
Abstract
Given the potential of enteral zinc to reduce enterohepatic circulation of unconjugated bilirubin, we aimed to synthesize evidence from randomized controlled trials (RCTs) on zinc supplementation for prevention of neonatal hyperbilirubinemia (NNH). We searched PubMed, Embase, Scopus, and CENTRAL for RCTs evaluating zinc supplementation in healthy or at-risk neonates for prevention of NNH. Primary outcomes were incidence of significant NNH and requirement for phototherapy. Secondary outcomes included duration of phototherapy, bilirubin levels, and adverse effects. Two reviewers independently screened, extracted data and assessed risk of bias. Random-effects meta-analysis was performed with RevMan 5.4. The certainty of evidence was assessed using the GRADE approach. We included six RCTs, enrolling 725 neonates, in this review. Four trials were judged to have high risk, while two had some concerns of bias. Low certainty evidence suggested no significant effect of zinc on the incidence of significant NNH (RR 0.91, 95% CI 0.58 to 1.44; five trials, 657 participants) or need for phototherapy (RR 0.73, 95% CI 0.42 to 1.28; five trials, 618 participants). Zinc supplementation was associated with a shorter duration of phototherapy (MD -14.79, 95% CI -21.27 to −8.30; four trials, 108 participants). No significant differences were observed in bilirubin levels on day 3 or 7. Adverse events were rare and comparable between groups. In conclusion, there is limited evidence to support or refute the role of zinc supplementation in the prevention of NNH. Rigorous multicenter RCTs with standardized dosing and outcome definitions are needed to further explore its utility.
Introduction
Neonatal hyperbilirubinemia (NNH) refers to the clinically observable signs of elevated total serum bilirubin (TSB). The clinical manifestations vary depending on the underlying cause but primarily include yellow discoloration of the skin, sclera, and mucous membranes. Approximately 60% of term and 80% of preterm neonates develop visible jaundice within the first week of life. 1 Most often, this condition is mild, transient, and self-resolving, referred to as physiological jaundice. However, it is critical to differentiate this entity from pathological jaundice, which may indicate a more serious underlying condition.
The real concern arises from the failure to timely recognize and manage pathological jaundice, particularly in low- and middle-income countries (LMICs) where advanced diagnostic tools are scarce. 2 Such delays can lead to bilirubin-induced neurological dysfunction (BIND), which, if inadequately managed, may progress to acute or chronic bilirubin encephalopathy, also known as kernicterus. Kernicterus is a severe and feared complication, causing irreversible brain damage and profound long-term disabilities in survivors such as cerebral palsy, non-syndromic auditory neuropathy, hearing loss, and learning disabilities. 3 Severe NNH continues to be a long-standing contributor to neonatal mortality in LMICs, particularly in India, where between 1990 and 2019, a total of 1,189,856 infant deaths and an estimated economic burden from US$7.2 to 11.7 billion were linked to severe NNH. 4
The cornerstone of treatment for severe NNH includes phototherapy and exchange transfusion. 5 Despite being effective, phototherapy and exchange transfusion are not without risks. Phototherapy can disrupt maternal-infant bonding, cause insensible water loss, electrolyte imbalance, and lead to bronze baby syndrome, along with psychological and financial stress of hospitalization. 6 Exchange transfusion, on the other hand, may result in complications such as graft-versus-host disease, infections, thrombocytopenia, hypocalcemia, and hyperkalemia. 7 Hence, a need arises to shift focus towards prevention alongside enhancing treatment strategies to reduce the incidence and severity of NNH and minimize the need for prolonged phototherapy and invasive interventions.
Emerging therapies for NNH include Sn-protoporphyrin, a heme oxygenase inhibitor that lowers bilirubin level, and ursodeoxycholic acid, which improves bile flow and decreases enterohepatic circulation, which have shown promise as adjuncts in managing NNH.8–10 Another area of active investigation is the role of oral zinc in the reduction of NNH. In experimental studies, Sánchez et al. demonstrated that zinc salts, especially those flocculating at physiological pH, can effectively adsorb unconjugated bilirubin from micellar bile salt solutions. 11 Additionally, oral zinc administration was shown to reduce biliary bilirubin secretion in animal models. 12 In humans, short- and long-term administration of zinc sulfate in Gilbert’s syndrome resulted in a significant reduction in unconjugated bilirubin level. 13
Subsequently zinc supplementation has been evaluated in neonates undergoing phototherapy, and found to lower bilirubin levels and reduce the duration of phototherapy.14–16 Although zinc supplementation has been studied as an adjunct to phototherapy, its role in the prevention of NNH in healthy neonates remains underexplored. The only review on prophylactic use of zinc in neonates was published a decade back and included only one trial enrolling 286 neonates. 17 Based on limited evidence, the authors concluded that zinc supplementation was not effective in reduction of significant NNH or need for phototherapy. However, subsequent studies have shown promising results with zinc supplementation in preventing NNH.18,19 Therefore, we planned this systematic review to update the evidence on the efficacy of zinc supplementation in preventing NNH.
Methods
We conducted this review in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. 20 The review protocol was prospectively registered with PROSPERO (registration number CRD42024612253).
Inclusion and exclusion criteria
We included all randomized controlled trials (RCTs) that compared prophylactic zinc supplementation with or without a placebo, for preventing NNH in healthy or at-risk neonates, irrespective of gestation age (GA). The trials which enrolled neonates receiving oral zinc along with phototherapy were excluded from the review. Unpublished studies, non-RCT designs, conference abstracts and studies published in language other than English were not included in the review and were eliminated during the search.
