
Abstract
Introduction
Kinesio tape is an alternative non-surgical treatment approach for addressing symptoms of carpal tunnel syndrome. The purpose of the study was to investigate individuals’ experiences with the dorsal application of Kinesio tape for carpal tunnel syndrome management and its impact on pain and function.
Method
The study design was a limited phenomenological design study embedded in a randomized controlled trial. Daily symptom journals and semi-structured interviews were completed with 15 participants who were purposefully recruited and randomly allocated to the intervention group of a single blind randomized controlled trial. Kinesio tape was applied dorsally on the affected forearm, wrist, and digits for a duration of two weeks. Transcribed data were analyzed using descriptive coding, coding schemes, and frequency charts to identify emerging themes.
Results
Three themes emerged: Kinesio tape was positively perceived to be effective on decreasing pain, increasing self-efficacy, and improving daily functional performance on tasks previously avoided or abandoned. The most common problem identified was maintaining Kinesio tape on the hands and fingers, to which the majority of participants expressed a desire to learn application.
Discussion
Results of this study suggest that Kinesio tape is a positively perceived intervention for decreasing pain and increasing function for individuals with carpal tunnel syndrome and warrants further consideration as an alternative conservative intervention for carpal tunnel syndrome.
Introduction
Carpal tunnel syndrome (CTS) is the most common neuropathy of the hand; it causes pain and disability, and affects approximately 22 million individuals in the United States alone. 1 In the past 10 years, there has been a 5% increase in proportion of population needing care for upper extremity (UE) musculoskeletal disorders, including CTS.1,2 However, less than 2% of the US National Institute for Health budget is allocated to researching solutions for these disorders, which limits the number of comprehensive studies available to inform therapeutic interventions for conditions such as CTS. 3
Individuals with CTS commonly experience symptoms of pain, numbness, burning, and weakness of the forearm, wrist, and hands. 4 Moreover, loss of participation in meaningful occupations of self-care, work, and leisure frequently impacts their quality of life, functional performance, and mastery over their environments. 4 Symptoms of CTS can be intermittent and individuals with CTS often delay seeking skilled treatment, with options ranging from conservative treatments to surgical interventions. 5 In one study 30% of individuals experienced a return of symptoms following surgical intervention. 6 One effective non-surgical intervention for long-term relief of CTS symptoms is a combination of orthoses with lumbrical exercises. 7 However, there are no standardized protocols for the management and treatment of CTS and a number of studies have found that client compliance and adherence to orthotic wearing schedules and exercise routines is limited.8–10 Additionally, there is no evidence for how to increase client adherence to these interventions over time, nor is there consensus regarding which type of orthotic design to use or what wearing schedule is most effective.4,8–10
The need to find alternative non-surgical interventions that may improve client adherence and thereby reduce symptoms for the effective management of CTS has led to a range of clinical investigations, including Kinesio tape.
Kinesio tape is applied to the skin creating improved muscle contraction, increased circulation of blood and lymphatic fluid, activation of an endogenous analgesic system which inhibits nociceptive pain impulses, and musculoskeletal correction.11–13 Emerging evidence is suggestive for the use of Kinesio taping for individuals with CTS, with studies indicating improvements in symptoms, function, and physiologic parameters similar to that of other modalities such as low-power laser treatments.14,15 Moreover, although CTS is the third most studied diagnosis for distal upper limb rehabilitation less than five percent of studies have explored patient experiences using qualitative methods. 16 Such studies are needed to better answer clinical questions regarding successful intervention options, the impact of self-efficacy on performance, and adapted responses to environmental tasks. In the absence of recent evidence regarding perceptions of interventions for CTS outside of surgical interventions, and no evidence regarding perceptions of Kinesio tape as a treatment option, there is a need to further explore and understand individuals’ experiences when using Kinesio tape. Learning the perspectives of individuals using Kinesio tape for CTS may provide insight regarding functional performance, sense of self-efficacy, and likelihood of follow through with the intervention.
The purpose of this qualitative study was to investigate how participants experiencing CTS in a single blind randomized controlled trial (RCT) using a dorsal application of Kinesio tape on wrist extensors perceived the Kinesio tape intervention and if changes in functional performance were noted. Understanding the perspectives of individuals using Kinesio tape for CTS may provide needed insight regarding the therapeutic potential of Kinesio tape as an alternative intervention for CTS.
