
Abstract
Plain language summary
In the clinical care of patients with Parkinson's disease (PD), dyspnea is a frequent symptom alongside the classic motor symptoms such as bradykinesia and rigidity. However, the underlying mechanisms of dyspnea in Parkinson's disease and how it is affected by dopaminergic medications like levodopa and dopamine agonists, which represent the mainstay treatment of motor symptoms in Parkinson's disease, are not yet fully understood. Various diagnostic tools exist to help clinicians evaluate patients with respiratory issues. In this case study, we report on the utilization of electromyography of the diaphragm, a previously not described diagnostic tool in the field of PD-related dyspnea, to study a patient with Parkinson's disease presenting with recurrent unexplained dyspnea when the dopaminergic medication wears off. We identified an altered sequence of respiratory motion, that is the contraction of diaphragm and excursion of the chest wall, during medication-off in this patient. We propose that the diaphragm-chest wall asynchrony, being a novel finding, likely leads to impaired mechanical output during breathing and contributes to the patient's experience of dyspnea when the medication wears off.
Dyspnea is frequently encountered in managing Parkinson's disease (PD), with an estimated prevalence between 11% to 40% in PD populations. 1 The underlying mechanisms and treatment approaches remain under ongoing study. 2 Here, we report on utilizing diaphragmatic electromyography (EMG) to investigate dyspnea in a PD patient in an effort to provide further insight into its pathophysiology.
A 69-year-old man with idiopathic PD diagnosed in his early fifties underwent bilateral globus pallidus interna (GPi) deep brain stimulation (DBS) five years ago. He had no relevant family history. His daily levodopa equivalent dose was approximately 2300 mg, 3 consisting of: levodopa/benserazide 200/50 mg five to six times daily at three-hour intervals during daytime; opicapone 50 mg at bedtime; amantadine 100 mg thrice daily; and a rotigotine patch 8 mg daily. Over the past year, he has experienced worsening motor fluctuations. Concurrently, he started suffering from recurrent, non-exertional shortness of breath described as “suffocation.” Breathing discomfort manifested primarily during early-morning “off-state,” lasting minutes to hours without clear triggers (Video S1), and resolved once he entered “on-state.” During dyspnea, peripheral oxygen saturation remained stable at around 98%. Medication-off spirometry indicated a mild restrictive ventilatory defect. Laboratory workups, including cardiac enzymes and serial electrocardiograms, were unremarkable. No concomitant choreo-dystonic movements were observed during dyspneic episodes.
To further investigate his unexplained dyspnea, we performed ultrasound-guided diaphragmatic needle EMG. The methodology followed the previously described protocol and is shown in detail in Supplementary Material (Figure S1). 4 An accelerometry sensor (sampling rate 100 kHz, band-pass filter 0.3–30 Hz; Sierra Summit, Cadwell Industries, Kennewick, WA) was affixed to xiphoid process to detect simultaneous respiratory chest wall motion. Figure 1 (and Figure S2 in Supplementary Material) illustrates the diaphragmatic EMG and chest wall accelerometry findings. In non-dyspneic medication-on state (Figure 1(a)), diaphragmatic contraction preceded inspiratory chest wall elevation and ended simultaneously with the start of expiratory chest wall relaxation. During a medication-off dyspneic event (Figure 1(b)), diaphragmatic contraction was delayed relative to inspiratory chest wall elevation and persisted during expiratory chest wall relaxation. This altered temporal relationship, or asynchrony, between diaphragm contraction and chest wall motion created a mechanical conflict, likely driving the patient's “off-state” dyspnea.