Search strategy
A comprehensive electronic database search was conducted in PubMed, Embase, Scopus, and Cochrane Central Register of Controlled Trials in January 2026 using the following string of terms with Boolean operators: “(infant OR newborn OR neonate) AND (zinc) AND (hyperbilirubinemia OR hyperbilirubinaemia OR jaundice).” The U.S. National Library of Medicine’s ClinicalTrials.gov was searched for registered ongoing and completed trials. Additionally, reference lists of the retrieved articles and any previous systematic reviews and meta-analyses relevant to our systematic review were hand-searched to identify eligible studies. Follow-up reports of included studies were sought by searching for their trial registration numbers in MEDLINE.
Outcome measures
The primary outcomes of interest were the incidences of NNH requiring phototherapy and significant NNH, defined as TSB levels exceeding 15 mg/dL or as defined by the individual studies. The secondary outcomes included duration of phototherapy, TSB or transcutaneous bilirubin (TcB) levels measured at specific time points through the trial period (such as day 2, 3, 7 etc. of the respective trial), frequency of stools (reflects the effect on bilirubin excretion), and any adverse effects reported in association with the intervention. These outcomes were systematically extracted from each included study using excel sheets.
Study selection and data extraction
Two investigators independently conducted the study selection, screened titles and abstracts, reviewed full texts, and extracted relevant data from the included studies. Discrepancies were resolved by discussing with a third reviewer to reach a final decision. In cases of incomplete data or unavailability of full-text articles, attempts were made to contact the study authors via email. The extracted data included publication year, design, population characteristics (gestational age, ethnicity, setting, sample size, country), details of the intervention (zinc), comparators used, and other reported outcomes. For binary outcomes, the number of participants and events in each group was collected, while for continuous outcomes, number of participants, means and standard deviations were extracted. A web-based tool (PlotDigitizer, https://plotdigitizer.com/) was used to extract relevant data from graphs for meta-analysis, if not provided in the full-text of the study.
