
Abstract
Introduction
Patients with Severe Recessive Dystrophic Epidermolysis Bullosa (RDEB-S) develop hand contractures that progress over time and impact function and quality of life. The role of the Occupational Therapist includes hand assessment and interventions to help maintain function. We developed the Assessment of Hand Contractures in Epidermolysis Bullosa (ACE-EB) to facilitate sensitive and detailed assessment. The purpose of this article is to describe its development and use.
Methods
We undertook a literature search of existing hand assessments and evaluated their use for children with RDEB-S. Most measure contracture recurrence post-operatively and none was sensitive enough to capture emerging contractures seen in children. We developed the ACE-EB by adapting the most relevant existing assessments, to include specific component contracture measurements, a Hand Deformity Grade and a hand surgery Patient Reported Outcome Measure. We explored the validity by surveying clinicians in the field of Epidermolysis Bullosa and we tested the inter-rater reliability.
Results
We describe the development of the ACE-EB. The results of the validity survey showed most respondents agreed that the ACE-EB had sufficiently sensitive grading scales, included relevant aspects of hand assessment and was a useful clinical or research tool. Inter-rater reliability tests showed good strength of agreement.
Discussion
The ACE-EB is a novel clinical tool designed for use with children with RDEB-S. It can be used to monitor changes, track natural history of hand contractures, guide practice and serve as a post-operative outcome measure in children and adults. Further testing of its validity and reliability is required.
Introduction
Epidermolysis Bullosa (EB) is a group of rare, inherited skin disorders which are characterised by skin fragility and blistering. There are four major subtypes, each with different clinical features and a wide range of severity. This paper focuses on the severe subtype of Recessive Dystrophic Epidermolysis Bullosa (RDEB-S) which is associated with mucocutaneous blistering, chronic wounds, scarring, impaired nutrition and growth, anaemia and the development of aggressive cutaneous squamous cell carcinomas, which are the main cause of death in early adulthood. Children with RDEB-S are born without hand deformities. They develop contractures over time, resulting in severe hand function impairment. Contractures are characterised by skin and soft tissue shortening, causing web space and joint contractures of all digits, eventually leading to secondary bony changes. Hand assessment is complicated by the presence of blisters, wounds and dressings. The condition is painful and younger children may have difficulty complying with assessment. Hand therapy is provided to help delay the development of contractures, to monitor changes and to preserve function.
There is wide agreement in the literature that individuals with RDEB-S develop hand contractures during early childhood. The reported likelihood of developing hand contractures in this subtype of EB is 16% by the age of 1 year and 98% by the age of 20 years. 1 A systematic review 2 of the natural history of RDEB-S reported there was little information about the onset of hand deformity in the literature. However, many authors agree that hand contractures progress over time and have a significant impact on function and quality of life.3–9
Most existing EB hand contracture assessments were designed for baseline hand assessment pre-operatively and follow up of hand contracture recurrence post-operatively.3,10–15 We, the authors, have many years of shared clinical experience working with children with this rare condition. In our experience, EB hand assessments currently used in clinical practice are not sensitive enough to capture emerging and evolving contractures seen in young children with RDEB-S. This is particularly relevant in a paediatric setting, as children start life without hand contractures. We developed the Assessment of Hand Contractures in Epidermolysis Bullosa (ACE-EB) through our clinical practice, working with children with RDEB-S at one of the National Highly Specialised EB Centres in England. Occupational Therapy (OT) is one of many professions within the multi-disciplinary team (MDT) caring for these children at this centre. One of the OT roles is to assess children’s hands as they grow, provide hand therapy advice and treatment to help delay the progression of hand contractures, discuss the option of hand surgery and provide post-operative hand rehabilitation. The purpose of this article is to describe the development of the ACE-EB and its use in children with RDEB-S.
Methods
The evolution of the ACE-EB took place over many years during our clinical practice working with patients with RDEB-S. We became aware that the available assessments were not sensitive enough to capture early contracture development in children. Over time, we modified these assessments, reflecting on their usefulness and refining the format. There was, and still is, limited published information about the natural history of hand contracture development in RDEB-S, specifically the onset of individual component contractures affecting web spaces, finger flexion and thumb adduction. We needed a sensitive, valid and reliable hand assessment tool to document the natural history, inform families and add to the body of knowledge about this condition.
We undertook a comprehensive literature search to identify relevant EB hand contracture assessments, using Medline, CINAHL and Embase databases. We used the terms and key words “epidermolysis bullosa”, hand, dystroph* and contract* or deform*. Inclusion criteria included a specific and measurable EB hand contracture assessment. Exclusion criteria included non-English articles, those written before 1990 and those that did not specifically consider hand contracture assessment in EB. We did not exclude older articles as they remain relevant given the paucity of more recent articles describing hand assessment. We developed the ACE-EB by adapting existing EB hand assessments and we describe it in greater detail below. We explored its validity by surveying EB clinicians working across the four National Highly Specialised EB centres in England. We explored the inter-rater reliability of webspace and thumb adduction contracture assessment.
