
Abstract
BACKGROUND:
To determine the association of placental pathologic lesions with postoperative outcomes, survival, and white matter injury (WMI) in preterm infants with NEC.
METHODS:
A retrospective chart review of 107 neonates with NEC (Bell stage > IIa) from Jan 2013- June 2020 was completed. Demographic, clinical, and outcome data were compared between infants with or without placental pathologic lesions.
RESULTS:
In this cohort, 59/107 (55%) infants had medical NEC, and 48 (45%) had surgical NEC. The infants had a mean gestational age of 28.1±3.7 weeks and a birth weight of 1103±647 g. Maternal vascular malperfusion (82/107, 76.6%) and acute histological chorioamnionitis (42, 39.3%) were the most common pathological placental lesions. Acute histologic chorioamnionitis with fetal inflammatory response was more common in infants with surgical NEC vs. medical NEC (35.4% vs. 15.3%; p = 0.02). The NEC Infants with WMI on brain MRI scans had a significantly higher incidence of acute histological chorioamnionitis (52% vs. 27.8%; P = 0.04). No significant differences in mortality, length of stay and postoperative outcomes in neonates with and without acute histologic chorioamnionitis with fetal inflammatory response were noted. On unadjusted logistic regression, acute histologic chorioamnionitis without fetal inflammatory response was also associated with higher odds of WMI (OR 2.81; 95% CI 1.05–7.54; p = 0.039).
CONCLUSION:
Acute histological chorioamnionitis without fetal inflammatory response was associated with higher odds of WMI in infants with NEC, with no significant impact on mortality and other postoperative outcomes.
Introduction
Necrotizing enterocolitis (NEC) affects ∼5–10% of preterm infants with a birth weight≤1500 grams [1, 2]. Despite advances in neonatal intensive care, NEC remains a leading reason for surgical intervention, severe clinical course, and mortality in neonates born preterm [3–7]. The need for surgical intervention in NEC is associated with increased resource utilization and cost of care due to prolonged hospitalization [8, 9]. The risk factors associated with NEC are complex and multifactorial, including preterm birth, adverse intrauterine environment (inflammatory/hypoxic) and poor perinatal transition [10]. Intrauterine exposure to inflammatory/hypoxic stimuli may prime fetus’s innate immunity cells to a reactive phenotype with exaggerated production of proinflammatory cytokines triggered by risk factors such as formula feeds, blood transfusion, infection, etc., associated with NEC (double-Hit) [10]. Placental histopathologic examination can give us good insights into the intrauterine environment as well as maternal and fetal health but has been under-utilized for bedside clinical decision-making [11, 12].
Some recent studies have reported that the presence of placental fetal vascular malperfusion lesions, placental infarcts, acute histological chorioamnionitis with evidence of fetal inflammatory response is associated with increased frequency of NEC in preterm infants [13–15]. Our group also reported that infants with multiple placental histopathologic lesions, including inflammatory and vascular lesions, are at increased risk of developing NEC in the postnatal period [16]. However, the impact of the placental histopathologic lesions on postoperative outcomes and white matter injury following surgical NEC has not been studied. We hypothesize placental histopathologic lesions may be associated with worse clinical outcomes in preterm infants diagnosed with NEC. The specific aim of this study was to determine the correlation of placental histopathologic lesions with postoperative outcomes and white matter injury on brain MRI scans in preterm infants following medical and surgical NEC, by using a uniform Amsterdam consensus statement classification of placental histopathology [17].
Methods
This retrospective cohort study was conducted at the University of Mississippi Medical Center (UMMC) in Jackson, Mississippi, after approval by the Institutional Review Board (2017–0127). UMMC has a Level 4 neonatal intensive care unit and a regional referral center for neonates with advanced NEC for the entire state. A detailed review of the electronic medical records identified 284 patients with medical and surgical NEC (Bell stage 2 and above) who underwent management of NEC between January 2013 and June 2020. After excluding 29 infants who had duplicate clinical data and 148 infants with missing placental pathology information due to being outborn, we identified 107 infants who were eligible for this study (Fig. 1).
