
Abstract
Introduction
Handedness and hemispheric dominance are thought to influence manual performance, especially dexterity and grip strength, which underpin daily and occupational function. We investigated the effects of handedness and hemispheric dominance (inferred from a neurobehavioral inventory) on dexterity and grip strength, focusing on whether balanced hemispheric dominance confers advantages in mixed-handed/ambidextrous individuals.
Methods
This cross-sectional study included 182 adults (aged 19–50 years) who completed the Edinburgh Handedness Inventory to identify hand dominance and a neurobehavioral inventory to assess hemispheric dominance. Grip strength was measured using Constant 14,192-709E and Saehan Pinch Gauge SH5005, while dexterity was evaluated with the Purdue Pegboard Test. Statistical analyses were performed using SPSS 16, with significance set at P < 0.05.
Results
Right-handed participants exhibited significantly higher dexterity in the right hand (P < 0.001), while left-handed individuals showed greater grip strength in both hands, with marginal significance in the right hand (P = 0.046). Mixed-handed/ambidextrous individuals showed significantly higher assembly dexterity scores (P < 0.001). Interhemispheric balance was marginally associated with improved assembly dexterity (P = 0.05), suggesting its role in enhancing motor coordination.
Conclusion
Hand dominance and hemispheric dominance significantly influence motor performance. Balanced hemispheric function in mixed-handed/ambidextrous individuals enhances complex coordination tasks, highlighting potential benefits for rehabilitation strategies. Future research should explore these relationships using neuroimaging techniques and include a broader demographic range to further investigate underlying neural mechanisms.
Introduction
Upper limb motor abilities, particularly of the hands, play a critical role in maintaining independence in daily activities. 1 This significant role makes it essential to evaluate hand abilities and efficiency as an integral part of physical examinations and therapeutic processes. 2 Dexterity and grip strength, two primary components of motor ability, directly influence accuracy and skill in interactions with objects during daily, occupational and social activities.3,4 Reduced hand dexterity, especially due to injury, can lead to considerable limitations in performing precise and independent tasks; thus, strengthening and assessing dexterity are crucial in rehabilitation processes. 5 Moreover, grip strength, an indicator of forearm muscle force, not only reflects the functional health of the upper limbs but is also used as a marker for general health and a predictor of physical and cognitive disabilities, including neurodegenerative diseases.2,6,7 These measurements are also valuable in assessing cardiovascular health in older adults, evaluating functional capacity post-surgery, tracking recovery and muscle strength in athletes.2,7,8 Therefore, improving hand motor abilities forms the foundation for designing and developing effective rehabilitation strategies. 3
Research has shown that individual, environmental and occupational factors influence hand dexterity and grip strength. 9 Among these factors are age, sex, weight, height and hand dominance.4,6,7 Due to greater motor dominance and coordination, the dominant hand typically has superior dexterity and grip strength compared to the non-dominant hand.1,10 Previous studies have demonstrated that the dominant hand also performs better in fine motor tasks, 9 a trend observed across all age groups.6,11 However, some research has reported no significant difference in grip strength between the dominant and non-dominant hands, suggesting that this difference is independent of handedness type (right or left). 12
Evidence indicates that hand dominance is not solely a result of motor abilities but arises from complex interactions involving neuro-anatomical differences and specialized brain functions. 5 Studies reveal that motor and sensory control of the dominant hand is mainly governed by the contralateral hemisphere. 13 For instance, a study by Mentese et al. demonstrated that brain lateralization leads to left hemispheric dominance in right-handed individuals and right hemispheric dominance in left-handed individuals. 11 This dominance in right-handed individuals can be linked to stronger connections between the left sensory-motor cortex and movement control regions, particularly for fine motor skills involving distal, simple hand and finger movements. 5 Evidence from neuroimaging shows that, beyond fine motor control, complex manual praxis may rely on different hemispheric organizations. In many cases this control is bilateral, and the degree of lateralization varies widely across individuals, especially when handedness is considered as a continuum. 14
However, this pattern can vary in left-handed and mixed-handed/ambidextrous individuals, as suggested by previous studies on brain lateralization.14,15 This pattern suggests that hemispheric dominance in complex manual tasks is not fixed. It varies markedly across individuals. Adamo et al. reported that many left-handed people, whose neural organization is typically less strongly lateralized, show greater proficiency in using both hands. 13 Several studies also point to advantages in those classified as mixed-handed or ambidextrous.9,16 Mixed-handed refers to using different hands for different tasks. Mixed-handed/ambidextrous denotes equal proficiency in both hands across tasks. These groups often perform better on bimanual coordination tasks, which may suit occupations that require simultaneous use of both hands.9,16 Importantly, individuals who demonstrate task-specific variation in hand use are considerably more prevalent in the population, whereas individuals who exhibit truly equal proficiency across both hands are exceptionally rare. 17
