
Abstract
Background
To reduce avoidable Special Newborn Care Unit (SNCU) admissions by 15% over a 4-month period through focused quality improvement (QI) interventions at a high-volume tertiary care hospital in Kolkata, India.
Methods
This QI study was conducted from August to November 2024. Baseline data revealed that 25% of weekly SNCU admissions were avoidable. A multidisciplinary team implemented evidence-based admission criteria, enhanced perinatal care practices, and strengthened postnatal monitoring. Key interventions included improved delivery room practices (respiratory support with CPAP, delayed cord clamping, early skin-to-skin contact, and early initiation of breastfeeding) and standardized triage protocols. Feeding support, prefeeding oromotor stimulation, antibiotic stewardship, and reverse transport to nearby SNCUs were also integrated. Four Plan-Do-Study-Act (PDSA) cycles supported infrastructure planning, staff training, protocol implementation, and sustainability.
Results
Avoidable admissions declined from 25% to 10% over 4-months. Bed occupancy dropped from a peak of 125% to 102%. Process indicators improved significantly: delayed cord clamping increased from 30% to 88%, early initiation of breastfeeding from 40% to 90%, and exclusive breastfeeding at discharge from 67% to 81%. Admissions for neonatal jaundice decreased following the implementation of updated AAP guidelines, with 21% of cases managed without phototherapy. Only five re-admissions (0.59%) and one emergency NICU transfer (0.13%) occurred.
Conclusions
Neonatal care should extend beyond SNCU optimization to include strengthened delivery point and postnatal-ward practices. When integrated with protocol based SNCU management, this continuum helps reduce morbidity, ease overcrowding, enhance efficiency, and optimize resource utilization in high-burden, resource-limited settings.
Keywords
Introduction
Special Newborn Care Units (SNCUs) constitute a critical component of India’s healthcare infrastructure, providing specialized care for sick and low birth weight neonates (<1800 g) who do not require advanced respiratory support or surgical intervention. 1 SNCUs are typically located in district hospitals, sub-district hospitals, and medical colleges. India currently has 1087 SNCUs, with 69 situated in West Bengal. 2
India has made notable progress in reducing child mortality, with the under-five mortality rate (U5MR) dropping by 49% and the neonatal mortality rate (NMR) by 38% between 2000 and 2017. While current trends suggest India may achieve the Sustainable Development Goal (SDG) target for U5MR by 2030, the slower decline in NMR indicates the country is unlikely to meet the SDG target of 12 per 1000 live births. 3 This disparity underscores the need for greater focus on neonatal deaths, particularly in the early neonatal period, which accounted for nearly 80% of neonatal deaths in India in 2017. 3 The availability of Level 2 and Level 3 neonatal care beds remains grossly inadequate. In some public hospitals, SNCUs are overcrowded, with up to five sick neonates sharing a single radiant warmer bed. 4 Many of these admissions involve stable neonates with mild conditions that could be safely managed in postnatal wards or through enhanced monitoring protocols, without the need for SNCU admission. While structural deficiencies persist, quality improvement initiatives focused on process optimization can play a vital role in maximizing available resources and enhancing outcomes. As part of the National Health Mission (NHM), India, facility-based newborn care has been prioritized to improve neonatal outcomes. 5 The MusQan quality improvement initiative under NHM further strengthens this framework by implementing standardized protocols to enhance service delivery in SNCUs. 6
Admission rates to Level 2 and 3 neonatal units have increased even in developed countries. 7 Near-term and term infants form the largest share of admissions, yet most do not present with high-acuity illness. 8 Variability in illness severity suggests that admission practices often reflect institutional differences, raising concerns about overuse of resources and related consequences.8–10
Unnecessary admissions to the SNCU lead to overcrowding, strain on limited resources, and reduced care quality for critically ill neonates. They also cause avoidable mother-infant separation, hindering bonding and breastfeeding, and expose stable neonates to hospital-acquired infections.11,12
Common avoidable SNCU admissions and prevention strategies.