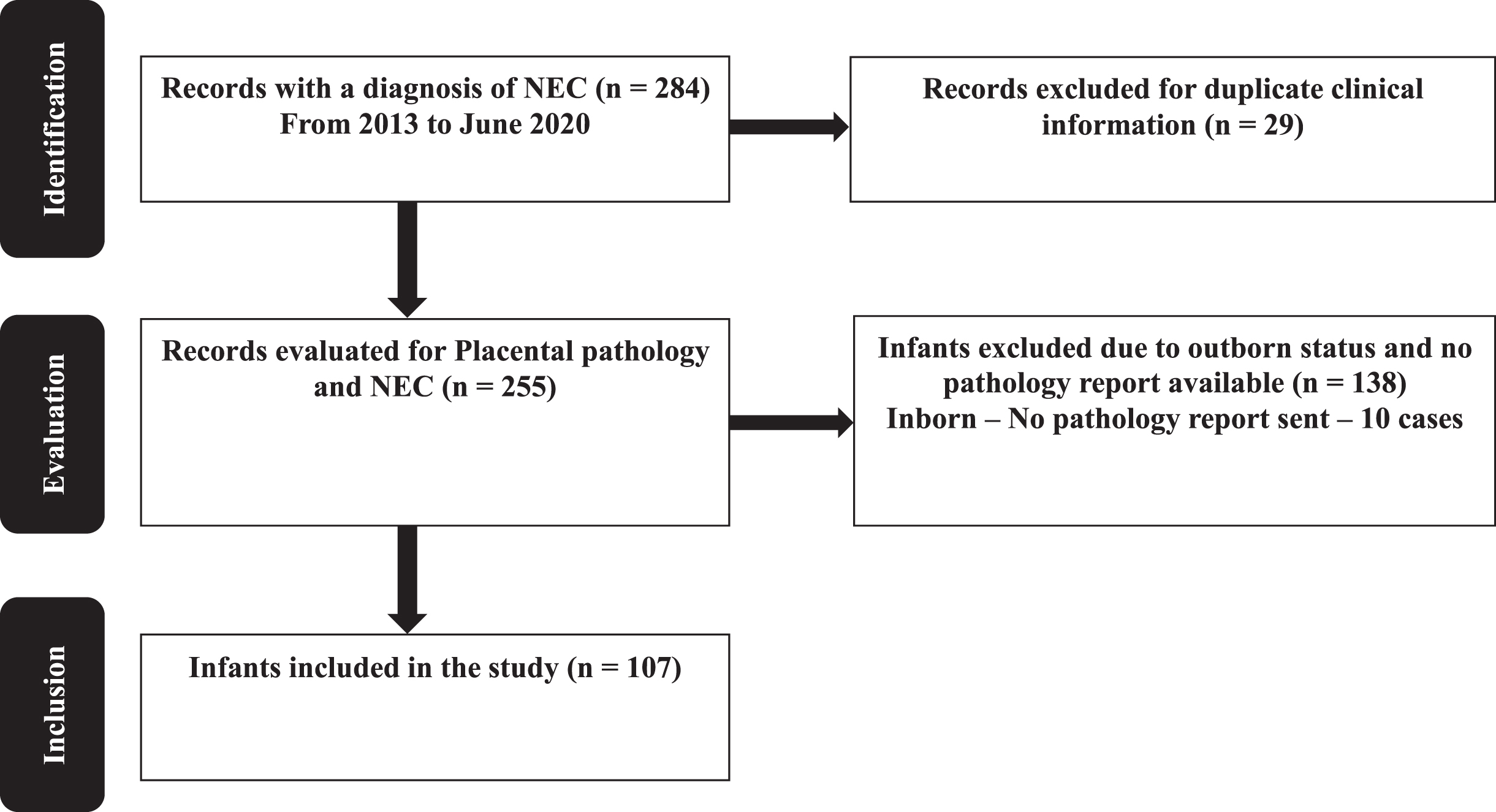
Patient flow diagram of enrolled patients.
We recorded demographic characteristics including birth weight, gestational age (GA), sex, race (African American, Caucasian, or Latino), mode of delivery (cesarean section or vaginal delivery), APGAR score at 5 minutes, out-born status and small for gestational age status. We also collected information regarding maternal factors, including pregnancy-induced hypertension, clinical chorioamnionitis, and antenatal steroids.
NEC data
Infants who did not show obvious pneumatosis intestinalis on abdominal radiographs were classified as≥stage 2 NEC only if they displayed highly suggestive clinical signs with loss of bowel sounds, including generalized abdominal tenderness, abdominal distension, systemic instability with increased needs for respiratory and hemodynamic support, and radiological evidence of intestinal dilatation, fixed bowel loops and/or portal venous gas on abdominal X-ray. We noted the NEC features such as the age of NEC onset (in days), pneumatosis, and clinical presentation (abdominal distension, feeding intolerance, and bloody stools).