Methods
This was a qualitative study embedded within a RCT and employed a limited phenomenological research design. Phenomenology is a qualitative approach used to describe how people experience a specific phenomenon, 17 which in this study was the perceived effect and experiences of individuals with CTS who wore Kinesio tape. Further, this study’s qualitative design reflects the constructivist paradigm which recognizes that personal experiences are realities that are context dependent, idiographic, and can vary from person to person. 17 Though the qualitative study could have employed a case study method; the initial purpose of this study was to explore individual experiences related to wearing the Kinesio tape within a short time frame and in whatever context the participants completed their daily life tasks. Data for this qualitative study were obtained through a demographic questionnaire, direct self-report on daily symptom journals, and face-to-face semi-structured interviews conducted at the conclusion of the intervention period.
Participants
Participants for the RCT were recruited from the general population in Southern California by advertising at public facilities, clinics, common public places, snowball sampling as well as social media following approval from the Institutional Review Board. To be included in the study participants were adults over 18 years of age and fluent in English who reported symptoms of CTS and demonstrated a positive Phalen’s Test or Tinel’s Test. 18 Qualifying symptoms of CTS included pain, numbness, and tingling of the forearm, wrist, or hand within the median nerve distribution. Exclusion criteria included undergoing current treatment for CTS, a history of surgical carpal tunnel release, an allergy to adhesives, compromised skin integrity, or past history of traumatic event, surgery, or congenital impairment of the forearm, wrist, or hand. In addition, individuals with the following conditions were excluded: pregnancy, diabetes not controlled by medication, radiculopathy (e.g., cervical radiculopathy, diabetic radiculopathy), and thoracic outlet syndrome. Signed informed consent was obtained from all participants prior to the study. Individuals randomized to the Intervention Group were asked to volunteer for a face-to-face recorded semi-structured interview of approximately 30 minutes immediately following enrollment in the study in order to capture the perceptions of the use of Kinesio tape, none declined. Of the 44 adults who participated in the single blind RCT, 15 were randomized to the intervention group (i.e., Kinesio tape), and participated in the interviews which are the focus of this paper.
Data collection
Three intervention groups were part of a randomized controlled trial examining the efficacy of the dorsal application of Kinesio tape for CTS: A Sham Group with a 4 inch strip of Kinesio tape applied to the participant’s shoulder worn continuously between visits (scapular spine), the Intervention Group with Kinesio tape applied to the dorsal surface of the forearm, wrist, and digits one and five and worn continuously between visits, and the Splint Protocol group assigned to wear a wrist cock-up splint nightly or as able and lumbrical stretching exercises throughout the day. A total of 68 participant wrists (44 participants) were in the study.
Study procedures consisted of completing a demographic questionnaire, obtaining baseline and subsequent measurements of grip and pinch, completion of pain scale questionnaires, the Boston Carpal Tunnel Questionnaire, 19 and application of the intervention. Participants were encouraged to record daily activities, pain ratings, and perceptions of the Kinesio tape while completing functional tasks within the context of their daily lives in symptom journals. The symptom journal was collected at each of the subsequent meetings during the intervention period. The journals were a means of capturing the daily experiences of the participants. Symptom journals were transcribed and entered verbatim alongside the interview transcription onto an Excel spreadsheet, no data were missing.
