
Abstract
BACKGROUND:
Jaundice is the quite common benign condition in neonates, but due to its potential toxicity, neonates must be monitored. This study was aimed to evaluate the effect of serum albumin level on the transcutaneous bilirubin (TcB) measurements in term neonates with unconjugated hyperbilirubinemia.
METHODS:
Serum albumin and total serum bilirubin (TSB) of 252 jaundiced term neonates were estimated and simultaneously TcB was measured over sternum and the effect of serum albumin on TcB measurements was evaluated.
RESULTS:
The correlation between TSB and TcB was linear and significant for the entire cohort. When this correlation was studied separately in the groups with different albumin levels, maximum correlation (r = 0.888, R2 linear = 0.789, p < 0.001) was observed in group 1 with hypo-albuminemia followed by in group 2 with normal albumin levels (r = 0.854, R2 linear = 0.729, p < 0.001) and group 3 with higher albumin levels (r = 0.809, R2 linear = 0.689, p < 0.001). Bland-Altman plot analysis of whole study population demonstrate good agreement between TSB and TcB [95% CI = –0.038 to 0.493 mg/dL, 17/252 = 6.75% outside the limits of agreement, Mean difference = 0.227]. This analysis in different groups also show good agreement between TSB and TcB.
CONCLUSIONS:
The correlation between the TSB and TcB may affected by serum albumin level. Therefore, transcutaneous bilirubinometry is not able to replace invasive TSB measurement. However, in the absence of TSB it could be an alternative to measure the level of bilirubin in term neonates.
Introduction
The unconjugated hyperbilirubinemia is one of the most common clinical condition encountered during the first few days following birth. The incidence estimated to be 60 percent in term neonates which may even higher in preterm neonates [1]. It may be safe for the most of the healthy neonates but high levels of unconjugated bilirubin can cause acute bilirubin encephalopathy in susceptible newborns. It is therefore necessary to measure the bilirubin levels of neonates to prevent hyperbilirubinemia and providing phototherapy if the levels exceed the cutoff limits. The total serum bilirubin (TSB) estimation from the blood serum is still the gold standard to measure bilirubin levels but it has its drawbacks. Invasive blood sampling is painful and stressful for the neonate as well as parents, resulting in blood loss and an increased risk for infections at the site of sampling [2]. In addition, the method is laborious and time consuming, lacking the possibility for immediate diagnosis. A possible alternative for invasive blood sampling is transcutaneous bilirubinometry, a noninvasive and painless method that provides an instantaneous read-out of the cutaneous bilirubin concentration (TcB) and reduces repeated sampling [3]. Transcutaneous bilirubinometry is based on optical spectroscopy, which relates the amount of light absorption by bilirubin to the concentration of bilirubin in the skin [4]. Transcutaneous bilirubinometer allows a quick non-invasive estimate of bilirubin concentration to be used as an aid for screening and management of jaundice in newborn infants [5].
However, since last thirty years of its invention, still no transcutaneous bilirubinometer could replace invasive blood sampling. Race, duration of phototherapy, gestational age, rate of bilirubin accumulation, bilirubin binding capacity including distribution of bilirubin between intravascular and extravascular spaces can influence the relationship between these two measurements [6]. One of the important plasma components influencing plasma free bilirubin concentration is albumin which is also an acute phase protein and frequently is very low in sick babies [7]. Bilirubin binds to albumin in an equimolar ratio. Low production of albumin will lower its transport and binding capacity.
Nevertheless most of the previous studies have tested the validity of transcutaneous bilirubinometry almost solely by comparing the degree of exact correlation with the serum value [8–13]. But no study has been demonstrated the effect of serum albumin level on correlation of TcB and TSB. Our objective was to assess whether the serum albumin levels have any effect on co-relation of transcutaneous bilirubin measurements and total serum bilirubin in North Indian neonates.
Methods
This cross-sectional study was carried out at neonatal intensive care unit of Uttar Pradesh University of Medical Sciences, Saifai, Etawah, India between July 2018 and June, 2021. All term neonates≤2 weeks of postnatal age, weighing≥1500 g and requiring phototherapy for treatment of unconjugated hyperbilirubinemia according to American Academy of Pediatrics (AAP) nomogram chart [14] were enrolled in the study. Newborns having high serum bilirubin level in the range of exchange transfusion as per AAP nomogram chart [14] or with the history of previous phototherapy, blood transfusion, exchange transfusion or having biliary tract obstruction, major congenital malformation, conjugated hyperbilirubinemia, impaired liver functions or critically ill neonates were excluded from the study.
