
Abstract
Introduction
The overall aim of this study was to determine whether physical impairments – loss of range of motion and grip strength – could be used to predict hand dexterity functions in patients at 1 and 2 years after distal radius fracture.
Methods
This was a prospective cohort study. Hand dexterity was assessed at three different levels using the NK hand dexterity test. We used a manual goniometer to measure the active range of motion in the affected hand for wrist flexion and extension movements, and a J-Tech grip strength device to measure patients’ hand grip strength levels. Assessments were performed at 1- and 2-year follow-ups. Separate multivariable regression analyses were performed to determine if range of motion predicts hand dexterity functions at 1 and 2 years after distal radius fracture.
Results
A total of 160 patients with distal radius fracture were included in this study. Range of motion (flexion and extension) and grip strength were both statistically significant (p < 0.05) independent variables in predicting hand dexterity functions at all three levels among patients after distal radius fracture at 1-year follow-up. Range of motion and strength levels accounted for 31%, 33% and 22% of the variance in patients’ large, medium and small hand dexterity functions, respectively. At 2 years, grip strength remained the only statistically significant (p < 0.001) independent variable in predicting hand dexterity functions at all three levels.
Conclusions
Physical impairments (loss of range of motion and grip strength) have higher predictive values for large and medium hand dexterity functions, than small hand dexterity functions, in patients after distal radius fracture, at both 1- and 2-year follow-up periods.
Introduction
Distal radius fracture (DRF) is regarded as one of the most common types of fractures, with consequences that lead to loss of work hours and independence, as well as lasting disability.1–3 DRF accounts for nearly 18% of all fractures in older adults and is caused by falls from a standing height with a dorsally outstretched hand.1–3 DRF can cause major functional decline in elderly. 3 Patient-reported outcomes refer to subjective assessments and can capture function after discharge by administering questionnaires or collected via mail, whereas performance-based measures like grip strength and range of motion (ROM) require equipment, therapist time and patients’ visit to clinics. 4 However, expert consensus indicates that performance-based measures of grip strength and ROM are two of the most important standardized outcome assessments for DRF. 4
Hand dexterity has been defined as a series of skills and abilities that a person requires to use one’s hands with ease and efficiency and to manipulate objects of different sizes.5–6 Dexterous use of hands is needed to carry out activities of daily living and occupational tasks; therefore, hand dexterity is regarded as a component of hand function. 6 Furthermore, impairments in ROM and grip strength levels, have been shown to explain nearly one-third of the variation in hand dexterity function at 6-month follow-up. 5
However, there is a paucity of reports in the literature, and subsequently in a Cochrane review and the American Academy of Orthopaedic Surgeons practice guidelines, concerning the long-term hand dexterity outcomes following DRF.7–10 Assessing the long-term relationship between ROM, grip strength impairments and hand dexterity following a DRF, can potentially provide researchers and clinicians with a far better understanding of which impairment-based treatments are likely to have an impact on hand function. Therefore, the overall aim of this study was to determine whether physical impairments (loss of ROM and grip strength) could be used to predict hand dexterity functions in patients at 1 and 2 years after DRF.
Methods
Study design
We conducted a prospective cohort study. However, the research questions were formulated retrospectively. We obtained ethical approval through the Faculty of Health Sciences Ethics Committee of Western University.
Setting
This study was carried out in a clinical lab, the Roth McFarlane Hand and Upper Limb Centre, London, Ontario, Canada. Two research assistants performed all the measurements between September 2011 and August 2015 and ensured that standardized procedures were followed. Patients were informed to visit the clinic for follow-up assessments after 1 and 2 years.
Recruitment and participants
The inclusion criteria for this study included individuals who ranged in age between 18 and 75 years, with a DRF. Patients with DRF who presented with neurological or comorbid conditions that limited their ability to manipulate large, medium and small objects were excluded from the study. A total of 391 patients with DRF were initially referred by their orthopaedic surgeons to be recruited for this study; however, 160 patients were re-assessed at 1- and 2-year follow-ups. Patients provided written informed consent and agreed to participate in this study.