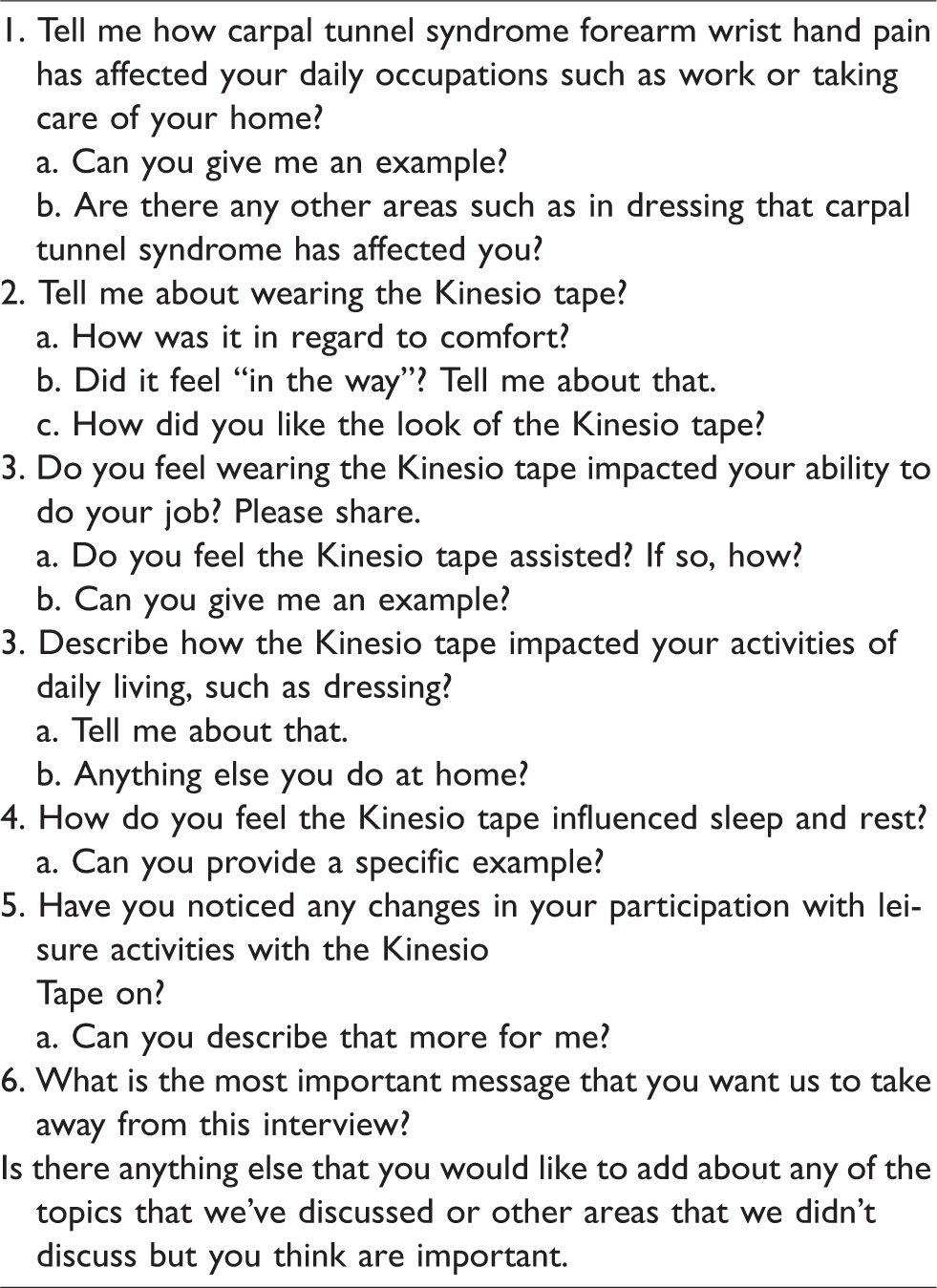
The use of semi-structured interview questions guided the conversation while still allowing participants to raise other important issues. 20 Interviews were guided by the Theory of Occupational Adaptation, 21 in which occupational performance is described as one’s ability to perform daily activities, and will be referred to as functional performance. This framework focuses on the person, the environment, and the interaction of the two; and for which successful performance or mastery of a task requires adaptation of either the person (internal mastery) or the environment (external mastery). 21 Six open ended questions were asked, such as “Tell me about wearing the Kinesio tape?,” with follow-up questions under each question and centered around understanding the experience of wearing the Kinesio tape and its impact or effect on pain and functional performance (see Table 1). Interviews were conducted from February 2018 to October 2018, lasting approximately 30 min, ranging 9 to 61 min. Interviews were recorded and transcribed verbatim. All participants had equivalent levels of participation, except those who wrote or spoke more than others in the symptom journals or interviews.
Semi-structured interview guide.
Data analysis
Data analysis followed a modified grounded theory procedural approach as the intent was to answer specific research questions related to understanding participant’s experiences wearing the Kinesio tape for CTS, if Kinesio tape had an effect on functional performance, and the perceived effectiveness of Kinesio tape as an intervention. 22
Participants were coded with pseudonyms and all qualitative data from the interviews, demographic questionnaire, and symptom journals were managed through a computer assisted qualitative data analysis software (CAQDAS), Dedoose (Version 8.0.35). 23 Descriptive coding was applied to analyze the data. 20 Three researchers coded the transcripts independently, followed by two of the researchers clarifying and confirming the codes. The same two researchers continued to condense the codes by developing coding schemes and applying frequency mapping and code co-occurrence within Dedoose, to identify categories until the emerging themes were identified and consensus reached. The symptom journals provided indirect daily responses from participants while the interviews provided direct responses at the end of the study.