Results
Literature search
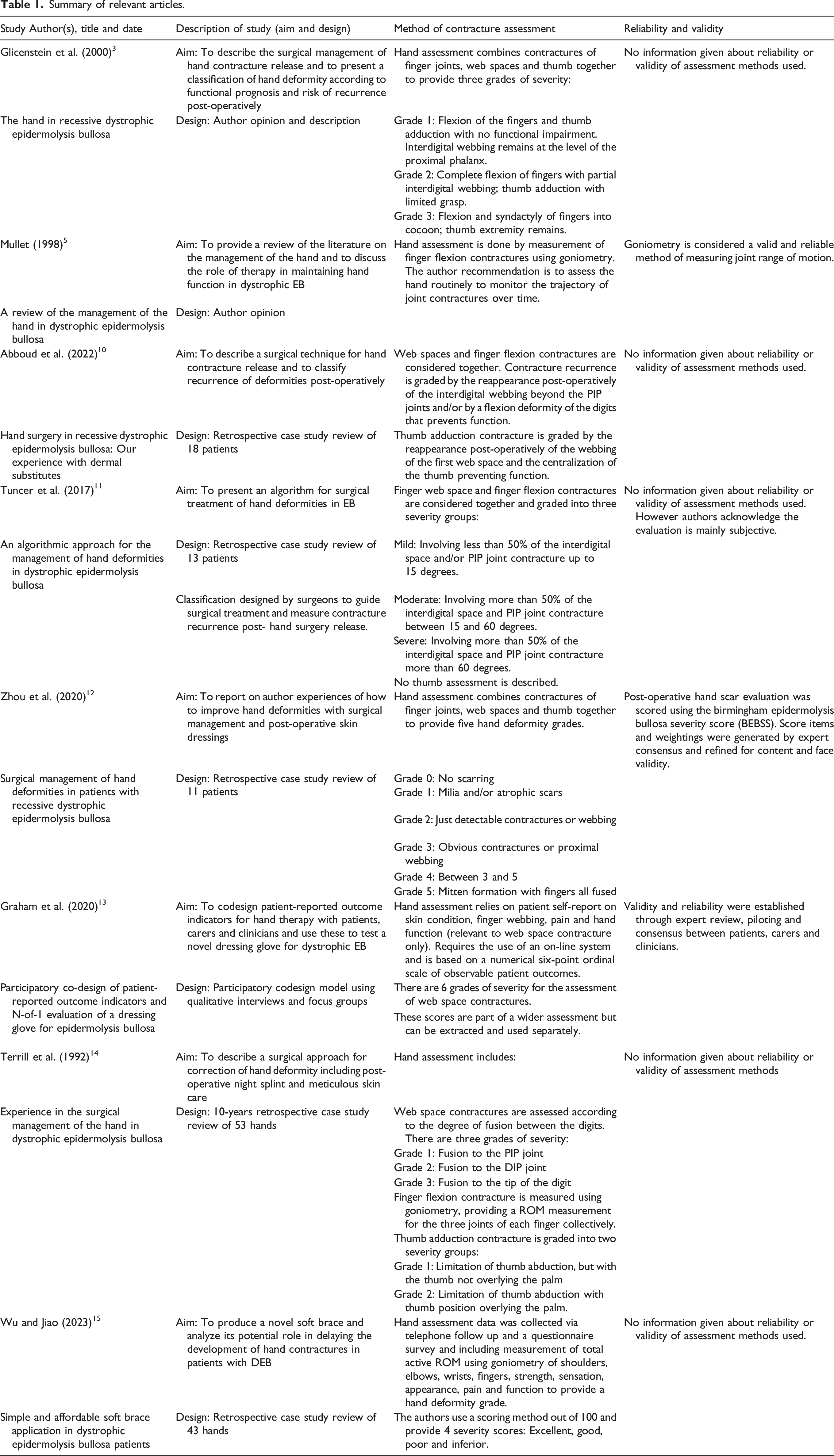
Summary of relevant articles.
The development of the ACE-EB
For many years, our hand assessment practice was based on two existing EB hand assessments; one by Terrill et al. 14 which measured and graded individual component contractures separately (web spaces, finger flexion and thumb adduction); and Glicenstein et al. 3 who combined the three components to provide a hand deformity grade. Both of these assessments lacked sensitivity, validity and reliability and were designed primarily for hand surgery outcome measurement. However, in our opinion they were the best available. Over time we modified and refined these two assessments to suit our paediatric patient group for both routine and post-operative reviews. This was an iterative process generating several versions of the ACE-EB over time. Our EB MDT members valued the information that was being generated by our use of the ACE-EB and we were encouraged to develop it further; this required testing of its validity and reliability and reviewing the literature for recent evidence. The literature search revealed newer assessments, which still lacked sensitivity, validity and reliability10,11,15 and/or did not measure all three contracture components separately.10–13 What was lacking was a clinical tool, intended for use with children to detect subtle and emerging hand contractures, that provided information about all three typical components separately, and also provided a whole hand deformity grade. Additionally, we needed the tool to be used in post-operative context to capture recurrence of hand contractures following surgical release.
Below we describe in detail the ACE-EB.
The ACE-EB has 4 parts:
Part A: Contracture Assessment measures hand, wrist and forearm contractures and provides a severity score for each of the three most typical hand contractures.
Part B: Hand Deformity Grade provides an overall impression of hand deformity using all the severity scores from Part A. This grade is used to summarise the severity of all contractures affecting the whole hand.
Part C: Reported Hand Care Routines records the patient’s use of hand splints, dressings and gloves.
Part D: Hand Surgery Patient Reported Outcome Measure reports on the patient/parent satisfaction with hand appearance and function following hand surgery.
Part A: Contracture Assessment
This section provides detailed measurements of the three hand contractures that are typically seen in children with RDEB-S including the 2nd to 4th finger web spaces, finger flexion and thumb adduction contractures. We also measure contractures affecting the wrist and forearm which usually develop in adolescence. We suggest photographing the child’s hands as this may support the assessment and help in the scoring process.
