
Abstract
Background and Objectives:
Single-point hand acupuncture with movement is a novel technique that can be used to provide immediate pain relief in the treatment of musculoskeletal disorders. It involves inserting just one needle along the second metacarpal bone, and then having the patient move through motions that were previously painful while retaining the needle. This study is a preliminary three-arm, single-blinded, randomized comparative trial looking at this technique compared with two control techniques.
Methods:
Twenty-four patients were recruited in an outpatient musculoskeletal practice with neck, shoulder, low back, or hip pain. Patients were randomized to one of three treatment arms. The three treatment arms were verum single-point hand acupuncture with movement, single-point hand acupuncture without movement, and control acupuncture with movement. Range of motion (ROM) and numeric pain rating scale were recorded before and after treatment (about 10 min).
Results:
The combined results of all patients showed that the mean difference in post-treatment versus pretreatment ROM was 11.6 degrees and this was statistically significant (p = 0.0027). The mean difference in post-treatment versus pretreatment pain was −2.3 and this was statistically significant (p = 0.0000). There was no statistically significant mean difference between the single-point hand acupuncture with movement and the other two techniques. Also, there was no significant mean difference whether a de qi response was elicited or not.
Conclusions:
Despite single-point hand acupuncture not being able to demonstrate superiority over the other techniques, it can still be a useful technique to learn, given its ease of use and wide applicability.
Keywords
INTRODUCTION
There are several studies showing that acupuncture can provide immediate improvements in pain. A systematic review showed that acupuncture can provide immediate improvements in pain for nonspecific low back pain. 1 Studies have shown that distal needling (press tack needles and classical needles) can immediately improve Constant–Murley pain scores in patients with shoulder pain due to adhesive capsulitis. 2 Another commonly used treatment that can give immediate results is battlefield acupuncture, an auricular acupuncture protocol that has been successfully used in the military setting and in emergency departments.3,4 Electroacupuncture has also been shown to demonstrate immediate improvements in pain and gait in patients with knee osteoarthritis. 5