The same researcher, a registered occupational therapist with advanced certification in Kinesio Taping, proposed the study, completed the tape application, and conducted the post semi-structured interviews. In this way rapport and familiarity developed between the researcher and the participants; however, this also presented opportunity for response bias. In order to mitigate for researcher and response bias, open-ended questions were asked in the interviews, and both positive and negative aspects of participants’ experiences were collected, reported, and coded. Furthermore, interview and symptom journal content were independently coded by two researchers in addition to the interviewer. The daily symptom journals served as an indirect communication method to elicit natural responses without the researcher present. Dedoose was used to further address researcher bias by structuring the data analysis process.
Results
Fifteen participants were included in this study, 2 males and 13 females (see Table 2), who represented a wide age range from 23 years to 67 years with a median age of 29.5 years. The duration of CTS symptoms ranged from 6 months to 10 years between participants with two indicating symptoms of CTS, one for 10 years and the other 17 years.
Demographic characteristics of the participants at baseline.

aPercentages do not add to 100% due to missing data.
Three themes emerged: (1) Effect of Kinesio tape on pain, (2) Effect of Kinesio tape on functional performance, (3) Increased self-efficacy. Problems regarding the use of Kinesio tape for UE rehabilitation were also identified.
Impact of CTS on functional performance
Limited range of motion, pain, and weakness among other symptoms made it difficult for participants to engage in meaningful roles and increase self-efficacy. For example, CTS-related tension and decreased range of motion impacted Grace’s ability to engage daily activities. She commented, In general, I can’t bend my wrist, I’ll start getting an increase in pain, and that affects a lot of the daily things I do.
Daily tasks that were most commonly impacted were in the areas of work, leisure, self-care, and driving. Related to work, fourteen participants commented that working on the computer increased symptoms of CTS. Additionally, eight participants specifically identified writing required in their work and daily life as increasing symptoms of pain, numbness, and tingling. Impacted leisure activities included crafting, swimming, jogging, boxing, working out, doing bench presses, and yoga. In terms of self-care, respondents described dressing and household chores such as cleaning and meal preparation as activities noticeably impacted by CTS. Lastly, a significant majority of participants (n = 12) identified driving as impacted by CTS pain and numbness.
Effect of Kinesio tape on pain
Participants reported both immediate pain relief with Kinesio tape and increased pain relief over time even for those with chronic symptomology. Example statements include: [I felt] immediate relief with tape on [Joy], [The tape] made me feel stronger and helped the pain to go away, especially in my wrists [Sue], and I [noticed] I was rolling my wrists less to relieve the tension while working on stuff at the computer [Donna]. the tape felt like an extra support for my hands, especially while sleeping. [The] weeks I've been wearing the Kinesio tape, my pain is almost gone. I liked [the tape] and it made my hands feel like they were more open, whenever you put it on freshly, it felt super secure [Kay]. I think that in the middle of a flareup, that putting the Kinesio tape on can help reduce the pain from the flareup and get over it more quickly.
Impact of Kinesio tape on chronic pain
One of the surprise findings, came from four of the participants who having experienced CTS pain for 7.5–10 years reported Kinesio tape to be effective in decreasing pain. Lee commented, It’s not typical for me to go this long without symptoms. I can’t believe ‘zero pain, Valerie happily stated. My hands feel more relaxed and the pain is almost gone. Especially at night [with] very little discomfort on the wrists, which is all so new [Grace]. I was feeling pain on my palms and wrists throughout the day, which diminished right after tape was applied in the evening.
[I] felt immediate relief with the rigidity and application of Kinesio tape!
[My]wrist felt relief with new tape application [Molly]. My daily activities include driving, typing on my laptop, and writing, which commonly causes problems, but I do not feel pain or any tingly sensation, [I] haven’t felt it in a while since wearing the tape [Sue].
