
Abstract
Introduction
There is a lack of evidence on the best method for rehabilitating extensor tendon injuries in zones V and VI. The purpose of this study was to evaluate the outcomes of modified relative motion splinting compared with immobilization following repair of extensor tendons in zones V and VI.
Methods
A retrospective analysis compared the outcomes of relative motion splinting with immobilization. Sixteen patients (16 fingers) were treated by conventional immobilization splinting for four weeks (immobilization group) followed by mobilization with avoidance of ‘at-risk/heavy’ activities for a further 4–6 weeks. Twenty-three patients (23 fingers) were treated with the modified relative motion splint (mRMS group) during the day and a resting splint worn overnight for the first four weeks. The relative motion splint was continued for ‘at-risk/heavy’ activities for a further 4–6 weeks.
Results
The mRMS group demonstrated statistically significant improvement in range of motion compared with the immobilization group. This effect was most marked at six weeks (P = 0.0194, two-way mixed ANOVA) with the mRMS group achieving a 12% higher mean percentage total active motion (P = 0.0076, Mann-Whitney U test). Results were similar for both groups 12 weeks postoperatively. Differences in return to work times between groups were statistically significant (P = 0.0062, Mann-Whitney U test). Average return to work was 9.4 weeks for the immobilization group and 3.3 weeks for the mRMS group, equating to a 42 days earlier return to work for the mRMS group. There was no incidence of tendon rupture in either group.
Conclusion
This study demonstrates that modified relative motion splintage (finger based without wrist component) can be applied in the postoperative management of single zone V or VI extensor tendon repairs. The main advantages of this protocol, compared with immobilization include the small simple splint design, and straightforward patient instructions that enable earlier mobilization, functional hand use and return to both daily living and work.
Introduction
Extensor tendon injuries are common in zones V and VI due to their superficial location on the dorsum of the hand and minimal soft tissue protection. Historically postoperative management of these injuries has consisted of immobilization of the repair for 3–4 weeks. 1 This increases the risk of tendon adhesions, can delay return to work and limits daily activities of living, thereby adding to the burden of the injury. An ideal treatment regimen provides protection for the tendon repair, is simple and easy to apply and avoids these risks. No treatment regimen currently within the literature meets this ideal.
Early mobilization protocols were developed in an effort to minimize the complications of immobilization by applying controlled stress to a repair and hence limiting adhesions. 2,3 A systematic review by Talsma et al. 4 demonstrated that ‘early controlled mobilization’ is superior to ‘immobilization’ in the short term for the postoperative management of zone IV to zone VIII extensor tendon injuries. However, their results were less conclusive when comparing ‘early controlled mobilization’ with ‘early active mobilization’ and there was no evidence to suggest that any of the three rehabilitation regimens is superior when assessing longer-term outcomes. 4 Only five studies met the criteria for the systematic review with most studies in the literature being excluded due to their single cohort design. Talsma et al. 4 emphasized the need for further research related to rehabilitation protocols. The three rehabilitation categories used to treat zone V and VI extensor tendon repairs are outlined below.
Immobilization
Over the last 70 years, numerous studies have demonstrated acceptable long-term range of motion results from immobilization following extensor tendon repairs. 1,5,6 Immobilization regimens aim to provide protection to healing tendon/s by preventing tendon movement. They are simple to apply, have a low profile design, require no exercise programmes and are suitable for use in non-compliant patients. 3 Immobilization, however, limits functional use of the affected hand.
Early controlled mobilization
Early controlled mobilization regimens seek to achieve passive motion of the repaired tendons. Techniques such as dynamic outriggers or extension splinting are most commonly used. Further, immobilizing the metacarpo-phalangeal (MCP) joints, preventing active MCP joint extension and leaving the interphalangeal (IP) joints free to mobilize is another therapy technique.
