
Abstract
Delayed cord clamping has been shown to be beneficial in both preterm and term babies. Practice guidelines have not been consistent between centers and the practice of delayed cord clamping has not been standardized. The concept of physiologic-based cord clamping emerged into practice as well. Cord milking has different physiological effect and might be harmful in preterm babies.
Abbreviations
American College of Obstetricians and Gynecologists American Heart Associatione Blood pressure Cerebral blood flow Congenital diaphragmatic hernia Canadian Paediatric Society Delayed cord clamping Data and Safety Monitoring Board Extremely low birthweight Immediate cord clamping Intra-thoracic pressure Intrauterine growth restriction Necrotizing enterocolitis The National Institute for Health and Clinical Excellence Neonatal Resuscitation Program Physiology-based Cord Clamping Pulmonary blood flow Patent ductus arteriosus Postpartum hemorrhage Pulmonary vascular resistance Retinopathy of prematurity Right ventricular output Systemic vascular resistance Umbilical cord clamping Umbilical Cord Milking World Health Organization
Introduction
Delayed cord clamping (DCC) as well as milking were described historically [1] with consideration against immediate clamping of the cord [2, 3]. Despite better understanding of potential benefits, DCC was not introduced into clinical practice for many reasons. First, immediate clamping was believed to prevent hemolytic disease of newborn by limiting excessive amounts of maternal antibody-containing blood from entering the neonate. Similarly, due to increased incidence of significant hyperbilirubinemia needing phototherapy in general, which is by far, the most reason for the hesitance in doing DCC in term or near-term babies. Second, there was a rush to assess the baby at 60 seconds after birth for initial scoring of APGARs [4, 5], as DCC was deemed a part of ‘slow delivery’, the language suggesting that delaying is unwise or unnatural. Third, it was believed that keeping the cord intact contaminates the ‘sterile field’. Lastly, there was a perception that DCC would result in more transfer of anesthetics to the infant.
The definition of delayed cord clamping is variable based on when to clamp. This can range from anywhere between 30 seconds to as long as 5 minutes or even until the cord stops pulsating [6]. More recently, with better understanding of the physiological effects of delayed cord clamping, physiological definition appeared.
Prior to recent understanding of the physiologic effects and benefits of DCC, the American College of Obstetricians and Gynecologists (ACOG) released directives advising for ICC in 2002. Also, the National Institute for Health and Clinical Excellence (NICE) recommended early clamping in their 2007 intrapartum care guideline [7]. However, those recommendations were not based on physiologic rationale and probably reflected lack of understanding of the potential benefits.
Methods
Comprehensive literature search was performed using MEDLINE December 2019 by using the keywords “Delayed Cord Clamping”, “Cord Milking”, and including all trials, reviews, clinical practice guidelines, follow-up studies and meta-analyses. The Cochrane Database was searched for reviews and articles relating to the cord management. Also, there was a manual search of abstract published from the Society of Pediatric research (SPR) and the European Society of Pediatric research (ESPR). The population of interest included newborns, both term and preterm infants.
The hierarchy of evidence from the Centre for Evidence-Based Medicine (http://www.cebm.net/) was applied to the publications identified. Recommendations are based on the format developed by Shekelle et al. [8].
Physiology of blood distribution after birth
Following umbilical cord clamping (UCC), there is an increase in the systemic vascular resistance (SVR) due to the occlusion of the umbilical arteries. This results in afterload increase on both right and left ventricles and a sudden increase in arterial blood pressure (BP) within only few minutes and as a result, there is a rapid increase in cerebral blood flow (CBF) [9].
On the venous side, cord clamping results in loss of the venous return due to occlusion of umbilical vein, which significantly reduces ventricular preload on both ventricles (mainly if done before lung aeration). The later, combined with the increase in afterload, greatly reduces the cardiac output. This state of low cardiac output persists until the lungs aerate and pulmonary blood flow increases to restore ventricular preload [10] (Fig. 1).
