
Abstract
Background
Qualitative studies following Brachial Plexus Injury (BPI) suggest that return to employment has a major influence on life satisfaction and psychological well-being. However, few studies have focused on return to work following BPI. The physical strain and intensity of an occupation may influence the ability of an individual to return to employment. This study aimed to provide information about the impact of workload intensity on employment status following BPI.
Methods
This is an observational, retrospective study of 74 participants who responded to a postal questionnaire, sharing information regarding their employment status pre- and post-BPI. The reported occupations were assessed for workload intensity and assigned a Reichsausschuss für Arbeitszeitermittlung (REFA) classification by two assessors.
Results
Forty-one out of 74 participants (57%) had to change their employment following their BPI. Changes in occupation were more likely if the pre-injury REFA score was 3 or 4 (n = 22). In the Complete plexus injury group (n = 8), 100% changed occupation. In the Partial plexus injury group (n = 66) 50% changed occupation. Hand dominance had no significant influence on change of employment (p = 0.37).
Conclusion
This study is the first to focus on the impact of BPI on employment status and workload intensity. Just over half the participants did not maintain the same employment following their BPI and one in five became unemployed. Future research should review the factors that contribute to the inability to return to work. This may direct enhancements in rehabilitation provision and enable healthcare services to focus on facilitating individuals back to the workplace.
Introduction
Brachial Plexus Injuries (BPI) have a profound effect on a person’s ability to use their affected upper limb. Successful outcomes are commonly associated with objective measurements of muscle strength; with the Medical Research Council (MRC) grade and muscle dynamometry being the most frequently reported.1,2 Typically, these studies examine isolated muscle strength, with the upper arm supported in a standardised position. When put in the context of everyday life, this information is not transferable to activities of daily living and does not consider the deficits in function that a loss of movement and sensation may contribute to. 3
Qualitative studies following BPI suggest that patients wish to return to ‘normal life’ with a return to employment being a major factor in their psychological health.4,5 However, few studies focus on return to work and none solely review occupation status including the physical requirements of employment. Those who report on return to employment suggest that only a minority of patients are able to return to work in a meaningful way. Interviews with patients who have been able to resume employment describe a positive impact on their psychological state by giving them a sense of purpose and life satisfaction.4,5 In these studies employment provided a feeling of ‘returning to a life role’ or being a ‘breadwinner’ within the family, additionally, it was recognised as a way to interact within an established social group.4,5 Other questionnaire studies report return to employment rates of between 45–54% within 1 year of injury.6,7 However, re-training and re-deployment are common features of this patient group with around 50% of those who returned to some kind of employment reportedly doing so in a new role or profession.6–8 Workload intensity and the physical strain which each occupation contains may be a contributing factor to those who are unable to return to their previous employment. To date, no studies have assessed workload intensity and return to work within a BPI cohort.
REFA classification of workload.

Methods
This observational cross-sectional study gathered information on employment status via a postal questionnaire among a cohort of patients who had suffered a BPI. This project gained approval by the NHS Research Ethics Review Board (ref: 20/SW/0081; IRAS Project ID: 281425). Informed written consent was gained from each participant.
Participants
The database of the host institution identified 1352 patients who had undergone surgical treatment for BPI since the commencement of the electronic database (13 years prior); of these 1203 met the inclusion criteria. It was considered unfeasible to contact this many individuals, therefore the decision was made to randomly select 10% of the overall sample. Using an online random number generator (www.random.org) 120 patients were identified for inclusion in the study.
Inclusion/Exclusion criteria
Patients over the age of 18 years (at the time of review) who had experienced a BPI were included in the study. Patients who sustained their injury at birth were excluded.
Data collection
A questionnaire (see Appendix 1) was developed which asked patients to report their occupational status and job title pre-and post-BPI. Patients were invited via letter to participate in the study. After a period of 8 weeks a second research pack was sent to those who had not responded, inviting them to participate in the study.
