systematically evaluate the best available evidence for the conservative management of children and adolescents diagnosed with camptodactyly and propose recommendations to guide clinical practice.
Methods
A search of six electronic databases and manual searches were carried out in January 2014. The search strategy aimed to identify any published clinical practice guidelines as well as articles on the conservative management of camptodactyly for children and adolescents. Included articles were appraised using the McMaster Critical Review Forms for quantitative studies and assigned a level of evidence according to the National Health and Medical Research Council guidelines.
Results
No published clinical practice guidelines were located; however, five quantitative articles met the inclusion criteria from the 31 articles identified. The evidence from all included studies was classified according to the National Health and Medical Research Council guidelines as level IV, pre–post study design. All were retrospective. Included studies demonstrate clinically significant changes in passive joint range of motion following conservative treatment protocols. The results of the literature review, combined with clinical experience, were used to develop recommendations to guide clinical practice in the conservative management of children and adolescents with camptodactyly.
Discussion
The effectiveness of conservative therapy for camptodactyly is promising but evidence remains weak. More rigorous research is needed and the proposed recommendations could be used to inform future research for the conservative treatment of camptodactyly in children and adolescents.
Background
Camptodactyly is a non-traumatic flexion deformity of the proximal interphalangeal joint (PIPJ) of one or several fingers. It is thought to affect less than 1% of the population 1 but the incidence is not consistently reported in the literature. Management of camptodactyly comprises a substantial portion of paediatric hand therapy practice.
The pathogenesis of and classification systems used to describe camptodactyly remain topics of debate in the literature. Some of the hypothesised causes of camptodactyly include tightness of the flexor digitorum superficialis (FDS) tendon, abnormal insertion of the lumbricals, an intrinsic minus fifth finger (metacarpal phalangeal hyperextension with PIPJ flexion) and volar skin shortage and a muscle imbalance between the flexor and extensor mechanisms.2–5
Intervention for camptodactyly includes both surgical and conservative management. Surgical techniques include capsular release, FDS lengthening, collateral ligament release, resection of the lumbricals, tendon transfer, osteotomies, arthrodesis and arthroplasties. 6 Surgical interventions tend not to be overly satisfactory.7–9 Adverse outcomes such as scarring and loss of active flexion have been reported in the literature by several authors.7–9 Some authors contend that surgery should be reserved for patients with more severe and progressive forms of the condition but only after conservative management has failed.4,7,10
Conservative interventions include stretching, splinting and casting. There is no consensus as to the most effective conservative treatment for camptodactyly. A Cochrane review by Katalinic et al. 11 on stretch for the treatment and prevention of contractures concluded that stretch interventions have little or no benefit in treating or preventing contractures of both neurological and non-neurological origin. There were however, only five paediatric studies included in the review, all including children with neurological conditions (Cerebral Palsy, Duchennes Muscular Dystrophy and Charcot-Marie-Tooth disease) and only one included children with contractures in the upper limb.
Whilst the findings of this high-quality Cochrane review should not be discounted, the review currently has limited scope to guide the development of evidence-based recommendations for children and adolescents diagnosed with camptodactyly currently undergoing ‘stretch’ as an intervention. Wallen and Stewart 12 do highlight, however, that the Cochrane review indicates the need for further research on the impact of stretch interventions in the management of contractures in the paediatric population, including those diagnosed with camptodactyly.
This literature review systematically evaluates the best available evidence regarding conservative management of children and adolescents diagnosed with camptodactyly. The resultant literature and evidence, along with clinical knowledge is used to propose recommendations to guide conservative management of camptodactyly, acknowledging that further research is required.
Methods
Inclusion and exclusion criteria.