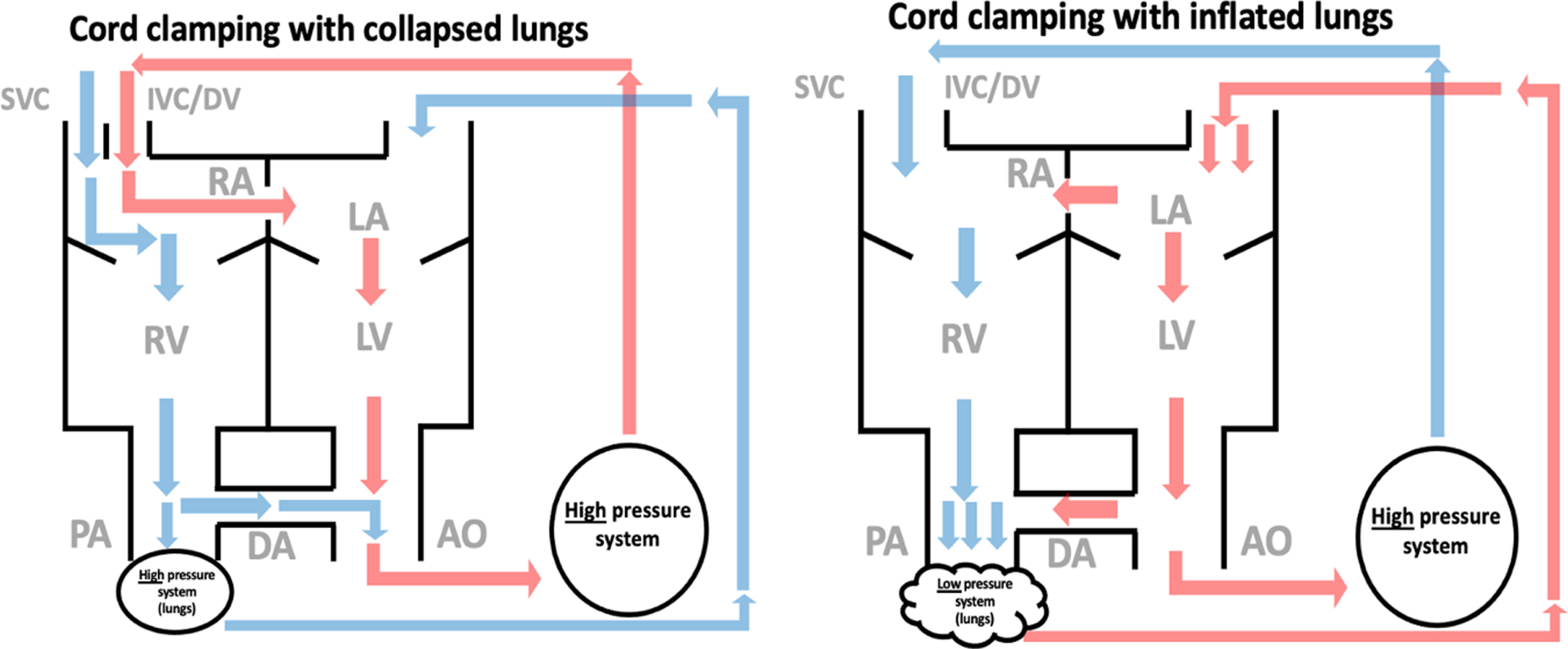
Blood distribution after birth.