In addition to immediate pain relief, a few studies have looked at immediate improvements in range of motion (ROM) with acupuncture.6–8 Studies have shown immediate improvement in cervical pain and ROM after acupuncture needling. 6 One study found that motion-related pain and cervical spine mobility improved more with distant acupuncture needling than needling of local myofascial trigger points. 7 A different study showed immediate improvement in lumbar flexion (measured with the Schober test) when needling the low back at the most tender site. 8 Acupuncture can also be combined with stretching to provide immediate improvements in cervical pain and ROM. 6
There have also been some negative studies for needling that show trigger point dry needling ineffective for improving gluteal ROM, and also trigger point dry needling not being any more effective than trigger point massage therapy.9,10
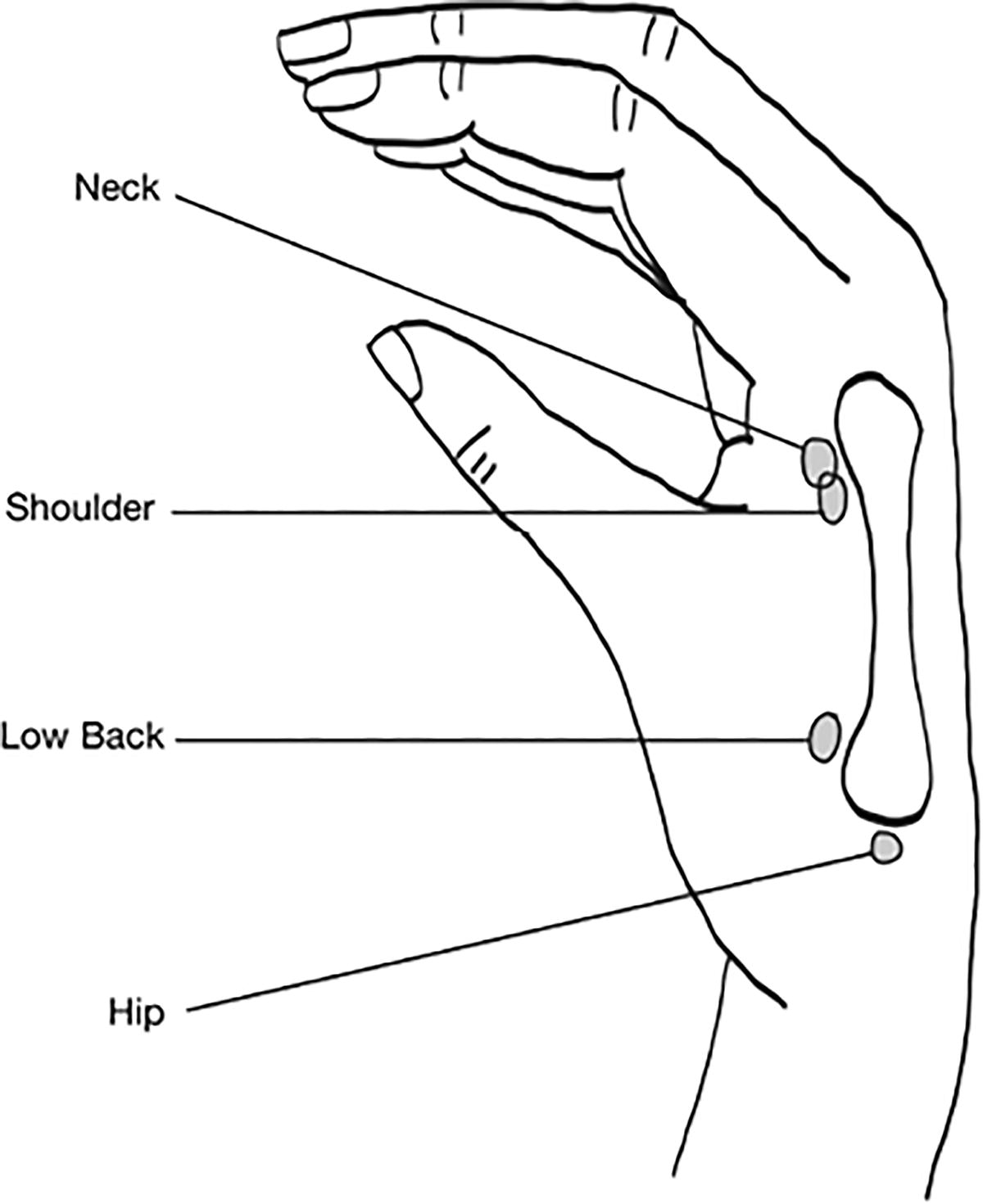
This study looks at a novel, easy-to-perform, and widely applicable acupuncture treatment called “single-point hand acupuncture with movement” for patients with various musculoskeletal pain disorders. Single-point hand acupuncture with movement involves inserting one needle in a specific location along the edge of the second metacarpal bone within the first dorsal interosseous space of the hand to treat pain at a distant location in the body. This is based on the theory of microsystems, also called the Embryo Containing the Information of the Whole Organism (ECIWO), where the whole body is mapped onto the second metacarpal. The needle is inserted toward the head of the second metacarpal for pain complaints involving the head/neck, the shaft for pain complaints in the chest/thorax, and near the base of the metacarpal for pain in the low back/foot. See Figure 1 for previously published second metacarpal ECIWO needling point locations. This one needle provides immediate pain relief, and subjects are then instructed to perform active ROM involving previously painful movements, while keeping the needle in place. The thought is that the movement after needling can alter pain perception, stretch tight muscles, and mobilize dysfunctional joints, thus potentially providing more sustained relief as well. The appeal of this technique is that it is easy to perform and can work for a variety of musculoskeletal disorders, regardless of the duration of symptoms and the location of pain.

Previously published second metacarpal Embryo Containing the Information of the Whole Organism (ECIWO) microsystem needling locations.