Web space contractures
Web space contracture (also known as pseudosyndactyly) is a typical feature of RDEB-S, where the skin between the fingers fuses progressively towards the fingertips, eventually forming a mitten-like deformity. Web space contracture is not present at birth and worsens over time especially where there is injury to the web spaces. It is different from congenital syndactyly, which is a non-progressive embryological failure of finger separation.
Early signs of web space contracture in children are subtle and can be difficult to recognise.4,5 In our practice, we assess the web spaces of children with RDEB-S from birth, to detect early changes and monitor their trajectory over time. We need an assessment sensitive enough to detect these small changes. Several studies3,10–12 describe assessments that combine web space contracture with finger flexion contracture and/or thumb contractures, and grade together. These assessments therefore are not able to detect small changes in only the web spaces.
Terrill et al.’s
14
web assessment is the most sensitive of those available and is not combined with other measurements of finger flexion or thumb abduction. It was originally a congenital syndactyly classification
16
and used to measure recurrence of web space contracture for EB patients following hand surgery. It has 3 levels of web space contracture, measured using the finger joints as landmarks. We adapted this assessment by increasing the number of gradations of contracture for each web space from 3 to 5. This provides greater sensitivity to detect subtle changes which are often overlooked in younger children. We designed a contracture key (Figure 1(A)) which uses the bones and joints of the adjacent fingers as landmarks to enable accurate and precise assessment. Using the contracture key to guide the assessment, the level of contracture for each web space is recorded on the diagram (Figure 1(B)). All three web space levels are added together to give a total of 0–15 for each hand. Web space Contracture Key (A) levels diagram (B) and web severity score (C).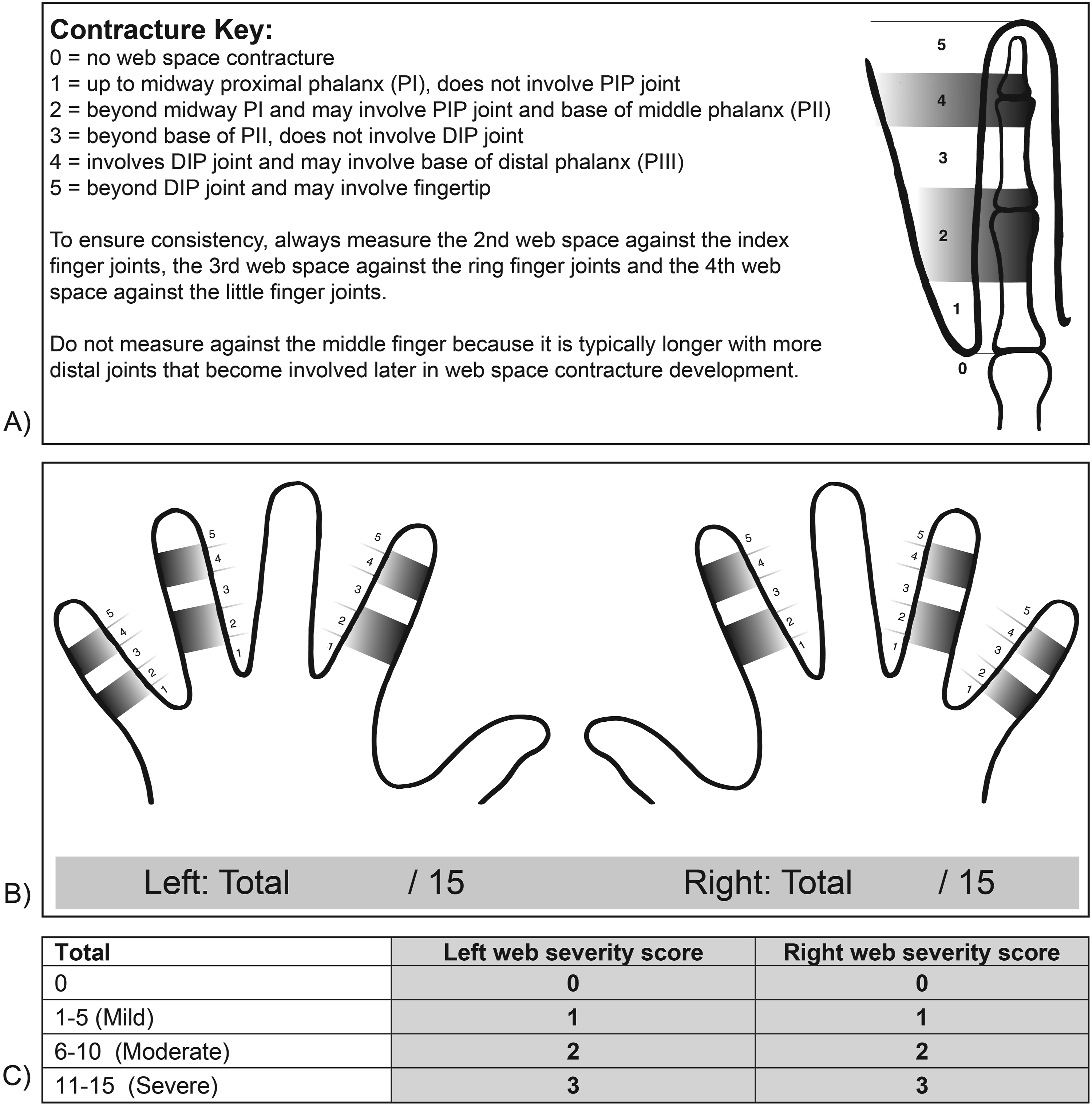
To summarise the measurements, we developed a web severity score from 0 to 3 to represent the severity of web contractures affecting the whole hand (Figure 1(C)). This was created by dividing the maximum score of 15 by three, so that 0 represents No contracture (severity score 0), 1–5 represents Mild contracture (severity score 1), 6–10 represents Moderate contracture (severity score 2) and 11–15 represents Severe contracture (severity score 3). The web severity score is used to calculate the Hand Deformity Grade in Part B.