Outcome measure: Hand dexterity
The dependent variable in this study was hand dexterity functions, assessed at three different levels using the NK hand dexterity test (NKHDT). The NKHDT is a computerized timed test that is used to assess the speed at which hand-related tasks such as lifting, placing or screwing are performed using small, medium and large groups of objects. In this study, we followed the NKHDT measurement protocol established by Turgeon et al. 11 and performed all the three levels (small, medium and large) of NKHDT, using the affected hand. The clinical measurement properties of NKHDT have been previously reported, and the NKHDT is considered a reliable, valid and responsive test in patients with DRF.6,11,12
Impairment measures: ROM and grip strength
We used a manual goniometer to measure active ROM in the affected hand for the wrist flexion and extension movements.13,14 Manual goniometry of the elbow and forearm has been shown to be a reliable, valid and responsive tool in measuring active ROM.13,14
We used a J-Tech grip strength device (JTech Medical, Midvale, UT) to measure patients’ hand grip strength levels. The device records grip strength levels in kilograms (kg) of force. We followed the hand grip strength testing protocol recommended by Clerke et al. 15 Patients were asked to hold the J-Tech dynamometer using the affected hand with the elbow flexed and the forearm and wrist in neutral positions, then instructed to squeeze the J-Tech handle for 2 to 3 s for recording of maximal grip strength. 15 A total of three measurements of grip strength were taken and the average recorded. A 15-s break period was allowed between each measurement. 15 All assessments were performed at 1- and 2-year follow-ups.
Statistical analysis