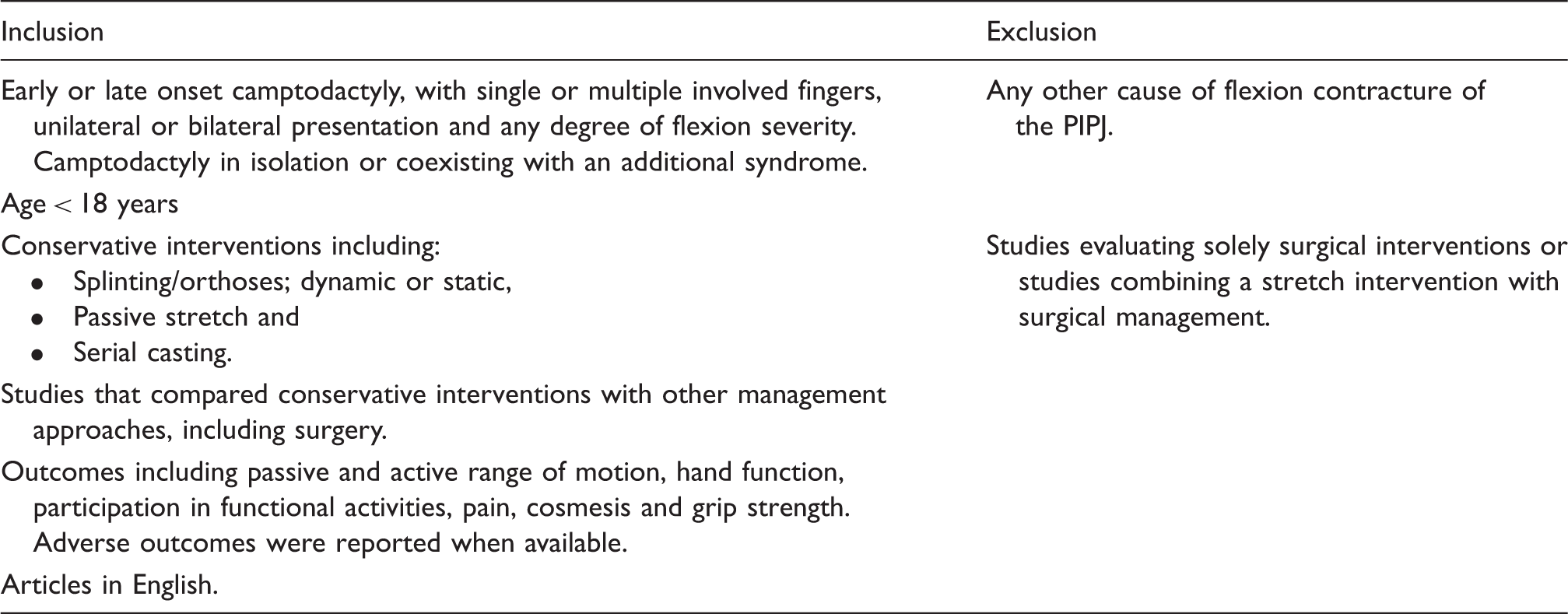
Study design and level of evidence of included studies.

Results
Using the search process, 31 potential articles were identified. The abstract of each article was reviewed by the authors, who then determined whether the article met the inclusion criteria. Five papers met the inclusion criteria.4,7–10 Included studies were of low methodological quality. All included studies used a retrospective, pre–post design and a convenience sampling method for participant selection. No included studies reported on the degree of blinding of assessors or participants. With the exception of Benson et al. 8 and Rhee et al., 9 it is unclear if the same practitioner collected data pre- and post intervention.
Functional implications
The impact of camptodactyly on upper limb function can vary between individuals.4,7 Hori et al. 10 reported minimal functional impact, while Siegert et al. 7 and Miura and Tamura 4 report functional problems including playing piano, typing, wearing gloves, writing and manual labour. The presence of pain 7 as well as dissatisfaction with the appearance of PIPJ contracture4,7 was identified in the literature as other reasons why treatment was sought.
Types of participants
Age ranges of participants from the included studies were from one month to 30 years. Participants had a range of diagnoses, from simple campatodactyly, affecting the little finger only, to complex, multi-digit involvement. The number of participants varied between studies, ranging from 13 to 62.