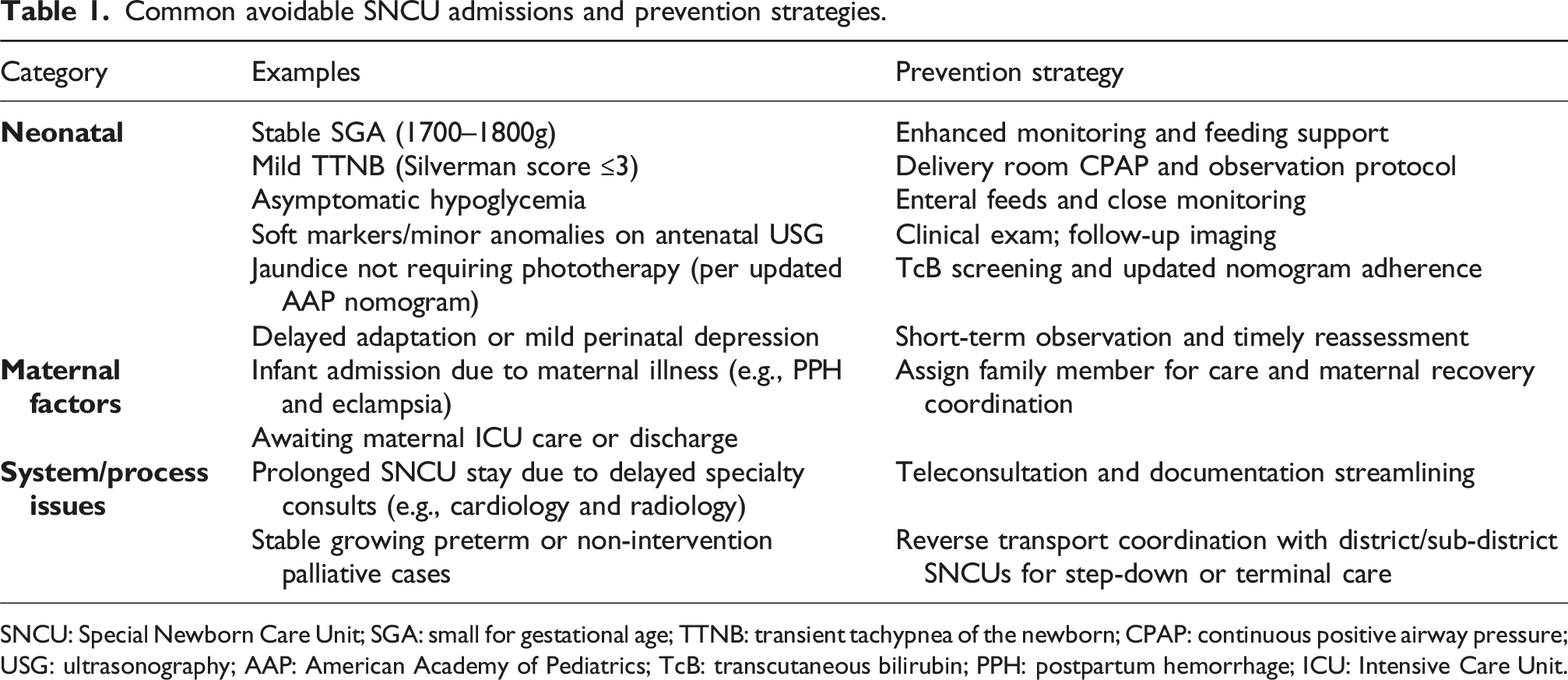
SNCU: Special Newborn Care Unit; SGA: small for gestational age; TTNB: transient tachypnea of the newborn; CPAP: continuous positive airway pressure; USG: ultrasonography; AAP: American Academy of Pediatrics; TcB: transcutaneous bilirubin; PPH: postpartum hemorrhage; ICU: Intensive Care Unit.
Methods
Context
The study was conducted in the department of neonatology at a tertiary care teaching hospital with a 100-bed neonatal unit comprising a 70-bed SNCU and a 30-bed Neonatal Intensive Care Unit (NICU). This quality improvement project was focused exclusively on the SNCU. The unit provides care for both inborn and out born neonates. In 2024, the hospital reported 6796 live births, with 2993 inborn and 770 outborn admissions to the neonatology department. The facility manages between 550 to 800 deliveries each month, with caesarean sections accounting for approximately 70% of all births.
Our SNCU admission data reveals three primary pathways: NICU step-down transfers (1-4 daily), postnatal ward referrals (2-8 daily), and direct admissions from labor/delivery rooms (2-4 daily). Notably, many postnatal referrals involve borderline cases such as asymptomatic hypoglycemia or delayed adaptation that could be managed with enhanced post-natal ward monitoring. Approximately 30-35% of weekly SNCU admissions originate directly from the delivery point, often as precautionary measures rather than due to clear clinical indications such as transient tachypnea or mild perinatal depression. Similarly, some labor room admissions are prompted by maternal indications rather than actual neonatal clinical needs. Targeted interventions in the delivery room can help reduce these unnecessary SNCU transfers while maintaining neonatal safety.
Intervention
The literature review and analysis of local admission trends informed the development of admission criteria and intervention strategies. The project design was guided by the Institute for Healthcare Improvement (IHI) Model for Improvement. A driver diagram (Figure 1) was used to identify key drivers and targeted interventions that were necessary to achieve the aim of reducing avoidable SNCU admissions. Driver diagram.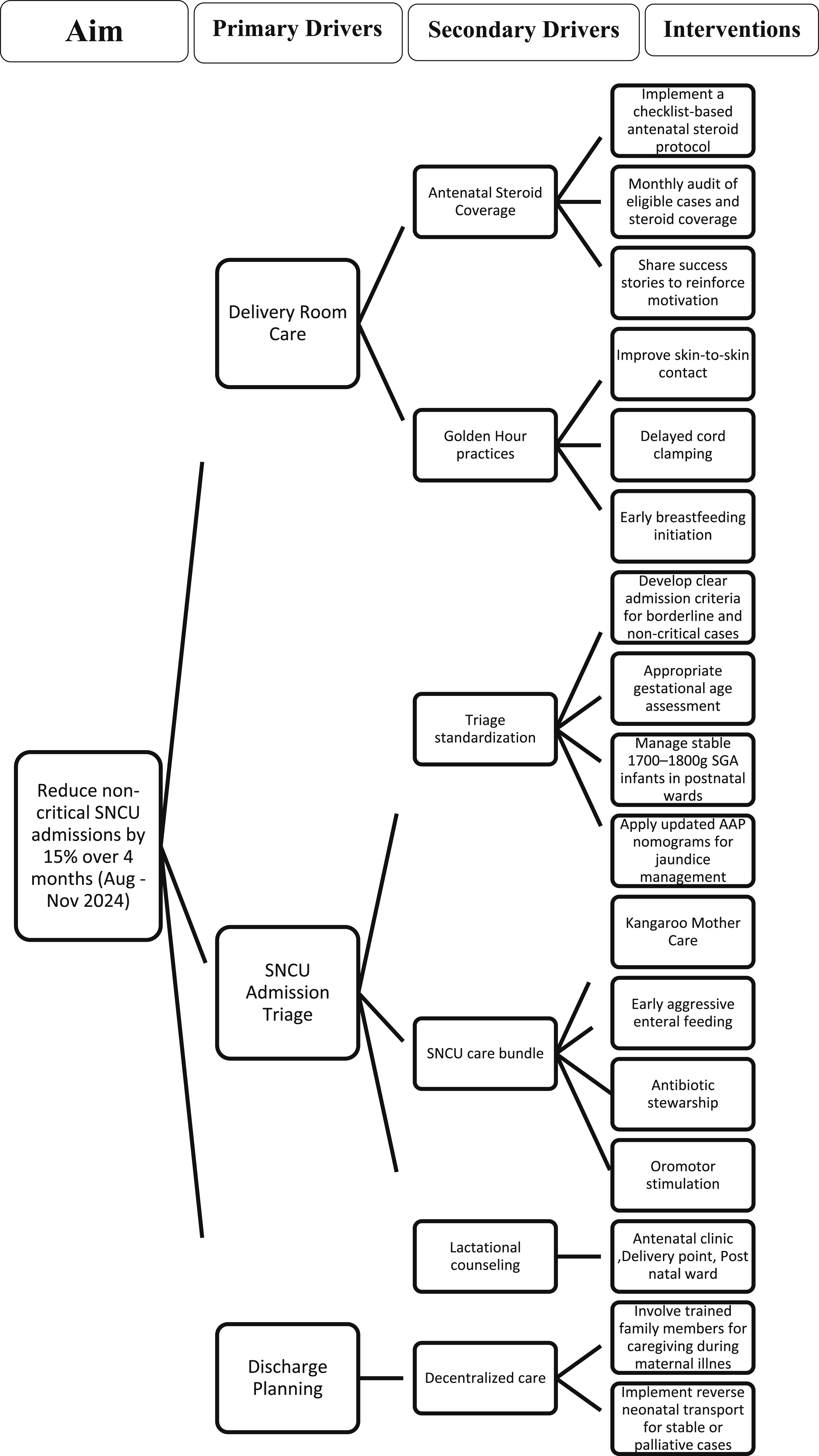