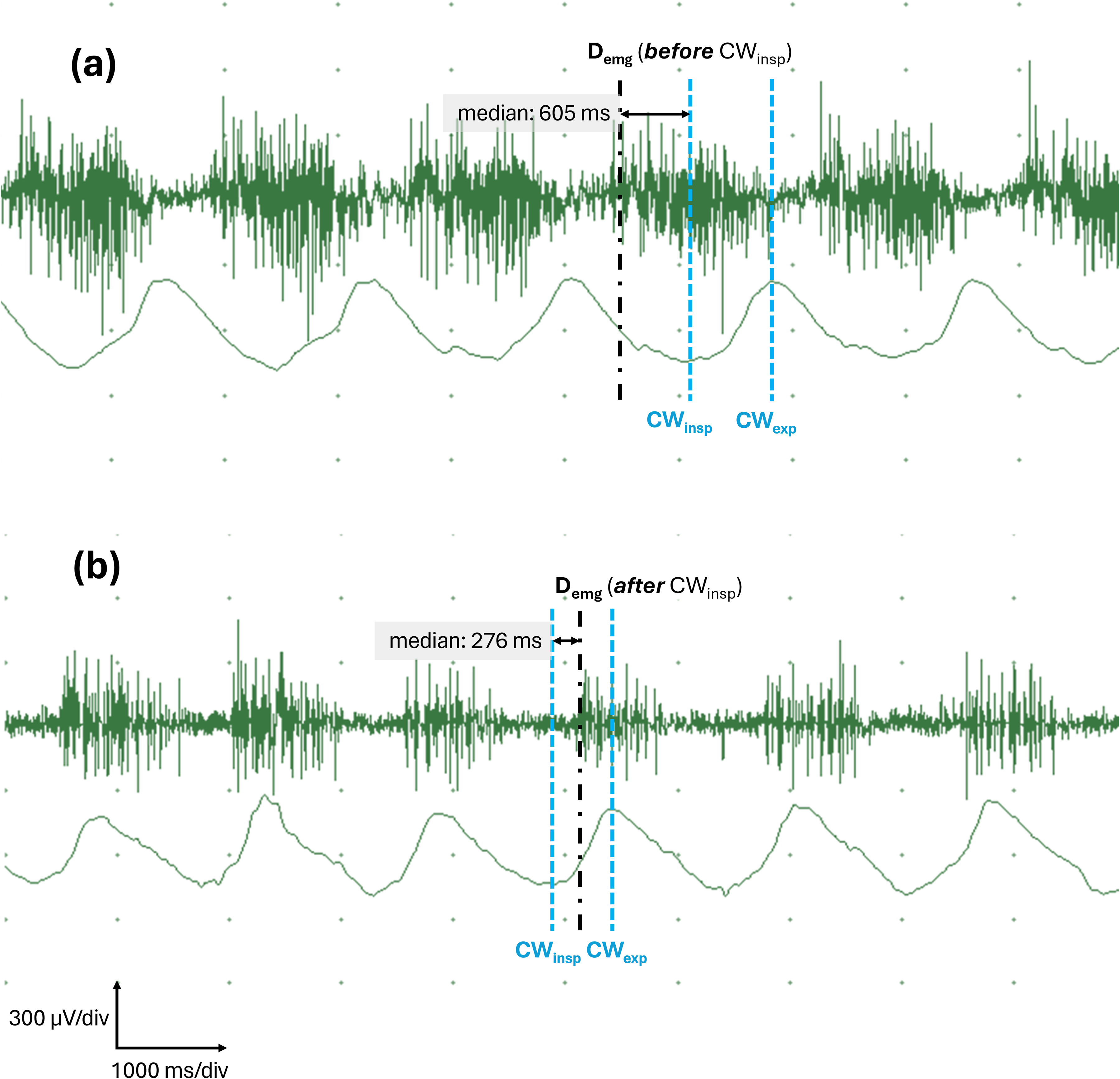
Representative diaphragmatic needle EMG findings during the medication-on state and a dyspneic episode in the medication-off state. The upper tracing in each panel displays the continuous diaphragmatic EMG recording, which shows regular bursts of diaphragmatic MUAPs in an incremental-decremental recruiting pattern. The lower tracing shows simultaneous chest wall motion recorded via accelerometry. (a) During the non-dyspneic medication-on state, the onset of diaphragmatic contraction (Demg, black dash-dot line) consistently preceded the corresponding inspiratory chest wall elevation (CWinsp, blue dashed line). Diaphragmatic EMG signals became silent at the onset of expiratory chest wall relaxation (CWexp), indicating cessation of diaphragmatic contraction. (b) During the dyspneic medication-off state, the temporal relationship between diaphragmatic contraction and chest wall motion was altered. Specifically, Demg lagged behind corresponding CWinsp, indicating a delay in diaphragmic contraction compared to the baseline in (a). Furthermore, diaphragmatic EMG signals persisted beyond CWexp, meaning persistent contraction of diaphragm despite the start of chest wall relaxation. Detailed quantification data are provided in Figure S2 in the Supplementary Material. Abbreviations: CWinsp, onset of chest wall inspiratory elevation; CWexp, onset of chest wall expiratory relaxation; Demg, onset of diaphragmatic EMG activity; div, division; ms, millisecond(s); MUAP: motor unit action potential; μV, microvolt(s).
Although adding safinamide 100 mg once daily improved his motor fluctuation, dyspnea remained. Similarly, adjusting DBS parameters yielded limited dyspnea relief. The respiratory symptoms were alleviated by 200 mg of levodopa or a rescue dose of subcutaneous apomorphine.
Dyspnea in PD is often attributed to restrictive ventilatory dysfunction resulting from bradykinesia and rigidity of the respiratory and upper airway musculature.1,5 Central mechanisms have also been proposed, including impaired drive and dysregulated respiratory muscle coordination due to PD pathology involving brainstem respiratory groups.1,6,7 While a case-control study identified irregular tidal breathing and prolonged inspiratory time in early-stage PD suggesting an altered breathing control, 8 these findings could not be definitely correlated with subjective dyspnea.