Figure 2 is an example of a hand with Mild web severity score. This 11-year-old has a level 1 contracture of the 2nd web space, a level 2 contracture of the 3rd web space and a level 2 contracture of the 4th web space. These are added together to total 5, which is a Mild web severity score. Example of a hand with a mild web severity score.
Finger flexion contractures
In RDEB-S, finger flexion deformity begins with the soft tissues shortening on the palmar side of the hand, pulling the joints into a flexed position, limiting finger extension and reducing finger joint range of motion (ROM). As finger flexion contractures progress, the palmar skin may begin to ‘bridge’ across the joints. In severe cases this can lead to fusion of the fingertips to the palmar surface and eventually encasement of the whole hand in a ‘mitten-cocoon’ deformity. Alongside this process, the bones of the fingers become osteoporotic with radiological changes becoming evident, including thinning and hooking of the distal phalanges and bony resorption. 17 In the ACE-EB, bridging and palmar fusion is recorded but is not given a severity score or included in the Hand Deformity Grade in Part B.
Goniometry is a widely accepted, valid and reliable method of assessing finger joint ROM
18
and is used by clinicians treating patients with EB.5,14,15 In the ACE-EB, finger ROM is assessed using goniometry by an experienced therapist to ensure accuracy of measurement. Range of motion can be measured passively or actively. When active motion is measured, the child is required to cooperate with instructions. Performance is influenced by strength, pain, fatigue, understanding and compliance. We chose to record passive ROM, where the therapist physically moves the joint through its possible range. This does not require complete cooperation from the child and shows the full potential motion. Goniometry can be time consuming with individuals who have blisters,
19
bandages and pain. Where there are time or compliance constraints, we prioritise measuring the proximal interphalangeal (PIP) joints. These are the most accessible finger joints for accurate measurement as they are easier to identify than the distal interphalangeal (DIP) joints in a contracted hand and typically contract before the metacarpophalangeal (MCP) joints.4,5 In the ACE-EB, passive flexion and extension is recorded for all finger joints (Figure 3(A)). Passive ROM table (A) total degrees of PIP joint flexion contractures (B) and finger flexion severity score (C).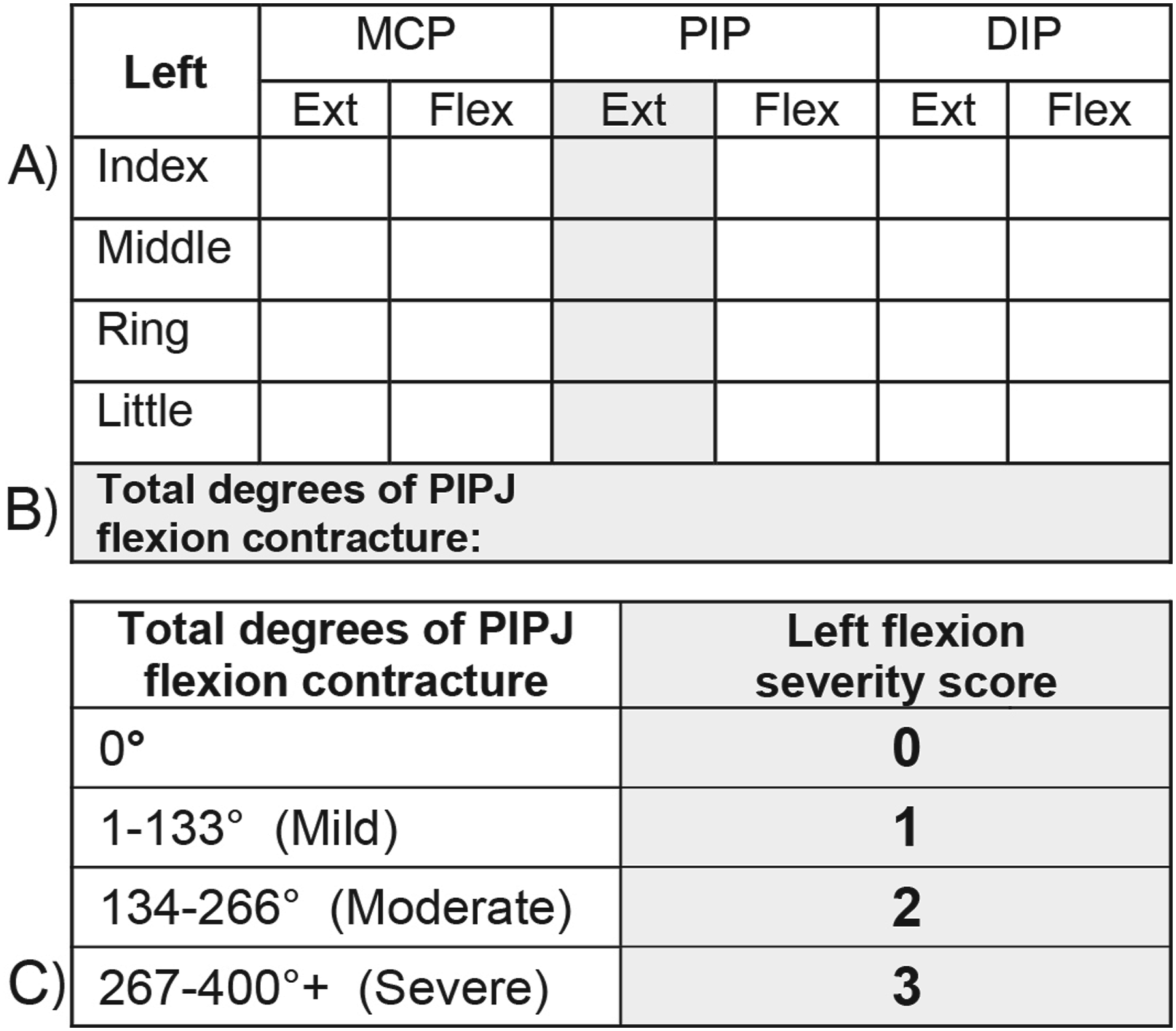
To summarise the ROM measurements, we developed a flexion severity score to represent the severity of finger flexion contractures affecting the whole hand. To calculate the flexion severity score, the extension deficit measurements (degrees of flexion contracture) of all PIP joints are added together (Figure 3(B)). Normal ROM for the PIP joints is 0-100 degrees 20 Therefore, we use 100 degrees as the maximum possible flexion contracture per finger, which equates to a potential 400 degrees for all 4 fingers when added together. This provides a single number representing the total degrees of PIP joint flexion contracture, for all fingers of each hand.
