
Abstract
Background
Chorioamnionitis is a significant perinatal infection that adversely affects maternal and neonatal outcomes. Diagnostic criteria, including Lencki’s criteria, are frequently used; however, they include subjective indicators, limiting their clinical utility. We aimed to establish diagnostic criteria using only objective indicators.
Methods
This retrospective cohort study involved patients who delivered at our hospital and underwent placental pathological examination from 2003 to 2022. Based on the Blanc classification, patients were classified into the CAM II/III (stage 2 or 3) and CAM I (stage 1) groups, followed by between-group comparisons of maternal and neonatal outcomes. Diagnostic indicators were selected through multivariate logistic regression analysis and used to develop a diagnostic model. Receiver operating characteristic curves were generated to compare the diagnostic performances of the new and previous criteria.
Results
Among 862 included patients, 538 and 324 were classified as CAM II/III and CAM I, respectively. The CAM II/III group showed significantly higher rates of neonatal acidosis and maternal postpartum hospitalization ≥10 days. In the new model, scores were assigned as follows: body temperature ≥38.5°C (2 points), C-reactive protein ≥1.0 mg/dL (2 points), white blood cell count ≥12 × 109/L (1 point), and nulliparity (1 point). A total score ≥4 points was considered the diagnostic threshold. The new criteria outperformed the existing criteria, with an area under the curve (AUC) value of 0.741 compared to 0.621 (p < 0.001).
Conclusions
The new criteria showed improved diagnostic accuracy for chorioamnionitis, which may facilitate early diagnosis and timely intervention for improved perinatal outcomes.
Introduction
Chorioamnionitis (CAM) is characterized by infection and inflammation of intrauterine structures; moreover, it is the most common perinatal infection, occurring in 1%–4% of births.1,2 The most common cause of CAM is bacterial invasion through the cervix, 3 while in rare cases it can be caused by transplacental infection. 4 CAM has significant maternal and neonatal effects; specifically, it results in a 2- to 3.5-fold increase in adverse perinatal events, including perinatal death, early-onset neonatal sepsis, and intraventricular hemorrhage. 5 To improve perinatal outcomes, early clinical diagnosis and prompt antibiotic administration with appropriate timing and delivery method are recommended. 6 Diagnostic criteria for CAM are divided into clinical and histological criteria. Although several diagnostic criteria for clinical CAM have been proposed, Lencki’s criteria are widely used in Japan. 7 Lencki’s criteria include maternal temperature ≥38°C, white blood cell count ≥15 × 109/L, maternal tachycardia ≥100 beats/min, uterine tenderness, and odor of vaginal discharge or amniotic fluid. A histological diagnosis of CAM is made upon observation of pathological findings of infiltration of maternal polynuclear leukocytes into the chorion and amnion. 8 The Blanc classification is based on the degree of infiltration of polynuclear leukocytes into the chorioamnion, with stages 1, 2, and 3 being defined as the intervillous space, chorioamnion, and amnion, respectively. 8 The prognosis for neonates worsens as the stage progresses. 9 Further, the frequency of fetal inflammatory response syndrome increases as the stage advances. 10 There is a need for clinical criteria that can predict histological CAM affecting perinatal outcomes; however, Lencki’s criteria, which are used as clinical criteria, have limited utility in clinical practice. First of all, low sensitivity has been reported, 11 and other reasons include the lack of objectivity in the evaluation items and difficulty of assessing uterine tenderness under painless delivery. Given these issues, this study aimed to develop novel diagnostic criteria for clinical CAM based solely on prenatal objective parameters, by retrospectively analyzing cases with histologically confirmed CAM. We also evaluated whether the new criteria improve diagnostic performance compared to conventional methods, with the ultimate goal of enhancing clinical management and improving maternal and neonatal outcomes.