Occupation descriptions (job role/title) were entered into a database which was reviewed by two scorers (KK and RT) who were blinded to each other’s scores. The scorers consulted the Dictionary of Occupational Titles (www.occupationalinfo.org) and O*NET (www.occupationalinfo.org/onet) when reviewing the occupation to assign a REFA score. The scores were then returned to the first author (HB) for comparison. In the case of disagreement between scores, the results were unblinded and presented back to the scorers. The scorers were requested to discuss their results and come to a consensus.
All participant demographic information (including age, injury method and hand dominance) was obtained from their medical notes. The operation notes of the participants were reviewed by TQ and then classified according to the surgical findings. For analysis purposes the participants were divided into a) partial plexus injury (injuries to part of the plexus) and b) complete plexus injury group (those who had nerve roots C5-T1 injured).
Statistical analysis
Descriptive statistics were used to analyse patient characteristics. A weighted Kappa method was used for the analysis of inter-rater reliability for the REFA scoring between the two raters. Values are presented with corresponding 95% confidence intervals (CI). Kappa scores were interpreted using an adapted version of the criteria recommended by Landis and Koch. 16 A Chi-Squared test was undertaken to assess the difference in return to work between individuals with injuries to the dominant and non-dominant upper limbs.
Results
Participant characteristics.
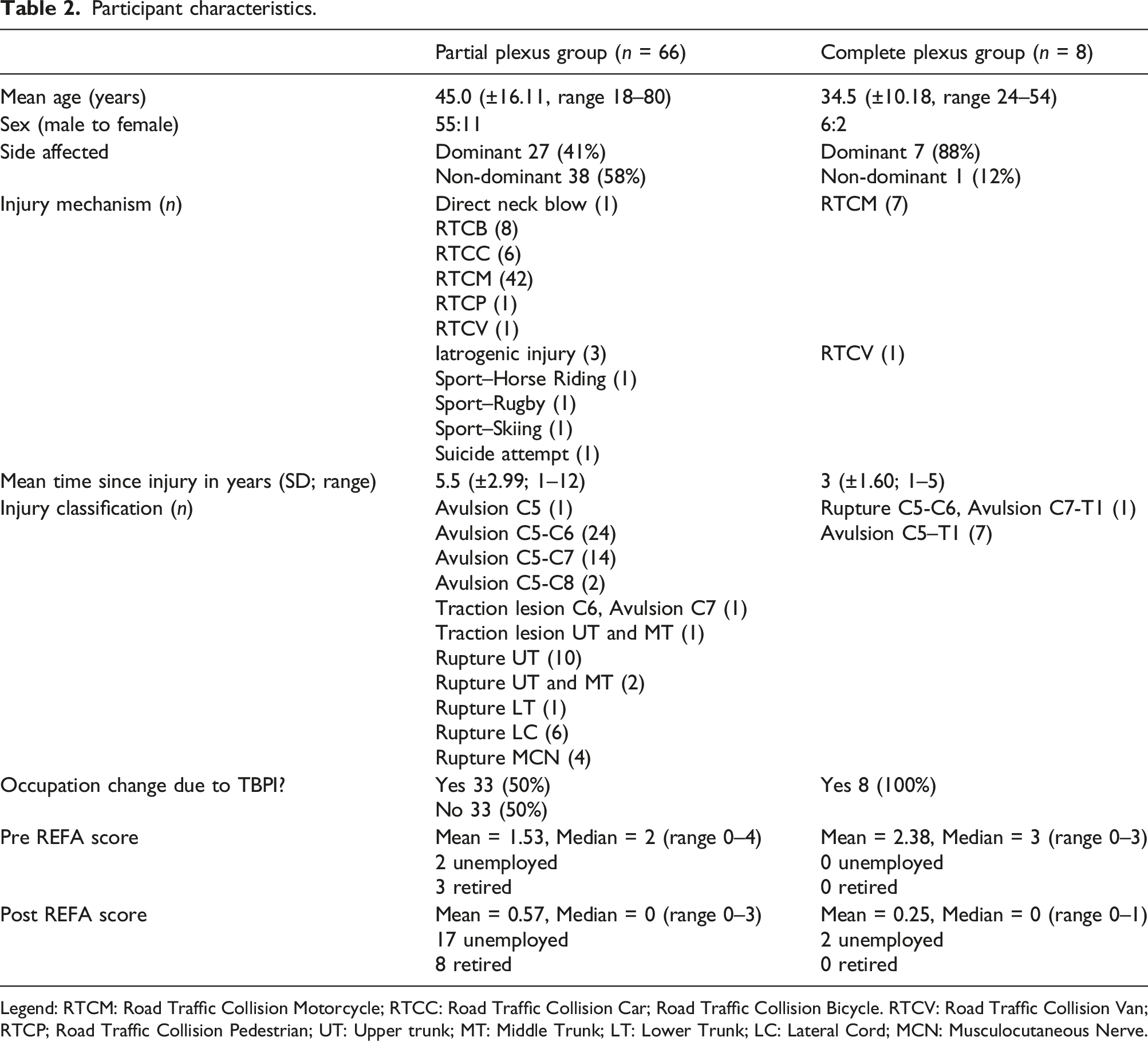
Legend: RTCM: Road Traffic Collision Motorcycle; RTCC: Road Traffic Collision Car; Road Traffic Collision Bicycle. RTCV: Road Traffic Collision Van; RTCP; Road Traffic Collision Pedestrian; UT: Upper trunk; MT: Middle Trunk; LT: Lower Trunk; LC: Lateral Cord; MCN: Musculocutaneous Nerve.
Occupational status and REFA scores