Many authors advocate dynamic splinting. 2,7–10 Techniques typically involve the use of elastic traction that limits active flexion and allows passive extension of the MCP joints while also allowing active IP flexion and extension. Disadvantages of a dynamic splint include wrist immobilization, a high profile design, and disciplined compliance with an exercise regimen. Recommended time for splint wear is between three and five weeks, with functional use of the hand not possible until splint removal. 2,8
Another splint design is the low-profile Levame splint that allows early controlled mobilization. 11 This hand-based splint with steel leaf springs passively returns the repaired finger/s into extension. It is most suitable in simple zone V repairs while a forearm-based splint is used for zone VI and more complex zone V repairs. 11 Limited-active flexion of the MCP and IP joints of the injured finger occurs and the uninjured fingers are free from the splint, allowing some functional hand use.
Additionally, functional static splinting was introduced by Slater and Bynum. 12 The simple static splint is worn for an average of six weeks and is fabricated to immobilize the wrist, hold the MCP joints in 20–30° of flexion while the IP joints are free to mobilize and patients are allowed to use the hand cautiously for basic activities of daily living. 12
Early active mobilization
Safe active motion of a repaired extensor tendon has been achieved via regimens that permit limited motion across the MCP and IP joints with support from static and dynamic splints. Two early active regimens have modified early passive protocols and have created an ‘early active regimen’ by including either active MCP joint extension 13 or active wrist extension 14 while preserving the use of a dynamic outrigger.
Another protocol, the Norwich regimen 15 uses a static forearm-based palmar splint and includes an exercise programme of combined active MCP and IP extension and MCP extension with IP flexion. Functional hand use is commenced after removal of the splint at four weeks. The study advocates this regimen as the splint and the protocol are not cumbersome and results are comparable with those found with dynamic splints. 15 Khandwala et al. 16 introduced active MCP extension and synchronous flexion of all MCP and IP joints with their palmar blocking splint that left the IP joints free. In their study, no statistically significant difference was found with regards to the outcome measure of range of motion analysed using both the Miller and total active motion (TAM) assessments between a dynamic outrigger splint and the palmar blocking splint. 16 They concluded the latter technique was preferred due to its simplicity, low cost, patient convenience and reduced therapy time. 16
The ‘relative motion splint’ was designed in the early 1980's by Merritt et al; 17 however, its supporting data were not published until 2000. The original version of this splint consisted of a static wrist splint linked via a strap to a static finger yoke-gutter splint. With time the splinting technique has been enhanced to produce the Immediate Controlled Active Motion (ICAM) splint programme, currently in its third version. This splint consists of two components worn full time for the first three postoperative weeks: a wrist extension splint with 20–25° of extension, and a finger yoke splint holding the repaired tendon/s in 15–20° more extension relative to the uninjured digit/s. Between weeks 3 and 5 the wrist component is discarded unless performing medium to heavy-duty tasks. Following this, to protect the repaired tendon while completing medium to heavy-duty tasks, the yoke splint is applied. Patients are given individual exercise programmes to achieve full active motion within the limits of the splint. 18 Merritt highlights that the splint allows the patient to continue normal activities. 18
Thomas et al. 11 describe in a personal communication with Hoel in 1993, a yoke splint in the postoperative management of incomplete lesions and isolated lesions of extensors to the index and little fingers. However, no data or trial outcomes of this splint have been reported in the literature.
This article describes the implementation of an alternative early active mobilization protocol. It is a modified version of ‘the relative motion splint’ and ICAM protocol described by Merritt et al. 17 and Howell et al. 18 We have labelled it the ‘Modified Relative Motion Splint’ (mRMS).
Modified relative motion splinting
Review of the literature suggests, with similar range of motion outcomes, a simple splint design is preferable to a dynamic outrigger. 15,16
By integrating the features of several splint designs and rehabilitation protocols the mRMS was developed. Central to the rehabilitation programme is a simple, small splint that permits functional hand use.