The flexion severity score range is from 0 to 3 and was created by dividing the maximum score of 400 degrees by three. Zero degrees of contracture represents No contracture (severity score 0); 1–133 degrees represents Mild contracture (severity score 1); 134–266 degrees represents Moderate contracture (severity score 2) and 267–400+ degrees represents Severe contracture (severity score 3). See Figure 3(C). The flexion severity score is used to calculate the Hand Deformity Grade in Part B.
Figure 4 is an example of a hand with Severe flexion severity score. This 8-year-old has flexion contractures of all fingers and skin bridging across the PIP joints of the little and ring fingers. The combined PIP joint flexion contracture scores of all four fingers is over 267 degrees which is a Severe flexion severity score. Example of a hand with a severe finger flexion severity score.
Thumb contracture
Thumb adduction contracture occurs as the soft tissues shorten and cause the carpometacarpal (CMC) joint to contract towards and across the palm. This causes the 1st web space to narrow. The thumb MCP and IP joints lose motion over time and may develop hyperextension to compensate for loss of abduction.
In the development of the ACE-EB, we adapted Terrill et al.’s
14
thumb classification which has three severity scores. To improve sensitivity, we increased the number of gradations from 3 to 4 and expanded the description to include CMC joint position and 1st webspace contracture (Figure 5). Unlike the web and flexion severity scores which require additional calculation, the thumb severity score is based on a single description and does not require further calculation. No contracture is represented by severity score 0, Mild contracture is represented by severity score 1, Moderate contractures is represented by severity score 2 and Severe contracture is represented by severity score 3. The thumb severity score is used to calculate the Hand Deformity Grade in Part B. Thumb adduction contracture descriptions and corresponding thumb severity score.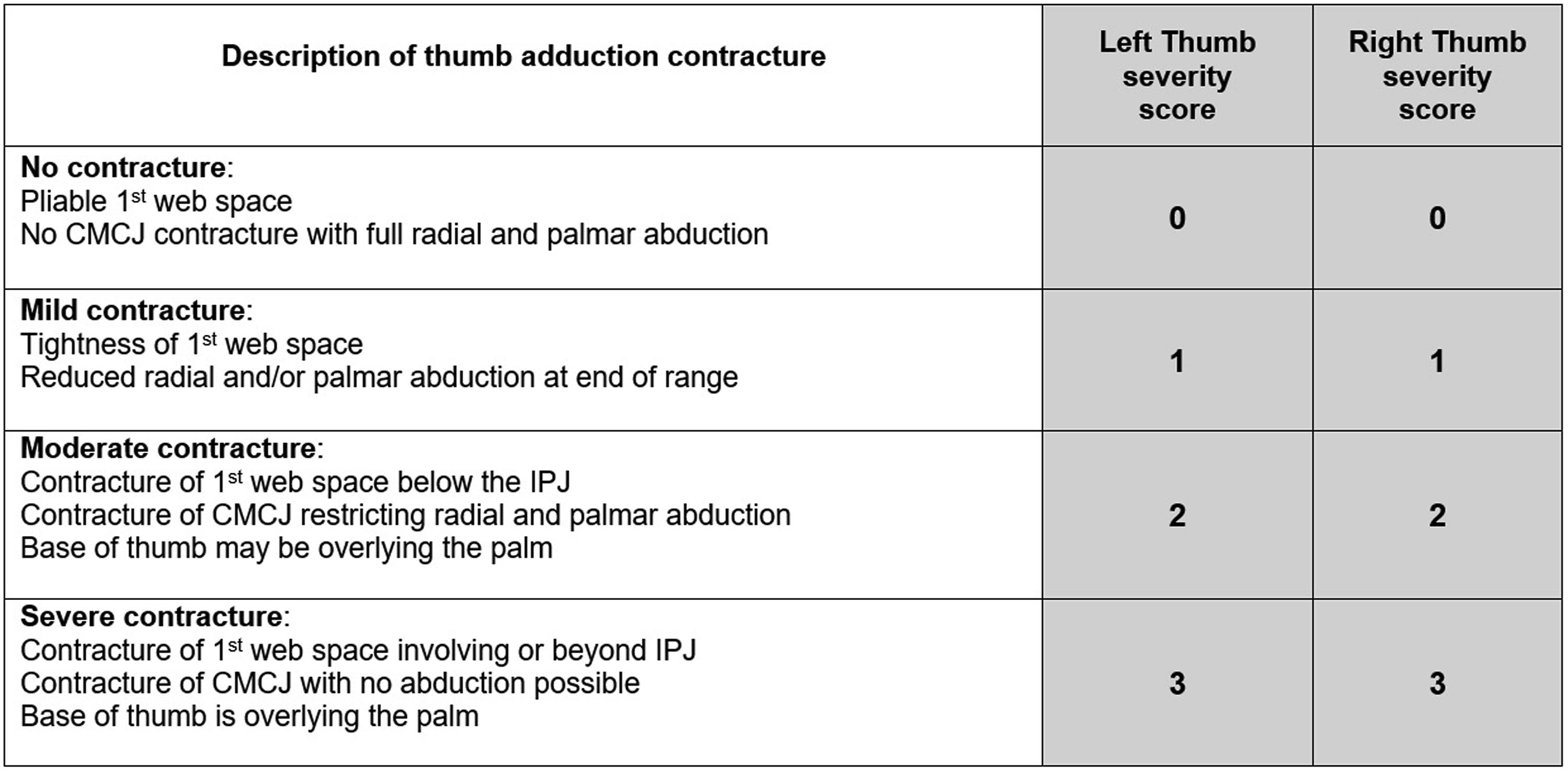