Ethical approval was taken from the university ethical committee. The parents of the newborn eligible for the study as per inclusion and exclusion criteria were briefed regarding the procedure and purpose of the study and a written consent was obtained from the parent. After taking consent, history was taken from mothers of all neonates regarding presence of risk factors for sepsis, perinatal asphyxia and prematurity. Anthropometrical and clinical examination including neurological, respiratory and cardiovascular examination was done. Gestational age was assessed using new Ballard score.
When the newborns had clinically visible jaundice then their blood samples were withdrawn and sent for serum albumin and serum bilirubin (total and differential) measurement to the central clinical laboratory where sample were processed by Selectra Pro XL clinical chemistry system by ELITech Group. It is a fully integrated system which determines the bilirubin levels by the principal of Modified Malloy Evelyn method and albumin levels by Bromo-Cresol green dye binding technique. Only the neonates whose TSB was measured to be above phototherapy cut-off as per AAP nomogram chart [14] were included in the study. Within 5–10 minutes, transcutaneous bilirubin was measured over sternum with the help of transcutaneous bilirubinometer (Drager JM-105, manufactured by Draeger Medical Systems, Inc., Lubeck, Germany). This bilirubinometer uses pulse xenon arc lamp as light source and has silicon photodiodes as sensors. The measurement range of the equipment varies from 0.0 mg/dl to 20 mg/dl (0μmol/l to 340μmol/l). All the measurements were performed with a single bilirubinometer in accordance with the manufactures’ recommendations. The device has a fiber-optic probe that is placed strategically which allows for a convenient application to the sternum of the infant. Once the appropriate skin application is established, the light source is triggered and the measured values appear on display. The mean of three serial measurements were recorded in order to reduce the measurement errors.
All the enrolled patients were divided into three groups on the basis of their serum albumin level. Group 1 comprises 32 patients whose serum albumin level were≤2.8 gm/dL, while the Group 2 comprises 124 patients having normal albumin level (> 2.8–3.3 gm/dL) and 96 patients having albumin level > 3.3 gm/dL were kept in Group 3.
After obtaining TSB, all enrolled neonates recei-ved double surface phototherapy. Distance between baby and light was kept at 35 cm. Irradiance was periodically measured, a minimum level of 15 microW/cm2/nm in (the wavelength range 460 to 490 nm) was ensured. Neonate’s position was changed at hourly interval under phototherapy so that maximal area of skin was exposed to light. Eyes were shielded to prevent retinal damage. Diapers were kept on to cover the genitalia of male infants. TSB measurements were repeated at 12-hour intervals until the measured levels were be below the designated cutoffs for phototherapy as per AAP nomogram chart [14].
Statistical analysis
Demographic and clinical characteristics of enrolled neonates were recorded. All data were analyzed using SPSS software version 25. Comparison between groups was performed by using one-way ANOVA test. To determine the correlation between TSB and TcB-sternum, Pearson correlation coefficients (r) were calculated with the use of linear regression techniques and scatter plots were made. Bland-Altman method was applied using the average difference±2SD as the 95% range of compliance for individual measurements to determine the agreement between the two methods of measurement in all groups. The level of statistical significance was established as p < 0.05.
Results
A total of 252 jaundiced term neonates with unconjugated hyperbilirubinemia were evaluated. Table 1 demonstrates the demographics of the patients enrolled in the study. Gestational age ranged from 37 to 42 weeks (mean 38.51±1.23 weeks), birth weight ranged from 1510 grams to 3800 grams (mean 2631.51±403.75 grams). The average time at which the first transcutaneous bilirubin measurement was recorded for the neonates was 46.23±24.16 hours after birth, with the earliest measurement obtained at 2 hour.
Study population characteristics
Study population characteristics
N: Number; SD: Standard deviation; SGA: Small for gestational age; AGA Appropriate for gestational age; LGA: Large for gestational age.
Table 2 depicts the mean of albumin level, TcB and TSB in all three groups. A statistical significant relation was found between the mean albumin levels of all three groups. (p value < 0.001) The mean TcB values recorded were higher as compared to TSB in all three groups.
Mean albumin, total serum and transcutaneous bilirubin in different groups
N: Number; TSB: Total serum bilirubin; TCB: Transcutaneous bilirubin.