Effect of Kinesio tape on functional performance
The impact Kinesio tape had on pain translated to positive impact on daily life activities for 14 of the 15 participants who identified Kinesio tape as positive and effective, particularly on decreasing pain. The quicker the pain was gone, the more involvement and engagement participants reported. For example, Cinthia expressed,
When the tape was on it made me feel more at ease, that I was like Oh, I’m gonna feel less pain. And then, because there was less pain I was able to come out of my shell.
Kinesio tape helps to easily be aware when overextending [my wrist] to change position to avoid pain.
With the tape I'm just doing my normal activities and because it's not invasive I am able to do everything.
Work
Fourteen of the 15 participants reported a significant decrease in pain and increase in amount of time without pain during functional work-related activities such as using computers, small devices, and writing. Some participants reported being able to engage in these activities for three or more hours with zero pain while wearing the Kinesio tape. Sue explained, Usually I feel it is difficult to grip my pen for a long period of the time, but the tape helped open my hand and release some pressure from my wrist. So, I think that having the tape definitely helps to prevent symptoms from happening because I didn't experience any symptoms while I was at work, while I was wearing the tape.
Leisure
One third of the participants reported improved engagement in leisure activities while wearing Kinesio tape. They identified increased engagement in specific tasks such as holding a book while reading and manipulating their smart phones. They also identified increased engagement in high intensity, high repetition activities such as yoga, bouldering, working out, setting up a campsite, and playing the string bass. Lee found that she experienced less pain while practicing yoga and Molly felt stronger and climbed higher on the rock wall. In addition to these examples, two participants experienced an extended duration of participation in high intensity physical activities. Lee reported being able to hike and camp without pain.
I spent the day hiking and did not feel my hands swell and fill as usual. I was able to set up the campsite including grasping, twisting, and pulling without numbness or tingling with the tape on.
Functional tasks
In addition to work and leisure, participants reported being able to return to a wide array of functional tasks while wearing the Kinesio tape. These included daily tasks of personal care and home management to community activities such as running errands and driving a car. Being able to return to such basic life management tasks elicited positive emotional responses as well. Josey shared, I did cooking tasks yesterday, like whisking, without pain. That was wonderful!
With the tape I’m just doing my normal activities and because it’s not invasive I am able to do everything.
I vacuumed at one point and that was fine. I have not done that in a while, I let my husband to it because I always get a flareup after, except this time.
“I did not have any symptoms today, even though I painted the kitchen and ran errands”. Overall, however, the emphasis of the comments about returning to functional tasks was on the everyday activities that keep life going.
Some of the everyday tasks discussed extended into the community, such as driving and errands. Several (n = 12) participants reported a decrease in symptoms while driving and ability to drive for longer periods of time. Randi felt better even on short 20–40 min drives. Grace expressed surprise when reporting being able to drive 2 hours without pain when the tape was on. Now, I drove two hours to my mom’s home and noticed my arms and wrists did not feel tired, no pain on my palms and wrists.
Perceptions of wearing Kinesio tape
Together, all 15 participants made 219 positive comments regarding the wearing of Kinesio tape. They also commonly compared Kinesio tape to their experiences with wearing orthotic devices, and discussed both difficulties and recommendations related to the use of Kinesio tape.
Strength and stability
I’m a superhero with the tape on
said Derek when summarizing his perceptions of wearing Kinesio tape. While not every participant used such illustrative language, the majority of them expressed positive perceptions of the tape. I felt more stabilized [Kay], My hands feel stronger and supported [Grace]. I feel more support there, or
I don't feel [my wrists are] as weak as before
I think the tape worked great, [I felt] it helped my strength improve. I noticed when I did have the Kinesio tape on my left, I felt a lot better driving with it. I felt confident, it put my wrist where it should be
Tape not in the way
Participants liked wearing the Kinesio tape as it was comfortable, did not restrict movement or involvement in activities and tasks for daily living. I would always try to be so careful on the way I move my hands or position my hands so that pain would not increase, but with the tape, I'm just back to my normal. I don't have to be so conscious on the way I move my hands or rest my hands because the pain is almost gone [Valerie].
I liked that it was discreet.
It was like a second skin, so I could do what I wanted [Valerie],
As a student I spend a lot of time on the computer, and I think anything else would be in the way.
You can’t do things with those [splints] on, you can’t wash dishes or anything.