The challenges in the neonatal care system arose from both upstream perinatal care gaps and inconsistencies in SNCU admission decision-making. Antenatal steroid coverage remained insufficient, with only 10-15% of eligible mothers receiving the complete course. Immediate newborn care was also suboptimal, skin-to-skin contact occurred in fewer than 30% of deliveries, delayed cord clamping (DCC) in less than 20%, and early breastfeeding was often delayed. These deficiencies compromised neonatal stabilization and contributed to preventable SNCU admissions.
Borderline cases, such as stable SGA infants weighing 1700–1800g, and uncertain gestational age due to discrepancies between the last menstrual period and ultrasound dating, often led to over-admission. Infants initially admitted for short-term stabilization (e.g., delayed adaptation and mild perinatal depression) often remained in the SNCU longer than needed due to administrative delays. Additionally, cases involving isolated soft markers without major anomalies were frequently admitted unnecessarily. Limited pediatric super-specialty support further complicated care, delayed discharge planning, and increased the length of stay.
To address these issues, a targeted intervention strategy was implemented, focusing on both delivery room and SNCU-level improvements (Figure 1). Delivery room initiatives included checklist-based antenatal steroid protocols for mothers at 24–34 weeks of gestation (with audit-driven coverage >80%) and optimization of respiratory support through a protocol that directed neonates with mild respiratory distress (Silverman score ≤3) to receive CPAP stabilization in the delivery room, followed by continued monitoring in the postnatal ward instead of immediate SNCU admission. A standardized “Golden Hour” bundle was enforced to ensure 60s DCC, promote early initiation of breastfeeding (target >90% within 1 h), and encourage skin-to-skin contact.
Revised SNCU admission criteria prioritized evidence-based thresholds: birth weight <1800 g, gestational age <34 weeks confirmed by early ultrasound or Expanded New Ballard Score (applied when last menstrual period was uncertain), major structural malformations, perinatal asphyxia (cord pH <7.30 and base excess <–10), or respiratory distress (SpO2 < 90% with retractions/grunting despite 10–15 min of CPAP at delivery point). Stable SGA infants (1700–1800 g) and those with isolated soft markers were closely observed in the postnatal-ward, with escalation to SNCU only in cases of clinical deterioration. Admissions for neonatal jaundice followed gestational age-adjusted, updated AAP nomograms, while feeding issues related to maternal factors were managed with support from a lactation nurse.