Demographic characteristics (age, ROM, grip strength and hand dexterity function) were described using means and standard deviations or for nominal data (sex, dominant/injured hand and types of treatments received) reported as frequency counts and percentages. We conducted separate multivariable regression analyses to determine if wrist ROM – flexion/extension and grip strength (independent variables) could be used to predict large, medium or small objects hand dexterity functions (dependent variables) at 1 and 2 years after DRF. To test whether assumptions for multivariable regression analysis were met, we conducted tests of normality, heteroscedasticity, multicollinearity and linearity prior to our analyses. We performed our analyses using IBM SPSS Statistics software version 22.0 and a significance level of p < 0.05 was considered statistically significant.
Results
Sample
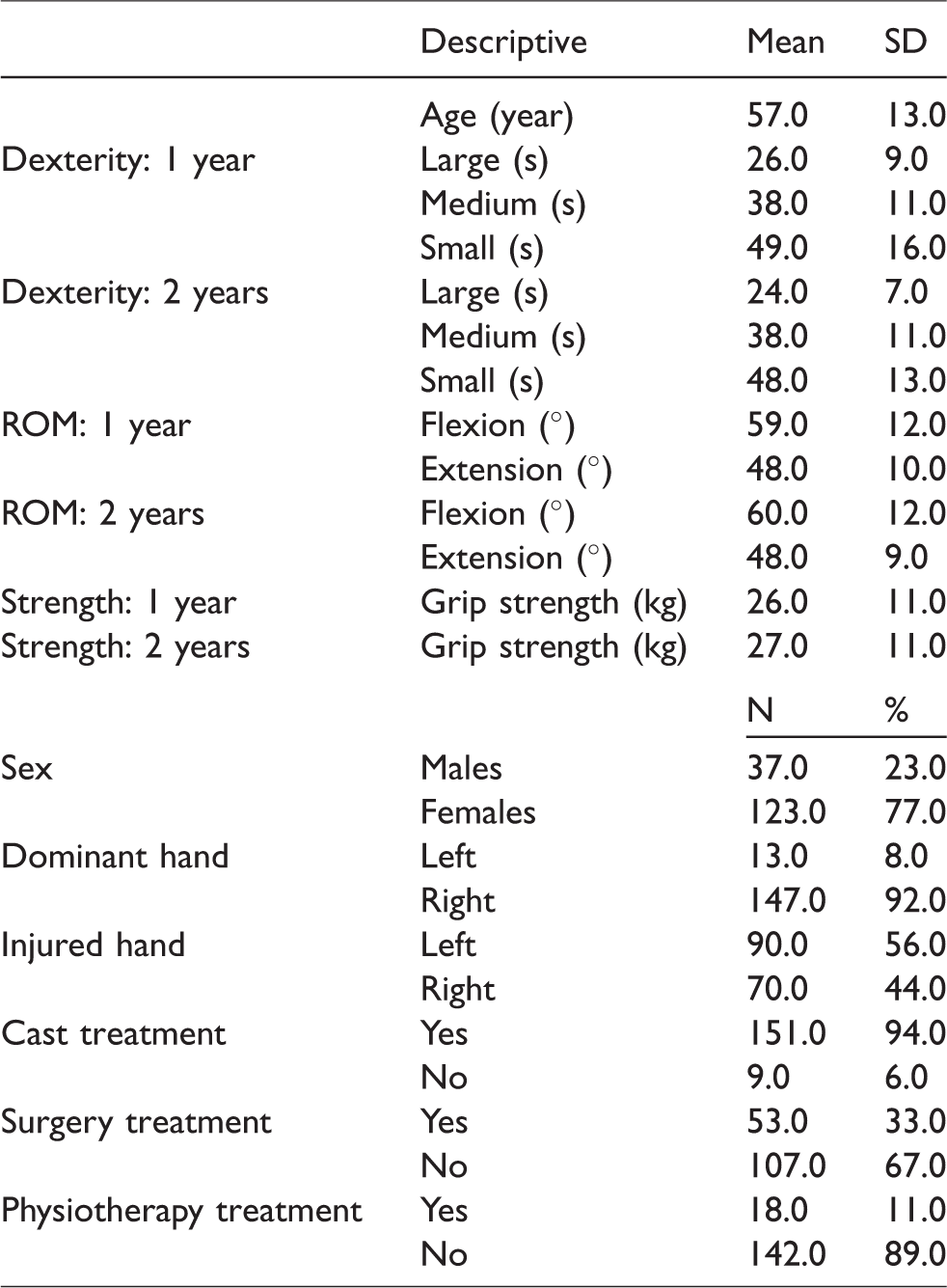
A total of 391 patients with DRF were initially referred. Of these, 160 were re-assessed at 1- and 2-year follow-ups. Therefore, 160 (123 females, 37 males) patients with mean age of 57 years (SD = 13) were included in the analysis (Table 1 and Figure 1). The majority of patients were right-hand dominant (92%). The proportions of injured hands were 56% and 44% for the left and right sides, respectively. At 1-year follow-up, the mean completion time of hand dexterity for manipulation of large, medium and small objects were 26 (SD = 9), 38 (SD = 11) and 49 (SD = 16) s, respectively. Similarly, mean completion times of 24 (SD = 7) for large, 38 (SD = 11) for medium and 48.0 (SD = 13) for small objects at 2-year follow-up. The mean measurements of ROM (flexion and extension) were 59° (SD = 12) and 48° (SD = 10) at 1-year, and 60° (SD = 12) and 48° (SD = 9) at 2-year follow-ups. Mean grip strength was 26 (SD = 11) and 27 (SD = 11) kg at 1- and 2-year follow-ups.