A study by Oka et al. found that in left-handed individuals, both brain hemispheres jointly control motor skills of both the dominant and non-dominant hands. This more balanced distribution of motor control between hemispheres improves motor coordination. 18 Other research supports that, in right-handed individuals, the dominant left hemisphere plays a major role in the precise movements of the dominant hand, whereas left-handed individuals show similar features between the dominant hemisphere and their non-dominant hand. 11 Moreover, studies indicate that the right hemisphere in right-handed individuals plays a lesser role in controlling fine movements of the non-dominant (left) hand, potentially leading to reduced motor skills in that hand. 19
The present study investigates the interaction between handedness (right-handed, left-handed, and mixed-handed/ambidextrous) and hemispheric dominance on dexterity and grip strength. Previous studies have focused primarily on handedness, whereas the role of hemispheric dominance has received less attention. Mixed-handed/ambidextrous profiles, which may reflect more balanced interhemispheric contributions to motor control, also remain understudied. Using standardized objective measures, this research seeks to clarify motor characteristics across these profiles and to inform individualized rehabilitation strategies tailored to patients’ needs.
Materials and methods
Participants
This cross-sectional study enrolled 182 adults aged 19–50 years (mean 26.36, SD 6.36); 102 (56.0%) were women and 80 (44.0%) were men. By the Edinburgh Handedness Inventory (EHI), 89 (48.9%) participants were right-handed, 67 (36.8%) left-handed, and 26 (14.3%) mixed-handed/ambidextrous. Hemispheric dominance was right-hemispheric in 86 (47.3%), balanced in 75 (41.2%), and left-hemispheric in 21 (11.5%). All participants provided written informed consent.
Recruitment
Volunteers were recruited from males and females meeting the study criteria, which included the absence of diagnosed musculoskeletal or neuropsychological conditions that would interfere with the tests.
Measures
In this study, the Edinburgh Handedness Inventory (EHI) developed by Oldfield was used to determine each participant’s handedness score on a scale from −100 to +100. Scores from −100 to −40 classified individuals as left-handed, scores between +40 and +100 as right-handed, and scores between −40 and +40 as mixed-handed/ambidextrous. In this study, mixed-handed/ambidextrous denotes low preference on the EHI and does not, by itself, indicate equal proficiency across tasks (true ambidexterity is uncommon). 20 The validity and reliability of this questionnaire have been confirmed in multiple studies, with Cronbach’s alpha scores generally exceeding 0.9.21,22 The hemispheric dominance of each participant was identified using the refined Neurobehavioral Inventory of hemispheric dominance, 23 a tool validated for its accuracy in distinguishing brain hemisphere usage.13,23,24 It is important to note that this inventory assesses behavioral and neuropsychological preferences commonly associated with hemispheric functions, rather than direct neuroimaging-based measurements of hemispheric dominance. 23 This inventory assesses the respondent’s individual preferences across 12 questions, each presenting four scenarios representing four types of hemispheric dominance: (a) Left (Logical), (b) Left (Verbal), (c) Right (Manipulative-Spatial) and (d) Right (Creative). According to the scoring protocol for this tool, the sum of responses in categories (a) and (b) represents the score for left hemisphere dominance, while categories (c) and (d) represent the score for right hemisphere dominance. Thus, with 12 questions, total scores range from −12 (fully right hemisphere dominant) to +12 (fully left hemisphere dominant). Wagner recommends a minimum score difference of three points between right and left hemisphere scores to distinguish hemispheric functionality clearly; therefore, scores between −3 and +3 are classified as balanced hemisphere dominance. 23
Power and pinch grip strength were measured using the Constant 14.192-709E and Saehan Hydraulic Pinch Gauge SH5005, respectively, with units in kilograms of force (kgf), which refers to a unit of force representing the amount of force applied by the hand. Grip force measurements followed the protocol outlined by the American Society of Hand Therapists. 25 Dexterity of both hands was assessed using the Purdue Pegboard™ (Model 32.020A), a tool designed to simplify the evaluation of hand performance by consolidating the desirable features of various dexterity tests into a single, executable test. The validity and reliability of this tool have been well established26,27 and the test was conducted according to its standard instructions. 28 The primary dexterity tests included four main evaluations:
(1) right-hand dexterity in 30 s, (2) left-hand dexterity in 30 s, (3) both-hands dexterity in 30 s, and (4) assembly dexterity in 60 s.