We collected information on clinical variables including patent ductus arteriosus (PDA), PDA treatment (medical or surgical), C-reactive protein (CRP) values after NEC onset, cholestasis (direct bilirubin > 2 mg/dL), blood cultures drawn at the time of NEC onset, duration of antibiotic therapy after onset, use of inotropes at 24 hours, and need for assisted ventilation. We also recorded post-operative information on duration of infant not receiving any enteral feeds (Postoperative ileus), day of resuming feeds after surgery, days on parenteral nutrition, the time to reach full enteral feedings (120 mL/kg/day), and intestinal failure (need for parenteral nutrition≥90 days following intestine resection). We also gathered information on length of stay defined as the total duration of hospitalization from the day of admission until discharge or death and mortality defined as death due to any cause before the hospital discharge.
Placental pathology
A board-certified pediatric pathologist routinely examines placentas from all preterm births at our institution for gross and histologic findings. The umbilical cord, membranes, and placental disc are inspected for any gross abnormalities. The placentas are weighed after removing the umbilical cord, fetal membranes, and non-adherent blood clots. Placental weight below the 10th percentile for estimated GA is considered small for GA, and those weighing > 90th percentile for GA are considered large for GA [18]. The placental disk is then serially sectioned at 1-2 cm intervals and examined for intraparenchymal lesions. Representative sections of the umbilical cord, fetal membranes, placental parenchyma, and any abnormalities seen on gross examination are submitted for standard histological examination.
Based on the Amsterdam Placental Workshop Group Consensus Statement recommendations, the histopathologic abnormalities assessed were divided into the following subcategories [17]: Acute histologic chorioamnionitis with or without fetal inflammatory response [19]. Chronic villitis with or without obliterative fetal vasculopathy. Maternal vascular malperfusion (MVM) including maternal vascular lesions (decidual arteriopathy, mural hypertrophy, incomplete transformation of spiral arteries, and decidual necrosis), infarcts, hemorrhage or hematoma, thrombi, villous changes (chorangiosis, syncytial knots, distal villous hypoplasia, and accelerated villous maturation), and placental hypoplasia [20–22]. Fetal vascular malperfusion (FVM). Other inflammatory lesions (chronic deciduitis with plasma cells, massive chronic intervillositis, perivillous fibrin, and histiocytic intervillositis), delayed villous maturation, and villous edema [23].
The presence of more than one of the defined placental lesions was classified as multiple placental pathologies. A representative set of placentas (n = 30) were randomly chosen by a pediatric pathologist and reassessed using the previous noted definitions. This pathologist was blinded to the existing placental reports, clinical history, and patient outcomes. Notably, there was 93% concordance.
Study patients were divided into three groups based on placental pathology: (1) no placental pathology, (2) single placental pathology, and (3) multiple placental pathologic lesions (presence of≥2 histopathologic lesions).
Neonatal MRI and white matter injury (WMI) data
MRI brain scans are routinely obtained at term equivalent age or before discharge home at UMMC for all preterm infants weighing less than 1500 grams at birth. The MRI images were scored independently by two pediatric neuroradiologists, who are unaware of the infants’ clinical course. We used the scoring system reported by Woodward, et al., that consists of eight 3-point scales (10,17). White-matter abnormality was graded according to five scales, which assessed the nature and extent of white-matter signal abnormality, the loss in the volume of periventricular white matter, and the extent of any cystic abnormalities, ventricular dilatation, or the thinning of the corpus callosum. Composite white-matter scores were created and used to categorize infants according to the extent of their cerebral abnormalities. The categories of white-matter abnormality were none (a score of 5 to 6), mild (a score of 7 to 9), moderate (a score of 10 to 12), and severe (a score of 13 to 15).
Statistical methods
For normally distributed continuous variables, we summarized the data as mean and standard deviation (±SD) and comparisons between groups were performed using Student’s t-test and analysis of variance for multiple groups (ANOVA). For continuous variables exhibiting skewed distribution, differences in the data were tested using Mann-Whitney U test or Kruskal-Wallis test. Categorical data were summarized as counts with relative frequencies as percentages and differences in the groups were analyzed using Chi-squared test (χ2 test) or Fisher’s exact test. First, we performed a univariate logistic regression analysis to examine the crude association between significant placental lesions and the clinical outcomes. Following this, an adjusted model was developed using the variables in the univariate logistic regression and then a multivariate logistic regression analysis was carried out. To avoid the multi collinearity, GA was not included in the model since it exhibited a significant positive correlation with BW. A p-value < 0.05 was considered statistically significant for all the analysis. All the statistical analyses were performed in SPSS software (version 27).