The correlation between TSB and TcB over sternum was linear and significant for the entire cohort (Pearson’s r = 0.830, R2 linear = 0.689, p < 0.001). When the correlation between TSB and TcB sternum was studied in all three groups, maximum correlation (Pearson’s r = 0.888, R2 linear = 0.789, p < 0.001) was observed in group 1 followed by in group 2 (Pearson’s r = 0.854, R2 linear = 0.729, p < 0.001) and group 3 (Pearson’s r = 0.809, R2 linear = 0.689, p < 0.001) (Fig. 1).
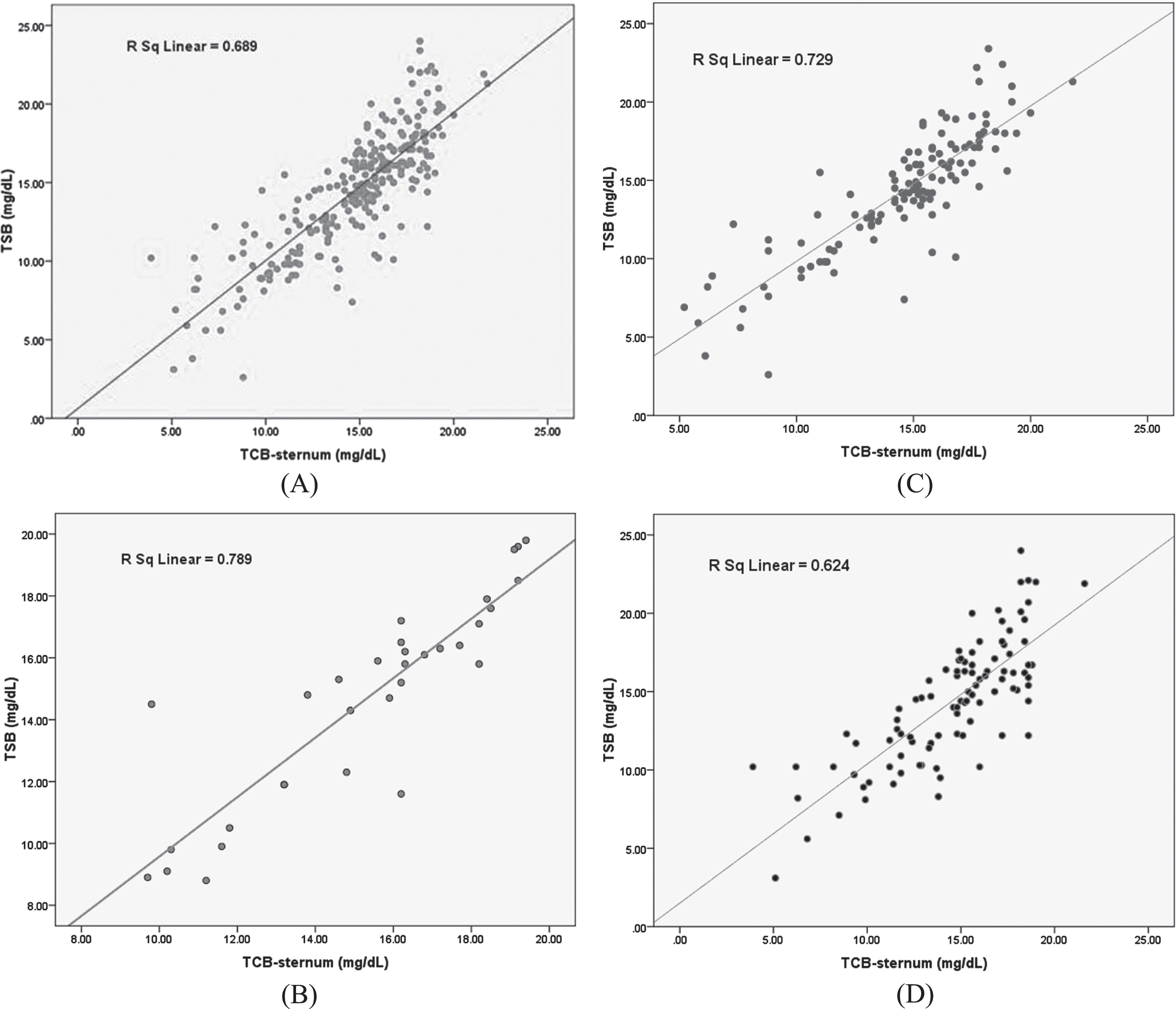
Linear regression plots showing the relationship between transcutaneous bilirubin and total serum bilirubin values (A) for entire study population (B) for group 1 (C) for group 2 and (D) for group 3 neonates, TSB: total serum bilirubin; TCB: transcutaneous bilirubin.