The main design modification from the ICAM 18 splint was to discard the wrist component, leaving only the finger yoke. The clinical reasoning behind this decision was four-fold. Firstly, Thomas et al. 11 had achieved successful results with their hand-based Levame splint for zone V injuries and reported successful results using a yoke-only splint for incomplete tendon lacerations and isolated injuries of the index and little fingers. Secondly, Evans' 13 immediate short arc motion protocol supported active finger extension when the wrist was positioned in 20° of flexion. Thirdly, Eissens et al. 14 advocated early active wrist mobilization. Finally, if synchronous wrist and finger flexion were avoided, a wrist splint may be unnecessary. Sharma et al. 19 in examining relative motion splinting in a cadaveric model, set the wrist at 25° extension and found it to be effective in reducing strain on repaired zone VI tendons. The authors reported that with the wrist splinted in extension, synchronous wrist and finger flexion is prevented and they recommended future studies to evaluate decreased wrist extension on repair site strain. 19
Methods
Following ethical approval from the Human Research Ethics Committee at Austin Health, a retrospective review was undertaken of 46 consecutive single finger zone V and VI extensor tendon repairs. The 46 patients received either immobilization or modified relative motion splinting between 2000 and 2009. Patients with isolated extensor indicis, extensor digiti minimi or extensor digitorum communis injuries and/or an associated capsular repair were included in the study. The exclusion criteria included patients with tendon repairs to more than one finger, associated fractures, incomplete data-sets and failure to attend for follow-up, or those aged 17 years and under. A total of 39 patients met these criteria. The Austin Health Plastic and Reconstructive Surgery Unit performed all tendon repairs and patients were referred to occupational therapy for postoperative management following an outpatient clinic appointment with the treating surgeon. Mode of rehabilitation was selected on the basis of delay of referral to therapy. This delay was due to administrative issues, primarily clinic availability for patients to attend and did not relate to any surgical variable. All patients were immobilized after surgery by a plaster of Paris back slab. Patients seen by the therapist within seven days of surgical repair were selected for the mRMS protocol and patients seen after seven days continued to be treated by immobilization. Sixteen patients (16 fingers) were in the immobilization group and 23 patients (23 fingers) in the modified relative motion splint (mRMS) group. Details of the protocols and splint designs are outlined below.
Treatment protocols
Immobilization group
A resting splint was fabricated at the initial outpatient clinic appointment following surgery. Patients were instructed to wear their splint at all times until review with the therapist. Mobilization was commenced four weeks following tendon repair. At this time splinting was ceased and a home exercise programme began that addressed any joint stiffness, tendon lag or scar adhesion. Patients attended therapy sessions weekly or fortnightly, depending on need. They were advised to avoid ‘heavy’ tasks for a total of 8–10 weeks.
mRMS group
At the initial outpatient clinic appointment, between two and seven days postoperatively, both the mRMS and the resting splint were fabricated. Patients were instructed to wear the mRMS during the day and to wear the resting splint overnight. No specific home exercises were prescribed. Patients were encouraged to use their hands functionally when wearing the mRMS, but were asked to avoid simultaneous wrist and finger flexion. Patients attended therapy at least fortnightly. The resting splint was ceased after four weeks when a home exercise programme began addressing any joint stiffness, tendon lag or scar adhesion. Patients were encouraged to wear the mRMS when performing ‘heavy’ tasks for a total of 8–10 weeks.
Splint designs
Resting splint
Forearm-based splints were fabricated with 3.2 mm thermoplastic. The wrist was immobilized in 30° extension, and the MCP joints in 30° flexion. IP joints were positioned in full extension. (Figure 1).

Resting splint beside modified relative motion splint
Modified relative motion splint
A 3.2 mm thermoplastic strip (1.5 cm × 15 cm) was moulded over the proximal phalanges holding the injured finger in 15–20° of relative extension to the uninjured fingers. (Figures 1–10). All four fingers are included in this splint design.