I was trying to do painting with the splint on but it wasn’t ideal so I had two choices, to not paint or paint and be in pain. I was able to paint while wearing the Kinesio tape and it helped hold my wrist in correct position and I did not have pain. I painted for six to eight or more hours a day, so this is really remarkable. Instead of seeing me as weak, like when I wear a splint, people saw the tape as something that is going to help you get stronger, like an active person trying to get better.
I am familiar with Kinesio tape from an athletic perspective, but had not considered it in a rehab context.
Problems with Kinesio tape
Two participants said they experienced
no change in pain or function [Donna], and
I don’t think it made a huge difference for me [Josey]. After we took it off, my skin was very sensitive to touch, it almost felt similar to when your foot is asleep, I would not leave it on the prescribed three days.
The tape came loose while exercising and I felt it got nasty. I wanted to be able to remove it and re-apply it.
If water or soap got under the finger strips they peeled and just did not adhere the same.
Tape was itchy, but better than an orthotic device.
Self-application request
All participants requested to learn the Kinesio tape application method, but only if trained first and received some education and protocols.
I think I do enjoy the feeling that it gives me, but I feel like I would probably change it every day, I wouldn’t wear it for three days
If I would have been able to take it off and redo it when it started peeling back I think that I would have loved to do that and [then] re-apply it on myself at home.
When issues of tape management arose, such as if it unraveled or lost adherence over the digits before returning to the lab, the participants stated a desire to contact the researcher for problem solving and guidance, though none of them did and waited for the next visit. Even in light of the problems encountered with using Kinesio tape on the hand, all 15 participants stated they would use the dorsal application of Kinesio tape again if someone showed them how.
Discussion
This study investigated the experiences of individuals with CTS and their perspectives on the dorsal application of Kinesio tape for symptom management and functional performance. The outcomes indicate perceptions regarding the use of Kinesio tape were positive and perceived as effective for decreasing symptoms of CTS and increasing self-efficacy. The primary implications noted in the data relate to the impact of CTS and Kinesio tape on functional performance and pain.
Occupational Adaptation framework
The Occupational Adaptation framework focuses on the person, the environment, and the interaction of the two. It emphasizes that successful performance of a task requires adaptation of either the person (internal mastery) or the environment (external mastery). 21 In this study, the dorsal application of Kinesio tape on the forearm, wrist, and fingers was an adaptation of the person that enabled increased functional performance in their environments.
Evidence suggests that Kinesio tape provides proprioceptive input which leads to increased action potentials in the cerebral cortex resulting in muscular co-contraction and joint stability.13,24 Participants commented that the Kinesio tape helped them feel as if their hand were stable and supported when in an open position, which is necessary for engaging in daily activities. The co-contraction provided by the tape may have contributed to the feeling of stability participants reported in the wrist, leading to increased engagement in functional tasks.
While the focus of non-surgical interventions for CTS has been on wearing orthoses and completing lumbrical exercises, functional performance is often inhibited. Orthoses have been shown to biomechanically position the wrist in neutral and relieve CTS symptoms, 7 but this intervention limits successful engagement with functional tasks, further limiting external mastery. Researchers have acknowledged this limitation and recommended alternative interventions in hand therapy which allow individuals to participate in meaningful activities.16,25–27 Kinesio tape is one such intervention, as it has been shown in this study to result in greater internal and external mastery.
External mastery
It is increasingly understood that symptom relief and return to function is the measure of success for interventions for musculoskeletal conditions of the hand, wrist, and forearm such as CTS. 28 This is consistent with the Occupational Adaptation framework concept of external mastery. There is growing evidence for using occupation-based assessment tools and intervention activities for therapeutic treatment of hand injuries.25,29–31 Jack and Estes 27 found that a holistic, client-centered, and occupation-based approach to the treatment of hand injures, resulted in improved patient outcomes. Similarly, Colaianni and Provident 26 found that such interventions increased client motivation, satisfaction and adherence, and promoted a faster functional recovery due to the relevance of the activities to the individual’s daily life and interests. Functional treatment activities increased confidence and decreased fear. Results of this study indicate that wearing the Kinesio tape increased client confidence and engagement in personal care, household activities, and community engagement. Several participants had a significant increase in the amount of time they were able to sustain their participation in activities, and others were able to return to high intensity, high repetition leisure activities. Most of the participants expressed symptom relief and improved function in self-care, home management, driving, work, community engagement, and/or leisure activities.