There are a few factors that impact blood distribution from the placenta to the newborn infant following birth. First is gravity, as placing the infant below or above the placenta was thought to increase or decrease the blood flow towards the infant. However, animal studies found no significant placental-to-newborn transfusion because the blood flow changes in both directions (umbilical vein and artery) making the net flow non-significant [11]. These findings are consistent with a clinical trial in humans showing no effect of placing infants above the mother on placental transfusion [12]. Second, the role of uterine contractions which is not simply a squeezing phenomenon. The venous system in the placenta is highly compliant, so during contraction, placental veins close earlier than the arteries and also take longer to reopen when the uterus relaxes [13]. As a result, the placental blood volume increases during contraction and then gets released back into the infant following the contraction when the veins open. Third, the increase in the pulmonary blood flow might shift a significant volume of blood from systemic blood flow through the fetal shunts during lung inflation, so if the lung aeration happens while cord is still intact, then a significant volume of cord blood might be added to the infant to compensate to the shifted volume [14]. Fourth, the intra-thoracic pressure (ITP) changes that arise during inspiration and crying influences the flow of blood. With inspiration and crying, and due to enhanced negative intra-thoracic pressure, the umbilical vein blood flow increases towards the infant with decreasing flow during expiration and vigorous crying. The flow in the umbilical artery is different as it is pulsatile and bidirectional, towards the placenta during systole, and away from the placenta during diastole [15]. Lastly, the timing of umbilical cord clamping is proportionally related to the blood volume following birth [16]. In a randomized trial, Aladangady et al. found that infants’ mean blood volume in the DCC group (74.4 mL/kg) was significantly greater than that in the ICC group (62.7 mL/kg; 95%confidence interval for advantage: 5.8-17.5) [17].
DCC has been shown to improve oxygen saturations (SpO2) and attenuate the swings in blood pressure and cerebral blood flow seen in ICC [18]. After birth, if the infant is still connected to a functioning placenta that continues to provide gas exchange and left ventricular preload, one might expect infants with DCC to have higher heart rates and higher SpO2 . A few small studies have reported the heart rate and SpO2 immediately after birth, in preterm and term infants who receive DCC. Winter et al. reported all infants maintained heart rate greater than 100 BPM at 60 seconds in a small pilot trial suggesting feasibility of DCC while providing respiratory support in infants less than 32 weeks [19].
Another potential mechanism for the benefits of delayed cord clamping is the relation with the superior vena cava (SVC) flow. In a small nested study by Sommers et al., DCC improved SVC flow compared to ICC [20]. Also, DCC has been reported to be associated with higher SVC flow in an observational study in preterm infants [21, 22]. It is known that SVC flow less than 30 ml/kg/min is associated with abnormal cerebral ultrasound findings such as extending of early IVH, late IVH and PVL [23] and low superior vena cava flow was associated with worse neurodevelopmental outcomes at 3 years of life [24]. This indirect relationship between delayed cord clamping and the flow in the SVC might explain some of the benefits of delayed cord clamping.
Delayed cord clamping is not merely placental transfusion of blood towards the infant. There is a body of evidence suggesting short and long-term benefits for delayed cord clamping. A Cochrane review by Rabe et al. found that delayed clamping is associated with higher mean arterial blood pressure at 4 hours of life compared to the early clamping [25] (level 1a). Also, there was less need for inotropic support and less blood transfusion in context of low blood pressure [25] (level 1a). Besides, infants who received delayed cord clamping were less likely to have respiratory distress [26] (level 1a). There is evidence that delayed cord clamping is associated with decreased incidence of brain injury specifically intraventricular hemorrhage (all grades) [25, 27] (level 1a), necrotizing enterocolitis(NEC) [25] (level 1a), decreased incidence of retinopathy of prematurity (ROP) [25] (level 1a).
There are a few studies reporting neurodevelopmental outcomes of DCC and UCM in preterm infants. Mercer and colleagues have published two studies finding that DCC up to 45 seconds versus ICC improves motor function at 18 months as assessed by the Bayler scales of infant and toddler development in preterm infants less than 32 weeks’ gestation [28, 29] (level 1b). Interestingly, improvement in motor function after DCC was more profound in male infants. Other trials reported some long term benefits as well at 4 months [26] (level 1a), and 2 years of age [30] (level 1b). This is not clear whether it is related to the improvement in cerebral oxygenation that has been reported in infants undergoing DCC [31], keeping in mind that low regional cerebral tissue oxygen saturation in the preterm infants is associated with worse grades of intraventricular haemorrhage and lower developmental scores at two years of age [32–34]. Also, the most recent study (SafeBoosC II) did not show an improvement in neurodevelopmental outcome at two years with reduction in cerebral hypoxia in preterm infants.