The idea of retaining the needle while having the patient move has been previously described in the literature and was named “motion-style acupuncture” by the author. 11 However, the previously published study selected different acupuncture points compared with our study, and the patient’s movement was primarily walking. The results of that study showed that motion-style acupuncture could help with acute low back pain. 11
Finally, this study looked at whether a de qi response influenced needling efficacy. The definition of de qi is debated, and has been described as a sensation of soreness, numbness, fullness or distension, and heaviness felt by the patient, but de qi has also been described as a muscular twitch or a grasping of the needle by the treated tissues. 12 Two different types of de qi responses were recorded in this study, both a local twitch of the muscle and a sensation felt by the patient.
The objective of this study was to test whether verum single-point hand acupuncture with movement was superior to the two control acupuncture methods with regard to immediate improvements in pain and ROM. The two control acupuncture methods were single-point hand acupuncture without movement and control acupuncture involving superficial needling into the first dorsal interosseous muscle with movement. The three arms of the study were designed to test whether precise needling location mattered and whether having the patient move while keeping the needle in place mattered.
METHODS
This study was approved by the Washington University in St. Louis Institutional Review Board on July 2, 2019, IRB ID# 201904173. This study was also registered under the US Clinical Trials Registry through the Good Clinical Practice Network, where the full protocol may be found under the Clinical Trial NCT04048941.
Participants
Participants were recruited from outpatient orthopedic clinics of the principal investigator and coinvestigators from October 2019 through February 2020, and informed consents were signed by all participants. Subjects underwent standard medical evaluations and were given a standard medical diagnosis and treatment plan. Inclusion criteria for the study included subjects who had primary pain localized to one of the four predetermined locations (neck, shoulders, low back, or hips), pain ≥4 on the numeric pain rating scale (NPRS) with at least one of the predetermined measurable movements, and willingness to partake in the study. The predetermined movements included the following: (1) Active cervical flexion, extension, rotation, and sidebend; (2) active shoulder flexion, extension, abduction, adduction; passive shoulder external rotation at side, internal rotation at the side, external rotation while abducted to 90 degrees, and internal rotation while abducted to 90 degrees; (3) active lumbar flexion, extension, rotation, and sidebend; and (4) active hip flexion, extension; passive hip flexion with knee bent, hip extension with knee bent, hip flexion with abduction and external rotation, and hip flexion with adduction and internal rotation. Exclusion criteria included fracture, malignancy, cervical myelopathy, or any condition that required urgent treatment. Other exclusion criteria included any contraindications to needling, such as active infection, pregnancy, extreme fear of needles, and history of significant vasovagal response to needling. Based on preliminary data and previously performed power analysis, the target recruitment for the study was 120 participants.
Design
This study was a three-arm, single-blinded, randomized comparative trial. The three groups included (1) verum single-point hand acupuncture with movement, (2) single-point hand acupuncture without movement, and (3) control acupuncture with superficial needling of the first dorsal interosseous muscle with movement. For the first group, the single-point hand acupuncture technique involved inserting one needle into the first dorsal interosseous space of the hand relatively deeper, along the edge of the second metacarpal bone. This was done to treat pain in a distant location of the body. See Figure 2 for needling locations used in our study, slightly modified compared with the previous published locations. After needling was complete, the patient was told to repeat a series of preset active movements to mobilize the painful body region for 10 min while the needle was kept in place. For the second group, the needling technique was the same as described above, but instead of having the patient go through movements, they were asked to lie on the examination table quietly for 10 min. For the third group, the control acupuncture involved inserting one needle superficially at the highest point in the muscle belly of the first dorsal interosseous muscle, just radial to the classical acupuncture point LI4. This point was selected because it was thought to be a good control point since it is in the same dermatome and myotome as the verum point, which minimizes confounding variables. The patient then went through the same preset active movements as the first group to mobilize the painful body region for 10 min while the needle was kept in place.
Single-point hand acupuncture needling locations used in our study.