A 1.5 cm strip of thermoplastic is cut to fabricate the modified relative motion splint

The injured finger is held in relative extension

The modified relative motion splint is moulded over the proximal phalanges

The therapist ensures the injured finger is held in relative extension to the uninjured fingers
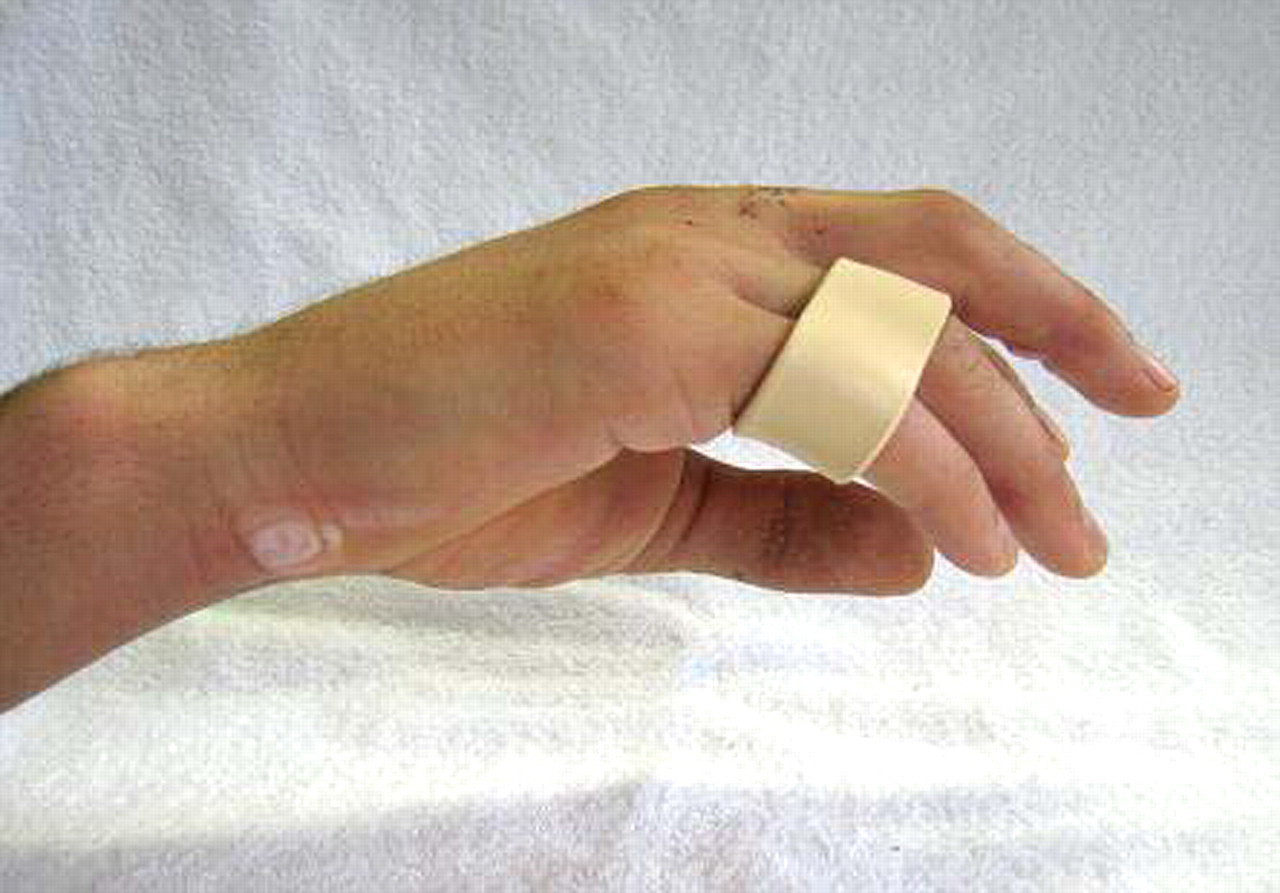
Lateral view of modified relative motion splint

Dorsal view of modified relative motion splint

Volar view of modified relative motion splint

Functional use of the hand including drinking from a cup is encouraged with modified relative motion splint

Early return to activities such as writing is possible with modified relative motion splint
Outcome measures
Range of motion was measured using a 15 cm plastic goniometer. Kleinert and Verdan's total active motion assessment of extensor tendons (TAM) system was then employed to compare group results at 6 and 12 weeks following surgery. 20 TAM is calculated by the following formula: TAM = ([MCP + PIP + DIP flexion] − [MCP + PIP + DIP extension lag]). 20 Ratings are achieved via comparison to the contralateral finger with ‘excellent’ corresponding to an equal TAM, ‘good’ for TAM > 75%, ‘fair’ for a TAM > 50% and poor with a TAM < 50%. 20 Information on return to work and return to activities of daily living was also recorded. Return to work data were collected in two categories: average return to work timeframe and manual workers return to full duties.