Two large, prospective, observational studies in resource-limited settings conducted by Ersdal et al. have investigated the relationship between DCC and death. In a cohort of over 12,000 spontaneously breathing term and late preterm infants, delaying UCC until after the initiation of spontaneous respirations reduced the risk of death and the combined risk of death and hospital admission at 24 hours after birth [35] (level 3b). This happened despite the fact that the number of infants who died in this cohort was small (0.2%of the infants enrolled). A second observational study described the timing of UCC in over 1200 infants who received PPV for apnea after birth [36] (level 3b). Initiating PPV prior to UCC did not significantly reduce the combined risk of death and admission at 24 hours after birth (18%if cord clamping occurred before initiating PPV vs. 14%if cord clamping occurred after initiating PPV, P = 0.328). The delay in the onset of PPV was significantly associated with the combined risk of death and admission at 24 hours. Of note, the timing of cord clamping was 39±35 seconds in infants who received PPV. Other trials reported some evidence of decreased neonatal mortality overall [26, 27] (level 1a) (30) (level 1b). A meta-analysis by Ghavam et al. found the same benefits specifically for extremely low birthweight (ELBW) [37] (level 1a). In term and near-term babies, there are hematological effects of the placental transfusion in terms of hemoglobin and ferritin values and at 6 weeks of age [38]. Specifically, for UCM, the milked blood contains mesenchymal stromal cells in addition to solely hematopoietic stem cells, a composition more favorable for hematopoiesis [39].
Safety of delayed cord clamping
Cochrane meta-analysis by McDonald et al. revealed that DCC was not associated with increase maternal complications including postpartum haemorrhage (PPH) (RR 1.04, 95%CI 0.65–1.65), maternal hemoglobin values, need for uterotonics, or duration of the third stage of labour regardless of mode of delivery (vaginal versus C-section) [26] (level 1a). Peak bilirubin serum levels were higher in infants in the DCC clamping group, but there was no statistically significant difference in the need for phototherapy between the groups [40] (level 1a).
Hemodynamically, in preterm neonates, DCC does not seem to be associated with any change in the incidence of patent ductus arteriosus (PDA) [20] (level 1b).
DCC after birth was found to be a safe procedure, particularly beneficial in newborns from HIV mothers. The risk of anemia is significantly decreased at 24 hours after birth and persists at age of 1 month without any increased risk of neonatal jaundice or polycythemia [41].
Contraindication to DCC
There are some clinical situations in which the immediate cord clamping should be considered. This may include maternal indications including hemorrhage, haemodynamic instability or both as well as abnormal placentation (previa, abruption). Fetal/neonatal considerations include the need for immediate resuscitation, placental circulation that is not intact (abruption, previa, cord avulsion, IUGR with abnormal cord Doppler evaluation.
Umbilical cord milking
There are at least two methods of UCM described in literature. First, leaving the cord intact and gradually “milking” 20 cm of the umbilical cord over 1 to 2 seconds, and releases the umbilical cord after each milk to allow the cord to refill with blood. This process is repeated 2 to 4 times prior to UCC [34, 45]. The second method is called the “cut-umbilical cord milking” when the cord is clamped close to the placenta the residual volume of blood is milked towards the infant [46–50].
It is assumed that the main benefit of DCC is placental-to-infant transfusion, which has led to the suggestion that umbilical cord milking (UCM) may be an alternative to DCC.