Within the SNCU care bundle, respiratory management emphasized timely non-invasive support for RDS/TTNB (using nasal high flow upon admission) and prompt escalation to the NICU for CPAP/NIPPV support when indicated. For infants admitted for short-term stabilization, efforts were undertaken to streamline administrative procedures and ensure their prompt transfer to postnatal wards as soon as they were clinically stable. Nutritional protocols prioritized early, aggressive enteral feeding and kangaroo mother care (8–10 h per day for infants <2000 g). An active antimicrobial stewardship program was implemented, where empirical antibiotic therapy was guided by the local antibiogram. Standardized antimicrobial prescription forms were used, clearly documenting the indication, dose, duration, and route of administration. All antibiotic therapies were regularly reviewed and reassessed at 48–72 h to ensure continued appropriateness and necessity. In addition, strict infection prevention and control measures were enforced throughout the unit. Growing preterm infants and those requiring only palliative care were transferred to SNCUs closer to their families for continued non-critical care. Key gaps included inconsistent specialty input (e.g., neurology, cardiology, and radiology) and delays in diagnostic services. To mitigate these issues, teleconsultation, multidisciplinary review, and improved documentation pathways were incorporated to streamline care and reduce bottlenecks.
We had four plan-do-study-act (PDSA) cycles. The first cycle focused on problem identification and infrastructure planning, including baseline data analysis, formulation of evidence-based SNCU admission criteria, development of intervention protocols, and creation of data tracking tools. The second cycle, which ran concurrently with first cycle, emphasized staff training and consensus building through targeted sessions to ensure team alignment and protocol adherence. The third cycle marked the full-scale implementation starting in August 2024, with unit-wide adoption of revised triage protocols, improved delivery room practices, structured postnatal ward observation, and the updated AAP jaundice management guidelines. The fourth cycle focused on sustaining improvements by reinforcing successful practices, implementing reverse neonatal transport, and strengthening coordination with nearby SNCUs. It also aimed to improve collaboration with pediatric super-specialty services to reduce delays in evaluation and decision-making.