Statistical analysis
Two-way mixed analysis of variance (ANOVA) was used to examine the interaction between splinting regimen and time. The significance of the effect of treatment protocol on mean %TAM and return to work data were tested using the Mann-Whitney U test with statistical significance set to P = 0.05 (GraphPad Prism 5 Software).
Results
Patient demographics are summarized in Table 1. The immobilization group mean age was 39.4, with a range of 18–69 years, and consisted of 13 men and three women. The mRMS group mean age was 37.2 with a range of 19–72 years, and consisted of 22 men and one woman.
Patient demographics
mRMs, modified relative motion splint; EDC, extensor digitorum communis; EDM, extensor digiti minimi; EI, extensor indicis
The majority of lacerations occurred in zone V, 13 in the immobilization group and 21 in the mRMS group. The joint capsule was breached in 6/13 zone V injuries in the immobilization group and in 12/21 in the mRMS group. Fewer lacerations occurred in zone VI, three in the immobilization group and two in the mRMS group.
As illustrated in Table 2, the mRMS group demonstrated significantly improved range of motion when compared with the immobilization group. This effect was most marked at six weeks with a 12% difference in mean %TAM between the two groups (P = 0.0076, Mann-Whitney U test). Figure 11 shows the corresponding mean category ratings for the two groups over time. At the six-week assessment the immobilization group achieved a mean category rating of ‘fair’ compared with the ‘good’ category rating of the mRMS group. In this way, the mRMS-treated patients achieved ‘good’ and ‘excellent’ range of motion scores earlier than the immobilization group. Of the patients in the mRMS group, 18 of the 23 recorded ‘good’ or ‘excellent’ results six weeks postoperatively, while the immobilization group recorded ‘good’ results in 10 out of 16 patients. Similarities were observed between groups 12 weeks postoperatively. All 23 fingers in the mRMS group and 15/16 fingers in the immobilization group recorded ‘excellent’ or ‘good’ results at this time point. Two-way ANOVA was used to test for a possible interaction between time and splinting regimen. No statistically significant interaction was found (P = 0.092); however, the use of mRMS protocol and increased time postsurgical repair (12 versus 6 weeks) both demonstrated statistically significant improvements in TAM scores (P = 0.014 and P < 0.0001, two-way ANOVA).
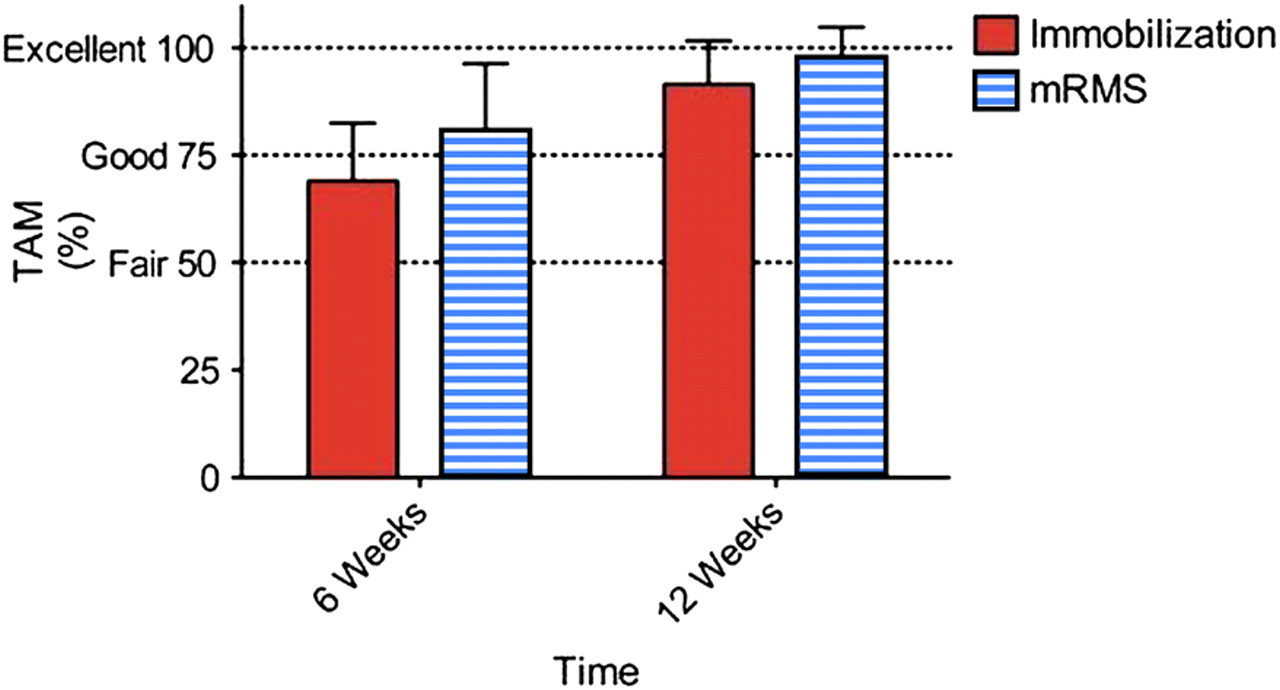
Total active motion (TAM) ratings and mean %TAM changes over time
Mean %TAM and proportion of patients in each outcome category
TAM, total active motion