Bland-Altman plot analysis of TSB versus TcB sternum show good agreement between the tests for the study population. Only 17/252 (6.75%) of the tests were outside the limits of agreement with a mean difference of 0.227 [95% CI = –0.038 to 0.493 mg/dL, p-value = 0.092]. This analysis in different groups also show good agreement between TSB and TcB and this agreement was found to be significant only in group 1 [95% CI = –0.088 to 1.174 mg/dL, 2/32 = 6.25% outside the limits of agreement, Mean difference = 0.631, p-value = 0.024] (Fig. 2)
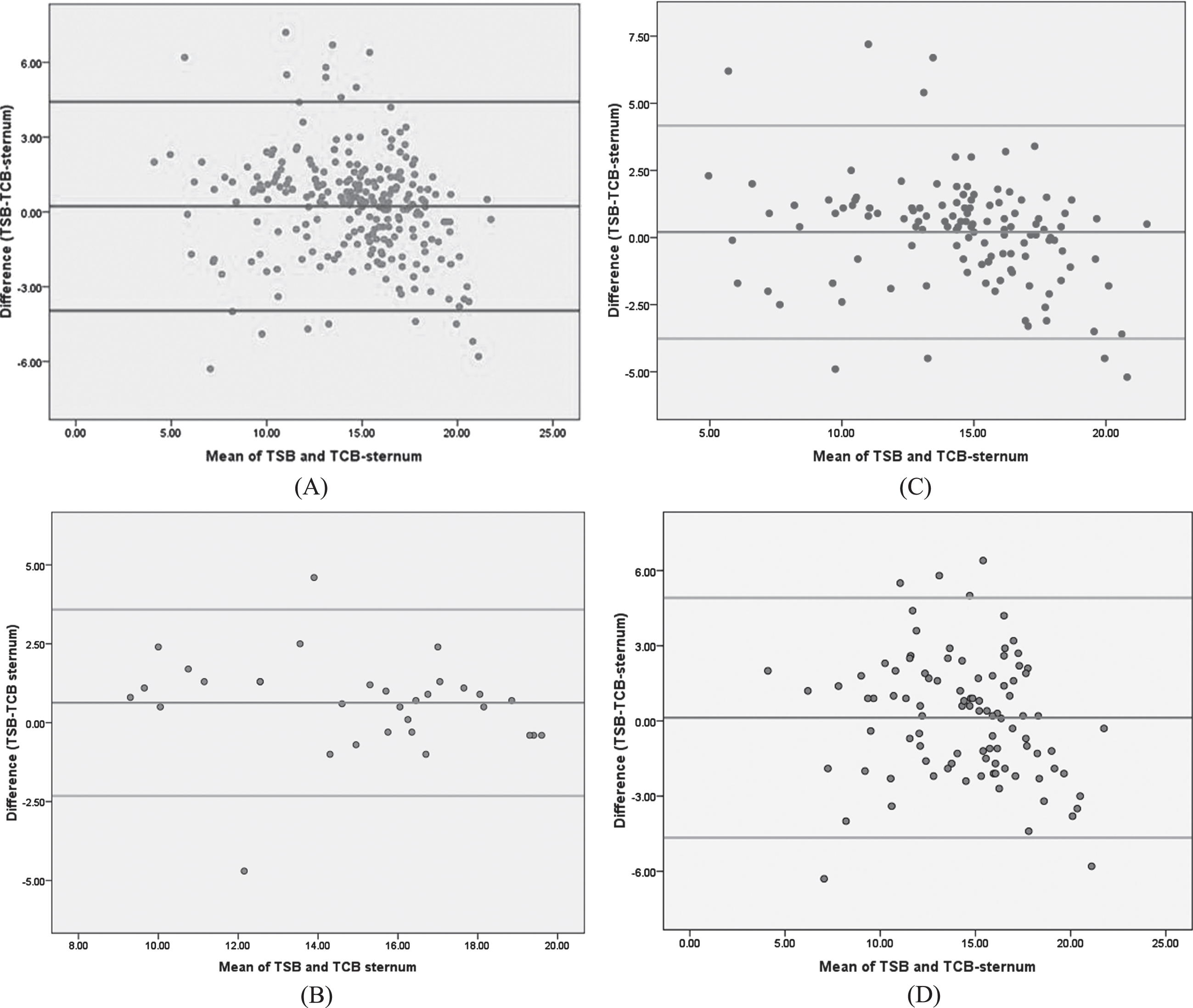
Bland-Atman Plots of transcutaneous bilirubin and total serum bilirubin values (A) for entire study population (B) for group 1 (C) for group 2 and (D) for group 3 neonates, TSB: total serum bilirubin; TCB: transcutaneous bilirubin.