Procedures
The testing procedure was conducted in a consistent laboratory environment with stable conditions regarding ambient noise, lighting and other potential confounding factors. Participants were seated and allowed to rest until their heart rate stabilized. They then completed a demographic questionnaire and the Edinburgh Handedness Inventory. Next, power grip strength for each hand was measured three times consecutively, with a one-minute rest interval between measurements using the Constant 14.192-709E. The mean of these measurements was used for analysis. Following this, pinch grip strength for each hand was measured in three rounds using the Pinch Gauge SH5005, with measurements taken in a manner similar to that of power grip assessment. Finally, after a one-minute rest, each participant’s dexterity was measured according to the Purdue Pegboard™ standard protocol.
Data analysis
Frequency (percentage) and mean (standard deviation) were employed to characterize categorical and continuous variables, respectively. The Kolmogorov-Smirnov test was utilized to evaluate the normality of the data. Demographic variables were compared using independent t-tests and paired t-tests. Furthermore, analysis of variance (ANOVA) and analysis of covariance (ANCOVA) were applied to investigate the impact of handedness and hemispheric dominance on various forms of dexterity and grip strength. Heat maps were generated using R software version 4.3.1 with the ‘MBA’, ‘spam’ and ‘fields’ packages. All statistical analyses were performed using SPSS software version 16, with the significance threshold set at 0.050.
Results
Manual performance by handedness (dexterity and grip strength).
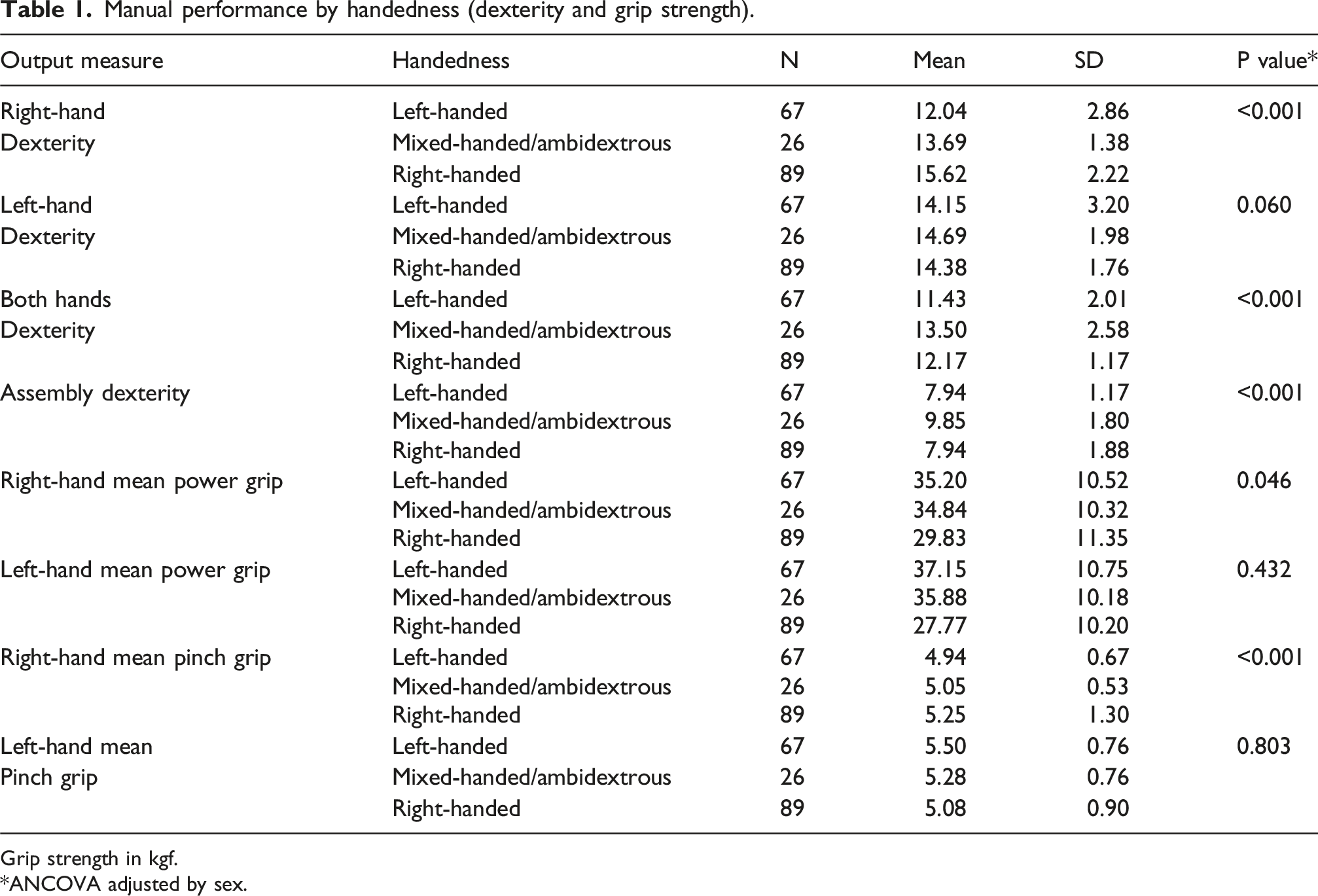
Grip strength in kgf.
*ANCOVA adjusted by sex.
Right-handed individuals showed significantly greater right-hand dexterity compared to left-handed and mixed-handed/ambidextrous participants (P < 0.001), while no significant differences were observed in left-hand dexterity (P = 0.060). Mixed-handed/ambidextrous individuals demonstrated significantly higher assembly dexterity scores compared to other groups (P < 0.001).
Left-handed participants exhibited the highest mean power grip strength values for both hands (right hand: 35.2 kgf; left hand: 37.15 kgf), with a borderline significant difference observed only for the right hand (P = 0.046). Right-handed individuals had significantly stronger pinch grip strength in the right hand (P < 0.001), with no significant differences detected for left-hand pinch grip strength across groups.