Classification system
Diagnostic imaging should be completed initially to exclude traumatic injury and to provide information on joint integrity as joint changes have been identified.4,10
There is a lack of consensus in the literature on the use of a single classification system to describe camptodactyly. The two classification systems described were author defined and varied between studies.7,9 Siegert et al. 7 described a two-tiered system: Simple – a flexion deformity of the PIPJ only; and Complex – where there is an associated deformity such as syndactyly or clinodactyly. Benson et al. 8 used three categories to classify camptodactyly: Type I (classic camptodactyly) – present in infancy, frequently confined to one or both little fingers (LF) with possible ring finger (RF) and middle finger (MF) involvement; Type II – shares similar characteristics to Type I but tends to present in adolescence and affects females more than males; and Type III – is a more severe form of the deformity with severe flexion contractures of multiple digits, associated with other syndromes (chromosomal disorders, craniofacial diseases and skeletal deformities). Other included studies did not outline the use of a classification system, but rather described participants as having either unilateral or bilateral small finger involvement only.4,10 Rhee et al. 9 utilised a combination of the classification systems described by Benson et al. 8 and Siegert et al. 7 to group study participants. The majority of appraised articles studied simple forms4,7,9,10 with only one study including participants with more complex forms of the condition. 8
There are several similarities between the classification systems used to describe camptodactyly in the appraised literature. There is agreement between all studies that camptodactyly varies in severity and ranges from unilateral or bilateral involvement of the little finger only,4,7–10 including one or two other fingers7–9 to more severe forms, often associated with other congenital anomalies.4,7,8 The condition may initially present in infancy or adolescence,4,7,8,10 with variability in the severity of the initial flexion contracture with severe contracture being less responsive to treatment.7–9
Types of interventions
Types of interventions and outcomes.
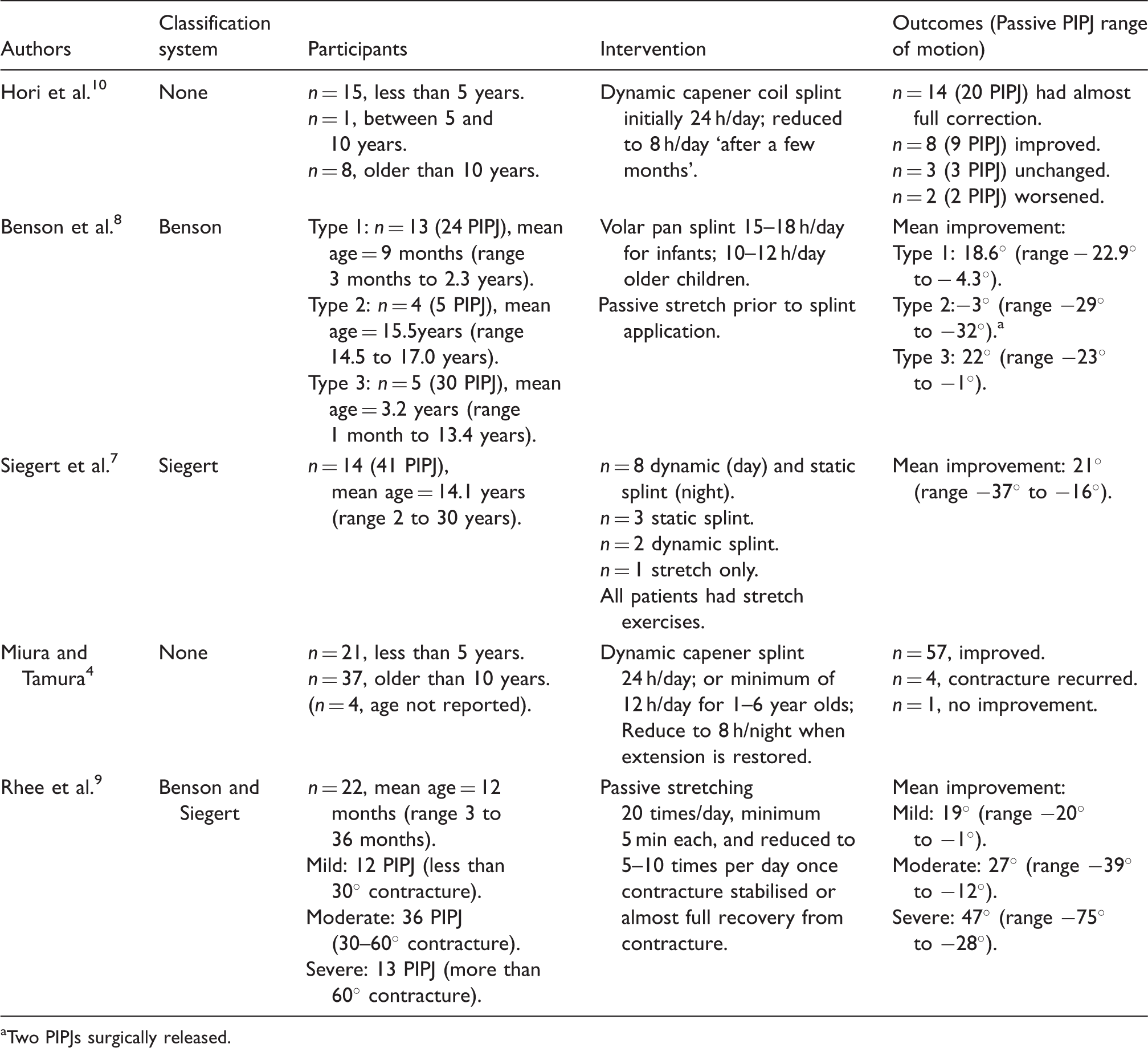
Two PIPJs surgically released.