Outcome measure
Primary outcome
• Percentage Reduction in avoidable SNCU Admissions Target: 15% reduction over the 4-month intervention period (August to November 2024)

This measure reflects the proportion of admissions that could potentially be avoided through improved triaging and stabilization protocols at the delivery point.
Process measures
These track adherence to key components of the intervention: • Percentage of Antenatal Steroid Coverage among eligible preterm deliveries • Percentage of Skin-to-Skin Contact initiated within 5 min of birth • Percentage of DCC for ≥60 s • Percentage of Early Breastfeeding Initiation within 1 h of birth • Percentage of Stable 1700–1800 g Infants safely managed in the postnatal ward instead of being admitted to SNCU • Percentage of Eligible Infants Receiving KMC • Exclusive Breastfeeding at Discharge (for inborn SNCU infants) • Neonatal Jaundice Cases Managed Per Updated AAP Guidelines Without Admission • Infants Admitted with Antenatal USG Soft Markers/Minor Congenital Malformations • Infants Transferred to Facility Nearer to Home for Continuation of Care
Balancing measures
These ensure that changes made to reduce admissions do not unintentionally compromise neonatal safety: • Percentage of Re-admissions to SNCU from postnatal-wards within 48 h • Percentage of Emergency Transfers to NICU from Postnatal-Ward
Results
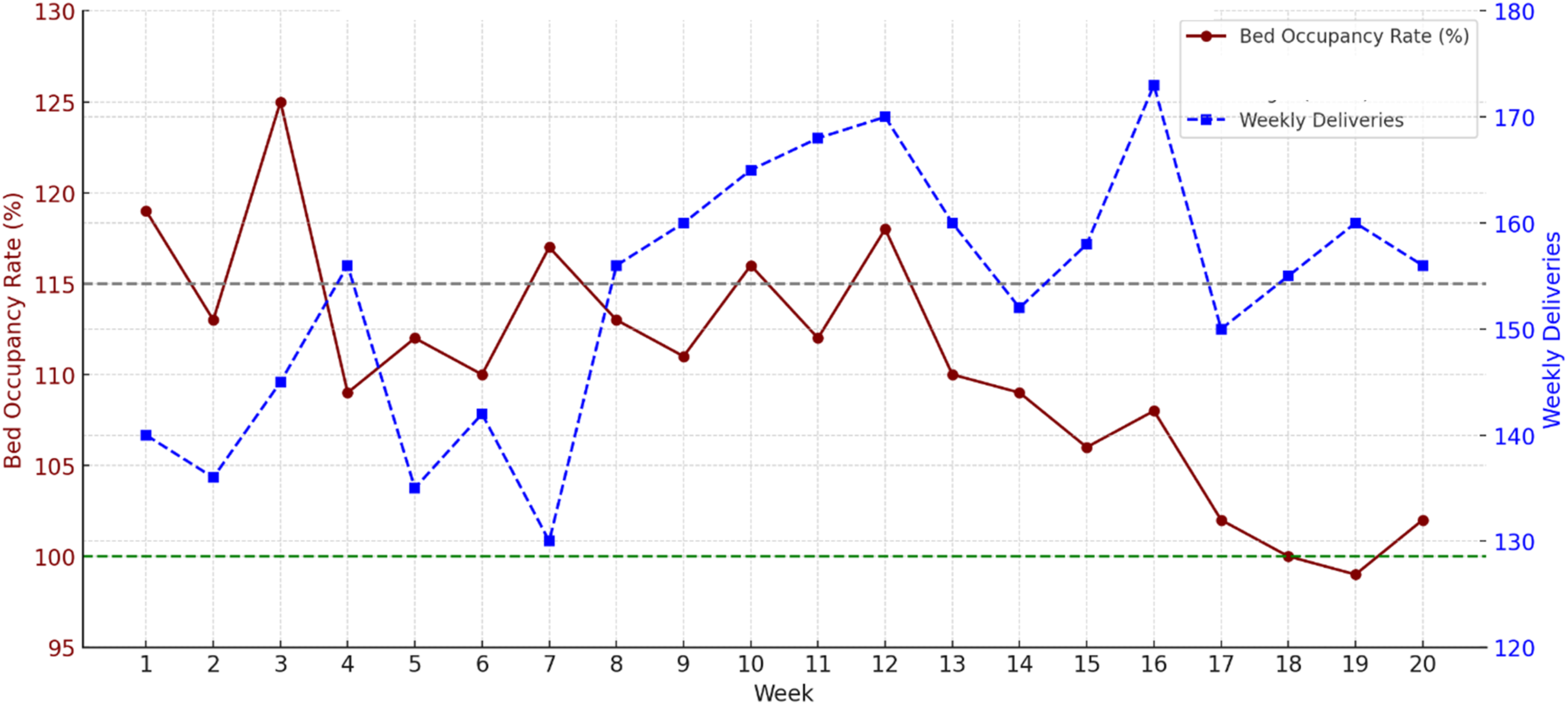
A total of 20 weeks of data (July to November 2024) were analyzed as part of this QI initiative. Baseline data from July 2024 showed that avoidable cases accounted for 25% of total admissions. Over the 16-week intervention period (August to November), this proportion steadily declined, reaching 10% by Week 16 (Figures 2(a) and 2(b)). Bed occupancy was notably high in July, peaking at 125% in Week 3, but decreased to 102% by Week 20 (Figure 3). As of writing this article, the occupancy rate at our SNCU has further dropped to between 75–95%, reflecting continued progress and sustained impact of the quality improvement measures. (a) RUN chart: Weekly avoidable SNCU admissions July–November 2024. (b) Run chart showing monthly mean avoidable SNCU admissions (July–November 2024) with 95% confidence intervals and statistical process control limits. RUN chart: Weekly bed occupancy rate and deliveries July–November 2024.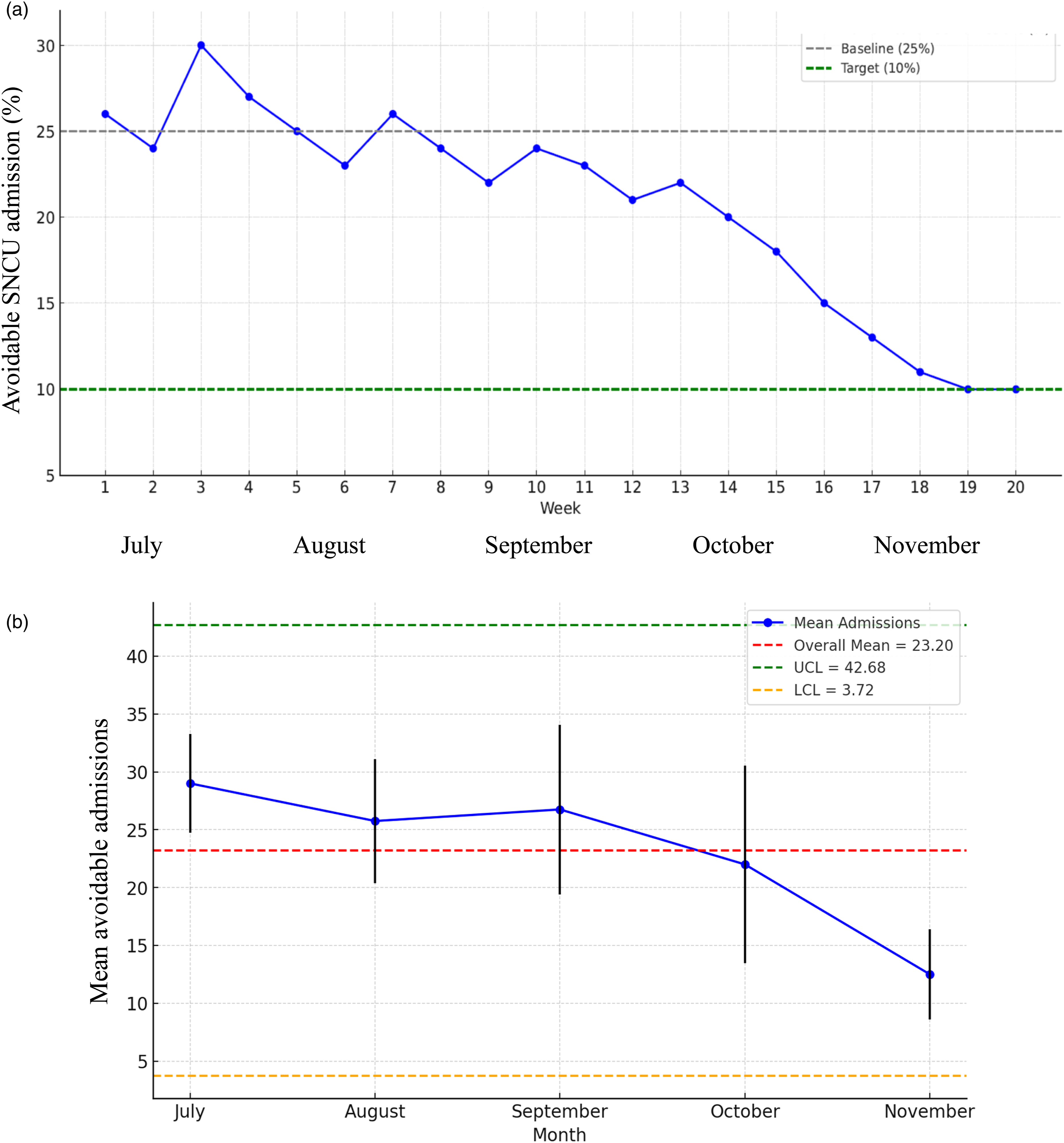
Summary of process and balancing measures (July–November 2024).