Impact of hemispheric dominance on different types of dexterity and grip strength.

*One-Way ANOVA.
Based on the data analysis section, heat maps were generated to illustrate the combined effects of handedness scores, classification of the three handedness types, and hemispheric dominance on hand performance variables. These heat maps correspond to right-hand dexterity (Figure 1), left-hand dexterity (Figure 2), both-hands dexterity (Figure 3) and assembly dexterity (Figure 4), consistent with the significant differences reported in Tables 1 and 2. Heat map showing the effect of handedness score and dominant hemisphere on right-hand dexterity. This heat map illustrates the relationships among right-hand dexterity (color scale), handedness scores, and hemispheric dominance. Darker shades denote higher dexterity. Among right-handed participants, those with right-hemispheric dominance exhibited the highest dexterity scores, indicating a right-lateralized dominance pattern. Mixed-handed participants with balanced hemispheric dominance showed relatively uniform performance across the map. Heat map showing the effect of handedness score and dominant hemisphere on left-hand dexterity. This heat map illustrates the relationships among left-hand dexterity, handedness scores, and hemispheric dominance. Left-handed individuals with right-hemispheric dominance demonstrate the highest dexterity scores, while mixed-handed/ambidextrous individuals with balanced hemispheric dominance exhibit consistent performance. The color gradient represents dexterity levels, with darker shades indicating higher dexterity values. Heat map showing the effect of handedness score and dominant hemisphere on both-hands dexterity. This heat map illustrates the relationships among both-hands dexterity, handedness scores, and hemispheric dominance. Mixed-handed/ambidextrous individuals with balanced hemispheric dominance achieve the highest scores in both-hands dexterity. Right-handed and left-handed individuals demonstrate lower performance compared to mixed-handed/ambidextrous participants, regardless of hemispheric dominance. The color gradient represents dexterity levels, with darker shades indicating higher scores. Heat map showing the effect of handedness score and dominant hemisphere on assembly dexterity. This heat map illustrates the relationships among assembly dexterity, handedness scores, and hemispheric dominance. The color gradient indicates dexterity levels, with darker shades representing higher values. Mixed-handed/ambidextrous participants with balanced hemispheric dominance perform best on assembly dexterity.