The primary outcome was the difference between pretreatment ROM and pain, and post-treatment ROM and pain. The secondary outcome included the presence of de qi response during needling. This could be either an aching or fullness sensation experienced by the patient or a local twitch of the muscle.
Procedure
After subjects were enrolled, the investigator determined the most painful and/or restricted ROM from the predetermined movements and told this to the research coordinator. The research coordinator then measured the pretreatment ROM and NPRS using this movement, for a total of three trials. The investigator then used a previously created randomly assigned Excel spreadsheet to select the treatment group. Patients were blinded to which arm of the treatment group they were assigned. The investigator then went back into the patient’s room to perform the assigned needling treatment.
For the single-point hand acupuncture treatment, the needle was placed on the same side of where pain was located. In patients with neck or low back pain in the midline, the needle was placed on the side where the second metacarpal was more tender to palpation. The area along the second metacarpal bone was palpated for painful or fibrous bands, and if these were near the correlating regions of pain, based on Figure 2, they were targeted. Needle insertion depth ranged from 5 to 20 mm, with the target being the radial side of the periosteum of the second metacarpal. If a de qi response was elicited, then the provider would leave the needle tip in that location and have the patient repeat the previously painful movement. If the patient noticed >50% improvement in pain, then needling was complete. If there was not >50% improvement in pain, the needle was manipulated (up to three times) to try and elicit a de qi response, and painful movement was retested after each needle manipulation.
For the control point acupuncture, needle insertion depth was 1–5 mm, and insertion was superficial because this arm was used primarily as a sham needling group. Similarly, the patient was asked if a previously painful movement was >50% improved after needling, and up to three needle manipulations were allowed, but needles were kept superficial.
After the provider performed the assigned needling treatment and patient completed the treatment, the provider went back into the patient room to remove the needle. The research coordinator then returned into the room to measure post-treatment ROM and NPRS with the previously painful movement, for a total of three trials. For both the pretreatment and post-treatment ROM and NPRS, the mean of the three trials was used in the analysis.
For statistical analysis, the difference score regarding ROM and pain was created between post- and pretreatment. One-way ANOVA was performed to test mean difference among the treatment groups. A two-sample t-test was used to compare the mean difference regarding whether the provider noticed a local twitch response as well as whether the subject noticed a de qi response. All statistical tests were two-sided at a significance level of 0.05, and statistical analyses were performed with SAS 9.4 (SAS Inc., Cary, NC).
RESULTS
Twenty-four subjects were enrolled with a mean age of 54.3 (SD ±15.6), with a minimum age of 35 and a maximum age of 88. All patients who were consented and enrolled completed the study. Eighteen patients were female (75%) and six were male (25%). Three patients presented with neck pain (12.5%), eight presented with shoulder pain (33.3%), nine presented with low back pain (37.5%), and four presented with hip pain (16.7%), see Table 1. Initially, the study was supposed to recruit 120 subjects, but the study was cut short by the COVID-19 pandemic when clinical research was halted and never restarted.
Baseline Demographics and Clinical Characteristics of Participants

For the randomization, 7/24 were randomized to the verum single-point with movement, 7/24 were randomized to single-point without movement, and 10/24 were randomized to the control with movement. See Figure 3 for the flow diagram of subjects through the study. Subjects had pain for a mean duration of 6.6 months (SD ± 8.2) with the shortest duration of 0.2 months (1 week) and longest was 30 months (2.5 years).