When compared to DCC, UCM improved the transition in preterm infants at birth(43)(22) (level 1b) and is associated with better SVC [51] (level 2b) flow and higher right and left ventricular outputs [44] (level 1b). In addition, UCM improves some of the neonatal outcomes including blood transfusion, hemoglobin at 12 and 24 hours after birth, hemoglobin and serum ferritin levels at 6 weeks of life and oxygen requirements at 36 weeks corrected gestation [44, 52] (level 1b).
A small prospective cohort study of neurodevelopmental assessment by the Bayley III method of very preterm infants, milking of the cord 4 times did not have any long-term adverse effect on neurodevelopmental outcome [38] (level 2b). The long term benefits could be related to the composition of the milked blood as it contains mesenchymal stromal cells in addition to solely hematopoietic stem cells, a composition more favorable for hematopoiesis, as suggested by its superior rescue of lethally irradiated bone marrow–depleted mice [39] (level 2b).
The primary advantage of UCM over DCC is the rapid blood transfer from the placenta to the infant immediately after birth without interfering with the evaluation and the resuscitation of the newborn and it is not dependent on uterine tone. The placental blood flow at 24 to 29 weeks’ gestation is about 8 mL/s in the umbilical vein which increases to 10 mL/s at term. Thus UCM may be a more effective technique to transfer blood during cesarean deliveries because the uterus is not vigorously contracting [22].
Despite some of the above-mentioned benefits for UCM, concerns had arisen. In a PREMOD trial, a multi-national trial of UCM in premature infants stratified by gestational age (low strata 23–27 weeks, high strata 28–31 weeks) and mode of delivery was stopped as recommended by the Data and Safety Monitoring Board (DSMB) based on the safety outcome of increased severe IVH in infants randomized to UCM in the lower gestational age strata. The probability of severe IVH in this strata was also significantly increased in the presence of chorioamnionitis [53] (level 1b).
The issue with cord milking is that it is associated with “see-saw” pattern of blood pressure changes in the carotid arteries which exposes the fragile cerebral vasculatures to potential injury [54] (level 2b). This could be a potential reason for the sever IVH findings found previously [48].
A retrospective cohort showed that even one-time milking after cord cutting had similar effects to multiple-time milking before cord cutting in very premature infants [48].
Cord milking was suggested by researchers as an alternative to immediate cord clamping in non-vigorous term/near term infants (MINVI trial: ClinicalTrials.gov Identifier: NCT03631940).
Meanwhile, and due to insufficient evidence, international recommendations currently discourage the use of UCM outside of clinical studies [55–59].
Physiology-based cord clamping (PBCC)
Animal models have shown benefits of initiating ventilation to increase pulmonary blood flow prior to UCC in preterm, anesthetized newborn lambs; newborn lambs at 126 days’ gestational age (equivalent to ∼26 weeks in humans) with UCC prior to ventilation had dangerous swings in cerebral blood flow, arterial blood pressure, heart rate, and cerebral oxygenation. Lambs that received ventilation prior to UCC had a much smoother transition to ex utero life, including attenuated changes in cerebral perfusion and blood pressure and increased levels of oxygenation [9, 60].
There are many factors to consider including: Immaturity, degree of prenatal asphyxia, distribution of the fetal-placental blood, position, uterine contractions, mode of delivery, facilitating the transition (breathing first, clamp later) or inhibiting the transition by intervention.
There is significant difference in the volume of placental transfusion towards the infant when the ventilation occurs before or after the cord clamping as the amount of blood retained in the placenta is significantly higher in the latter [61]. The intrathoracic pressure changes influence the venous return. Negative intrathoracic pressure increases venous return to the heart. However, during ventilating and recruiting the lungs, this actually create a reservoir to restore blood increasing the right ventricular output and it is clear that the pulmonary blood flow increases dramatically when ventilation starts even if cord clamp was placed prior [62]; subsequently, pulmonary venous return supplements left ventricular preload. In addition, the dramatic changes in the arterial blood pressure and the carotid arteries blood flow are ameliorated if the cord is clamped after the ventilation is established [62]. All of these factors facilitate a stable postnatal transition which is the fundamental concept of PBCC.