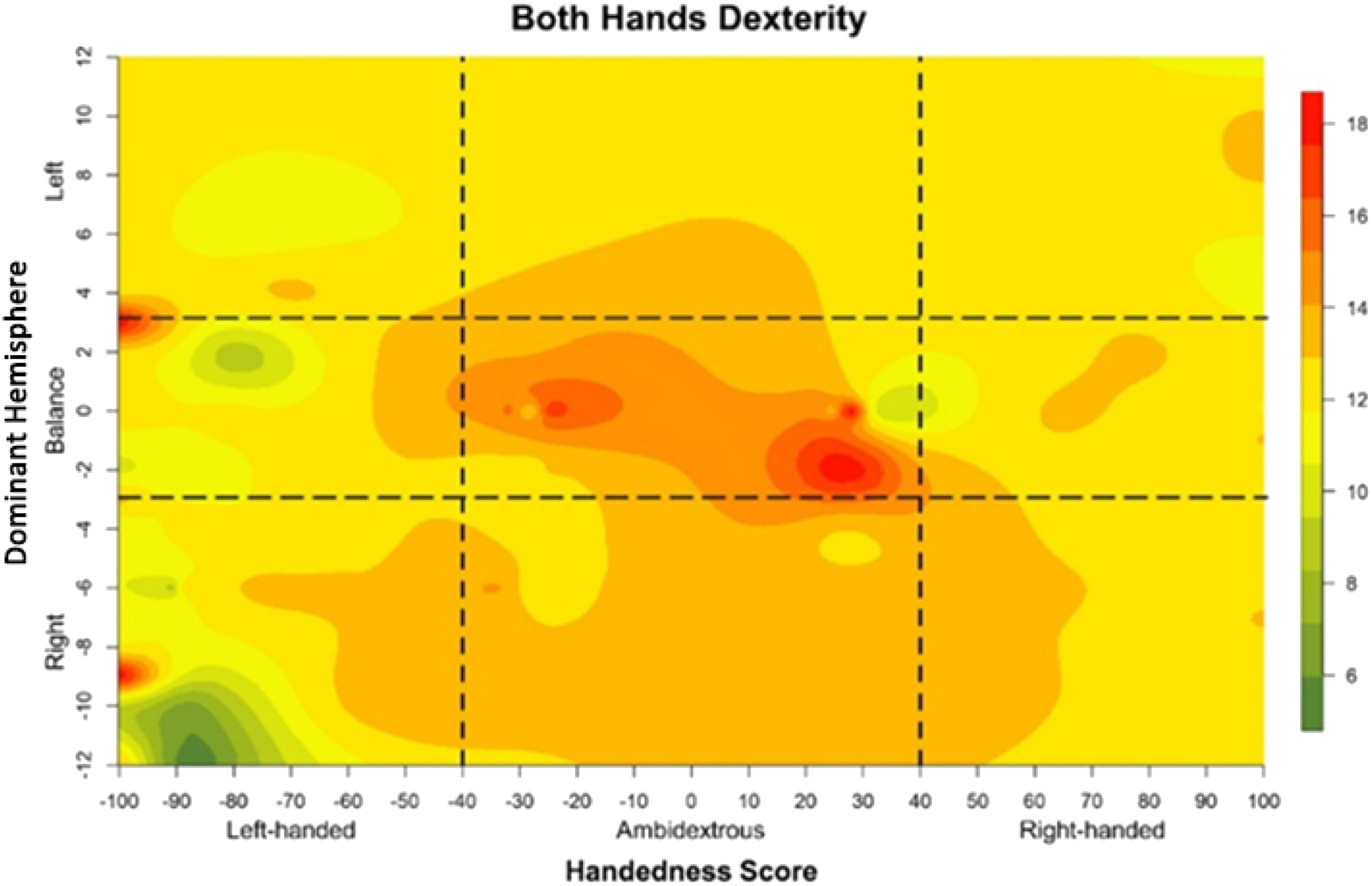

The color gradient in the heat maps illustrates levels of dexterity: darker shades indicate higher values, whereas lighter shades indicate lower values. This visualization facilitates the identification of patterns across groups, such as right-handed, left-handed, and mixed-handed participants, and their associations with hemispheric dominance and interhemispheric balance. For right-hand dexterity (Figure 1), the mean (SD) was 14.03 (2.89); range 5–22. The distribution indicates that right-handed participants with right-hemispheric dominance show the highest dexterity scores. This pattern indicates greater right-hand dexterity in profiles with right-lateralized dominance.