Differences in return to work times between groups were statistically significant (P = 0.0062, Mann-Whitney U test) and details of return to work timeframes are presented in Table 3. The average return to work was significantly better in the mRMS group (mean return to work 3.3 weeks) compared with the return to work data for the immobilization group (mean return to work 9.4 weeks). Those in the mRMS group returned to work on average 42 days earlier than those in the immobilization group. Seventeen patients were manual workers, 6/16 in the immobilization group and 11/23 in the mRMS group. Injuries sustained at work comprised nine of the 39 patients studied. Again, there was a significantly earlier return to work for manual workers in the mRMS group compared with the immobilization group (P = 0.0071 Mann-Whitney U test). None of the six manual workers in the immobilization group returned to any form of work duties by six weeks, with an average return to full duties at 11.7 weeks. Five of the 11 manual workers in the mRMS group returned to full work duties by six weeks with an average return to full duties at 7.7 weeks. There was no incidence of infection or tendon rupture in either group.
Mean return to work times and patient proportions of return to work
mRMs, modified relative motion splint; RTW, return to work
Discussion
Multiple postoperative protocols for the management of extensor tendon repairs have been described in the literature. When comparing the various regimens, range of motion is the predominant outcome measure. Similar range of motion outcomes are demonstrated 12 weeks postoperatively for each of the ‘immobilization’, ‘early controlled mobilization’ and ‘early active’ protocols. 4 Our study replicated these results with both treatment groups experiencing no significant difference in range of motion 12 weeks postoperatively. While direct comparison between studies is difficult due to differing study parameters, there is enough evidence to indicate a benefit associated with ‘early controlled or ‘early active’ protocols over ‘immobilization.’ 5 The range of motion outcomes for our ‘immobilization’ group are similar to other outcomes reported in the literature. 1,5,6 As with other studies comparing immobilization and early mobilization protocols, patients in our study achieved statistically significant differences between groups. 8,21,22 At the six-week postoperative time point, the early mobilization group attained 12% more TAM when compared with the immobilization group. The magnitude of this effect resulted in the mean %TAM score being graded as ‘good’ for the mRMS group, but only a ‘fair’ grading for the immobilization group. Clinically, this improved rating for the mRMS group may translate into improved hand function; however, this would require further investigation to accurately quantify.