Levels of evidence used in this statement
Levels of evidence used in this statement
Data from reference [8]. RCT Randomized control trial; SR Systematic review.
The concern that extremely very low birth babies may not cry or breathe spontaneously following birth is valid, however, a significant number of these babies would do so. A study by O’Donnell et al. revealed that even babies born less than 26 weeks of gestation either cry (56%) or breathe (67%) on their own [63]. The rest of the babies will quickly get either sustained inflation or invasive ventilation.
In a recent trial of premature infants randomized to DCC along with assisted ventilation or tactile stimulation with DCC, there was no difference in resuscitation interventions, transitional hemodynamics, or neonatal outcomes [64]. A feasibility cohort by Blank et al. also confirms the same regardless of mode of delivery [65]. It may be that a mechanism of benefit of DCC is allowing time for spontaneous breathing prior to the clamping of the cord and thus, by maintaining left ventricular preload, ensuring an unperturbed hemodynamic transition.
Few centres around the world started developing a purpose-built resuscitation tables to make it possible to keep the cord intact after birth until the lungs get aerated and the infant is breathing [66].
The mounting evidence for deferring cord clamping prompted changes to recent guidelines. The World health organization officially endorsed the practice of DCC in 1996; cord clamping should be delayed for at least one minute after birth in both term and preterm infants [58].
During the 2010 International consensus on cardiopulmonary resuscitation and emergency cardiovascular care science with treatment recommendations (2010 CoSTR) review, evidence began to emerge suggesting that DCC might be beneficial for infants who did not need immediate resuscitation at birth [67]. The neonatal resuscitation program (NRP) now recommends delaying the cord clamping for longer than 60 seconds in term and preterm infants not requiring immediate resuscitation at birth [55].
Also, the American college of obstetricians and gynecologists (ACOG) withdrew its directive for immediate cord clamping in 2002. ACOG is now recommending a delay in cord clamping in vigorous term and preterm infants for at least 30–60 seconds after birth [68]. The contraindications include maternal hemorrhage, maternal hemodynamic instability, abnormal placentation (previa or abruption). The fetal and neonatal contraindications include the immediate need for resuscitation, placental circulation not intact (abruption, previa, cord avulsion, IUGR with abnormal cord Doppler evaluation) [68].
Delayed cord clamping is not recommended in monochorionic twins because the risk of acute intertwin transfusion at birth outweighs the undetermined benefit of delayed cord clamping in this population (strong recommendation) (1B) [69].
The American heart association (posted: November 3, 2015) states that DCC for longer than 30 seconds is reasonable for both term and preterm infants who do not require resuscitation at birth(59).
A recent statement from the Canadian paediatric society (posted: Jun 21, 2019) recommended that DCC should be offered for all preterm infants not in need of immediate resuscitation (Grade A recommendation) and that cord milking should be offered for all preterm infants not in need of immediate resuscitation (Grade A recommendation), while cord milking can be considered when delayed cord clamping is not feasible (Grade B recommendation) [70].
Recommendations
Based on summaries of best evidence, the following recommendations for practice are offered to guide clinical care in term and preterm infants: Delayed cord clamping should be offered for all preterm infants not in need of immediate resuscitation (grade A recommendation) (Table 2); it is reasonable to practice delayed cord clamping for at least 30–60 seconds in both term and preterm infants who are not in immediate need for resuscitation at birth (grade A recommendation); Umbilical cord milking is not recommended at this point in term and preterm infants. Further research is required to elaborate whether it could be an alternative in non-vigorous infants (grade A recommendation).
Grades of recommendation
Grades of recommendation
Data from reference [8].
More studies are needed to delineate the responses of non-vigorous infants who receive aggressive resuscitation and UCM, since cord milking does not delay resuscitation and can be started simultaneously.
Disclosure statements
No disclosure to state.