For left-hand dexterity (Figure 2), the mean and standard deviation were 14.34 and 2.14, respectively, similar to those of the right hand. The map shows an inverse distribution compared to the right-hand dexterity, with left-handed individuals and those with right-hemispheric dominance exhibiting higher dexterity scores. This reinforces the notion that left-handed individuals, especially those with right-hemispheric dominance, perform better with the left hand.
In terms of both-hands dexterity (Figure 3), the mean and standard deviation were 12.09 and 1.87 units. The highest scores were observed among mixed-handed/ambidextrous individuals with balanced hemispheric dominance. The heat map for both hands highlights the advantage of balanced brain hemispheric dominance in achieving superior bilateral dexterity.
In the assembly dexterity heat map (Figure 4), higher scores cluster among mixed-handed/ambidextrous participants with balanced hemispheric dominance, indicating a pattern consistent with more effective performance in profiles characterized by interhemispheric balance.
Discussion
In this study of 182 adults, we examined the role of handedness and hemispheric dominance in manual performance and found significant effects of both handedness and sex on dexterity and grip strength. Right-handed participants demonstrated superior dexterity in the right hand relative to left- and mixed-handed individuals, while no group differences were observed for left-hand dexterity. Given that classification was based on preference inventories rather than objective performance, the category of “mixed-handed/ambidextrous” most likely included a substantial number of mixed-handed participants. These participants typically show low overall preference and select hands depending on the task, rather than demonstrating equal proficiency with both hands across all activities. With respect to strength, left-handed participants showed higher bilateral grip strength with the difference in the right hand only marginally significant. In contrast, right-handed participants demonstrated superior pinch strength in the right hand compared with the other groups. Taken together, these findings underscore the contribution of handedness to both strength and dexterity and support the routine incorporation of handedness assessment into individualized rehabilitation planning.
Although most outcomes did not differ significantly across hemispheric dominance categories, a marginal association emerged between assembly dexterity and balanced hemispheric dominance. In addition, exploratory heat-map analyses illustrated lateralized patterns within handedness strata: among right-handed participants, those classified with right-hemisphere dominance tended to show higher right-hand dexterity; among left-handed participants with right-hemisphere dominance, left-hand dexterity tended to be higher. These patterns should be interpreted cautiously and in the context of sampling variability and the indirect nature of the dominance measure; nevertheless, they are consistent with the view that inter-hemispheric balance, rather than strict unilateral dominance, may better support complex, multi-component actions (such as the assembly subtest) that integrate sequencing, visuospatial guidance and elements of bimanual coordination.
From a clinical perspective, clinicians should document handedness (EHI categories) and inferred hemispheric dominance at baseline to interpret grip/pinch (kgf) and Purdue Pegboard performance beyond default dominant-hand norms. In mixed-handed patients, practice may profitably emphasize bilateral, task-specific training with intentional hand assignment and alternation; in strongly lateralized patients, treatment can leverage dominant-side strengths while systematically training precision and endurance of the non-dominant hand. For complex activities of daily living (ADLs) and work tasks, programs should include bimanual coordination drills and careful task sequencing. Education in ergonomics such as hand selection, task rotation, and tool layout can also reduce strain. Progress is best monitored with both strength tests and all Pegboard subtests. Therapists should also acknowledge the potential roles of hemispheric dominance and inter-hemispheric balance when formulating rehabilitation plans, particularly where performance profiles appear atypical for handedness.