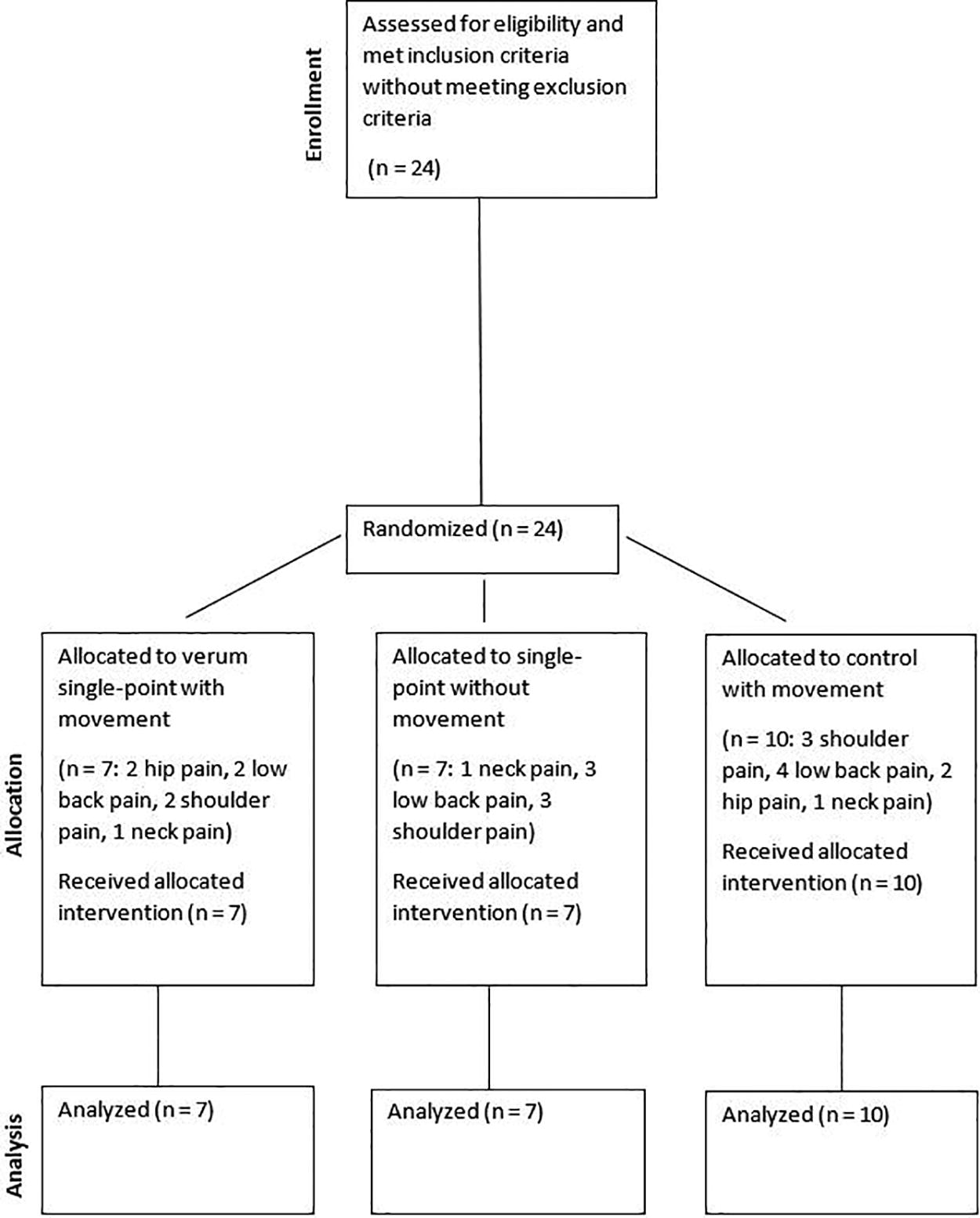
Diagram showing the flow of participants through each stage of the study protocol.
The combined results of all patients showed that the mean difference in post-treatment versus pretreatment ROM was 11.6 degrees (SD ± 16.9) for the most painful movement, and this was statistically significant (p = 0.0027). The mean difference in post-treatment versus pretreatment pain was −2.3 (SD ± 1.6) for the most painful movement, and this was statistically significant (p = 0.0000). There was no significant mean difference between the three arms of single-point hand acupuncture with movement, single-point hand acupuncture without movement, and control acupuncture with movement with regard to ROM (p = 0.4335) or pain (p = 0.1706). There was no significant mean difference in ROM or pain with or without a de qi response. This included both an ache and fullness felt by the patient, or a local muscle twitch. See Tables 2 and 3 for details. There were no harms or unintended effects in any group.