Methods
Study design and setting
This single-center retrospective cohort study included patients who delivered and underwent pathological examination of the placenta at our hospital from July 2003 to October 2022. Informed consent was obtained from the patients in the form of a website opt-out option. Specifically, information about the study was disclosed on the hospital’s website in accordance with institutional ethical guidelines. Patients were given the opportunity to decline participation by submitting an opt-out request via the website. This study was approved by the Institutional Ethics Committee (registration number, 22-R114) and complied with the requirements under the Declaration of Helsinki. The exclusion criteria were as follows: (1) patients without pathological evidence of CAM, (2) other obvious infections such as pneumonia and urinary tract infection, (3) autoimmune disorder, (4) corticosteroid users, (5) delivery before 34 weeks’ gestation, (6) multiple pregnancies, and (7) no blood test within 24 pre-delivery hours. By excluding cases of autoimmune disorder, corticosteroid use, and delivery before 34 weeks’ gestation, the effect of steroids on blood sampling results was eliminated. Indications for placental pathological examination at our hospital have been cases of suspected clinical CAM, preterm delivery, hypertensive disorders of pregnancy, overt diabetes in pregnancy, small-for-gestational-age infants, suspected placenta accreta or abruption, and neonatal asphyxia. This remained consistent throughout the study period. Therefore, accounting for background bias, we also excluded non-pathological CAM patients. The sample size was determined based on all eligible cases identified during the study period, as no formal sample size calculation was performed for this retrospective cohort study. This study was designed and reported following the STROBE guidelines.
Grouping