Internal mastery
Internal mastery, according to the Occupational Adaptation framework, is the belief in the ability to succeed in accomplishing a task, though adaptations of the person or environment may be needed for successful task completion. 21 The use of Kinesio tape to manage CTS symptoms is an adaptation to the person that has been shown to improve participant’s perceptions and report of external mastery in this study. Their response to the experiences of external mastery was to express the desire to learn to apply the tape themselves. The Occupational Adaptation model illustrates the interrelationship between internal and external mastery, showing how improvements in one lead to increases in the other in a cyclical manner. 21 In the case of wearing Kinesio tape for CTS, it appears that not only did Kinesio tape adaptation to the person lead to perceptions of increased self-efficacy and environmental mastery, but the improved external mastery also led back to a drive for increased internal mastery. This was evidenced by participants requesting to learn how to apply the tape themselves.
The need for an intervention that can be functionally integrated into daily life appealed to participants. They indicated that self-application of the Kinesio tape would allow them greater flexibility of wearing schedules. Being able to remove the tape for cosmetic concerns such as peeling edges, exposure to water or soap, following exercise, or due to skin sensitivity may enhance compliance with the use of the intervention. It is possible that being able to self-manage the dorsal application of Kinesio tape could improve adherence to the intervention, which is a known weakness of orthoses and exercises.7,8
It is recommended that application of Kinesio tape be overseen by a skilled professional, as clinical reasoning skills are necessary in order to ensure correct application and understanding of Kinesio tape properties, education, and problem management.
Implications for a younger demographic
It is possible, though not established, that the young average age of participants in this study reflects a societal trend toward CTS in younger people. Studies have identified that repetitive use of the fingers and wrist may contribute to symptoms of CTS. 32 Office workers who use computers 4 hours a day or more experience a high incidence of CTS.33,34 Furthermore, those who use computers and work for extended periods of time may be the primary at-risk population for CTS. This description may increasingly apply to young adults in screen culture.
Limitations
Limitations of the study include the application of Kinesio tape on first and fifth digits. The problems with tape adhering during activities that included water may have interfered with results. Participants were from Southern California and may not include other geographical or environmental challenges when wearing Kinesio tape for upper extremity rehabilitation. The sample was limited to the intervention Kinesio Tape Group of the RCT and therefore sampling was not continued through saturation.
Recommendations for future studies could focus on gathering participants perceptions over a longer period of time, perhaps including the experiences of individuals applying and using the tape. Other recommendations include gathering perspectives from participants in other geographical areas outside Southern California. Longer study duration for the comparative study between orthosis, orthosis types, and Kinesio tape are recommended as well.
Conclusions
Overall, participant’s perceived Kinesio tape as effective for decreasing pain, increasing self-efficacy, and daily functional performance improved, as demonstrated by successful engagement in work tasks, leisure activities, and functional activities including driving which had been avoided or abandoned. Problems were identified with maintaining Kinesio tape use on the hand and fingers, and consequently, learning self-application was recommended. The use of Kinesio tape allows for continued activity and participation in the environment and may be an option for therapists working in distal UE rehabilitation to consider, particularly the dorsal application of Kinesio tape for CTS.
Footnotes
Acknowledgements
Many thanks to the students and participants who volunteered their time with this study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received Funding was supported through Loma Linda University Allied Health Professions Dissertation grant not to exceed $4,000. The funders had no role in study design, data collection, and analysis, publication or preparation of the manuscript.
Informed consent
Signed informed consent was obtained from all participants prior to the study. Interview tapes, transcripts, and symptom journals are stored in a locked safe and under password protection. Participants’ identities were protected by removal of all identifiers and replaced with numbers at the start of the study. Names on all transcripts were also replaced with numbers at the start of the study to anonymize the analysis process.
Ethical approval
Internal Review Board approval through Loma Linda University, #5170437.
Guarantor
DCK.
Trial registration
The clinical trial was registered at ClinicalTrials.gov, #NCT03360344.
Contributorship
DCK completed the bulk of the research, literature review, data collection, analysis, and primary authorship. SR assisted with the bulk of data analysis and authorship. DK as the Advisor for the Dissertation Research Committee and assisted with data analysis, authorship, editing, and formatting. HJD conceived the study design. SCR and ND provided assist with study design, analysis, manuscript edits, and intellectual content. All authors reviewed and edited the manuscript and approved the final version of the manuscript.