Range of Motion Data
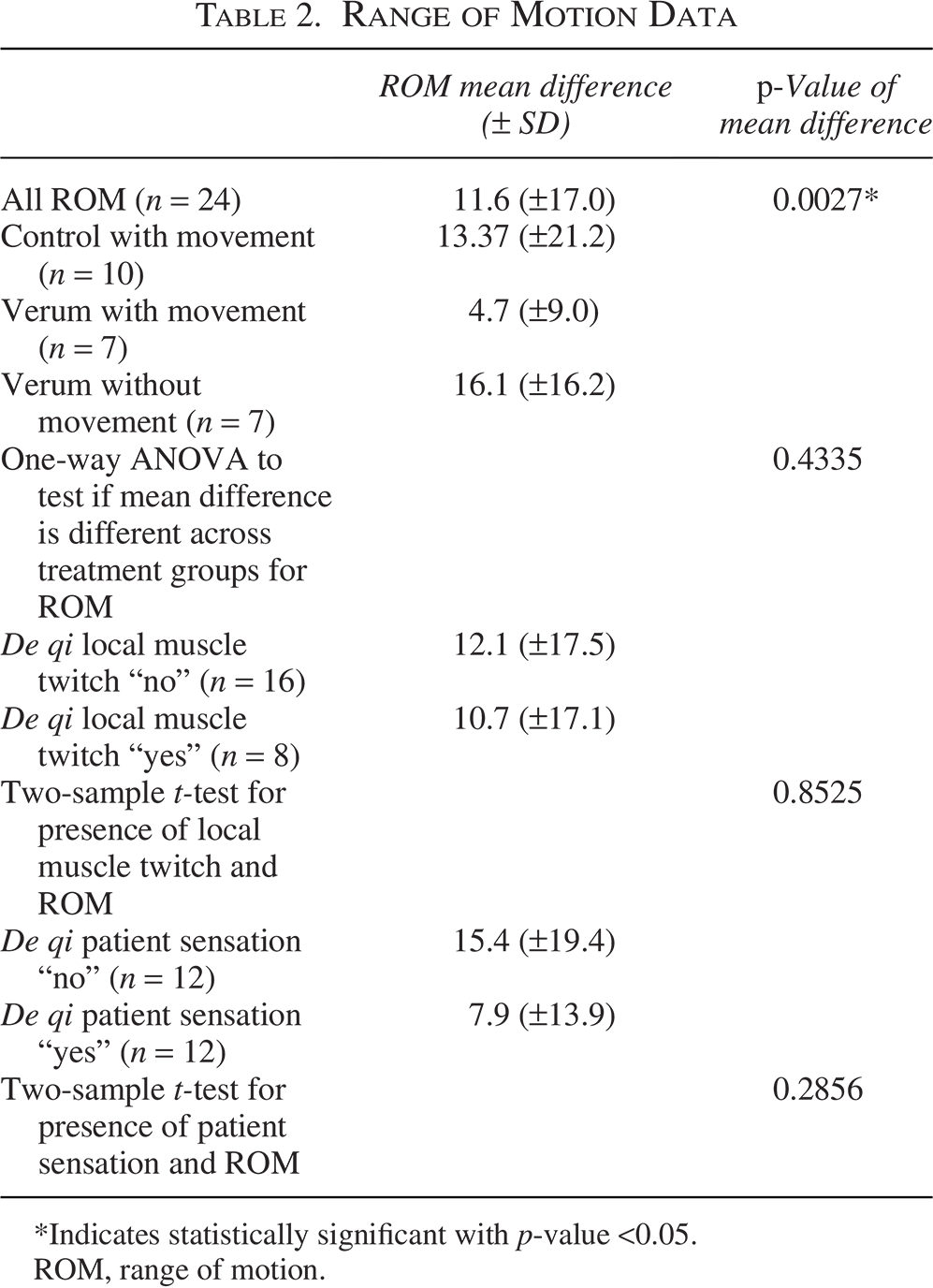
*Indicates statistically significant with p-value <0.05.