Demographic characteristics (n = 160).

Distal radius fracture patients flow diagram.
Regression models for factors predicting hand dexterity function
Independent variables ROM-flexion, ROM-extension and grip strength levels were entered into the models. Our multivariable regression models show that ROM (flexion and extension) and grip strength were both statistically significant (p < 0.05) independent variables in predicting hand dexterity functions at all three levels among patients after DRF at 1-year follow-up (Table 2). ROM and strength levels accounted for 31%, 33% and 22% of the variance in patients’ large, medium and small hand dexterity functions, respectively. At 2 years, grip strength remained the only statistically significant (p < 0.001) independent variable in predicting hand dexterity functions at all three levels (Table 3). ROM (flexion) was a statistically significant independent variable in predicting medium and small hand dexterity functions at 2 years. However, ROM and strength levels accounted for 26%, 30% and 20% of the variance in patients’ large, medium and small hand dexterity functions, respectively.
1-Year large, medium and small dexterity.
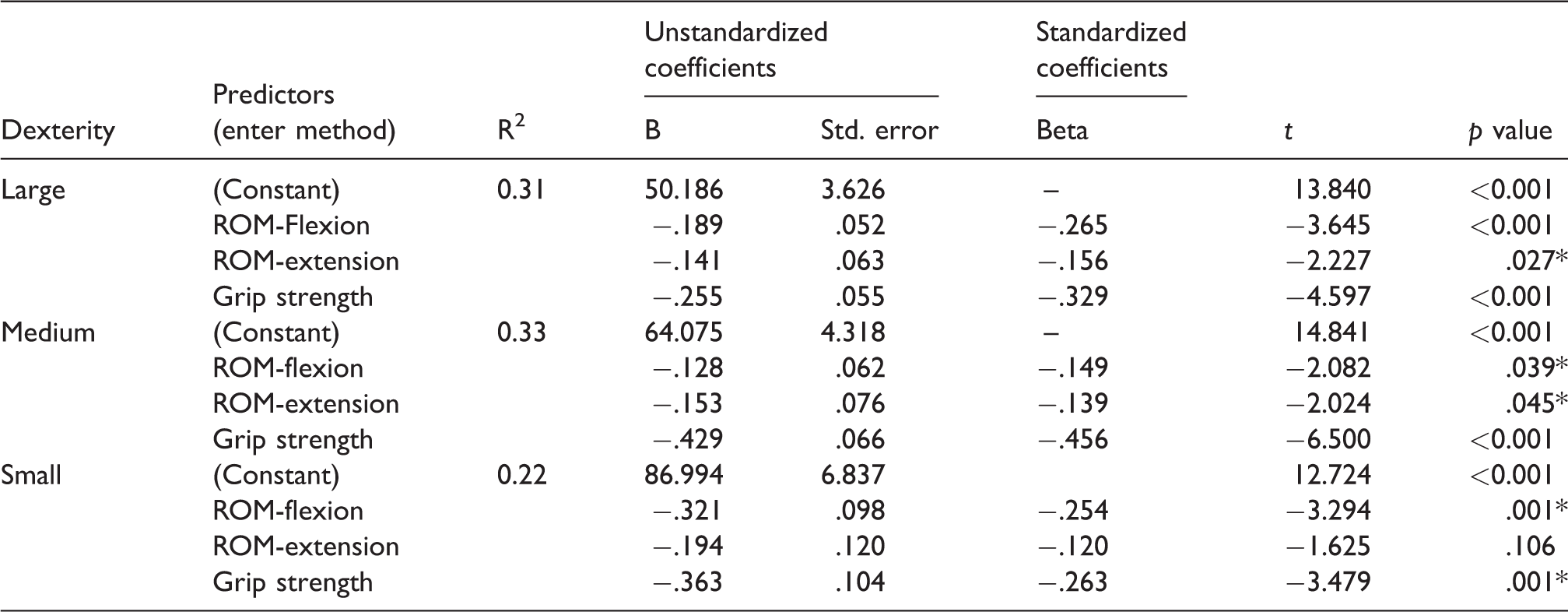
Note: R2 indicates the total amount of variation (predictive value) of the model based on the included variables. Standardized Beta Coefficients represent the unique contribution of each independent variable in predicting the outcome.
*p < 0.05 statistically significant.
2-Year large, medium and small dexterity.
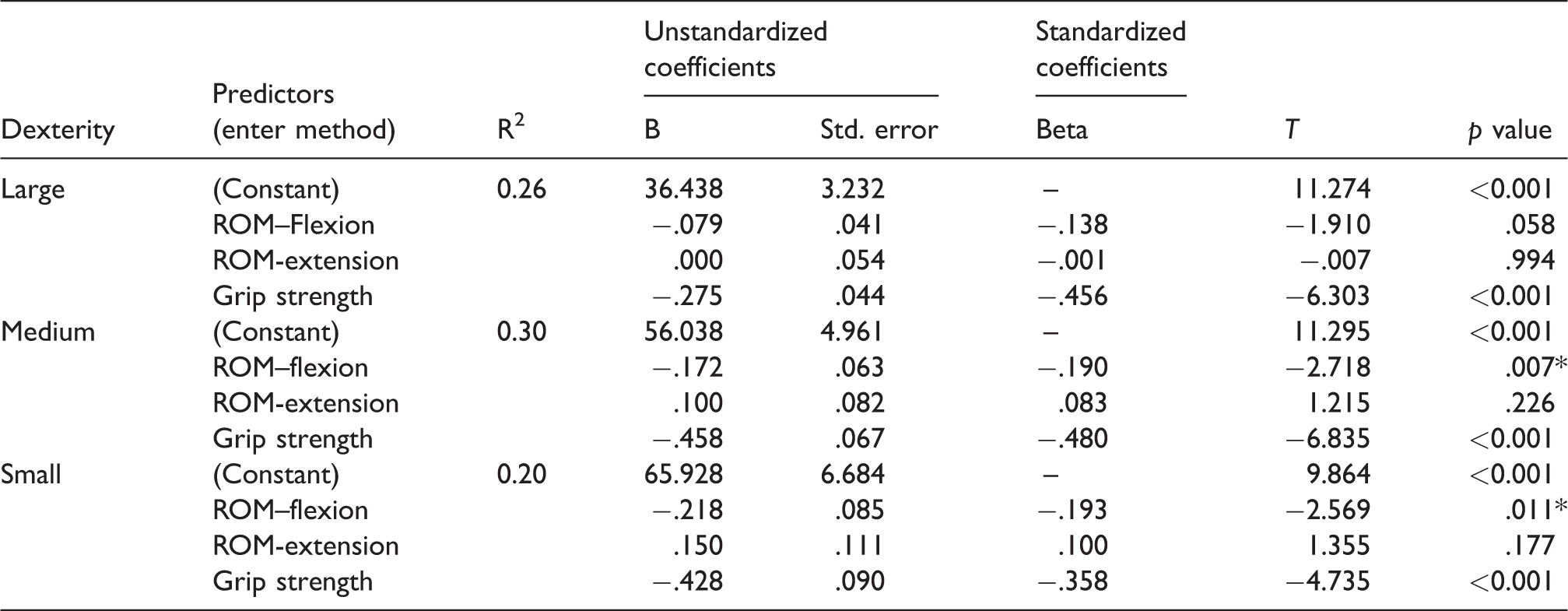
Note: R2 indicates the total amount of variation (predictive value) of the model based on the included variables. Standardized Beta Coefficients represent the unique contribution of each independent variable in predicting the outcome.