Sex also affected performance profiles in this cohort. Men and women differed in handedness distribution and in dominant-hand dexterity and grip strength, with men generally exhibiting higher grip strength. Previous studies have similarly shown that men tend to exhibit greater grip strength in both hands7,29 while sex-related differences in dexterity have also been noted. 4 Pediatric research further indicates that developmental and hormonal factors may shape these patterns over time. For instance, girls are often reported to perform better than boys on dexterity tasks, whereas boys generally demonstrate stronger grip strength. Other reports found no sex effect on hand dominance 30 or on fine motor skills, 11 possibly reflecting methodological differences (preference vs functional tests), sampling characteristics and the relatively low force demands of fine-motor tasks. Clinically, sex-sensitive programming may therefore be warranted. For example, relatively higher intensity or frequency for strength goals in male patients and targeted bilateral strengthening and dexterity training in female patients, so that dosage and content are matched to individual profiles.
Regarding hemispheric dominance distributions in our cohort, right- and left-handed participants appeared to differ: for example, in the overall sample, 47.3% were classified as right-hemispheric dominant, whereas left-handers displayed a more varied pattern. While classification here relies on a neurobehavioral inventory, prior behavioral and neuroimaging evidence links hemispheric asymmetries and corticospinal organization to manual skill,5,18,19 providing a plausible substrate for the observed behavioral asymmetries. Consistent with dynamic-dominance accounts of motor control, 31 the dominant hand may specialize in dynamic, feedforward aspects of control, whereas the non-dominant hand contributes more to stabilization and state regulation. This framework helps explain the advantages observed in dominant-hand pinch or dexterity among right-handers and the comparatively balanced bilateral patterns among mixed-handed participants. Our findings indicate that mixed-handed participants with balanced hemispheric dominance performed better on complex multicomponent tasks, such as assembly dexterity. This result is consistent with accounts that emphasize distributed or bilateral control in skilled action and with studies showing that balanced interhemispheric engagement supports spatial processing and motor control. 19
Not all findings in the literature converge on the same pattern. Some studies report greater dominant-hand grip strength regardless of handedness.7,29 In contrast, our cohort showed higher bilateral grip strength among left-handers, although the right-hand advantage reached only marginal significance.
Divergences across studies are likely due to differences in participant characteristics—such as age distribution and gender ratio—as well as methodological variation in measurement protocols and in classification thresholds for handedness. Similarly, while certain studies emphasize structural or connectivity differences that could be linked to manual performance,5,32 others underscore variability and task dependence, particularly for skilled or multicomponent actions. These discrepancies highlight three priorities: using standardized units such as kgf, reporting clear thresholds for handedness classification, and considering task complexity when comparing studies. They also underline the need for transparent reporting of exact P-values, effect sizes, and confidence intervals.
Several clinical and methodological considerations follow from these results. First, a combined evaluation of handedness and hemispheric dominance, including their potential interaction, offers a more comprehensive framework for rehabilitation planning than considering each factor in isolation. This is particularly relevant for patients with atypical dominance profiles or suspected interhemispheric imbalance. These patients could benefit from interventions designed to improve bilateral coordination and promote interhemispheric integration, particularly in activities of daily living and in occupational tasks requiring fine precision and spatial accuracy. Second, in light of the variability observed across handedness groups and between sexes, future research should seek to include larger and more demographically diverse samples. It should also employ multimodal measures of lateralization that combine behavioral testing, neurophysiological metrics, and structural or functional neuroimaging, and adopt longitudinal designs to examine how training modifies lateralized performance and whether these changes generalize to ADLs and work. Third, wherever possible, studies should harmonize dynamometry posture/position/instructions and Purdue Pegboard administration to facilitate comparability across cohorts. Finally, while individualized programs have been associated with improved motor performance and greater independence in daily activities, 33 the present observational findings highlight the value of tailoring training content and dosage to lateralized strengths and task demands rather than implying causal superiority of any single protocol.
