
Abstract
Background
Cerebral blood flow (CBF) is critical for neonatal brain health, and disruption of autoregulation may predispose infants to brain injury. The resistive index (RI) of the anterior cerebral artery (ACA), measured via Doppler ultrasonography, is a widely used non-invasive marker of CBF, but its relationship with vital parameters in critically ill neonates remains uncertain.
Methods
This retrospective study at Taipei Veterans General Hospital from January 2022 to December 2024 included neonates admitted to the NICU with ACA Doppler ultrasonography within 24 h of birth. RI values were stratified into three groups: low (<0.6), normal (0.6–0.8), and high (>0.8). Clinical characteristics, resuscitation needs, Apgar scores, blood gas analyses, and short- and long-term outcomes were compared across groups.
Results
Among 898 admissions, 386 neonates met the inclusion criteria (mean gestational age 35 ± 4 weeks, mean birth weight 2382 ± 847 g), abnormal RI was identified in 25.1% (low RI: 4.1%, high RI: 21.0%). Abnormal RI correlated with significantly lower pH, higher pCO2, lower 5-min Apgar scores, and greater need for delivery room intubation (p < 0.01). After adjusting for gestational age, birth weight, and evaluation timing, low RI remained independently associated with increased risks of systemic hypotension and fluid resuscitation (p < 0.05).
Conclusion
Abnormal ACA RI within 24 h of birth is associated with cerebral hemodynamic instability in critically ill neonates. Early RI assessment may provide insights into neonatal hemodynamic status and serve as a supplemental clinical indicator for identifying high-risk infants in the NICU.
Introduction
Cerebral blood flow (CBF) plays a pivotal role in maintaining neonatal brain health, particularly during the vulnerable perinatal and early postnatal periods. Disruptions in cerebral circulation and autoregulation can arise from various pathological conditions, including prematurity, intraventricular hemorrhage (IVH), patent ductus arteriosus (PDA), shock, and hypoxic-ischemic encephalopathy (HIE), and are associated with adverse neurodevelopmental outcomes. These conditions can alter cerebrovascular resistance and compromise oxygen and nutrient delivery to the developing brain. 1
Several non-invasive techniques have been developed to assess CBF, with Doppler ultrasonography being widely utilized in neonatal intensive care. The resistive index (RI), calculated as RI = (peak systolic velocity – end-diastolic velocity)/peak systolic velocity, is one of the most frequently adopted Doppler-derived parameters. 2 While the normal RI range varies among studies, the present work employs the Johns Hopkins reference range of 0.6–0.8. 3 Anterior cerebral artery (ACA) is a preferred vessel for Doppler assessment due to its accessibility via the anterior fontanelle and its sensitivity to systemic circulatory changes. Despite extensive research, the relationship between RI and various clinical parameters, such as Apgar scores and blood gas analysis, remains inconclusive. CBF is thought to be highly related to cerebral metabolism and arterial blood gas levels. 4 Some studies suggest that alterations in pCO2 play a key role in determining CBF velocity, raising concerns about its potential contribution to neonatal brain injury. 1 However, previous studies have reported no significant association between RI and 1- or 5-min Apgar scores, umbilical cord pH, or base excess levels. 3
Given these uncertainties, it remains unclear how early RI measurements relate to vital perinatal parameters and subsequent morbidity in critically ill neonates. Clarifying these associations could enhance early risk stratification and inform individualized management strategies in the NICU. Therefore, the objective of this study was to evaluate the correlation between ACA RI measured within the first 24 h of life and clinical vital parameters, perinatal conditions, and outcomes in neonates requiring intensive care.
Methods
Study design and setting
This was a single-center, retrospective cohort study conducted at Taipei Veterans General Hospital from January 2022 to December 2024. Eligible participants were neonates admitted to the neonatal intensive care unit (NICU) who underwent ACA Doppler ultrasonography within the first 24 h after birth. Neonates were excluded based on the following criteria: (1) admission to the NICU beyond 24 h after birth; (2) initial ACA Doppler ultrasonography performed more than 24 h after birth (e.g., due to logistical delays during weekends or other administrative factors); (3) ACA RI measurements were not performed or not documented in the specified time frame.
Patient population and clinical management
Admission to the NICU was determined by neonatologists based on clinical indications, including but not limited to respiratory distress, meconium aspiration syndrome (MAS), prematurity or very low birth weight, and other perinatal complications. A majority of patients required respiratory support during hospitalization.