The selected patients were divided into the case and control groups based on the Blanc classification. Patients with stage 2 and stage 3 of the Blanc classification, in which multinucleated leukocytes infiltrate deep into the chorion, were classified into the case group (CAM II/III). Patients with stage 1, in which multinucleated leukocytes remain subchorionic, were classified into the control group (CAM I). Each group was randomly divided into derivation and validation datasets at a 7:3 ratio using a computer-generated randomization program.
Data collection
We extracted continuous data regarding age, maternal pregravid body mass index, gestational week at delivery, total delivery time, time from rupture of the membrane to delivery, highest body temperature (BT) and maternal pulse rate within 24 hours of delivery, white blood cell (WBC) count, and C-reactive protein (CRP) value of the most recent pre-partum blood test, one-minute and five-minute Apgar score, umbilical cord arterial pH (UApH), and postpartum hospitalization period. Further, we extracted nominal data regarding history of delivery, premature rupture of membrane, gestational diabetes mellitus, insulin usage, and neonatal intensive care unit (NICU) admission. All data were extracted from electronic medical records.
Statistical analysis
Data were analyzed using the Mann–Whitney U-test, Fisher’s exact test, and the classification and regression tree (CART) model. Statistical analysis was conducted using R software 4.2.2 and EZR (Kanda 2013). p-values <0.05 were considered statistically significant. Missing data were assumed to be missing completely at random and were not imputed. The primary outcome was the between-group comparison of the postpartum prognosis of mother and child. The secondary outcomes were the risk factors for CAM and establishment of a clinical CAM diagnostic model. Univariate analyses were performed using derivation datasets, with a p-value of 0.1 being used as a