This study demonstrate a strong correlation be-tween TSB and TcB over sternum for entire cohort but when this correlation was compared between groups having different albumin levels, the strongest correlation was observed in group having lower albumin levels.
The correlation between TSB and TcB has been evaluated earlier in many studies but here we evaluated this correlation with relation to serum albumin level. Although, the most common site for TcB measurement in clinical practice is the forehead as it remains exposed and surface is hard enough to record TcB but in this study, we measured the TcB from the sternum as this remain covered with clothes and the measurement from this sight does not affected by the natural light. Yamauchi and Yamauchi have also reported better correlation of TSB to TcB-sternum compared to TcB-forehead [15]. The correlation coefficient we calculated for entire study population was found almost similar to those reported by others [16–18].
While recording the TcB, it should be considered that the TcB is a measurement of the tissue bilirubin whereas TSB represents a measurement of the circulating bilirubin [16]. TcB is an indirect measurement of total serum bilirubin as 99% of what is measured by transcutaneous bilirubinometer is the bilirubin in the extravascular tissue [19]. The mechanism responsible for the yellowness of the skin of jaundiced newborn is not exactly known. It can show variations due to the natural colour of the skin, the diffusion rate of bilirubin into extravascular space and the deposition of bilirubic acid into phospholipid membranes. In a state of equilibrium between plasma and dermal bilirubin concentrations, the intensity of the yellow colour of the skin is positively correlated to three indices: the plasma bilirubin concentration, the squared hydrogen ion concentration and the reciprocal of the reserve albumin concentration [20].
The bilirubin is transported and stabilized by the albumin in the blood. We hypothesize that increased reserve of albumin may be responsible for lower levels of unbound free bilirubin concentration by providing more binding sites and thereby reducing the diffusion of bilirubin to the extravascular compartment. Free bilirubin exits vascular space and enters the tissues at a rate that is proportional to the unbound or free bilirubin concentration [21]. There are many factors that can affect the free bilirubin reserve in the plasma like albumin concentration, presence of other ligands that compete with bilirubin for the binding site on albumin and pH of the blood [22]. Binding affinity of albumin to bilirubin decreases in sepsis and it is increased with the rise of body temperature [23]. Bilirubin movement between the intravascular compartment and skin is bidirectional and this event occurs in a specific balance. In other words, bilirubin which moves from the blood circulation to the skin at a constant rate also returns to the circulation at a constant rate. Here serum albumin considered as a reservoir of bilirubin. While binding of bilirubin by albumin keeps it out of the tissues, it is also a source of bilirubin that could rapidly enter the tissues [24]. Due to these effects, invasive serum bilirubin measurement is the gold standard method of bilirubin measurement.
Another finding of this study is that the transcutaneous bilirubinometer overestimates the bilirubin levels. This over-estimation will lead to some neonates receiving unnecessary phototherapy but it can be beneficial in resource limiting settings where frequent bilirubin monitoring is not possible and further it may prevent the potentially severe damage caused by kernicterus. Like our study, many studies including Afanetti et al. [25] and Olusanya et al. [26] have found slightly higher values in TcB with good overall correlation. In contrast to our study, Engel et al. found that TcB tend to underestimate the values of TSB in Hispanic infants [27].
The strength of this study is the large sample size of exclusively term North Indian neonates. This is the first study, to the best of our knowledge, which compares the TSB with TcB at different albumin levels.
This study has few limitations also. First the neonates enrolled in this study, were with different skin colours, whereas the most of other studies were included the neonates with same skin pigmentation. Second we had not excluded the neonates with sepsis and on antibiotics while these are the known factor which may decrease the affinity of albumin for bilirubin. Although high pressure liquid chromatography bilirubin (HPLC-B) is considered as the gold standard method for true reference value of TSB measurement but we have used principal of Modified Malloy Evelyn method which also have good accuracy [28].
Conclusions
Although TcB measurements using the transcutaneous bilirubinometer correlate closely with total serum bilirubin levels but this correlation may be affected by the serum albumin level along with the other factors. However, in absence of availability of invasive method or in case of delay in TSB results, TcB can still be used as an alternative for screening even at age < 24 hrs in term neonates.
Financial support and sponsorship
None.
Conflicts of interest
None.