ROM, range of motion.
Numeric Pain Rating Scale Data
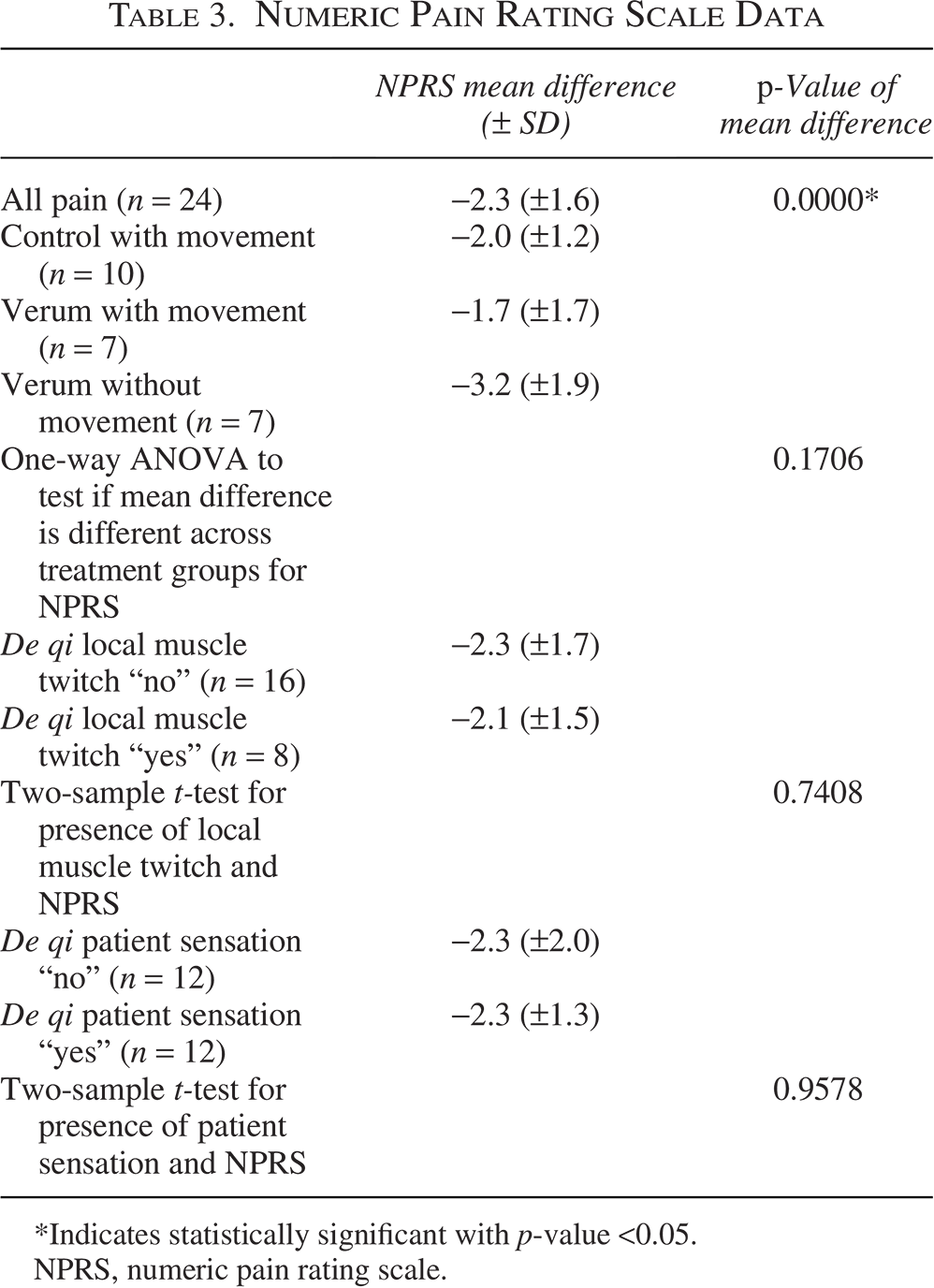
Indicates statistically significant with p-value <0.05.