cutoff threshold to select variables for multivariate logistic regression analyses. Factors associated with CAM were ranked using the CART model, and the diagnostic scoring model was developed using the regression coefficient. Given the difficulty in assessing subjective indicators in Lencki’s criteria, modified Lencki’s criteria (mLC) were assumed with exclusion of uterine tenderness and malodor of vaginal discharge/amniotic fluid. Receiver operating characteristic (ROC) curves and areas under the curves (AUC) in the validation groups were generated to evaluate the efficiency of the experimental model (EM) relative to that of mLC.
Results
Patient clinical characteristics
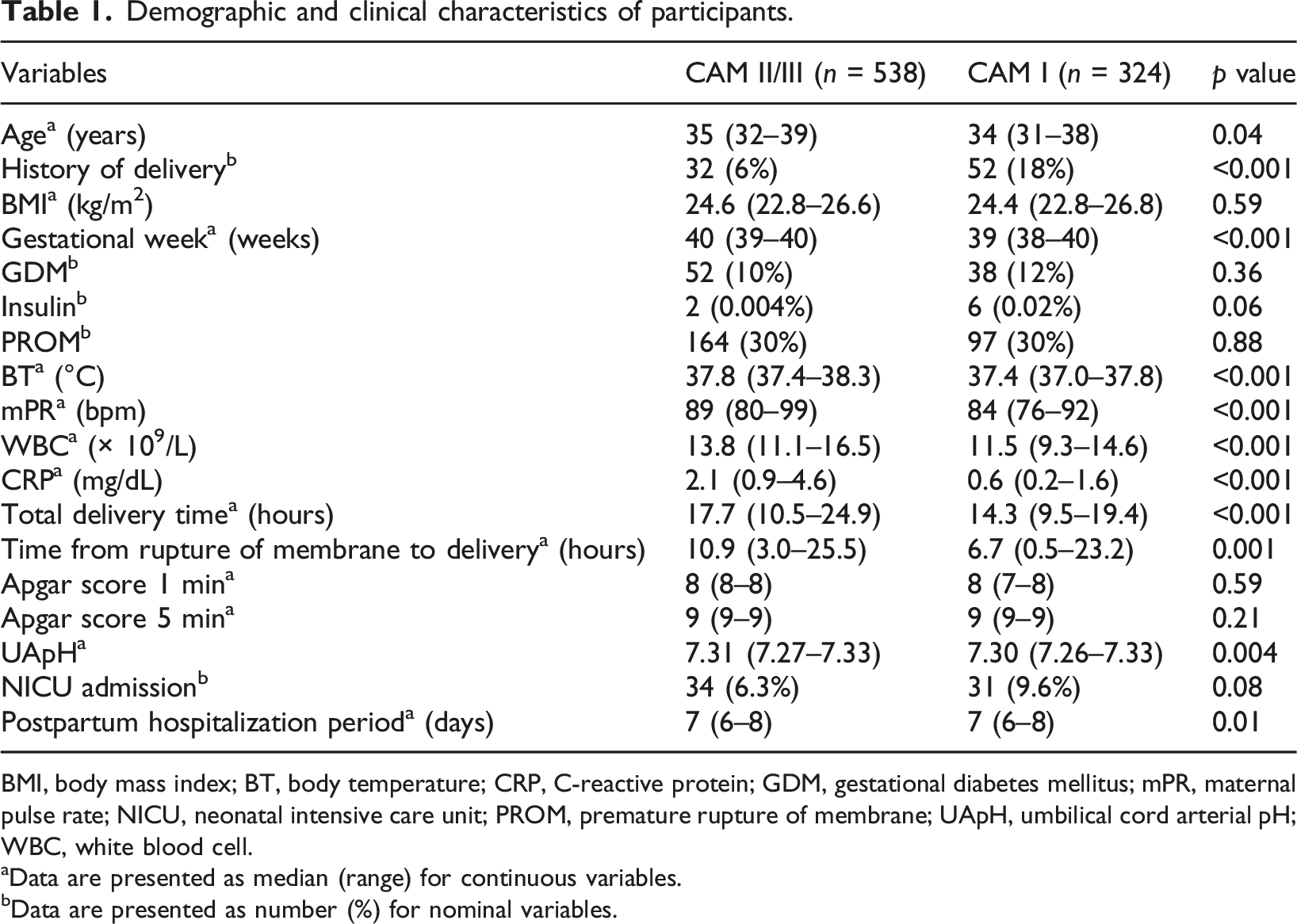
A total of 4135 patients underwent pathological examination of the placenta after delivery at our hospital between 2003 and 2022. As shown in Figure 1, 862 patients were included based on the inclusion/exclusion criteria and were classified into the case group (CAM II/III, n = 538) and the control group (CAM I, n = 324) based on the Blanc classification. Table 1 shows the clinical characteristics of all patients. The case and control groups were randomly assigned to the derivation and validation datasets at a ratio of 7:3, respectively (Figure 1). Flow diagram of the participants of the study. Demographic and clinical characteristics of participants. BMI, body mass index; BT, body temperature; CRP, C-reactive protein; GDM, gestational diabetes mellitus; mPR, maternal pulse rate; NICU, neonatal intensive care unit; PROM, premature rupture of membrane; UApH, umbilical cord arterial pH; WBC, white blood cell. aData are presented as median (range) for continuous variables. bData are presented as number (%) for nominal variables.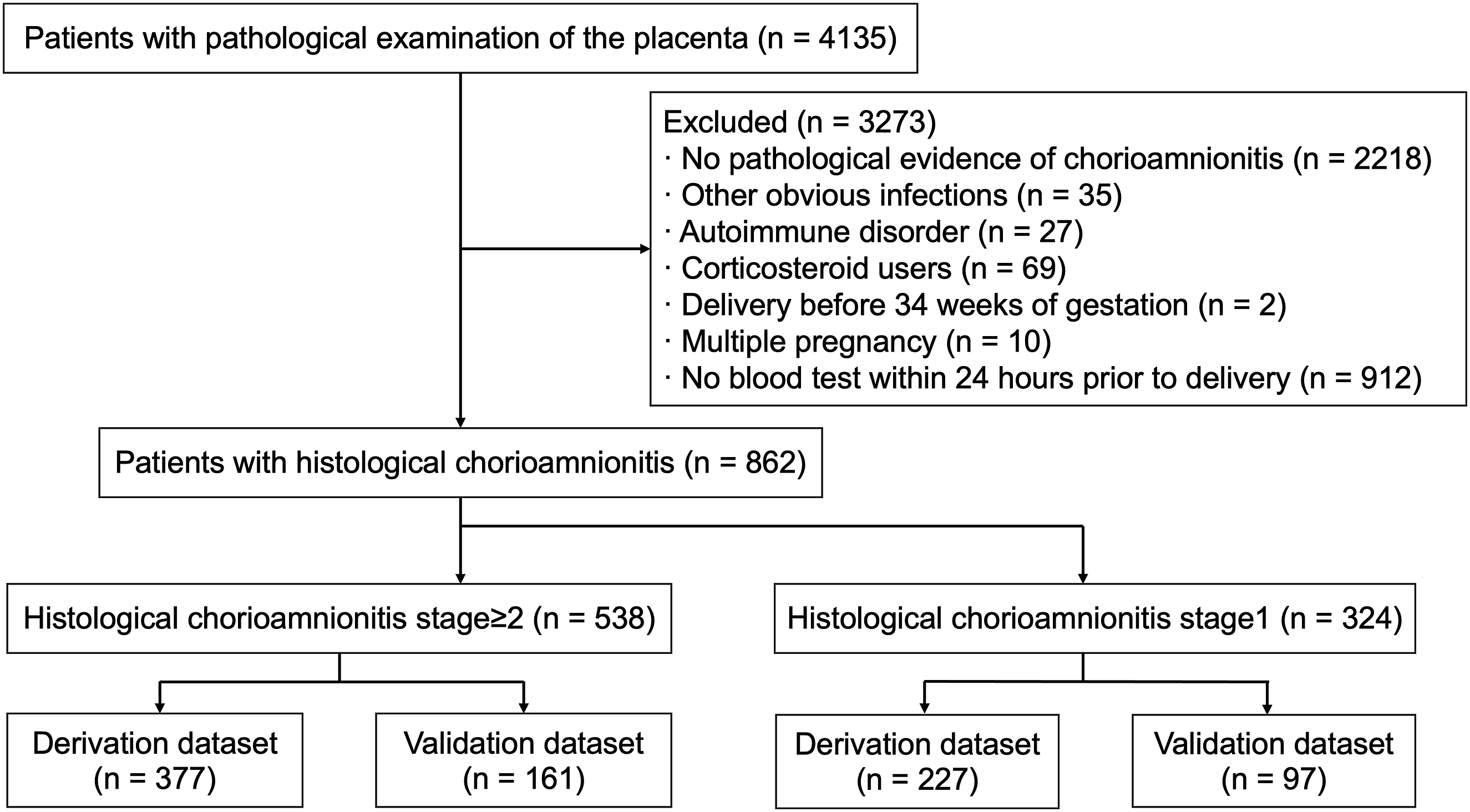
Postpartum maternal and neonatal prognosis
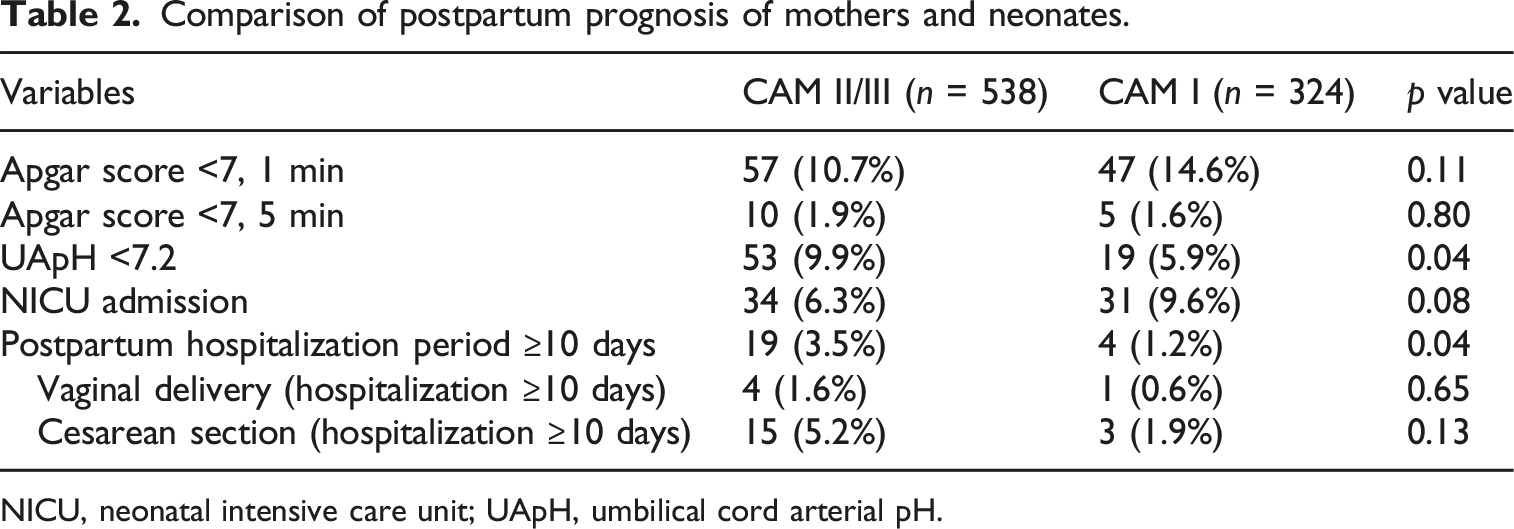
Comparison of postpartum prognosis of mothers and neonates.