Risk of bias assessment
Two review authors independently assessed the risk of bias in the included trials using the Cochrane “Risk of bias” (RoB 2.0) tool for the following domains: bias arising from the randomization process; bias due to deviations from intended interventions; bias due to missing outcome data; bias in the measurement of the outcome; and bias in the selection of the reported result. 21 In case of any discrepancy, a third reviewer resolved any disagreement.
Data synthesis and statistical analysis
Two investigators extracted data from the study, and if two or more studies exhibited similar and sufficient outcomes and had acceptable homogeneity, a meta-analysis was performed using Review Manager 5.4. The treatment effects of zinc were quantified as risk ratios (RR) and 95% confidence intervals (CI) for binary outcomes, and as mean differences (MD) and 95% CI for continuous outcomes. Given the clinical and methodological heterogeneity among the included trials, we used a random-effects model to pool individual study results. Statistical heterogeneity of the trials was assessed by inspecting the forest plots and quantifying the impact of heterogeneity using I2 statistic. If we detected significant heterogeneity (I2 >60%), we planned to explore the possible causes of heterogeneity. If there were more than 10 included studies, we planned to assess publication bias using funnel plot. We used GRADEpro software to assess the certainty of evidence for all relevant outcomes. 22
Results
The initial search yielded 485 references from electronic databases and trial registers (Figure 1). We additionally identified seven references from citation searching. Of these, six RCTs, involving 725 newborns, met the inclusion criteria and were included in the review.18,23–27 A list of excluded studies has been provided in the supplemental material (Table S1, Supplemental material). PRISMA flow chart.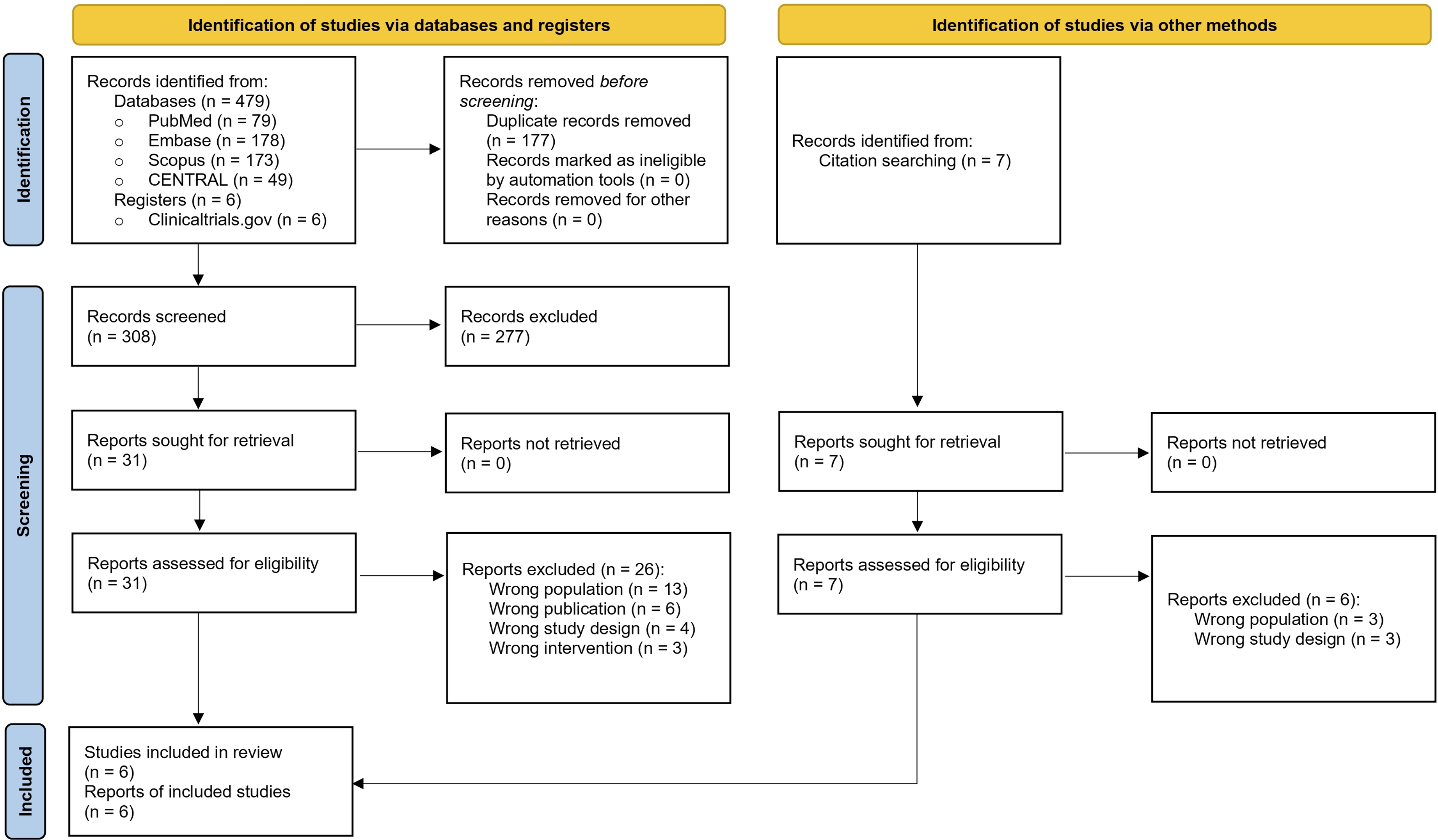
Characteristics of included studies
Characteristics of included studies.
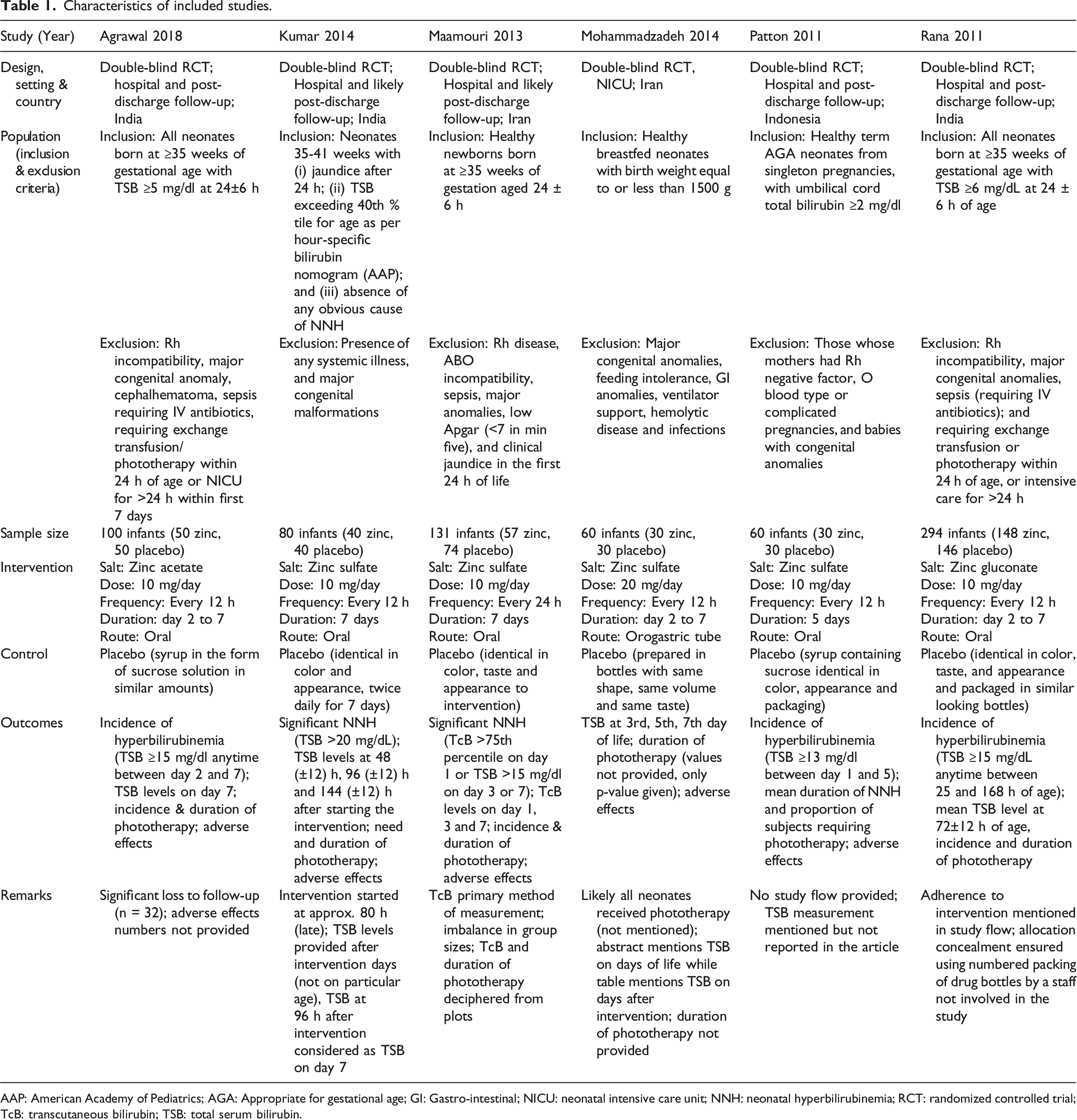
AAP: American Academy of Pediatrics; AGA: Appropriate for gestational age; GI: Gastro-intestinal; NICU: neonatal intensive care unit; NNH: neonatal hyperbilirubinemia; RCT: randomized controlled trial; TcB: transcutaneous bilirubin; TSB: total serum bilirubin.