Ultrasound measurement protocol
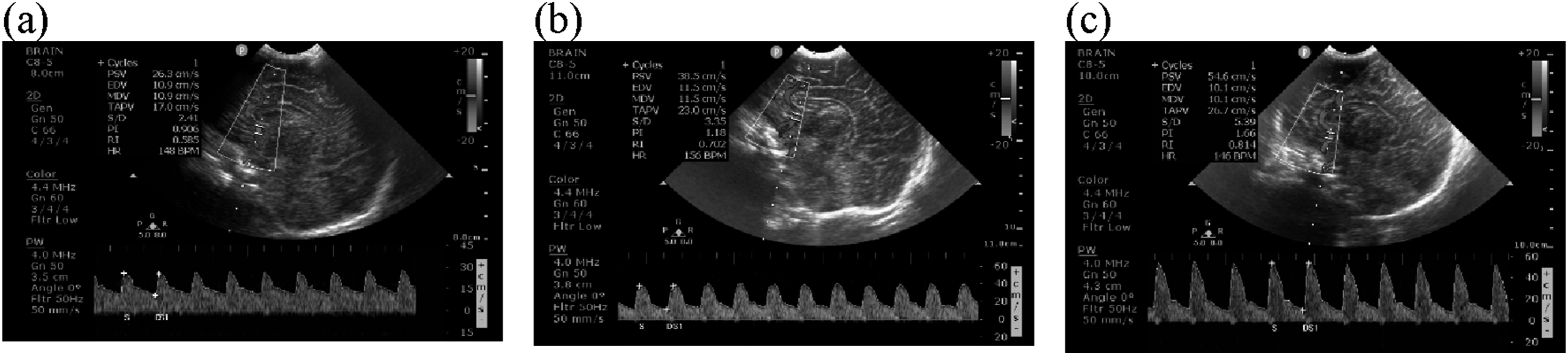
Routine cranial ultrasonography, including ACA Doppler assessment, was performed for all admitted neonates. Doppler measurements were acquired using a Philips CX50 vascular ultrasound system with a C8-5 curved array transducer (4.4 MHz). Imaging was performed via the anterior fontanelle in the sagittal plane, visualizing the ACA anterior to the corpus callosum. Cranial Doppler examinations were performed by neonatal fellows and subsequently reviewed by attending neonatologists for quality assurance; representative images are shown in Figure 1. RI values were categorized as follows: • Normal RI (Group N): 0.60–0.80 • Low RI (Group L): <0.60 • High RI (Group H): >0.80 Representative cerebral Doppler ultrasonography images of the ACA. The Doppler waveforms and RI measurements shown here are representative examples obtained at our institution. The images illustrate the hemodynamic patterns of the three study groups: (a) Low RI group (RI = 0.585); (b) Normal RI group (RI = 0.702); and (c) High RI group (RI = 0.814). Each panel displays the color Doppler flow signal (top) and the corresponding pulse-wave Doppler spectral waveform (bottom) used for clinical assessment. Abbreviations: ACA: anterior cerebral artery; EDV: end-diastolic velocity; PSV: peak systolic velocity; RI: resistive index.
Data collection
Demographic and perinatal data included gestational age, birth weight, sex, delivery mode, use of positive pressure ventilation (PPV), and endotracheal intubation during neonatal resuscitation in the delivery room. Clinical variables collected included 1- and 5-minute Apgar scores and blood gas parameters obtained within the first hour after birth (pH, pCO2, HCO3-, base excess).
Outcome measures
Primary short-term outcomes were interventions required within 7 days of life, including respiratory support, fluid resuscitation, inotropic support, and therapeutic hypothermia. Secondary outcomes included incidence and severity of intraventricular hemorrhage (IVH, graded by Papile classification), severe IVH (grade 3 or 4), bronchopulmonary dysplasia (BPD, per 2019 Jensen criteria), PDA treatment status, NICU and total hospital length of stay, and in-hospital mortality. Subgroup analyses compared preterm (<37 weeks gestation) versus term (≥37 weeks) neonates.
Statistical analysis
Data analyses were performed using Microsoft Excel and SPSS version 25.0. Continuous variables were analyzed using one-way ANOVA with Tukey post-hoc testing, or Kruskal–Wallis test for non-normally distributed data. Multivariate logistic regression analysis was performed to evaluate the independent association between RI groups and clinical outcomes, adjusting for variables that showed significant baseline differences or were clinically relevant. Categorical variables were compared using the Chi-square test. A two-tailed p value <0.05 was considered statistically significant.