NPRS, numeric pain rating scale.
DISCUSSION
This study was funded by the Washington University Orthopedic Clinical Research Center as part of the Richard Gelberman faculty development grant. The study was cut short by the COVID-19 pandemic and thus is labeled a preliminary study. This study was designed to compare single-point hand acupuncture with movement with two different control treatments. The study showed that all treatments provided significant improvements in ROM and pain outcomes, but there was no statistical significance between the groups. Given the premature termination of the study and the use of active control groups, our study was likely significantly underpowered. Despite this, there are still some useful conclusions that can be drawn from this study.
This study demonstrated that just one needle in the hand can have immediate improvements in ROM and pain for various musculoskeletal pain complaints. It is effective for both acute and chronic pain. This has advantages over other needling techniques because of its ease of use and wide applicability. This is a technique that can be easily taught and used by practitioners in a wide range of clinical settings. Immediate improvements in pain and ROM can be useful in the setting of patients who have difficulty progressing with physical therapy, or with acute pain flare-ups where the alternative is prescription opioid pain medications. Also, within-session changes in pain and ROM have been shown to provide favorable odds for between-session changes when patients with low back pain were being treated. 13 The degree of improvement in pain offered by this technique meets the generally accepted threshold for minimally clinically important difference in chronic musculoskeletal conditions, which is approximately 2.0 on the NPRS. 14
Some caution needs to be paid attention to when performing single-point hand acupuncture with movement. The main caution is being careful not to cause a vasovagal reaction.15,16 This may be a particular problem if the patient has a needle phobia and sees the needle in the hand. Therefore, it is recommended that the practitioner or an assistant monitors the patient during the movement phase of the treatment, while the needle is retained. Also, needling too deep near LI4 can cause hemorrhage of the palmar metacarpal artery. 17
There can be several critiques of the study design. First, the study used active control groups rather than a true placebo group, as all groups received some sort of treatment. The main author felt that the study would be more appealing to patients if they all received some sort of treatment, and that is why the design of the study was such. Another critique is the selection of the control needling location to be in the same dermatome as the verum acupuncture location (along second metacarpal). This point was originally selected so that the control acupuncture would be more similar to the verum acupuncture and to avoid confounding variables. However, it has been subsequently proposed that with the segmental structure of the body and its interconnected reflex system, this can explain why many acupuncture studies that use a sham point in the same dermatome as the verum point fail to show a difference between the groups. 18 At the inception of this study in 2019, the above article was yet to be published, and so the main author was unaware of this potential phenomenon.
CONCLUSIONS
Single-point hand acupuncture with movement is an easy acupuncture technique that can be used to treat an array of musculoskeletal pain complaints of varying chronicity. It can provide immediate improvements in pain and ROM. Although it was not shown to be superior to other acupuncture methods, it merits further research and could be a useful tool for practitioners who treat musculoskeletal pain.
AUTHORS’ CONTRIBUTIONS
C.T.T.: Conceptualization, methodology, validation, investigation, data curation, writing—original draft, and funding acquisition. A.Y.N.: Data curation, writing—review and editing, visualization, and project administration. H.P.: Conceptualization and investigation. L.C.: Formal analysis. A.L.C.: Methodology and investigation.
Footnotes
ACKNOWLEDGMENTS
This article and the research behind it would not have been possible without the mentorship of Dr. Ling Guan and also the support of the clinical research coordinator, Melissa Armbrecht.
AUTHOR DISCLOSURE STATEMENT
No competing financial interests exist.
FUNDING INFORMATION
This study was funded by the Washington University Orthopedic Clinical Research Center, as a part of the Richard Gelberman faculty development grant (OCRC01).