NICU, neonatal intensive care unit; UApH, umbilical cord arterial pH.
Analysis of independent factors influencing development of histological CAM II/III
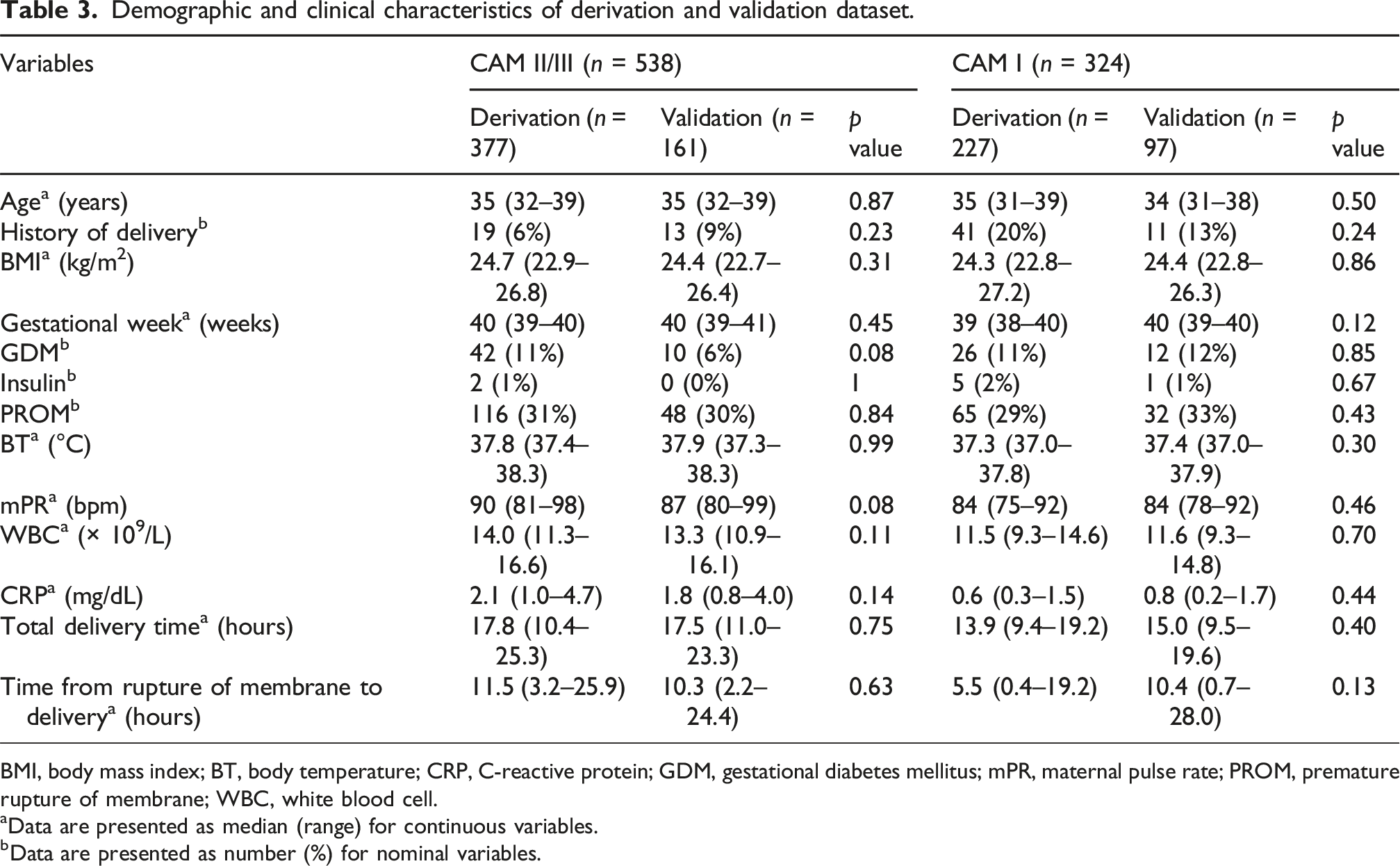
Demographic and clinical characteristics of derivation and validation dataset.