Figure 6 is an example of a hand with Moderate thumb severity score. This 8-year-old has a 1st web space contracture to below the IP joint, restriction of radial and palmar abduction and base of thumb overlying the palm. They have a Moderate thumb severity score. Example of a hand with a moderate thumb severity score.
Part B: The Hand Deformity Grade
Some studies3,12,15 describe a Hand Deformity Grade (HDG) which provides an overall impression of hand deformity. In the development of the ACE-EB, we also created a HDG which combines the component contracture measurements generated in Part A. It is used to summarise the deformities of each hand, to aid communication with colleagues and families and to guide clinical reasoning.
To calculate the HDG, we combine the three severity scores generated in Part A (see Figure 7). Each severity score ranges from 0 to 3 and when added together create a maximum of 9, thereby representing the three typical component contractures proportionately. The HDG score is converted into severity descriptions: A Mild HDG will have a severity score in one, two or all components. A Moderate HDG will have severity scores in at least two components and a Severe HDG will have severity scores in all three contracture components. Hand deformity grade.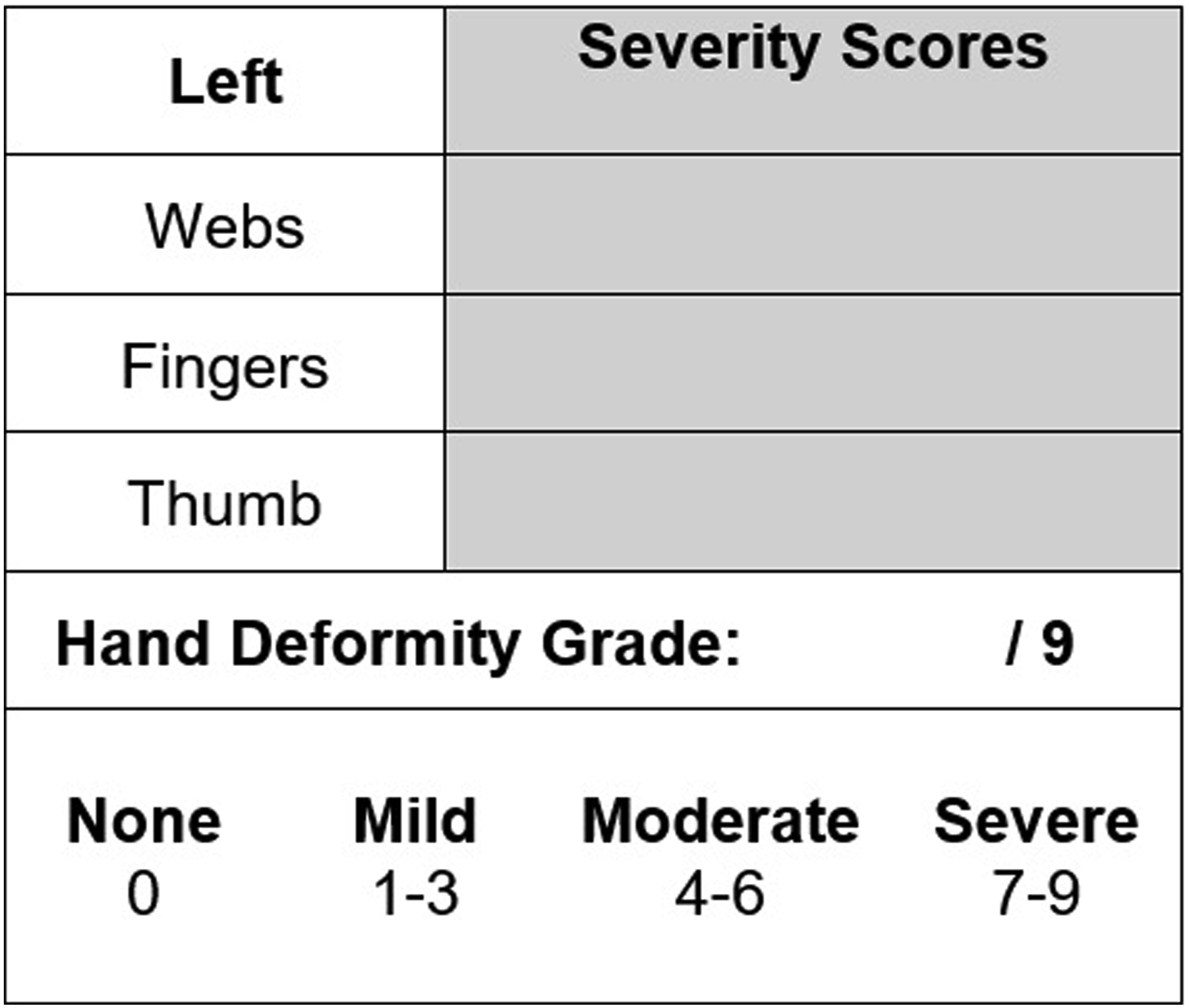
Figure 8 shows examples of each HDG: an 11-month-old with No contractures; a 5-year-old with Mild contractures; an 8-year-old with Moderate contractures and a 17-year-old with Severe contractures. Examples of hand deformity grades: None (A); mild (B); moderate (C) and severe (D).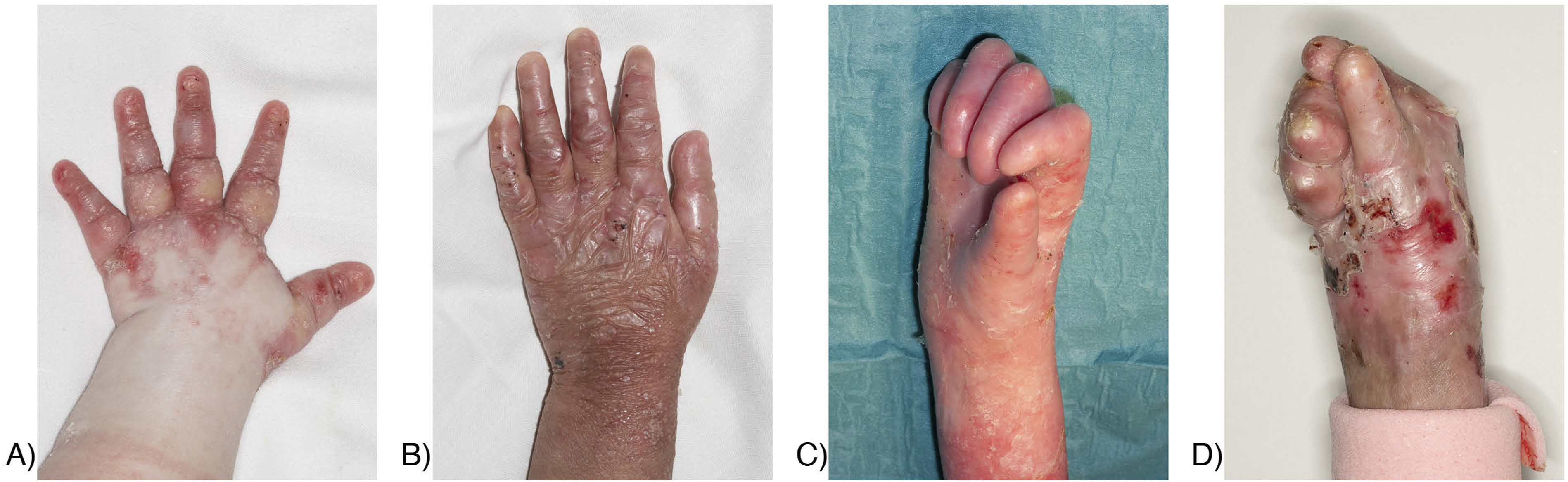
Part C: Reported Hand Care Routines
In this section of the ACE-EB, we record the patient’s reported usual hand care routines, including type and frequency of use of hands splints, web space bandaging and gloves. This information is important to document as part of the Occupational Therapist’s routine clinical review and to inform the MDT regarding the patient experience of these interventions.
Part D: Hand surgery – Patient Reported Outcome Measure