When comparing results of our study with other ‘early mobilization’ protocols, (either ‘early controlled’ or ‘early active’ protocols) the results are comparable. All patients in the mRMS group scored ‘excellent’ and ‘good’ results 12 weeks postoperatively. While direct comparison is difficult with varying outcome measures, our results appear similar to the 97% using the Levame splint, 23 the 86% using a functional static splint via Millar's classification 12 and 92% in the Norwich Regimen using the Dargan criteria. 15
Important considerations when designing a splint include splint size, aesthetics, costs, and ease of rehabilitation and protocol implementation. Most importantly the splint must protect the tendon repair.
Despite the wrist being free to mobilize during the day in the mRMS, no tendon rupture or tendon lag was noted in our 23 patients. The intraoperative trial conducted by Howell et al. 18 reported tension on an extensor tendon repair was reduced when the wrist was placed in 20° of extension. It is assumed that the majority of functional tasks occur within the tenodesis range. Hence, the simple instruction to avoid simultaneous wrist and finger flexion while wearing the mRMS may have prevented tendon rupture or gapping. Further studies are warranted to investigate the degree of tension placed on a tendon repair with this approach. Additionally, the overnight resting splint may have decreased the risk of tendon rupture or gapping by avoiding unintentional composite wrist and finger flexion during sleep. Furthermore, the night splint can assist in managing any oedema that occurred while wearing the mRMS. Thomas et al. 11 describe using Hoel's yoke splint for incomplete tendon repairs or isolated tendon repairs of the index and little finger only. Our study, however, has trialled and found that a yoke-only splint can be applied safely to complete tendon repairs of any finger.
It has been recommended that due to its simplicity an immobilization protocol should be implemented for non-compliant patients. 22 Hall et al. 21 have suggested that an immobilization protocol decreases the risk of tendon rupture, as a patient is not required to complete a precise home exercise programme. Patient compliance in regards to splint wear and therapy is essential for safe and effective rehabilitation. According to Khandwala et al. 16 many patients were excluded from their study due to failure to participate in therapy and suggested this is a recurring problem in a young, largely male population. The majority of patients within our study fit into this demographic. Further to this, with similar postoperative results of early mobilization protocols using either dynamic or static splints, use of a simple, inexpensive splint design is preferable to dynamic splints, which can be more expensive, complex to fabricate and inconvenient to wear. 12,15,16,21 Based on this hypothesis that simplicity encourages compliance, we postulate that our modified relative motion splint with simple design and simple instructions may not only yield better measurable results than an immobilization design, but also yield improved compliance as it enables early functional hand use.
Models of health, such as that described by Townsend, 24 reflect the importance of participation in meaningful daily living activities to promote wellbeing. All patients were able to perform activities of daily living while wearing the mRMS with the exception of activities requiring simultaneous wrist and finger flexion. Currently, there are three designs that enable early functional hand use. These are: the Levame splint, 23 Slater and Bynum's 12 functional static splint and the relative motion splint introduced by Merritt et al. 17 with the later development of the ICAM protocol by Howell et al. 18 It is understood that functional hand use is restricted while wearing any splint. However, we believe that our modified version of relative motion splinting is the smallest splint design presented in the literature, with the least functionally limiting protocol. An example of early return to functional activities when wearing the mRMS is the capacity to complete bilateral tasks such as eating, dressing and showering. In the latter case once showered, patients are instructed to remove the splint while their hand is supported on a table, dry the hand and splint, and then re-apply the splint. Additionally, functional hand use translates into the ability to return to work.
Hall et al. 21 state, ‘ultimately, the patient's goal is rapid return to work’ (p. 687). Little is published with regards to return to work activity for those treated with an immobilization regimen. Purcell et al. 6 noted in their study, all patients had returned to their previous employment at a four-month assessment; however, time from injury to return to work was not detailed. In our case, the immobilization group returned to work at an average of 9.4 weeks post-tendon repair, consistent with literature. 7,9,15,16,25 This was significantly later than the mRMS group, who returned on average at 3.3 weeks. These findings are consistent with the results obtained using the two-part splint and ICAM protocol. 18 The Norwich regimen, another early active mobilization protocol, recorded a lengthier return to work timeframe with an average return to work of 6.5 weeks for simple tendon injuries and 8.5 weeks for complex injuries. 15 Similarly, early controlled mobilization protocols detailed lengthier return to work timeframes. Browne and Ribik 9 reported an average return to work of 9.5 weeks, Bruner et al. 7 10 weeks, Hung et al. 25 8.5 weeks and Khandwala et al. 16 reported return to light work at 4 weeks, driving at 8 weeks and heavy manual work at 12 weeks. It is therefore, believed that the mRMS is a valuable splint option for return to work.