BMI, body mass index; BT, body temperature; CRP, C-reactive protein; GDM, gestational diabetes mellitus; mPR, maternal pulse rate; PROM, premature rupture of membrane; WBC, white blood cell.
aData are presented as median (range) for continuous variables.
bData are presented as number (%) for nominal variables.
Univariate and multivariate analysis of independent factors affecting development of histological CAM (stages 2 and 3).

BMI, body mass index; BT, body temperature; CRP, C-reactive protein; GDM, gestational diabetes mellitus; mPR, maternal pulse rate; OR, odds ratio; PROM, premature rupture of membrane; WBC, white blood cell.
aData are presented as median (range) for continuous variables.
bData are presented as number (%) for nominal variables.
Construction of a clinical CAM diagnostic model
Multivariate logistic regression analysis of risk factors for histological CAM and new scoring model.
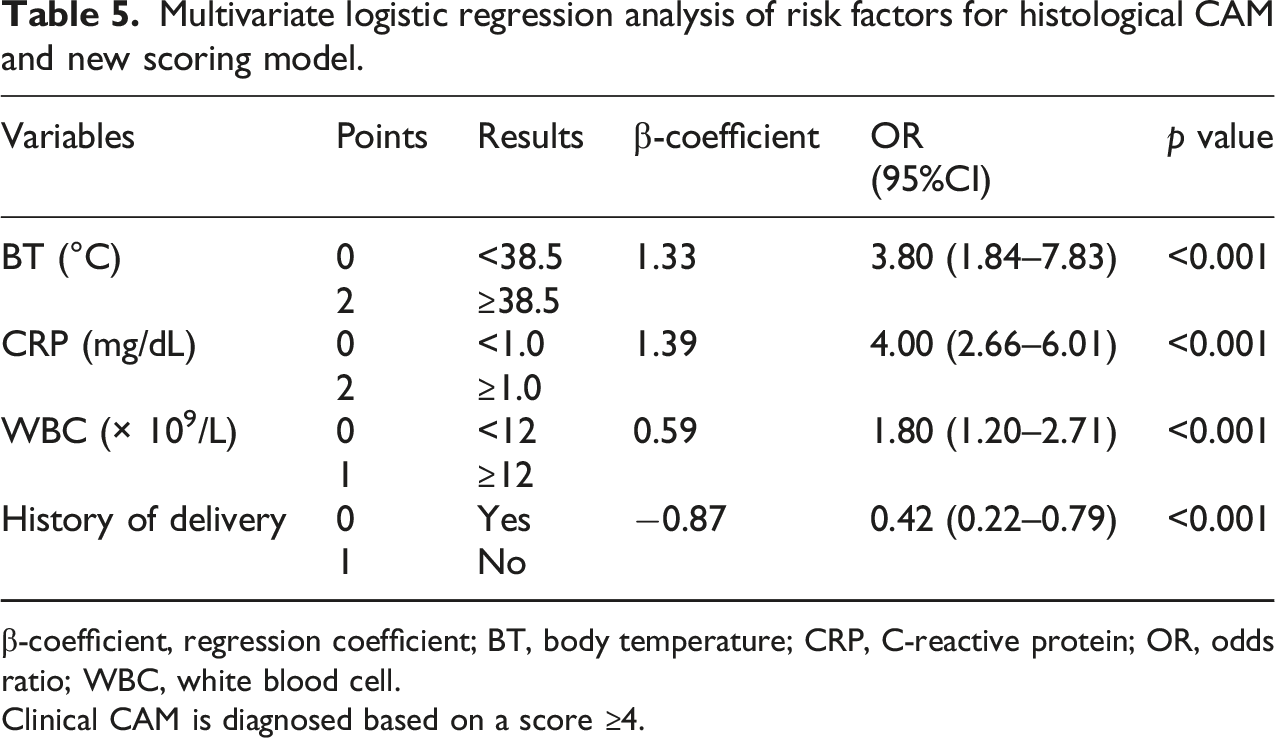
β-coefficient, regression coefficient; BT, body temperature; CRP, C-reactive protein; OR, odds ratio; WBC, white blood cell.