The impact of dopaminergic therapy on PD dyspnea remains heterogenous (Table S1). Levodopa benefits respiratory function by variable mechanisms such as mitigating restrictive deficits and enhancing both strength and endurance of respiratory musculature in some reports. However, subjective symptoms improvement was not always documented. Others, however, demonstrated that dopaminergic therapy would reduce subjective dyspnea and improve motor symptoms without significantly altering pulmonary function or respiratory muscle strength (see Supplementary Material for full references). Levodopa may, conversely, deteriorate respiratory symptoms or parameters.9,10 A study utilizing inductance plethysmography revealed ribcage-abdominal asynchrony during medication-on state, being thought to be related to levodopa-induced dyskinesia. 11 Interpreting these data requires caution, as PD-related central ventilatory impairments, motor symptoms, and challenge of performing maximal effort maneuvers during pulmonary function testing could confound measurements. Additionally, objective parameters do not always correlate with subjective symptoms. Moreover, brief examinations may not capture the dynamic daily respiratory demands.2,8
Our findings support the concept of respiratory incoordination in PD. At baseline, we recorded a normal diaphragmatic activation pattern where its contraction occurred in tandem with thoracic excursion, consistent with existing literature. 12 During dyspnea, however, the temporal relationship between diaphragmatic contraction and chest wall motion was disrupted, while there was no significant change in the duration of inspiratory and expiratory chest wall motion. As diaphragm is the primary inspiratory driver, 13 its delayed contraction likely contributes to the patient's perceived inadequate inspiratory effort. Furthermore, persistent diaphragmatic contraction during expiratory chest wall relaxation may impede effective exhalation. This asynchrony normalized following levodopa administration, coinciding with symptomatic improvement. A dyskinetic origin is unlikely, given the absence of accompanying limb/trunk choreo-dystonia or spasmodic dysphonia during dyspneic episodes and the lack of response to GPi-DBS adjustments. A primary neuromuscular disorder is also not likely due to the absence of intrinsic EMG abnormalities and the remarkable relief provided by dopaminergic therapy. While dyspnea can occur with subthalamic nucleus DBS, 14 it is rare with GPi stimulation; crucially, our patient's symptoms persisted despite device adjustment or temporary deactivation.
We postulate that central respiratory incoordination was the primary pathophysiological driver in this case, which was mitigated by robust dopaminergic activation. Optimizing levodopa therapy seems to be a reasonable approach for similar patients, particularly when dyspnea is associated with medication-off state. As such, we suggest that clinicians treating PD dyspnea carefully track symptom fluctuations relative to specific treatments including levodopa dosing and DBS, while carefully excluding cardiopulmonary comorbidities. However, individual pathophysiological variations should be considered. Furthermore, as our EMG recordings were limited to diaphragm, we could not fully evaluate the temporal activation of other respiratory muscles, such as the intercostals or scalenes, nor conclude that diaphragm is the sole contributor to the observed mechanical conflict. The effects of non-levodopa antiparkinsonism agents and DBS on respiratory function warrant further investigation.
Current research into PD dyspnea relies predominantly on spirometry and inductance plethysmography. While needle and surface EMG studying respiratory musculature are established in fields such as critical respiratory care and neuromuscular disorders,13,15 they are not systematically applied to evaluate PD dyspnea. Similarly, diagnostic imaging research remains limited in this context. We demonstrate that ultrasound-guided diaphragmatic needle EMG could safely facilitate the evaluation of diaphragm-chest wall motion. In our case, this technique identified a specific, levodopa-responsive respiratory dysfunction that might otherwise remain unrecognized.
The diaphragm-chest wall asynchrony in our case represents a novel observation in PD dyspnea. We propose that this phenomenon, likely arising from impaired central drive timing and respiratory discoordination, could contribute to dyspnea in PD and appears modifiable with dopaminergic therapy.
Supplemental Material
Supplemental Material
sj-docx-1-pkn-10.1177_1877718X261455572 - Supplemental material for Off-State dyspnea induced by diaphragmatic-chest wall asynchrony in Parkinson's disease: A novel observation and review of the literature
Supplemental material, sj-docx-1-pkn-10.1177_1877718X261455572 for Off-State dyspnea induced by diaphragmatic-chest wall asynchrony in Parkinson's disease: A novel observation and review of the literature by Wen-Che Li, Li-Ta Keng and Kai-Hsiang Stanley Chen in Journal of Parkinson's Disease
Footnotes
Acknowledgment
This study received no funding. The authors declare that there are no additional disclosures to report. We offer special thanks to the patient for his willingness to engage in the electrophysiological study and share his clinical data.
Ethics approval
All investigations performed were done during clinical practice and patient care. Our institution does not require ethical approval for reporting individual cases.
Consent for publication
The authors confirm that written informed consent for the publication of the medical data was obtained from the patient. Written consent is with the authors.
Author contributions
1. Research project: A. conception, B. organization, C. execution, D. patient care;
2. Ultrasound-guided electromyography study: A. performance, B. formatting;
3. Statistical analysis: A. design, B. execution, C. review and critique;
4. Manuscript preparation: A. writing of the first draft, B. review and critique;
W.C.L: 1D, 2B, 4A
L.T.K: 1A, 1B, 1C, 2A
K.S.C: 1A, 1B, 1C, 1D, 2A, 2B, 4B
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
Data sharing is not applicable to this article as no datasets were generated or analyzed during the current study.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.