The intervention included oral zinc prophylaxis across the included studies, with minor differences in protocol. Four studies used zinc sulfate,23–26 one zinc acetate, 18 and one zinc gluconate. 27 All studies, except Mohammadzadeh 2014, 25 evaluated an elemental dose of 10 mg per day for a duration of 5 to 7 days. All trials used a placebo, similar in color, appearance and taste, at similar doses, frequency and duration, ensuring a double-blind design.
The primary outcomes of interest, that is, significant NNH and NNH requiring phototherapy, were reported by all trials, except Mohammadzadeh 2014. 25 However, significant NNH definition varied across trials; one trial as TSB ≥13 mg/dL 26 and three as TSB ≥15 mg/dL.18,24,27 Although Kumar 2014 did not define significant NNH, the authors reported incidences of TSB >20 mg/dL, which we considered as significant NNH. 23 While Kumar 2014 and Rana 2011 mentioned using guidelines recommended by American Academy of Pediatrics (AAP), 2004 29 to decide phototherapy,23,27 other trials did not specify the criteria for starting phototherapy. All trials used TSB to measure bilirubin levels, except Maamouri 2013 which used TcB. 24 None of the included trials reported the outcome of stool frequency. All trials reported adverse effects to the intervention, but only Kumar 2014 and Rana 2011 mentioned the numbers of affected neonates.
Risk of bias