In summary, the study confirms that handedness is a major determinant of manual ability, while balanced hemispheric involvement appears especially important for complex dexterity. Integrating these factors into evaluation and rehabilitation strategies may accelerate recovery and promote functional independence.
Suggestions for future research
Larger and more demographically diverse samples, coupled with broader measurement batteries, are needed to improve generalizability and precision. Future studies should move beyond preference inventories and employ direct indices of lateralization, including EEG, fMRI, DTI, and TMS. This approach can more precisely define hemispheric dominance and help distinguish truly mixed-handed/ambidextrous individuals from those who are mixed-handed on the basis of task-dependent hand use. Because lateralization effects are task-dependent, upcoming work should include complex, skilled and bimanual actions in addition to simple measures of grip and pegboard performance and should harmonize dynamometry (posture/position/instructions, unit reporting in kgf) and dexterity-testing protocols across sites.
Methodologically, longitudinal and interventional designs are warranted to test whether training that targets bilateral coordination or leverages lateralized strengths produces durable gains that transfer to activities of daily living and work. Stratified sampling across EHI categories (right-, left-, mixed-handed) and dominance profiles will help ensure adequate power for subgroup analyses, including age-by-sex interactions. To reduce residual confounding, future studies should measure and adjust for hand anthropometrics, occupational exposures, habitual physical activity and comorbidities. Finally, pre-specified analyses with a priori power calculations and transparent reporting of exact P-values, effect sizes and confidence intervals, will facilitate comparability and cumulative evidence building.
Study limitations
Several limitations warrant consideration. First, the sample was recruited from a single geographic region and was modest in size (n = 182), which may limit generalizability. Second, the design was cross-sectional, precluding causal inference regarding relationships among handedness, hemispheric dominance and performance. Third, hemispheric dominance was inferred from a neurobehavioral preference inventory rather than from direct neurophysiological or neuroimaging measures; this indirect approach may result in misclassification, thereby conflating mixed-handed individuals with truly mixed-handed/ambidextrous persons. Handgrip dynamometry and the Purdue Pegboard Test were administered in accordance with standard protocols. Nevertheless, unmeasured covariates such as hand anthropometric characteristics, occupational exposures, habitual physical activity and comorbidities may have influenced outcomes. Finally, some effects were only marginal. Future studies should therefore report exact P-values, effect sizes, and confidence intervals, and should recruit larger and more diverse cohorts. It would also be valuable to use multimodal indices of lateralization such as EEG, fMRI, or DTI in longitudinal designs to test whether findings generalize to daily and work activities.
Conclusions
This study indicates that handedness is significantly associated with differences in hand dexterity and grip strength, whereas hemispheric dominance showed largely non-significant effects, with a marginal association observed for assembly dexterity. Right-handed participants demonstrated superior dexterity in the dominant (right) hand; left-handed participants exhibited greater bilateral grip strength, with the right-hand difference marginal. Participants categorized as mixed-handed/ambidextrous tended to perform better on bilateral and assembly tasks. These patterns, together with observed sex differences, are consistent with neurobehavioral accounts of lateralization and support individualized rehabilitation that explicitly considers handedness and hemispheric dominance, with attention to potential benefits of balanced hemispheric dominance for complex, multi-component coordination.
The observed variability in motor performance underscores the need for broader demographic sampling and direct indices of lateralization in future work. Prospective studies should examine age-by-sex interactions, standardize dynamometry and dexterity testing protocols and evaluate whether training that targets lateralized strengths and bilateral coordination produces durable gains in functional independence.
Footnotes
Acknowledgements
The authors thank the staff and students of Hamadan University of Medical Sciences for their support in participant recruitment and data collection. Special thanks to the Vice-Chancellor for Research and Technology for their financial support.
Informed consent
Written informed consent was obtained from all participants.
Ethical approval
Approved by the Ethics Committee of Hamadan University of Medical Sciences (Approval Code: IR.UMSHA.REC.1402.700).
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the Vice-Chancellor for Research and Technology at Hamadan University of Medical Sciences under the grant number 1402112410251.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.