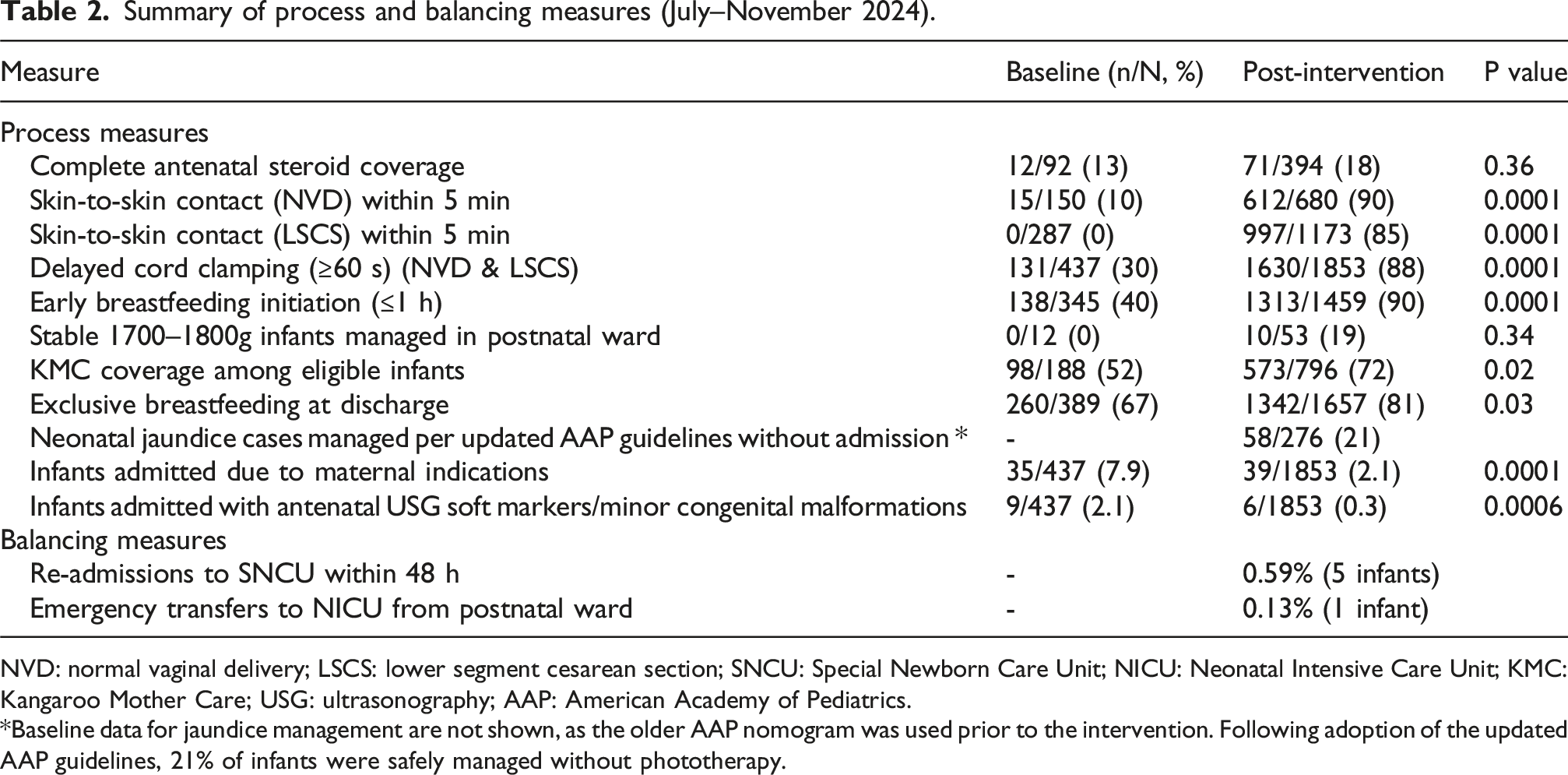
NVD: normal vaginal delivery; LSCS: lower segment cesarean section; SNCU: Special Newborn Care Unit; NICU: Neonatal Intensive Care Unit; KMC: Kangaroo Mother Care; USG: ultrasonography; AAP: American Academy of Pediatrics.
*Baseline data for jaundice management are not shown, as the older AAP nomogram was used prior to the intervention. Following adoption of the updated AAP guidelines, 21% of infants were safely managed without phototherapy.