Of the included trials, four were judged to have high risk,18,24–26 while two to have some concerns of bias (Figure S1, Supplemental material).23,27 The trial protocol was not registered for Kumar 2014, 23 while Rana 2011 registered it retrospectively, 27 leading to a judgment of some concerns of bias. For other trials, the common reasons of bias included inadequate information on allocation concealment, deviations from intended interventions and possibility of selective reporting.
Primary outcomes
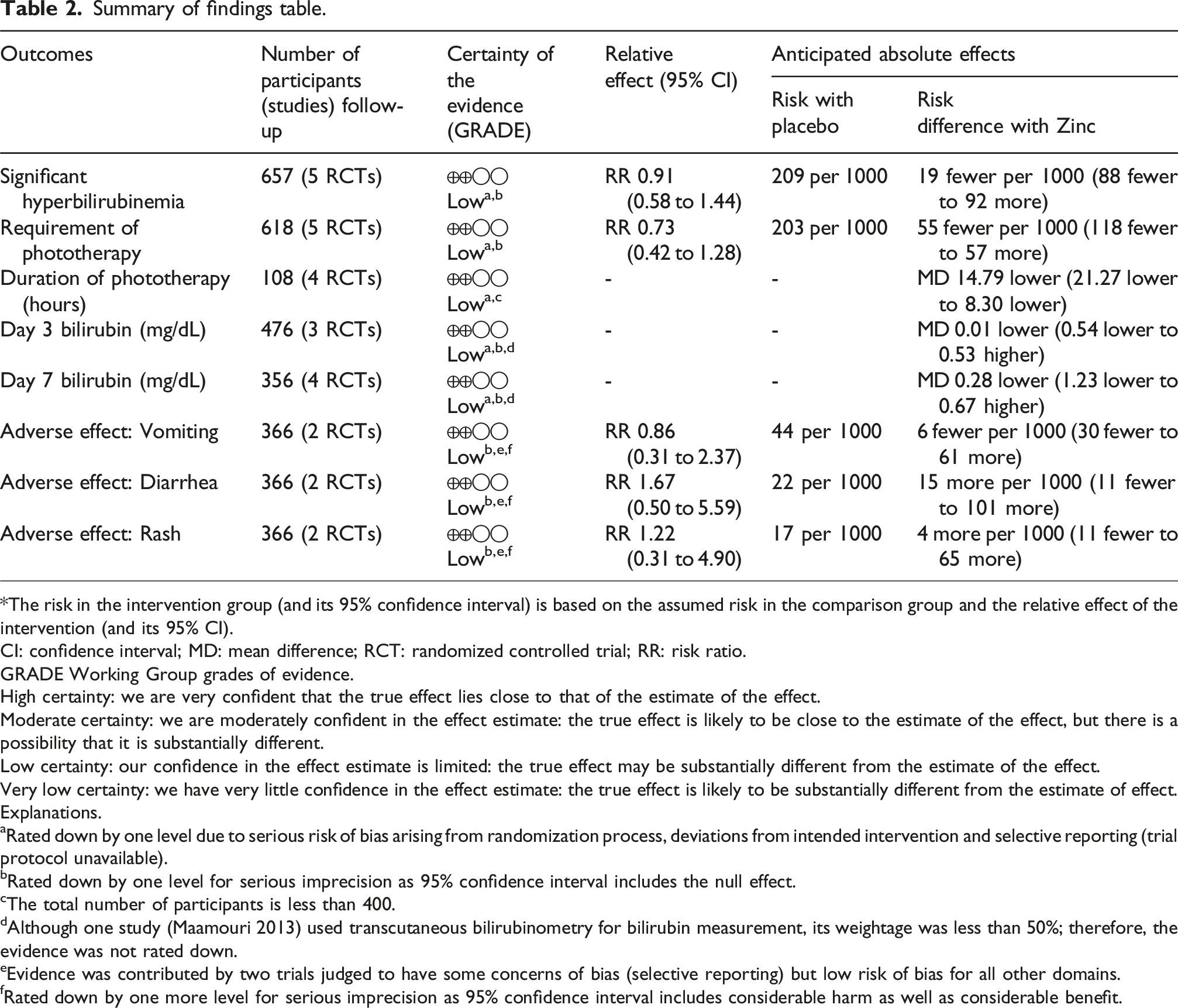
The pooled analysis did not demonstrate a statistically significant difference in the incidence of significant NNH (RR 0.91, 95% CI 0.58 to 1.44; I2 = 51%; five trials, 657 participants; low certainty evidence; Figure 2(a); Table 2), and in the need of phototherapy (RR 0.73, 95% CI 0.42 to 1.28; I2 = 57%; five trials, 618 participants; low certainty evidence; Figure 2(b)). Forest plot (random-effects model) for primary outcomes: (a) Significant hyperbilirubinemia and (b) Requirement of phototherapy. Summary of findings table. *The risk in the intervention group (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). CI: confidence interval; MD: mean difference; RCT: randomized controlled trial; RR: risk ratio. GRADE Working Group grades of evidence. High certainty: we are very confident that the true effect lies close to that of the estimate of the effect. Moderate certainty: we are moderately confident in the effect estimate: the true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different. Low certainty: our confidence in the effect estimate is limited: the true effect may be substantially different from the estimate of the effect. Very low certainty: we have very little confidence in the effect estimate: the true effect is likely to be substantially different from the estimate of effect. Explanations. aRated down by one level due to serious risk of bias arising from randomization process, deviations from intended intervention and selective reporting (trial protocol unavailable). bRated down by one level for serious imprecision as 95% confidence interval includes the null effect. cThe total number of participants is less than 400. dAlthough one study (Maamouri 2013) used transcutaneous bilirubinometry for bilirubin measurement, its weightage was less than 50%; therefore, the evidence was not rated down. eEvidence was contributed by two trials judged to have some concerns of bias (selective reporting) but low risk of bias for all other domains. fRated down by one more level for serious imprecision as 95% confidence interval includes considerable harm as well as considerable benefit.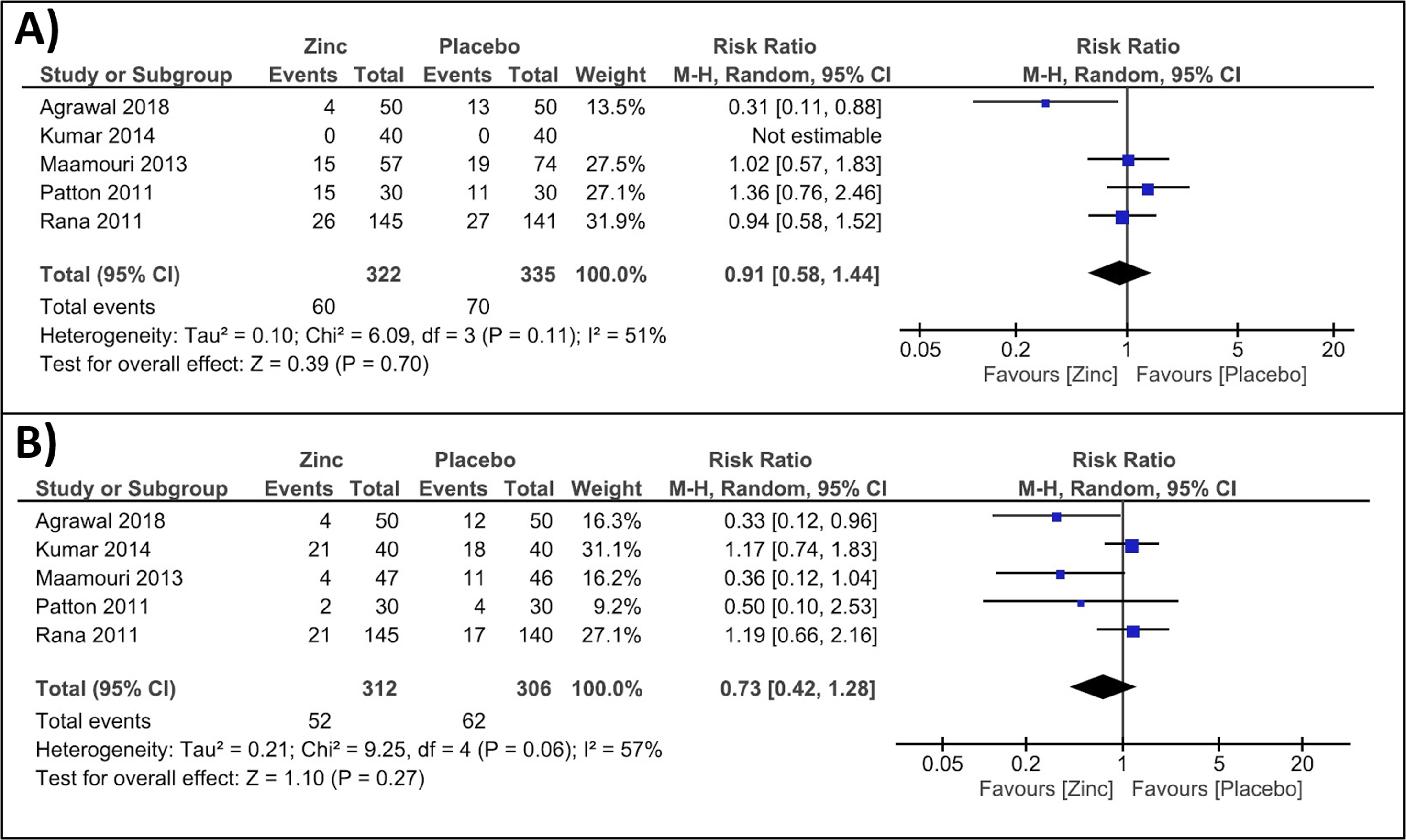
Secondary outcomes
The duration of phototherapy was significantly lower in the zinc group, compared to the control (MD -14.79, 95% CI -21.27 to −8.30; I2 = 48%; four trials, 108 participants; low certainty evidence; Figure 3(a)). Total bilirubin levels on day 3 (MD -0.01 mg/dL, 95% CI -0.54 to 0.53; I2 = 0%; three trials, 476 participants; low certainty evidence; Figure 3(b)) and on day 7 of life (MD -0.28 mg/dL, 95% CI -1.23 to 0.67; I2 = 52%; four trials, 356 participants; low certainty evidence; Figure 3(c)) showed no significant differences between the groups. Forest plot (random-effects model) for secondary outcomes: (a) Duration of phototherapy, (b) Bilirubin levels on day 3, and (c) Bilirubin levels on day 7.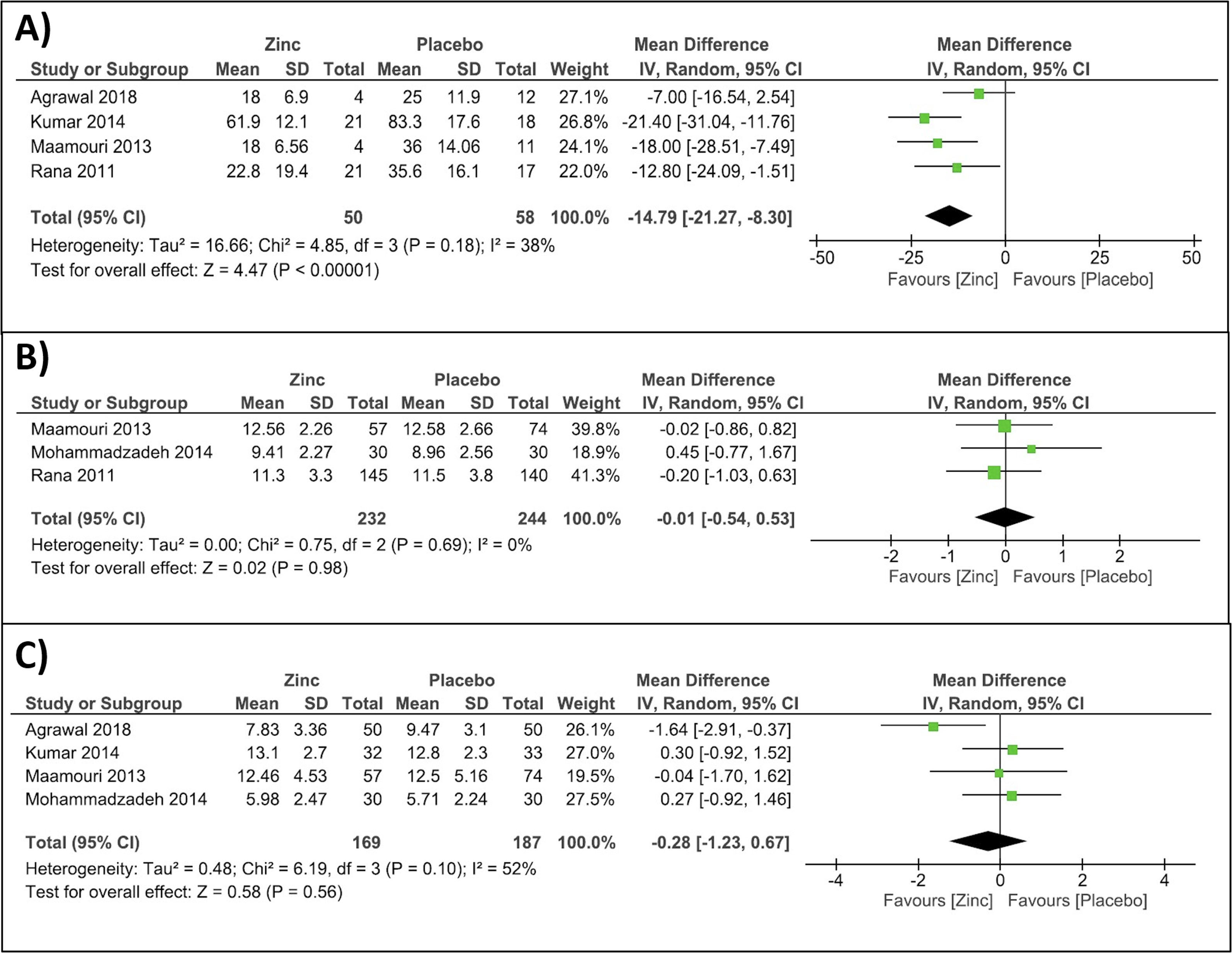