Clinical CAM is diagnosed based on a score ≥4.
Validation of the diagnostic model
The validation datasets were used to test the validity of EM against mLC. The sensitivity and specificity values were 0.528 and 0.845 in EM, respectively, and 0.317 and 0.876 in mLC, respectively. Figure 2 shows ROC curves, with the AUC values being 0.741 and 0.621 for EM and mLC, respectively. The analysis confirmed the effectiveness of EM (p < 0.001). Comparison of the diagnostic performance of the new scoring model and modified Lencki’s criteria. The ROC-AUC values of the new scoring model and modified Lencki’s criteria were 0.741 and 0.621, respectively.
Discussion
Our findings have confirmed that CAM adversely affects the perinatal outcomes of both mothers and infants by analyzing clinical data and placental pathology reports, which is consistent with previous reports. Additionally, we have developed new clinical diagnostic criteria for CAM solely based on objective evaluation items. The new criteria showed improved diagnostic performance compared to existing criteria.
There are several diagnostic criteria for clinical CAM, including Lencki’s criteria; however, they all include subjective indicators and have limited utility.2,7,12 Furthermore, although the amniotic fluid culture test is highly specific, its practicality is limited since it takes up to 3 days to obtain results. 2 In the present study, we used logistic regression analysis to identify clinical items correlated with histological CAM. Subsequently, we established a new scoring model by extracting four items: maternal BT, WBC count, CRP level, and delivery history. The inclusion of delivery history may be attributed to the progression of infection being influenced by prolonged labor in primiparas. By establishing validation datasets, comparison of ROC curves indicated that the new scoring model had a significantly improved AUC compared with mLC (Figure 2).
CAM is known to increase the risk of perinatal adverse events. 5 In addition, CAM is associated with long-term disabilities, including delayed neurodevelopment and cerebral palsy. 13 As shown in Table 2, neonatal acidosis was significantly increased in the CAM II/III group. Moreover, the rate of NICU admission showed a non-significant increase in the CAM II/III group.
Regarding the delivery method after the diagnosis of clinical CAM, there is no established correlation of delivery time with poor neonatal outcomes; therefore, cesarean section is not indicated to reduce delivery time,14,15 Contrastingly, uterine contraction failure associated with intrauterine infection has been reported to increase the rate of prolonged labor and arrested labor, which increases the risk of cesarean section. 16 Cesarean sections increase the risk of postoperative wound infection and pelvic abscess increases, necessitating careful postoperative management. 14 In the present study, as shown in Table 2, the CAMII/III group, especially cesarean section cases, showed an increased rate of postpartum hospitalization for ≥10 days, which may be due to the influence of intrauterine infections or pelvic abscesses during the postpartum period. Accordingly, appropriate antibiotic therapy during the intrapartum period is important for improving perinatal outcomes, including the length of hospital stay for mothers and infants. 6
This study has several limitations. First, there was a selection bias regarding the cases where pathological tests of the placenta were performed, highlighting the need for a prospective study in which pathological tests are conducted for all deliveries. Second, we could not extract cardiotocography findings, which prevented its incorporation into diagnostic criteria; further, the validation data were limited. Additionally, it is important to collect data regarding the neonatal clinical course to assess whether the new criteria contribute to improved medium- to long-term prognosis. In this model, primiparous women tend to score 4 points relatively easily; therefore, treatment planning should take labor progression and fever course into account.
In conclusion, our findings demonstrated the impact of CAM on perinatal outcomes and the performance of the new clinical diagnostic criteria for CAM based on objective indicators. Early and appropriate diagnosis of clinical CAM using the new criteria as well as planning the proper timing and method of delivery with antibiotic therapy is expected to improve perinatal outcomes.
Footnotes
Acknowledgments
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.