Consideration should be given to using a volar hand/forearm based static splint, when multiple fingers are affected.7,8 Both dynamic capener and volar static splints should be modified to be forearm based for children less than six years of age to ensure it is safely secured to the child’s hand(s)4,8,10 to assist with keeping the splint in place 8 and minimise an infant’s risk of choking on a small splint. Dosage of therapy varied and included passive stretching for 5 min at least 20 times per day, to splinting for up to 24 h a day.4,9,10 Despite variability in treatment regime, four of the five authors agreed that the therapy dose can be reduced once almost full,9,10 or full4,8 passive ROM is obtained or the condition had stabilised.4,8–10
Three of five studies utilise daily stretch as a treatment modality either prior to splint application, 8 in conjunction with the splinting intervention 7 or as the treatment protocol. 9 With the exception of Rhee et al. 9 no specific details of the type or dosage of stretches were reported. Rhee et al. 9 described a stretch-only protocol for children of three years of age and younger with simple camptodactyly. While the stretch protocol was well described and results promising, it is a time intensive program (20 sessions of 5 min stretches per day) and the PIPJ stretch technique described where the wrist is extended and the metacarpophalangeal joint (MCPJ) hyperextended, is unconventional and no rationale was provided of its benefit over a more traditional technique. Further research is needed to determine the efficacy and safety of the stretch technique described by Rhee et al. 9
Outcome measures
All included studies used passive PIPJ range of motion as the primary outcome measure.4,7–10 There is a lack of consensus in the literature on a standardised assessment procedure for measuring passive range of motion of the PIPJ in children with camptodactyly. Rhee et al. 9 detailed the position of joints and use of a goniometer when collecting pre- and post-intervention data; however, details of the type of measurement tool used and the position of joints was lacking in other included studies.
Two studies attempted to measure active range of motion, but found it was difficult to measure reliably with young children and data was not reported.9,10 While the literature highlights difficulties obtaining AROM measurement in young children,8,10 it should be measured and documented where possible as passive range of motion may not necessarily translate into improvement in AROM of the PIPJ due to the presence of underlying anatomical variance.
None of the included studies reported any other outcomes. There was a wide range in follow-up times, both within and between studies (Table 3). Only Siegert et al. 7 described outcomes between participants who received either conservative management or surgical treatment; however, it was unclear how participants were allocated into treatment groups. Rhee et al. 9 provided statistical analysis of the magnitude of change in passive range of movement (PROM), while other authors reported average improvement of PROM pre- and post-intervention, but without statistical analysis. The follow-up period varied between studies and ranged from seven months to 20 years.
Outcomes of intervention
All included studies reported that conservative treatment improved the PROM of affected PIPJs in most cases. Table 3 highlights the reported changes in ROM.
Most authors agree that surgical intervention should be reserved for children and adolescents with a persistent, severe flexion contracture, who do not respond to conservative treatment.4,7,8,10 Adverse outcomes of conservative management were reported in two studies which included progression of the deformity; loss of flexion range; mild skin irritation and skin breakdown.7,10
Discussion
Overall, the use of conservative therapy to manage camptodactyly in paediatrics is promising but evidence remains weak. Included studies demonstrate clinically significant changes in passive joint range of motion following conservative treatment protocols. The majority of participants made gains in passive range of motion following conservative management, with a small number either unchanged or worse.