Results
We reviewed the medical charts and placental pathology reports of 107 inborn infants with a diagnosis of medical or surgical necrotizing enterocolitis (Fig. 1). Their mean GA was 28.1±3.7 weeks, with a mean birth weight of 1103±647 g. The cohort of infants was predominantly African American (n = 81, 77%), male (n = 58, 54.2%) and born by cesarean delivery (n = 86, 80.4%) (Table 1).
Clinical and demographic characteristics of cohort
Clinical and demographic characteristics of cohort
N is the number of patients in the column and the number in parenthesis is the percent of patients. †Values are the median and 25th, 75th centiles. **Data analyzed by Fisher exact or χ2 test; medians analyzed using Mann-Whitney U-test. P-values compare values for Medical and Surgical NEC cases.
The median age of NEC onset was 17 days (IQR 8, 30). Seventy-three neonates (68.9%) had abdominal distension as the presenting symptom. The abdominal x-ray showed pneumatosis in fifty-three (50.5%) and portal venous gas in eight (7.6%) cases. The blood culture obtained at the time of NEC onset was positive in twenty-two (20.6%) infants. Cholestasis (direct bilirubin > 2 mg/dL) at any time following NEC onset was seen in twenty-nine (35.4%) infants. The mean length of hospital stay was 90 (IQR 44, 134) days, and twenty-five neonates (31.6%) had WMI on the brain MRI at term equivalent age. Twenty-three neonates (21.7%) died in our study cohort.
Fifty-nine neonates (55%) had medical NEC and 48 (45%) had surgical NEC. The neonates with surgical NEC had significantly lower median GA (26 wks. [IQR 24, 30] vs. 28 [IQR 26, 32]; p = 0.02), lower birth weight [IQR 725 gm (593, 1285) vs. 1040 gm (IQR 700, 1660); p = 0.02], and more likely to have a patent ductus arteriosus (60.4% vs 36.2%; p = 0.01), 24 hours dopamine support (68.1% vs 21.4%; p < 0.001), extended days on parenteral nutrition (77 days [52, 113] vs. 34 [22, 44]; p < 0.001) and cholestasis (56.4 vs 16.3; p < 0.001). Neonates with surgical NEC had significantly longer length of stay (121 days [73, 180] vs. 75 [39, 107]; p < 0.001) and higher mortality (31.9 vs 13.6; p = 0.02). The occurrence of WMI on brain MRI was higher (43.8% vs. 23.4%) in neonates with surgical NEC. The demographic and clinical information are summarized in Table 1.
In our institution, the baseline incidence of acute histologic chorioamnionitis is 9.6% (Vermont Oxford network hospitals – median 7 [IQR 1.8,15.1]) and maternal hypertension 69.6% (Vermont Oxford network hospitals median- 34.8 [26.1,42.3]). In this cohort of preterm infants with NEC, maternal vascular malperfusion (82/107, 76.6%) was the most common placental histopathologic lesions followed by acute histological chorioamnionitis (42, 39.3%). Acute histologic chorioamnionitis with fetal inflammatory response was seen in the placentas from 26 (24.3%) neonates. Fifty-three neonates (49.5%) had multiple placental pathologic lesions and 48 (44.9%) neonates had single placental pathologic lesions. The incidence of other placental pathologic lesions is summarized in Table 2. Neonates with surgical NEC were twice as likely to have acute chorioamnionitis with fetal inflammatory response than neonates with medical NEC (35.4% vs 15.3%; p = 0.02). The occurrence of other lesions did not different between the two groups (Table 2).
Placental pathology characteristics of cohort
Placental pathology characteristics of cohort
*The data are presented as the number of neonates in the column with values in parenthesis as the percent of total in the column. **P values compare Medical and Surgical NEC using Fisher exact or χ2 test used for analysis.
On subgroup analysis, we compared the clinical and demographic information between the two groups neonates with surgical NEC based on acute histologic chorioamnionitis with and without fetal inflammatory response. We did not any find any significant clinical and demographic differences except for lower rate of pregnancy-induced hypertension and cesarean section rate in neonates with acute histologic chorioamnionitis with fetal response. The data are summarized inTable 3.