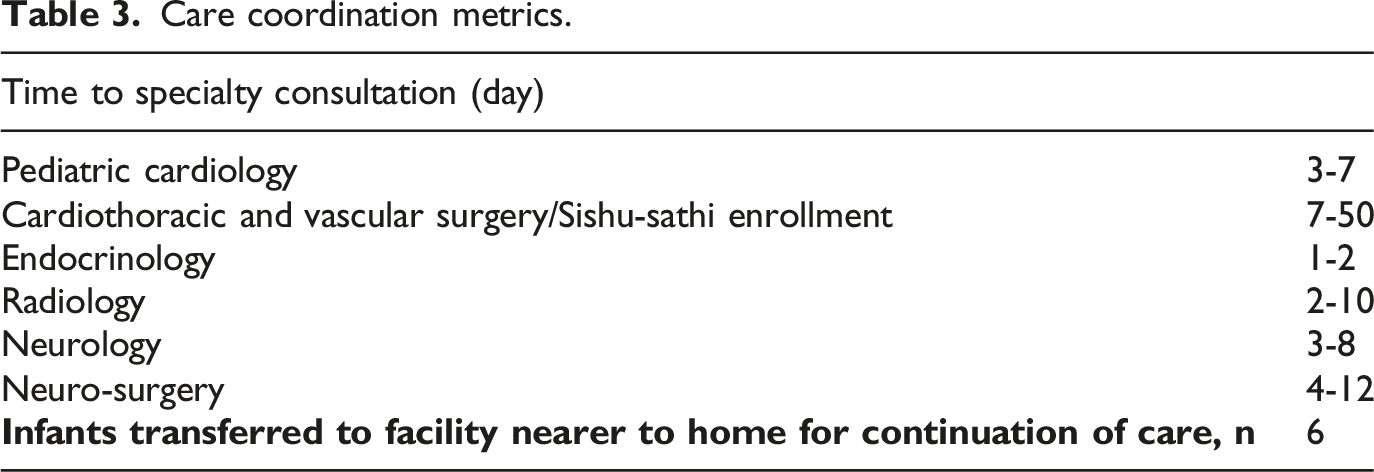
Care coordination metrics.
Discussion
This quality improvement (QI) initiative, conducted over a 4-month period, demonstrates that structured interventions targeting upstream perinatal care gaps, improved triaging, and evidence-based neonatal care practices within the SNCU can significantly reduce avoidable admissions. We achieved a meaningful reduction in low-acuity admissions from 25% to 10%, and a corresponding decrease in bed occupancy from a peak of 125% to 102%, with sustained improvement observed beyond the intervention window.
In high-volume centers like ours, many SNCU admissions occur due to precautionary practices, inadequate early stabilization at delivery, and unclear triage protocols. A major strength of our intervention was the focus on optimizing delivery room practices. Recognizing the critical nature of the “Golden Hour,” improvements in DCC, skin-to-skin contact, and early breastfeeding initiation led to reduced SNCU transfers and better thermoregulation, bonding, and with additional benefits for the immediate neonatal period and long-term developmental outcomes.13–15 DCC increased from 30% to 88%, and early breastfeeding from 40% to 90%, largely due to an ongoing QI initiative and a parallel randomized controlled trial. Improvements were also observed across nearly all tracked indicators, including a fivefold increase in the rate of skin-to-skin contact following cesarean delivery (0% to 85%), and a substantial rise in exclusive breastfeeding at discharge (from 67% to 81%).
Respiratory care optimization was another key driver. Timely initiation of CPAP at the delivery point, use of nasal high flow in the SNCU, and early escalation to NICU for CPAP/NIPPV minimized mortality, reduced the duration of respiratory support, and shortened hospital stays.16,17
Another critical component of our intervention was the consistent practice of antibiotic stewardship, which remains a cornerstone of care in our SNCU. This approach is particularly vital in high-volume units where overuse of antimicrobials is common and contributes to rising antimicrobial resistance, prolonged hospitalization, and microbiome disruption.18,19
We adopt early full enteral feeding for term neonates and early aggressive enteral feeding for preterm infants to ensure timely feeding establishment. 20 Conversely, the unnecessary use of intravenous fluids and oxygen, along with delayed initiation of feeding as observed in some SNCUs across the state contributes to slower unit turnover. To support feeding readiness, we also routinely perform prefeeding oromotor stimulation in preterm infants, which enhances feeding efficiency, reduces hospital stay, and improves breastfeeding outcomes. 21
Revised admission criteria based on birth weight combined with gestational age facilitated safe ward-based management of stable SGA infants. By adopting the new AAP nomogram (2022) and using ENBS or first-trimester ultrasound for accurate gestational age assessment when LMP was uncertain, we significantly reduced unnecessary SNCU admissions for phototherapy. However, successful implementation requires 24/7 access to total serum bilirubin testing or point-of-care devices, along with regular jaundice assessments in postnatal wards every 6–12 h, especially for at-risk infants. 22 Structured lactation support contributed to a drop in breastfeeding-related jaundice, and routine predischarge bilirubin screening combined with structured post-discharge follow-up further reduced hazardous hyperbilirubinemia risk.
Importantly, our balancing measures affirm the safety of these strategies. Re-admissions to the SNCU within 48 h were minimal (0.59%), and only one emergency NICU transfer was recorded. No adverse outcomes were linked to postnatal ward observation of stable infants.
Soft markers are sonographic findings that are structurally minor, nonspecific, and often transient, typically considered normal variants with minimal pathological significance. 23 Although they may occasionally be associated with underlying chromosomal abnormalities particularly when multiple markers are present, they are rarely life-threatening. The presence of a soft marker alone is not a justification for SNCU admission. In our practice, such infants are not routinely admitted to the SNCU. If further evaluation is needed, it is carried out either in the postnatal ward or during post-discharge follow-up.