*p < 0.05 statistically significant.
Discussion
This study demonstrated that grip strength and active ROM scores can be used to predict hand dexterity functions at both 1 and 2 years after DRF. Despite their predictive ability, more than two-thirds of the variability remains unexplained. Factors such as pain, oedema and motor control may provide further insights into large, medium and small hand dexterity functions. However, these factors were not addressed in this longitudinal study.
The literature reports both ROM (arc flexion–extension) and grip strength as significant predictors, accounting for 28% of the variance in patients’ large hand dexterity functions after DRF, at 6 months’ follow-up. 4 Our multiple regression analysis at 1-year follow-up similarly displayed that ROM (flexion and extension) and grip strength were significant predictors of hand dexterity in manipulating large and medium objects. However, the significant predictors to manipulate small objects included ROM (flexion) and grip strength. This suggested that wrist extension motion might be less related to patients’ small hand dexterity functions and that factors such as finger extension motion or coordination of movement might have been of a greater importance in predicting small hand dexterity functions after DRF at 1-year follow-up.
At 2 years’ follow-up, our regression model variables (ROM and grip strength) explained similar amounts of variations in patients’ large, medium and small hand dexterity functions as compared to our 1-year follow-up models. Grip strength was a significant predictor for all-size object subtests. We were unable to compare regression models with other studies because of the lack of long-term reports addressing large, medium or small hand dexterity function after DRF.
Strengths of this study included the fact that we sampled a large number of patients and reported outcomes at 1- and 2-year follow-up periods. Despite this, our work has some limitations which should be considered when interpreting our results. Data collection was done prospectively; however, data analyses and the research questions were formulated retrospectively. Therefore, this prevented us from collecting additional details which might have further contributed to the predictive value of hand dexterity function. This can potentially contribute to selection bias (i.e. inadequate description of baseline characteristics of individuals in the study sample). In addition, our study sample included a smaller proportion of males than females, lowering precision and confidence in our findings in regards to males. There might be the potential for attrition bias within our study. However, it is generally accepted to include 10 to 15 participants per number of independent variables used in the linear regression model. Therefore, our final sample size of 160 participants was considered adequate.
Our study findings emphasise that performance-based assessments (grip strength and ROM) after DRF can provide clinicians with the knowledge that grip strength and active ROM contribute to better hand dexterity functions at both 1- and 2-year follow-up periods. Therefore, careful monitoring of hand dexterity recovery and prescribing of dexterity exercises would allow clinicians to improve grip strength and motion and incorporate valid rehabilitation goals as part of the rehabilitation program in patients after DRF.
Conclusions
This study provides information about the long-term (1 and 2 years) effects of loss of ROM and grip strength on hand dexterity functions in patients after DRF. It highlights that physical impairments (i.e. loss of ROM and grip strength) have higher predictive values for large and medium hand dexterity functions, than small hand dexterity functions, in patients at 1 and 2 years after DRF.
Footnotes
Acknowledgements
Special thanks go to Katrina Munro and Joshua Vincent for their valuable assistance in the data collection.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: JM was supported by a CIHR Chair in Gender, Work and Health and the Dr. James Roth Research Chair in Musculoskeletal Measurement and Knowledge Translation. The study was supported by Canadian Institutes of Health Research (FRN: 122070).
Ethical approval
We obtained ethical approval for this study through Faculty of Health Sciences Ethics Committee of Western University.
Informed consent
Written informed consent was obtained from the patient(s) for their anonymized information to be published in this article.
Guarantor
GN
Contributorship
GN researched literature, generated the research questions, analysed the date and prepared the first draft of the manuscript. PB was involved in protocol development and data analyses, and reviewed the written manuscript. JM reviewed the data analyses and edited the final version of the manuscript. EL and RG both reviewed the manuscript and provided valuable feedback.