Clinical differences in neonates with and without chorioamnionitis with fetal response in surgical NEC
Clinical differences in neonates with and without chorioamnionitis with fetal response in surgical NEC
#N is the number of patients in the column and the number in parenthesis is the percent of patients. †Values are the mean and 25th, 75th centiles. Data analyzed by Fisher exact or χ2 test; student t-test. *P-values compare values for chorioamnionitis with and without response in neonates with Surgical NEC.
When we compared the placental pathology in non- survivors (23, 21.4%) and survivors (84, 88.6%). There was no association between placental histopathology and death in preterm infants with NEC (Table 4).
Placental findings in survivors vs. non - survivors
Placental findings in survivors vs. non - survivors
*n (%) is the number of patients in the column and the number in parenthesis is the percent of patients. Data analyzed by Fisher exact or χ2 test; P-values compare values for death and alive neonates with surgical NEC.
In our study population, seventy-nine infants qualified for term equivalent MRI brain scans. The 25/79 infants (31.6%) had WMI and were compared with neonates without WMI (54/79, 68.3%). WMI was associated with a significantly higher incidence of acute histologic chorioamnionitis as compared to infants without WMI on brain MRI (52% vs 27.8%; p = 0.04). No other placental pathologic lesion was significantly associated with WMI in the two groups of neonates with NEC (Table 5).
Placental pathology in neonates with and without white matter injury in neonates with medical and surgical NEC
Placental pathology in neonates with and without white matter injury in neonates with medical and surgical NEC
*n (%) is the number of patients in the column and the number in parenthesis is the percent of patients. Data analyzed by Fisher exact or χ2 test; **P-values compare values for with and without white matter injury in neonates with surgical and medical NEC.
On unadjusted logistic regression, acute histologic chorioamnionitis without fetal inflammatory response was also associated with higher odds of WMI (OR 2.81; 95% CI 1.05–7.54; p = 0.039). However, on adjusted logistic regression, acute histologic chorioamnionitis without fetal inflammatory response was not significantly associated with higher odds of WMI (OR 2.68; 95% CI 0.98–7.32; p = 0.055; Table 6).
Multivariate logistic regression analysis for WMI
*Adjusted for birth weight.
The association of placental pathology with the clinical outcomes in preterm infants with NEC is poorly studied. In our cohort of preterm infants with NEC, we noted that infants with surgical NEC had poor clinical outcomes. When we examined placental pathologic lesions, acute histologic chorioamnionitis was associated with increased odds of surgical NEC, but had no significant effect on postoperative outcomes, length of stay or death before discharge from the hospital. However, acute histologic chorioamnionitis was associated with the presence of WMI on MRI brain scans in infants diagnosed with NEC. These observations suggest an association between prenatal exposure to acute intrauterine inflammation and the pathogenesis, severity, and clinical outcomes of NEC in preterm infants.
Our study suggests that placental inflammation with evidence of a fetal response may place the fetal intestine at greater risk of subsequent injury, when exposed to NEC-related stimuli such as formula feeds, sepsis, or platelet/red blood transfusions after birth. Thus, supporting the double hit model hypothesis for surgical NEC [10]. Placental pathologic evidence of a fetal inflammatory response includes the presence of fetal neutrophils within the muscular walls of veins and/or arteries in the chorioamniotic plate and/or umbilical cord [24, 25]. Cute histologic chorioamnionitis with fetal inflammatory response is associated with systemic inflammatory responses in the fetal circulation in the form of an exaggerated proinflammatory cytokine response [26]. Intrauterine exposure to proinflammatory cytokines may switch the fetal innate immunity cells, such as macrophages, to a reactive phenotype (priming). Such sensitized cells can sustain an exaggerated production of proinflammatory cytokines when reconfronted with renewed postnatal inflammatory stimuli(two-hit hypothesis). The development of fibrin deposition in response to endothelial damage of the placental vasculature due to vasculitis may form part of the mechanism linking chorioamnionitis with a fetal response and postnatal development of NEC or intestinal injury [27, 28]. Many investigators have reported an association between activation of inflammatory pathways in the fetal circulation via cytokines and subsequent neonatal morbidity and mortality [27, 29–31]. Satar, et al. [29] reported that infants with NEC had higher IL-8 levels in their umbilical cord blood when compared to those without NEC (p < 0.05). In another study, elevated levels of IL-6 in umbilical cord blood predicted early-onset sepsis in preterm neonates, suggesting the role of an altered intrauterine environment affecting the fetus and subsequent postnatal outcomes [30]. The higher levels of cytokines in mixed umbilical cord blood in these studies could be fetal or maternal/placental in origin. It is notable that we reported that proinflammatory cytokines (IL-6, and IL-8) increase in the umbilical arterial blood during normal parturition in uncomplicated term pregnancies [32]. Thus, the inflammatory cytokines IL-6 and -8 are derived from the fetus and not either the mother or placenta. Moreover, there was 100% non-saturable placental clearance over the range of blood concentrations measured [32]. In a recently published study, we observed that in the presence of clinical chorioamnionitis, there is marked elevation in the umbilical arterial concentrations of IL-6 and IL-8, and placental clearance falls to 65%, not only demonstrating a fetal source, but also concentration-dependent clearance with saturation of the clearance mechanisms at very high concentrations [33]. However, these findings need to be studied further to make conclusions about the source of cytokines in umbilical cord blood in pregnancies complicated bychorioamnionitis.