Thirty-three out of the total of 74 participants (43%) did not report that they had to change occupation due to their BPI. Of these, 18 (55%) had pre-injury REFA scores of 0. Three had REFA scores of 1, five had REFA scores of 2, one had a REFA score of 3 and one had a REFA score of 4. Two participants were unemployed at the time of their injury and three were retired.
Forty-one out of the total of 74 participants (57%) reported that they had not returned to their previous employment following their BPI. Three participants had pre-injury REFA scores of 4, 19 had pre-injury scores of 3, 12 had pre-injury scores of 2, one participant had a pre-injury score of 1 and 6 had pre-injury scores of 0. No participants reported themselves to be unemployed or retired pre-injury.
Nineteen out of the 41 participants (46%) were not able to maintain their pre-injury REFA score. Eight patients decreased their REFA score by 3 points, six decreased by 2 points and five decreased by 1 point.
Sixteen out of the 41 (40%) participants became unemployed secondary to their BPI; of these 8 (50%) had pre-injury REFA scores of 3 or 4. Three participants maintained the same REFA scores despite a change in occupation. Two participants became retired following their BPI. Figure 1 demonstrates the pre- and post-injury REFA scores. Sankey diagram of REFA scores pre and post injury.
Hand dominance and change of occupation
Thirty-four participants (46%) sustained injuries to their dominant arm and thirty-nine (51%) to their non-dominant arm. One patient reported themselves ambidextrous.
Of those, whose dominant arm was affected (n = 34) 21 (62%) reported that their injury had made them change their occupation. This difference is not statistically significant (p = 0.37). Median REFA pre-injury for the dominant arm group was 3 (mean 2.14, range 0–4), median post-injury was 0 (mean 1.9, range 0–1). 10 participants (29%) were not in employment (unemployed or retired) post-injury.
Of those whose non-dominant arm was affected (n = 39), 20 (51%) reported that their injury had made them change their occupation. Median REFA pre-injury was 2.5 (mean 2.4, range 0–4), median post-injury was 0 (mean 0.4, range 0–3). Nine participants were not in employment post-injury (23%).