Authors used different classification systems to describe camptodactyly and there remains no consensus in the literature over which classification to use. Clinicians are encouraged to select and use one of the two identified classification systems in clinical practice to reflect the common clinical features present in camptodactyly, streamline communication between doctors and therapists and enhance the translation of research findings into practice.
Included participants ranged in age from newborn to adulthood and presented with differing levels of severity, with the majority of contractures involving simple camptodactyly, with either mild or severe contractures. There also exists a lack of details on the method of collecting pre and post passive and active range of motion data. Both active and passive range of motion should be collected as they may not improve concurrently and improvements in PROM alone may not be sufficient to address identified impairments in hand function.
Moreover, different types of interventions, at different doses and follow-up times make it difficult to compare outcomes across studies.
There remain many gaps in our knowledge related to the use of conservative therapy programs for camptodactyly in children and adolescents. Specific questions which warrant further research include:
When should splinting/stretching commence and cease? What is the best type of splint to use? How many hours a day should splints be worn for? What effect does passive stretch have on improving the flexion deformity of camptodactyly? What, if any, are the functional issues associated with camptodactyly? What, if any, specific exercise or therapy programs should be used to increase active PIPJ extension?
Limited use of activity and participation-based outcome measures in the literature limits our understanding of how, and indeed if, camptodactyly impacts on development and function over time. Additionally, it remains unclear as to whether conservative therapy improves child and adolescents functioning in daily activities. Pain, cosmesis and functional issues were identified as reasons for seeking treatment;7,10 however, outcome data addressing these reported issues following conservative treatment were not reported. McFarlane et al. 3 reports that less than 15° contracture does not cause any functional or cosmetic deficit.
There was no consensus as to when conservative treatment should be ceased. Some authors reported that conservative treatment which may involve ongoing active intervention, and/or monitoring, should continue until late teens or skeletal maturity due to the impact of growth on contracture recurrence; however, further research is required.4,7,8,10
Other features of conservative programs that may impact on outcomes include ongoing parental education, access to a skilled therapist for treatment and supervision and active parental and patient participation of which none have been well documented or researched to date.7–10
Evidence and information obtained from this literature review was synthesised and incorporated with clinical knowledge to develop recommendations to guide clinical practice.
These recommendations should be applied with caution and in conjunction with a high level of clinical knowledge due to the difficulty with comparing outcomes between studies.
The objectives of these recommendations are to:
provide guidance for uniformity in assessing and managing children and adolescents with camptodactyly; identify the need to use outcome measures in order to evaluate the effectiveness of treatment. This includes understanding the effect camptodactyly may have on a range of occupational performance areas such as self-care, leisure, play and development, school and social participation; provide a basis for conducting research into the effects of conservative management of camptodactyly.
Clinical recommendations
These recommendations aim to guide occupational therapists, physiotherapists and medical professionals in the conservative management of camptodactyly in children and adolescents aged 0–18 years.
Children and adolescents appropriate for conservative management include those with:
a diagnosis of simple or complex camptodactyly; bilateral, unilateral or multiple fingers affected; presence of other congenital upper limb co-morbidities.
These recommendations do not address PIPJ contracture associated with:
traumatic injuries of the PIP joint, i.e. volar plate injury and fractures; ulna nerve palsy; juvenile idiopathic arthritis; trigger finger; Kirner’s deformity.
Conservative treatment may involve a splinting or stretch program. A flowchart (Figure 1) has been developed to assist clinicians in implementing conservative therapy programs.