The ACE-EB Patient Reported Outcome Measure provides information regarding the level of satisfaction with surgical outcome from the patient’s perspective. We use a Likert scale to report patient or parent satisfaction with hand function and appearance following surgery. When used at specific time points alongside the objective contracture measurements from Part A, it provides comprehensive information on hand contracture recurrence post-operatively.
Validity
To explore the validity of the ACE-EB, we surveyed the opinion of all Hand Surgeons, Dermatologists and Occupational Therapists working across the four National Highly Specialised EB centres in England. We selected this group of professionals for our survey as we have regular meetings across the centres and well-established professional relationships. RDEB is an extremely rare condition, and our survey numbers reflect the small number of professionals available to approach for their opinion. We invited all 12 professionals with a caseload of patients with RDEB, and who are familiar with EB hand deformity, to participate in the content validity survey. The respondents were not asked to assess a patient using the ACE-EB before completing this survey, but rather to comment on its potential use. This was to simplify and expedite gaining feedback and to avoid obtaining ethical approval across various sites.
The survey consisted of 10 multiple choice questions relating to the content, sensitivity and clinical usefulness of the assessment with free-text space for additional comments. The Survey is available as a supplemental file. The response rate was 67% and included 4 Hand Surgeons, 2 Dermatologists and 2 Occupational Therapists.
We asked if the grading scales for web space, finger flexion and thumb adduction contracture in Part A were sufficiently sensitive and if instructions were easy to follow. Most respondents (87.5%) agreed that they were. One comment suggested MCPJ hyperextension should be noted when recording joint ROM and we adjusted the instructions to recognise this. Another comment suggested recording if bone reabsorption had occurred, however as x-ray would be required to confirm this, it is beyond the scope of the ACE-EB.