In our study, infants with NEC were more likely to have evidence of WMI on brain MRI scans, which may also be related to the enhanced fetal inflammatory responses and the subsequent postnatal inflammatory surge secondary to the development of surgical NEC [34–37]. Salas et al. reported that subacute necrotizing funisitis (risk ratio 1.87; 95% CI, 1.04–3.35; P = 0.04) and chorionic plate vasculitis with thrombosis (risk ratio 2.21; 95% CI, 1.10–4.46; P = 0.03) were associated with severe neurodevelopmental impairment/death [34]. Korzeniewski et al. proposed a multi-hit model of neonatal WMI, suggesting that chronic placental inflammation, acute fetal inflammation, and postnatal inflammatory conditions such as surgical NEC might contribute to the risk for WMI and/or directly damage the developing brain of neonates delivered very preterm [38, 39]. In contrast, Bierstone, et al., did not find an association between histologic chorioamnionitis and WMI or cognitive or motor neurodevelopmental outcome at 18 to 24 months corrected age after accounting for perinatal factors [40]. Of interest, Niño, et al., studying a mouse model of NEC identified a gut-brain signaling pathway in which activation of intestinal TLR4 signaling led to release of high-mobility group box 1 in the intestine that, in turn, promoted microglial activation in the brain and neurological dysfunction [35].
To our knowledge, this is the first study to examine the impact of placental histologic pathology in preterm infants on postoperative outcomes and brain injury following NEC in a predominantly African American population using a uniform classification of placental pathologic lesions. We acknowledge that our study is limited by its single-center and retrospective design. The relatively small sample size may also reduce the generalizability of the study outcomes and the statistical power to detect associations between histopathology and NEC. MRI brain scans of only ∼73% of the patient population was available, and that might have biased theresults.
In conclusion, in this single center retrospective cohort of predominantly African American preterm infants with NEC, acute histologic chorioamnionitis was associated with WMI on brain MRI at term equivalent age. However, there were no significant effects on postoperative recovery, length of stay or mortality. In addition, infants with WMI on MRI brain scans obtained at term equivalence also had a greater incidence of acute histologic chorioamnionitis. In the future, prospective multi-center studies, which include additional clinical, maternal and laboratory predictors, such as fetal and neonatal serum inflammatory biomarkers, may improve our understanding of the mechanisms associated with the presence of prenatal placental pathology and the subsequent development of NEC and its impact on postoperative and brain injury outcomes. There is need to better understand the inflammatory surge and response in postnatal life to identify the at-risk infants for surgical NEC timely and develop better immunomodulatory approach for theseinfants.
Author contribution
P.M. Garg designed, collected, analyzed, and wrote the manuscript.
J. Paschal: Collected/analyzed the data and wrote the manuscript. M.A.Y Ansari: Analyzed the data and wrote the manuscript. Jennifer Ware, Kristin Adams, Charlotte Taylor, Kartik Reddy, Charles R. Rosenfeld, Imran N. Mir collected and analyzed the data and wrote the manuscript.
All authors approved the manuscript.
Funding
Dr. Parvesh Garg is partially supported by the National Institute of General Medical Sciences of the National Institutes of Health under Award Number 5U54GM115428. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Consent
Patient consent was not required for de-identified retrospective data.
Footnotes
Acknowledgments
We would like to thank Dr. Redline from Case Western University and Dr. Suhas Kallapur from UCLA for all the guidance for the project.
Conflicts of interest
The authors disclose no conflicts.