Flowchart to assist clinicians in implementing conservative therapy programs.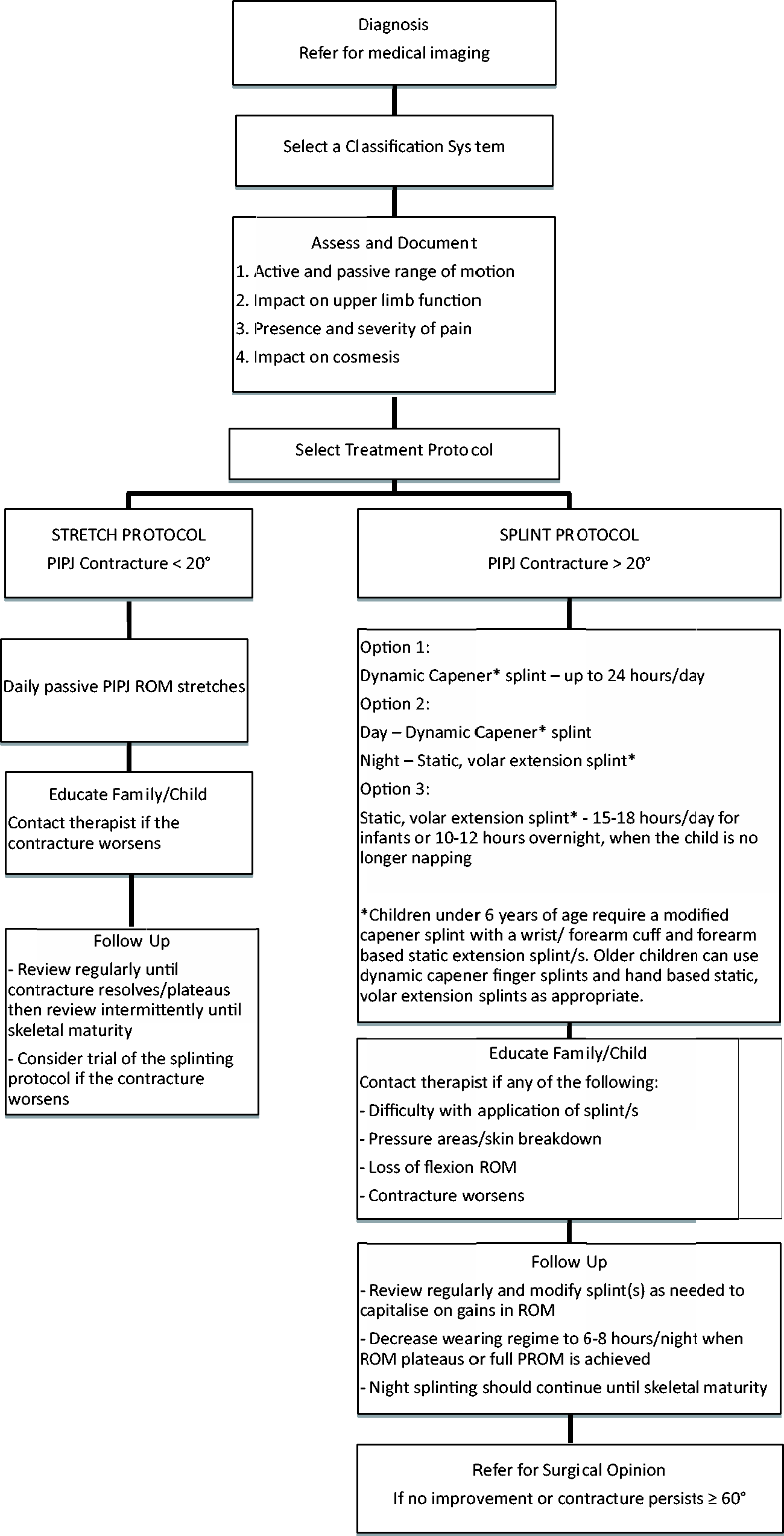
Assessment
Assessment of camptodactyly is multi-fold and includes selection of a classification system, imaging, measurement of passive and active range of motion and determining the impact on upper limb function, pain and cosmesis.
Recommendation 1: Confirm diagnosis
Medical imaging should be obtained for diagnostic purposes and to exclude other joint pathology, i.e. traumatic injury.4,10
Recommendation 2: Select a classification system
Classify and document camptodactyly using the classification system of either Seigert et al. 7 or Benson et al. 8
Recommendation 3: Identify impact on upper limb function
Assess the impact of PIPJ contracture on upper limb function.4,7,10
Recommendation 4: Determine the presence of pain
Because of the subjective nature of pain, self-report is considered the most reliable method to identify its presence. Use of an age appropriate pain scale to determine the presence and severity is recommended. 15
Recommendation 5: Identify concerns with cosmesis
Cosmetic concerns should be identified and documented.