We also addressed admissions due to maternal indications, which decreased from 7.9% to 2.1%. In cases of short-term maternal illness, infants were temporarily managed in the SNCU. For critically ill mothers, we engaged a designated family member as early as possible in participation in caregiving activities, oral feeding and kangaroo care as early as possible, under the supervision of nursing staff. Once the infants were clinically stable and adequate caregiver support was ensured, they were safely discharged. Family members beyond parents are key participants in family-centered care. 24 Involving them in caregiving, decision-making, and home support can improve neonatal outcomes. This approach is linked to better weight gain, shorter hospital stays, and potentially improved long-term development. 25
Care decentralization was also impactful. Reverse neonatal transport of stable preterm or palliative care infants to SNCUs nearer to home reduced bed burden and enhanced family integration.26–28 However, successful implementation required effective communication and coordination with the receiving facilities.
Despite these gains, persistent challenges remain. Complete antenatal steroid coverage remained low post-intervention (18%) due to late maternal presentation, poor coordination with referring centers, and occasional iatrogenic prematurity. Addressing these gaps remains a priority, especially as even a single dose within 24 h significantly improves neonatal outcomes. Efforts are ongoing to address these gaps, recognizing that even a single dose within 24 h of delivery significantly reduces neonatal morbidity and mortality. 29
The QI also highlighted persistent bottlenecks, particularly in specialty coordination and diagnostics. With in-house neonatal surgical support, procedures within the scope of neonatal surgery are performed in a timely manner. However, persistent delays in other specialty consultations, particularly in pediatric cardiology and cardiothoracic and vascular surgery (CTVS), contributed to prolonged admissions. Many infants with critical CHD remain in SNCU for weeks to months awaiting evaluation or surgery. In India, approximately 2.4 lakh children are born with CHD annually, contributing to 10% of infant mortality. 30 Most cases are missed antenatally and present late with complications such as malnutrition, infections, anemia, pulmonary hypertension, and ventricular dysfunction, all of which negatively impact surgical outcomes. While timely diagnosis and treatment can ensure over 90% survival into adulthood with good outcomes, limited access to pediatric cardiology and cardiac surgery in government setups makes it challenging to provide timely surgical repair or palliation for many CHD cases. 31 Although the Sishu Sathi Scheme offers free cardiac surgeries at designated private hospitals in West Bengal, delays in approval and scheduling limit its impact. 32 To address these systemic gaps, strengthening structured referral pathways, enhancing collaboration with pediatric cardiology and CTVS services (including private centers with specialized expertise), and streamlining Sishu Sathi scheme approval and scheduling through state-level coordination will be essential to reduce waiting times and improve outcomes.
This study has several limitations. As it was conducted in a single tertiary care hospital, the findings may not be generalizable to smaller or resource-constrained settings. In addition, the before-after design without a control group introduces potential biases, including the Hawthorne effect and regression to the mean, which should be considered when interpreting the results. The definition of “avoidable admissions” was adapted locally and, although derived from Facility-Based Newborn Care (FBNC) admission criteria under the National Health Mission (NHM, India), was not externally validated; inter-rater reliability was not formally tested, which may introduce classification bias. 33 The study also did not include qualitative feedback from parents or caregivers, limiting insights into family-centered care and reverse transport experiences. Furthermore, certain interventions such as delivery room CPAP and transcutaneous bilirubin screening may not be easily replicable in all public hospitals due to staffing or equipment constraints. Balancing measures were limited to 48-h re-admissions, without capturing later complications (e.g., hyperbilirubinemia and feeding intolerance), mortality, or severe morbidities (e.g., culture-proven sepsis, NEC, and IVH), which restricts comprehensive safety assessment. Lastly, the improvements reported here were measured over a relatively short post-intervention period, and data on long-term sustainability are lacking. Continued monitoring, periodic audits, and integration into existing health system frameworks will be essential to sustain and scale these gains across different settings.
This QI study was conducted in parallel with other ongoing initiatives, including two studies focused on cord management practices.34,35 One of these overlapped with the current QI project and may have contributed to observed improvements in Golden Hour care. However, as it was limited to a highly specific subgroup (preterm infants with twin gestations), its impact on the primary outcome of reducing avoidable SNCU admissions is likely to have been minimal.
UNICEF recommends a minimum of 12 SNCU beds for hospitals with over 3000 annual deliveries, with 4 additional beds per 1000 extra births, a practical and justified standard. 36 However, SNCU bed shortages often stem not just from limited infrastructure, but from low turnover due to avoidable admissions and delayed discharges. This QI study underscores how avoidable admissions significantly impact bed availability for critically ill neonates.
While neonatal care often centers on optimizing SNCU practices, our findings highlight the equally important yet frequently overlooked need to strengthen care at the delivery point and within postnatal-wards. Improvements in perinatal care must be supported by consistent postnatal monitoring and timely support. Just as crucial is the strict adherence to standardized, protocol-driven care within the SNCU. In resource-limited environments, reinforcing this continuum of care from birth through postnatal observation to specialized SNCU support can meaningfully reduce neonatal morbidity, relieve overcrowding, and improve the overall efficiency of neonatal services.
Footnotes
Authors’ contributions
Dr. Md Habibullah Sk: Conceptualized and designed the study, did data collection and analysis, and drafted the initial manuscript.
Dr. Bijan Saha: Contributed to protocol development, data interpretation, and critical revision of the manuscript for important intellectual content.
Dr. Anindya Kumar Saha: Participated in study design, coordinated implementation of quality improvement interventions, and contributed to data analysis and manuscript editing.
All the authors approved the final manuscript as submitted and agree to be accountable for all aspect of the work.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data supporting the findings of this study are available from the corresponding author upon reasonable request.