Return to manual work prior to 10–12 weeks post-tendon repair has not been recommended in the literature. 14,16 Manual workers in our study allocated to the mRMS group were able to return to full duties by 7.7 weeks. Discussion with the patient is essential to determine their work duties and suitability for return to work. An electrician within our group chose to wait 10 weeks before returning to work, as he believed he could not avoid composite wrist and finger flexion in his role. In contrast, a carpenter was able to return to work and use his tools following mRMS application 10 days following surgery. We believe that while the mRMS is being worn and after adequate education, earlier return to work is permitted as the tendon is sufficiently protected and the wrist is free to move. For patients aiming to return to full manual work prior to the previously anticipated 10–12 weeks, this splint may allow them to return immediately following splint application. A suitable return to work plan would be enhanced via collaboration between the treating surgeon, therapist and patient.
Implications for hand therapy practice
Considering comparable range of motion results are ascertained using either the mRMS protocol or other early mobilization protocols, we advocate use of the mRMS as it is small, inexpensive, simple to fabricate and associated with a simple treatment regimen.
Successful outcomes using the mRMS protocol in this study were achieved by patients wearing the mRMS during the day and a resting splint overnight for the first four weeks, then continuing to wear the mRMS for a total of 8–10 weeks for ‘at risk’ activities. Further investigation into the temporal components of this protocol are warranted, such as reviewing the postoperative timing of initial mRMS application, and the length of time the splint should be worn to adequately protect the healing tendon/s. Exploration of adjunctive therapy in treatment sessions is also recommended. For instance, incorporating active flexion and extension exercises in the first four postoperative weeks, such as those outlined in the Norwich regimen, 15 may enhance this protocol and minimize any later therapy required to regain movement, in particular MCP flexion. Optimal patient outcomes will also be achieved when the treating therapist considers both the art and science of hand therapy via clinical reasoning. Individual variations to the mRMS protocol need to be made based on patient progress and therapist judgement. For example, the frequency of exercises may need to be increased for a particularly stiff joint, or early detection of a tendon lag can be addressed by decreasing the amount of MCP joint flexion in the night resting splint.
The mRMS protocol should be explored to assess its suitability for use in more complex cases where associated injuries exist other than underlying capsular repair. The inclusion criteria for this study were single finger tendon repairs. External to this study, the authors have successfully used the modified relative motion splint for patients who have sustained tendon injuries to two fingers. This splint design has enabled a patient who had bilateral ring and little finger tendon repairs in zone V to be functionally independent following splint application five days after surgery.
The small sample size and lack of random allocation to the two treatment groups are limitations of this retrospective review. There is potential for selection bias and systematic differences in the groups as a result. Additionally, different therapists collected data and various plastic and reconstructive surgeons conducted the surgical tendon repairs adding to the number of variables in this retrospective review. We recommend future randomized controlled trials.
Conclusion
The modified relative motion splint used in conjunction with a night resting splint can be safely applied in the postoperative management of a single zone V or VI extensor tendon repair. Advantages to this protocol include the small simple splint design, and straightforward patient instructions that enable early mobilization, early functional hand use and early return to both daily living and work.
Footnotes
Acknowledgements
The authors wish to thank: Tanya Cole, Pearse Fay and Georgia McGuinness, Occupational Therapy colleagues at Austin Health for assisting in data collection; Amanda Bladen, Austin Health Occupational Therapy Manager for her support and encouragement, the late Leanne Breen who was involved in the early implementation of this splint design and Natalie Horman for her assistance with manuscript preparation.