Classification of injury
Sixty-six participants (55 male, 11 female) aged 18–80 years (mean 45.0 ± 16.11) were classified into a partial BPI group. Twenty-seven participants (41%) had injuries to their dominant arm. Thirty-three (50%) patients reported a change in occupation secondary to their BPI. Fourteen (21%) were unemployed and five (7.5%) retired after their injury. Median REFA pre-injury was 2 (mean 1.53, range 0–4), median REFA post-injury was 0 (mean 0.57, range 0–3).
Eight participants (6 male, 2 female) aged 24–54 years (mean 34.5 ± 10.18) had complete BPIs. Seven patients (88%) sustained injuries to their dominant arm. All eight patients in the complete BPI group (100%) reported that they had to change their occupation secondary to their BPI. Two were unemployed due to their injury (25%). Median REFA pre-injury was 3 (mean 2.38, range 0–3), median REFA post-injury was 0 (mean 0.25, range 0–1).
Inter-rater reliability for REFA between scorers
Out of the full list of 148 occupations (74 pre-injury plus 74 post-injury) raters' scores differed on 11 occasions. Between-rater agreement (weighted Kappa) was 0.93 (95% CI: 0.74–1.00) for the pre-injury REFA and 0.91 (95% CI: 0.69–1.00) for post-injury scores. These equate to ‘almost perfect’ agreement according to the adapted scale by Landis and Koch. 16
Discussion
This study represents the first focused assessment of the relationship between employment status and work intensity within the BPI literature. The findings from this study were slightly better than those of the existing literature in which around half of the individuals are reported to have returned to the workplace following BPI.5,6,7 In this study, only 28% (21/74) of the participants had not returned to work (including retired and claiming benefits) following their BPI. As might be predicted from clinical experience, the partial brachial plexus injury group demonstrated that 50% of respondents changed their occupation following their injury in comparison to 100% of those within the complete brachial plexus injury group. This correlates with the findings of Choi et al. 5 where 18 of 32 of their BPI patients had returned to work at the time of their study, with 10 of these reporting a change in jobs secondary to their injury. In a study by Kretschmer et al. 6 70% of the patients who had to undergo occupational retraining were in the complete plexus (C5-T1) group. Further comparisons are difficult to draw as previous studies only assessed return to work as a binary outcome (yes/no). In the present study, mean and median REFA scores were higher in the complete plexus group. This may indicate a tendency towards this group participating in occupations which are more physically demanding; however, it is recognised that the sample size of this group is small and further studies with larger samples would be required to confirm this.
The data created within this study provides information on associations (individuals attributing their change of occupation to their BPI) but cannot fully imply causation. Many of the participants suffered polytrauma, thereby other injuries may have influenced their capacity to be able to work. Further information was not sought by the participants as to the details of their change in employment status, retraining or time taken to return to work. The factors that lead to changes in employment are driven not just by physical health but also by a variety of other factors including social and psychological.17–19 Data were not collected regarding the presence of pain, coping strategies, function and litigation, which are also recognised as features that may prolong return to the workplace. 20 Recovery time following BPI may also be protracted as patients often require multiple surgeries to help to return to function in the upper limb. 4 This study included five patients who were 1 year post-injury. Three participants were in the partial plexus group and two in the complete plexus group. One participant was unemployed post-injury (previously a sales assistant) and another participant became fully retired (previously working part-time in agriculture). A further participant had become a student (studying trading), whereas a further two had become self-employed with computer-based work.