Recommendation 6: Measure and document passive and active range of motion (ROM)
PROM8–10 and AROM8,10 should be measured using a goniometer. Clinicians should use a consistent measurement technique to enable outcomes to be documented reliably. Assessment of ROM of the PIPJ should take into account the impact that intrinsic and extrinsic structures have on PIPJ ROM. MCPJ extension will cause an intrinsic stretch while flexion of the MCPJs will relax the intrinsics. 16 Therefore, PIPJ ROM should be measured with the wrist in neutral and the MCPJs in both a neutral and flexed position. 9
Recommendation 7: Therapists should be skilled in splint fabrication
Therapists should be skilled and competent in fabricating hand splints and providing therapy to a paediatric population.7,8,10
Recommendation 8: Provision of education as a core component of intervention
The importance of providing families and children/adolescents with appropriate education has been highlighted in the literature.7–10 Parental education and where appropriate, child/adolescent education should be provided on:
Recommendation 9: Implementation of a passive (manual) stretch program for children and adolescents with < 20° PIPJ contracture
The use of splints is not recommended for the management of PIPJ contractures less than 20°.4,7–10 Rhee et al. 9 suggest stretches should be completed daily; however, there is currently no conclusive literature to direct the frequency and duration required for stretches. Clinical judgement should be applied. Consider implementing PROM stretches around the established routines of the family, for example, before or after nappy changes/feeds for younger children or meal times for older children, rather than at night during sleep, as recommended by Rhee et al. 9
Recommendation 10: Frequency of follow up for stretch programs should occur regularly then intermittently, until skeletal maturity
Monitoring of a stretch program should initially occur regularly. 9 Once the contracture has plateaued or resolved, intermittent reviews should occur until skeletal maturity due to the risk of contracture regression.4,7,8,10 If the contracture progresses, clinicians could trial a splinting program.
Recommendation 11: Implementation of a splinting program for children and adolescents with > 20° PIPJ contracture
The aim of splinting for camptodactyly is to provide a prolonged stretch to the affected PIPJ/s. The PIPJ/s should be positioned midway between the PIPJ resting position and maximum passive extension. 8
Splint options
Dynamic capener splint* only; worn up to 24 h per day, since flexion of the PIPJ is not restricted.4,7,10 Dynamic capener splint* during the day and a static volar, extension splint* at night.
7
Static, volar extension splint.7,8 The wearing regime should be a total of 15–18 h per day for babies and infants, reducing to overnight wear when the child is no longer napping.
8
*Children less than six years of age require a modified capener splint with a forearm based outrigger/wrist cuff4,10 and a forearm based static, volar extension splint.
8
A forearm based splint will ensure the splint is safely secured to the child’s hand/s;4,8,10 assist with keeping the splint in place
8
and minimise an infant’s risk of choking on a small splint. Older children can be fitted with finger-based dynamic capener style splints4,10 and hand-based static volar extension splints as appropriate.7,8
Recommendation 12: Intensity of splinting can be reduced when the condition has resolved or stabilised
Splinting programs can be reduced in intensity to a wearing time of between 6 and 8 h/day, where splints can be worn overnight once the condition has resolved or stabilised.4,10
Recommendation 13: Frequency of follow up for splint programs should occur regularly to capitalise on gains in ROM, then intermittently as required, until skeletal maturity
After initial provision, splint(s) need to be incrementally modified into further PIPJ extension to capitalise on gains in passive ROM.7,8 Once the frequency of splint wear has reduced to night only, intermittent reviews should occur until skeletal maturity due to the risk of contracture regression.4,7,8,10
Recommendation 14: Refer for surgical opinion if no improvement with conservative treatment and PIPJ contracture persists ≥ 60°
Refer for surgical opinion when children and adolescents have persistent PIPJ contractures ≥ 60° that have not responded to conservative treatment.4,7,8
Conclusions
There is a paucity of good-quality evidence to guide clinical practice for the conservative management of camptodactyly in children and adolescents. This position paper was developed based on appraisal and synthesis of the best available evidence, combined with clinical expertise and experience. These recommendations form the basis for clinical practice and may guide future research.
Footnotes
Acknowledgements
We would like to acknowledge the assistance of Dr Margaret Wallen, Occupational Therapist, The Children’s Hospital Westmead.
Conflict of interest
None declared.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.