Overall, the reported adverse effects were infrequent and showed no difference between the two groups in the included studies. Based on pooled data from two trials (366 neonates), low certainty evidence suggested no difference in the incidences of vomiting (RR 0.86, 95% CI 0.31 to 2.37; I2 = 0; Figure 4(a)), diarrhea (RR 1.67, 95% CI 0.50 to 5.59; I2 = 0%; Figure 4(b)) or rash (RR 1.22, 95% CI 0.31 to 4.90; I2 = 0%; Figure 4(c)). Forest plot (random-effects model) for adverse effects: (a) Vomiting, (b) Diarrhea, and (c) Rash.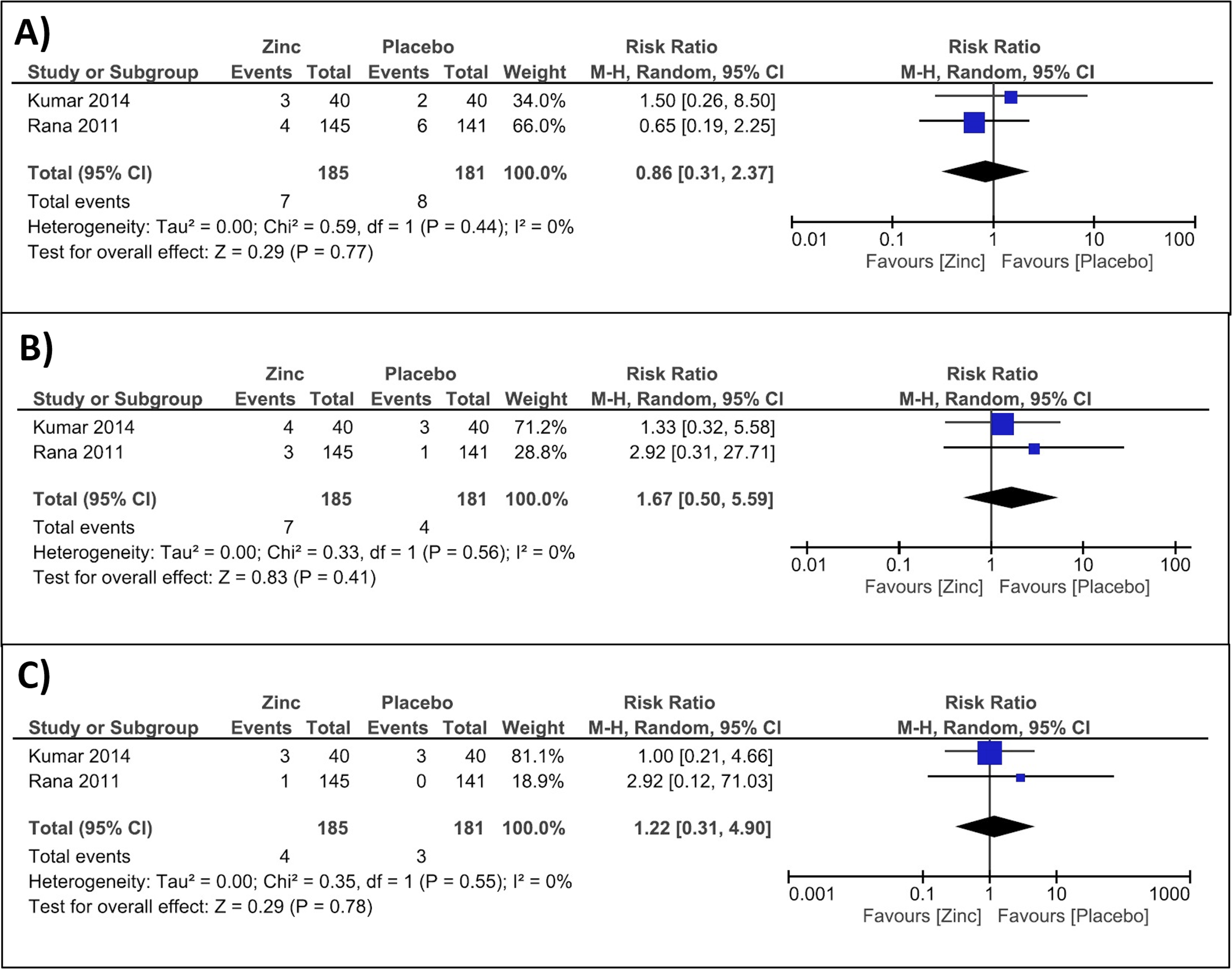
Discussion
This systematic review evaluated the role of prophylactic zinc supplementation in healthy and at-risk neonates for the prevention of NNH. We included six RCTs enrolling 725 neonates, which evaluated the effect of zinc supplementation at doses of 10–20 mg/day for 5-7 days. The trials were judged to have some concerns or high risk of bias related to randomization process, deviations from intended intervention and selective reporting. Low certainty evidence suggested that zinc supplementation did not result in a reduction in the incidence of significant NNH or need for phototherapy. Low certainty evidence indicated a significant reduction in the duration of phototherapy duration, without any differences in bilirubin levels measured at specific timepoints through the intervention period. The adverse effects were rare and showed no difference between the two groups in the included trials.