When participants are categorised according to whether their injury had affected their dominant or non-dominant limb the percentage of participants who were not in employment due to their BPI appears to be almost equal (48% in the dominant group and 45% in the non-dominant group). When reviewed in terms of whether the injury led to a change in occupation, 62% of those whose injuries affected their dominant arm reported a change compared to 51% of those whose non-dominant arm was injured. The difference was not statistically significant. Previous studies have also reported that hand dominance does not appear to influence return to work in a BPI cohort.7,20
In brain injury leading to hemiplegia or upper limb impairments vocational rehab is encouraged and recognised as a factor which contributes to increased post-injury employment rates.14,15 The structured way traumatic brain injuries, stroke and spinal cord injuries have developed nationally, in specialist centres has allowed this as a focus of rehabilitation. To the authors' knowledge, in-patient rehabilitation for BPI is presently only possible in one centre in the UK (for a 5-days inpatient stay). Most patients are managed in outpatient settings (hand therapy and physiotherapy), where access to assessment facilities (such as kitchen, bathroom, bedroom) is limited. Personalised, patient-focused care centring on returning to employment is practised by clinicians facilitating communication between patients and employers as well as focusing on individual work-based tasks and ergonomic advice. Aids and adaptations are also frequently discussed with patients with recommendations for patients to purchase. Future focus on clearer rehabilitation strategies and processes to enable BPI patients to return to employment could have beneficial effects for the individual, the provision of therapy services as well as wider societal gains. 21 In addition, the consideration and further identification of new, innovative, splints, supports and prostheses may also further improve the ability to return to work for those individuals with BPI.
In the group of individuals who did not report that their occupation had to change due to their BPI REFA scores were predominantly 0 (n = 18, 55%). This contrasts with the findings of those who did report a change in occupation where the pre-injury REFA scores were mostly 3 (n = 19, 46%). This may suggest that those individuals with higher REFA scores pre-injury may be more likely to have to find alternative employment with a lower workload intensity. Given the long-term symptoms of pain, decreased range of movement and fatigue that BPI patients frequently report, this is somewhat logical. Some participants within the no change group reported a change in occupational status which they did not attribute to their BPI. Two participants were students prior to their injury. Following this, they became employed and their REFA scores were 0 and 2 respectively. One participant reported a change in occupation, however, his pre- and post-injury scores were equal (REFA 2). Two participants retired and one became unemployed following their injury.
This is the first study to use the REFA classification system within a BPI cohort. Previously, the REFA system has been used to measure the capacity to work following upper-limb surgery.12,22 The present study findings demonstrated that of those 66 individuals who were employed pre-injury, 26 were able to maintain their REFA score of work-load intensity post injury. Of the 74 participants in this study, only two increased their REFA score following injury. The first was a college student pre-injury and subsequently moved to employment as a sound technician. The second did not report a change in their employment. However, the REFA score assigned by the raters differed pre- and post-injury. This is recognised as a flaw within the study methodology whereby the occupations were provided to the raters separately. Scores were only unblinded once unanimous agreement was sought for the 11 cases where the raters had scored differently. Other limitations of the study include the fact that this cohort is entirely composed of those who have undergone surgical management, therefore, it does not represent any milder injuries that have a more favourable prognosis and spontaneous recovery. In addition, this was a single-centre study, therefore the results may not be generalisable to those who have experienced a BPI throughout the whole of the UK or internationally. Finally, no information regarding the timescale of return to work following injury was sought from the participants. This information would have been useful to determine how long it took individuals to return to employment. Future studies should include this data to give a more accurate assessment of the features of returning to work and to help identify ways to improve vocational rehabilitation within this patient group.
Conclusion
This study is the first to focus on the impact of BPI on employment status, return to work and workload intensity. Just over half the participants did not maintain the same employment following their BPI and one in five became unemployed. Patients in the partial plexus group had a 50% change in occupation compared to 100% of those in the complete plexus group. Hand dominance was not a significant factor in returning to work. Individuals with higher pre-injury workload strain (REFA scores 3–4) tended to change occupation to a post-injury occupation with a lower workload intensity. Individuals with workload intensity scores of 0–1 were generally able to maintain the same employment post-injury. Further research into the contributing factors for these changes as well as the facilitators and barriers of returning to work is recommended.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.