To generate the Hand Deformity Grade, we used the three severity scores from Part A to summarise and represent overall hand deformity. We chose this rationale so that all three components contribute proportionately to the HDG. In the survey we asked if the relevant components (the combined web space contracture score, the combined PIPJ joint contracture score and the thumb adduction score) were included. Six respondents (75%) agreed that they were. One respondent (12.5%) thought that MCP joint deformities should be considered and another (12.5%) thought the DIP joint deformities should be considered. We accept that MCP and DIP joint contractures occur and impact function. However, in our experience we have found that PIP joints typically contract first in young children and have the most impact on function. One of the advantages of the HDG is to offer assessors a quick way of capturing and summarising hand deformity. Thorough hand assessment can be difficult in young children with RDEB-S due to blisters, pain, compliance and competing medical appointments. Therefore, we chose the PIP joints to represent finger contracture; this allows the assessor to measure the most accessible joints, prioritise the joints that contract first and have the most impact on function.
All the survey respondents working with children reported they would use the ACE-EB in their practice. Those working with adults felt they were unlikely to use it as part of regular clinical review, as the adult population typically have more advanced contractures. We suggest that the ACE-EB has a role in pre-operative and post-operative hand assessment in paediatric and adult settings, however this question was not asked in the survey.
Reliability
We explored the inter-rater reliability of the web space assessment using the Web space Contracture Key and the thumb assessment using the Thumb adduction contracture descriptions. All study participants were children with RDEB-S and patients at our Highly Specialised EB Centre. Three raters were involved, all therapists with experience of working with children with RDEB-S.
The web space study involved two raters independently assessing 9 patients (18 hands) face-to-face over a three-week period. Written informed consent was obtained from individuals participating in this study. Kappa values ranged from 0.7 to 0.9 across the three web spaces indicating substantial strength of agreement.
The thumb study involved two raters independently rating 25 images of hands of patients with RDEB-S. All photographs were held on the hospital image database with consent for teaching purposes, therefore ethical approval was not required. The Kappa value was 0.58 indicating moderate strength of agreement.
The reliability of goniometry was not tested as this is a widely accepted method of joint ROM measurement, with accuracy dependent on the experience and skill of the therapist. 18
Discussion
There is currently no published study on the natural history of hand deformity in RDEB-S, nor are there appropriate standardised hand assessments. Existing EB hand assessments focus on pre- and post-operative measurements. We suggest that the ACE-EB is used as a clinical tool to monitor hand contracture development in young children and to measure the effectiveness of existing and future therapies. It can be used to gather information on the natural history, specifically when contractures first emerge, the sequence in which they occur and the rate at which they progress. Part A of the ACE-EB considers each component contracture separately (webs, flexion and thumb) and is more sensitive than existing assessments. We recognise that increasing gradations of web space contracture assessment may make it more difficult to distinguish between scores. Therefore, we developed the web space contracture key to define clear score boundaries and to improve the reliability of assessment. We recommend that assessors are experienced with hand bone and joint anatomy and use photographs to support their assessment.
The ACE-EB can also be used to track recurrence of deformity following hand surgery in children and adults. The Hand Surgery and Hand Therapy Clinical Practice Guideline for EB (2022) 9 report the consensus in the literature is that recurrence is inevitable, with the time frame between 2 and 5 years, although this is difficult to evidence without an accepted method of assessment and agreed intervals for measurement. Alongside the contracture assessment in Part A, the Patient Reported Outcome Measure in Part D provides essential information of the patient or parent’s satisfaction over time with the outcome of hand surgery.
Limitations
In our survey exploring the ACE-EB’s overall validity, we had a very small sample size of clinicians from the four Highly Specialised EB centres in England. RDEB-S is an extremely rare condition with limited number of health care professionals in this clinical area. While the survey response rate of 67% was good, the sample size was small and insufficient to confirm validity. Furthermore, the respondents were not asked to use the ACE-EB with patients, only to comment on its use theoretically; this limited the depth of information gathered from of the survey.
One of the limitations of the Hand Deformity Grade is the use of only the PIP joints for the severity score to represent finger contracture. While these typically are the joints that contract first in children with RDEB-S, we acknowledge that if the MCP and/or DIP joints contract before the PIP joints, then this will affect the validity of the HDG score.
In testing the reliability, we had a very small sample size of patients and only two raters. To demonstrate better validity and reliability of the ACE-EB, multicentre testing is required on a larger scale, with greater numbers of patients and assessors. Clinicians would need to use the ACE-EB with patients and report on their results.
Conclusion
RDEB-S is a rare and complex condition and hand assessment is challenging. The ACE-EB is a novel hand assessment for children with RDEB-S which can be used within clinical review as part of routine care and to track the natural history of hand deformity. It also has an important role as a surgical outcome measure to detect contracture recurrence post-operatively, and to assess the effectiveness of existing and future therapies and interventions. If used alongside age appropriate functional and quality of life assessments, it may help us to understand the impact of hand deformities more holistically. The ACE-EB is available as supplemental file.
Supplemental material
Supplemental material - Assessment of hand contractures in epidermolysis bullosa (ACE-EB): Describing the development of a novel hand assessment for children
Supplemental material for Assessment of hand contractures in epidermolysis bullosa (ACE-EB): Describing the development of a novel hand assessment for children by Nicky Jessop, Catherine Miller, Gill Smith, Gabriela Petrof, Anna E Martinez in Hand Therapy
Footnotes
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.