NNH remains one of the most common morbidities in the early neonatal period, with significant implications for neurodevelopmental outcomes, particularly in LMICs. This meta-analysis provides a systematic understanding of the available evidence on zinc supplementation as a preventive strategy for NNH. Previous published reviews have primarily focused on zinc supplementation used as an adjunct to phototherapy in the treatment of NNH.14–16 The latest reviews by de Oliveira et al. and Ghadirzadeh et al. included 11 and 20 studies, enrolling 1349 and 2127 neonates, respectively.14,15 While the first review concluded that zinc supplementation was effective in reducing TSB levels when used with phototherapy in NNH, 14 the second review found a significant heterogeneity in the results and could not draw conclusions on the efficacy of zinc supplementation as an adjunctive treatment. 15 While there is a substantial body of evidence for zinc as an adjunctive therapy, there is a paucity of research in its prophylactic role in NNH. The only review on prophylactic effect of zinc in NNH was published 10 years back, included single study, and concluded that there was limited evidence. 17 A more recent review included 17 studies, which evaluated zinc supplementation in 1565 neonates with or at risk of NNH. 16 Therefore, the review assessed both, prophylactic as well as adjunctive therapeutic effect of zinc in neonates. The authors concluded that zinc supplementation led to a reduction in phototherapy duration, but did not affect other outcomes. While the conclusion is similar to our review, there are several important differences. First, our review included six trials on prophylactic zinc supplementation, whereas the other review included five trials, owing to misclassification of one study. 25 Second, the authors pooled data from both prophylactic and therapeutic studies together for certain outcomes, such as duration of phototherapy and bilirubin levels. This may not be desirable given the differences in intervention among these studies in terms of timing, dosing, duration of therapy and potential modification of zinc effect by concurrent phototherapy. Third, the results and conclusions were presented without clearly distinguishing between prophylactic and therapeutic effects, leading to ambiguity regarding the specific role of zinc prophylaxis in the prevention of NNH.
Although prophylactic zinc did not affect the incidence of significant NNH or the bilirubin levels on day 3 or day 7, the reduction in phototherapy duration observed in our review may be clinically relevant. This finding has been consistent and observed in multiple reviews previously.14–16 This effect may be explained by the potential synergistic effect of phototherapy and zinc on enterohepatic circulation of bilirubin. Phototherapy is well known to increase stool frequency by stimulating intestinal water and electrolyte secretion. 30 This may provide zinc with greater opportunity to precipitate unconjugated bilirubin in the intestine and thereby enhance its fecal excretion. 11 Therefore, zinc supplementation is more likely to be effective in shortening the phototherapy duration, rather than in preventing NNH, as has been observed in existing literature.
We acknowledge certain limitations in the review. Although our review included six trials, the included number of participants was small, with only 725 neonates. Methodological quality was variable, with most of the trials at high risk related to randomization process and deviations from interventions. There was substantial clinical and methodological heterogeneity among the trials in terms of gestational age, risk stratification criteria, zinc formulation, dose, and duration, which restricts the generalizability of findings to the neonatal population. Furthermore, the primary outcomes, that is, significant NNH and need for phototherapy, were affected by variability in definitions and phototherapy criteria, respectively. The reliance on TcB measurements in one trial introduced additional concerns. 24 We pooled bilirubin levels on day 3 and 7 using two distinct methods of measurement (TcB and TSB) together, which may not be desirable. However, previous studies have reported an excellent correlation and agreement between TSB and TcB. 31 We could not extract accurate bilirubin levels from Maamouri 2013, 24 and therefore, had to use an online tool to extract data from graphs. This may have introduced possible small errors in the reported TcB values from the study. Although this review contributes to clarifying the role of zinc supplementation in preventing NNH, the available evidence was of low quality to draw any conclusive interpretation. These findings highlight the need for larger, well-designed, multicenter RCTs with standardized dosing regimens and outcome measurements to further evaluate the preventive potential of zinc in neonatal jaundice.
Conclusion
While biologically plausible and well tolerated, there is currently insufficient evidence to support or refute the role of zinc supplementation as a prophylactic intervention against NNH. There remains a need for large multicenter RCTs with standardized protocols, stratification by risk profile, and long-term follow up to determine whether zinc has a role in targeted prophylaxis or in health systems with limited access to phototherapy.
Supplemental material
Supplemental Material - Zinc supplementation for prevention of neonatal hyperbilirubinemia: A systematic review and meta-analysis
Supplemental Material for Zinc supplementation for prevention of neonatal hyperbilirubinemia: A systematic review and meta-analysis by Gagan Deep Reddy Chitiki, Hemant Pandita, Pramod Kumar Mehta, Akanksha Deshwali, Arnav Ranjan, Harshul Sood, Sumit Garg, Mayank Priyadarshi in Journal of Neonatal-Perinatal Medicine
Footnotes
ORCID iDs
Authors contributions
Drs Chitiki, Pandita, and Kumar conducted literature search and extracted data. Drs Chitiki, Pandita, Kumar, Deshwali, Ranjan, Sood, Garg, and Priyadarshi analyzed and interpreted data. Drs Chitiki, Pandita, Kumar and Deshwali prepared the first draft of the manuscript. Drs Ranjan, Sood, Garg, and Priyadarshi reviewed and modified the final draft.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
All data analyzed in this study are derived from published articles and their supplementary materials. No new datasets were generated or analyzed.
PROSPERO registration number
CRD42024612253.
Supplemental material
Supplemental material for this article is available online.