Results
Patient characteristic
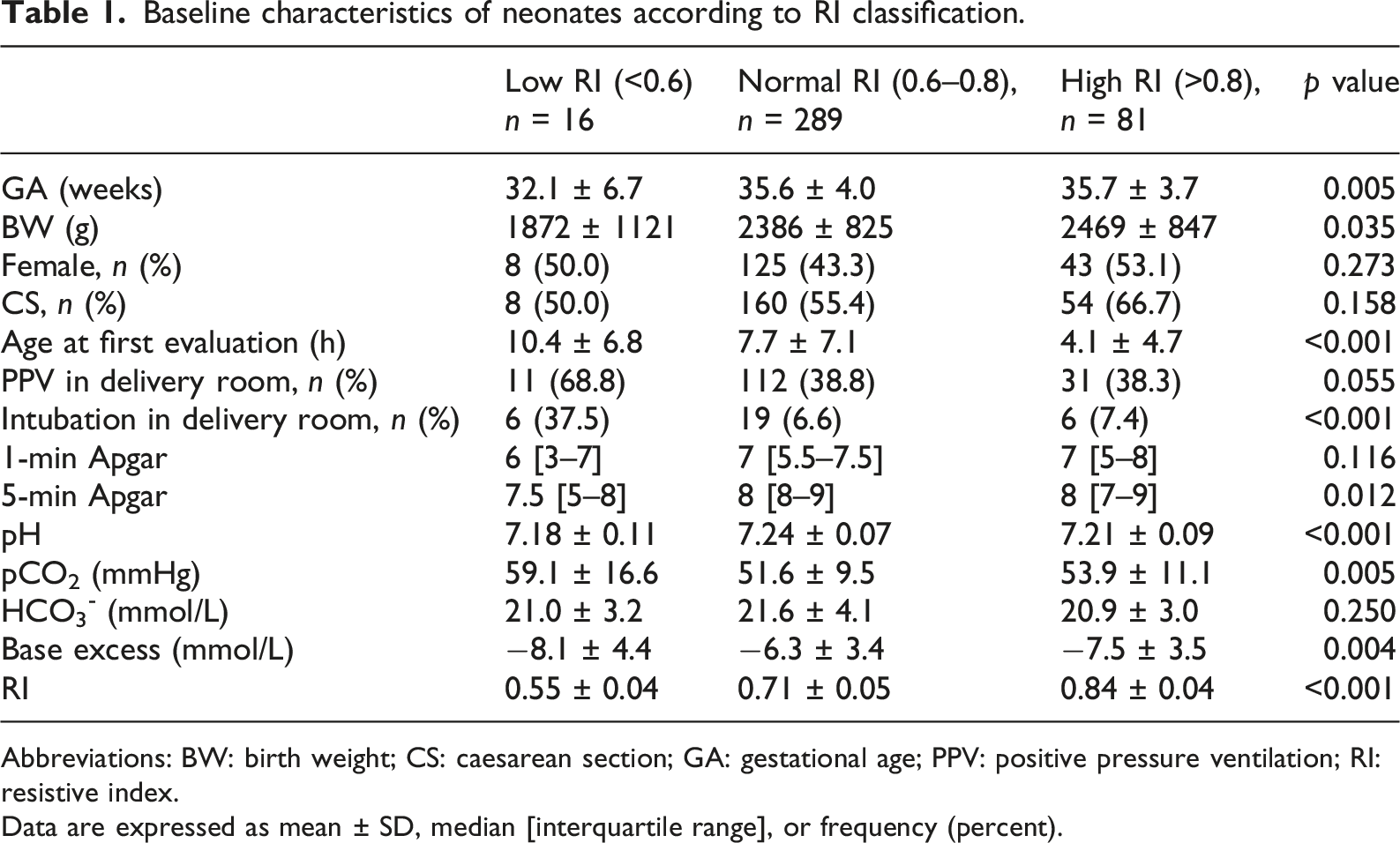
Between January 2022 and December 2024, 898 patients were admitted to the NICU. Among them, 512 were excluded because no ACA RI Doppler examination records were available within the first 24 h of life Figure 2. The clinical characteristics of the excluded infants are detailed in Table S1. Overall, 386 neonates entered the study, with a mean gestational age of 35 ± 4 weeks and mean birth weight of 2382 ± 847 g. Based on anterior cerebral artery (ACA) resistive index (RI), 289 infants (74.9%) were classified as normal (RI 0.6–0.8), 16 (4.1%) as low RI (<0.6), and 81 (21.0%) as high RI (>0.8). Baseline characteristics across groups are summarized in Table 1. Neonates with low RI had significantly lower gestational age (32.1 ± 6.7 weeks) and birth weight (1872 ± 1121 g) compared with the normal and high RI groups (p < 0.05). The timing of first evaluation was later in the low RI group (10.4 ± 6.8 h vs 7.7 ± 7.1 h and 4.1 ± 4.7 h, p < 0.001). Intubation during delivery room resuscitation was more frequent in the low RI group (37.5%) compared to the other groups (6.6% and 7.4%, p < 0.001). Significant differences were also observed in 5-min Apgar scores, arterial pH, pCO2, and base excess among the three groups (all p < 0.05). Flowchart of patient selection. A total of 898 neonates were admitted to the NICU during the study period. Of these, 512 were excluded. Reasons for exclusion included: age at admission >24 h (n = 199), ACA RI performed ≥24 h after birth (n = 32), and ACA RI not performed (n = 281). The remaining 386 neonates were eligible and included in the final analysis. Abbreviations: ACA: anterior cerebral artery; NICU: neonatal intensive care unit; RI: resistive index. Baseline characteristics of neonates according to RI classification. Abbreviations: BW: birth weight; CS: caesarean section; GA: gestational age; PPV: positive pressure ventilation; RI: resistive index. Data are expressed as mean ± SD, median [interquartile range], or frequency (percent).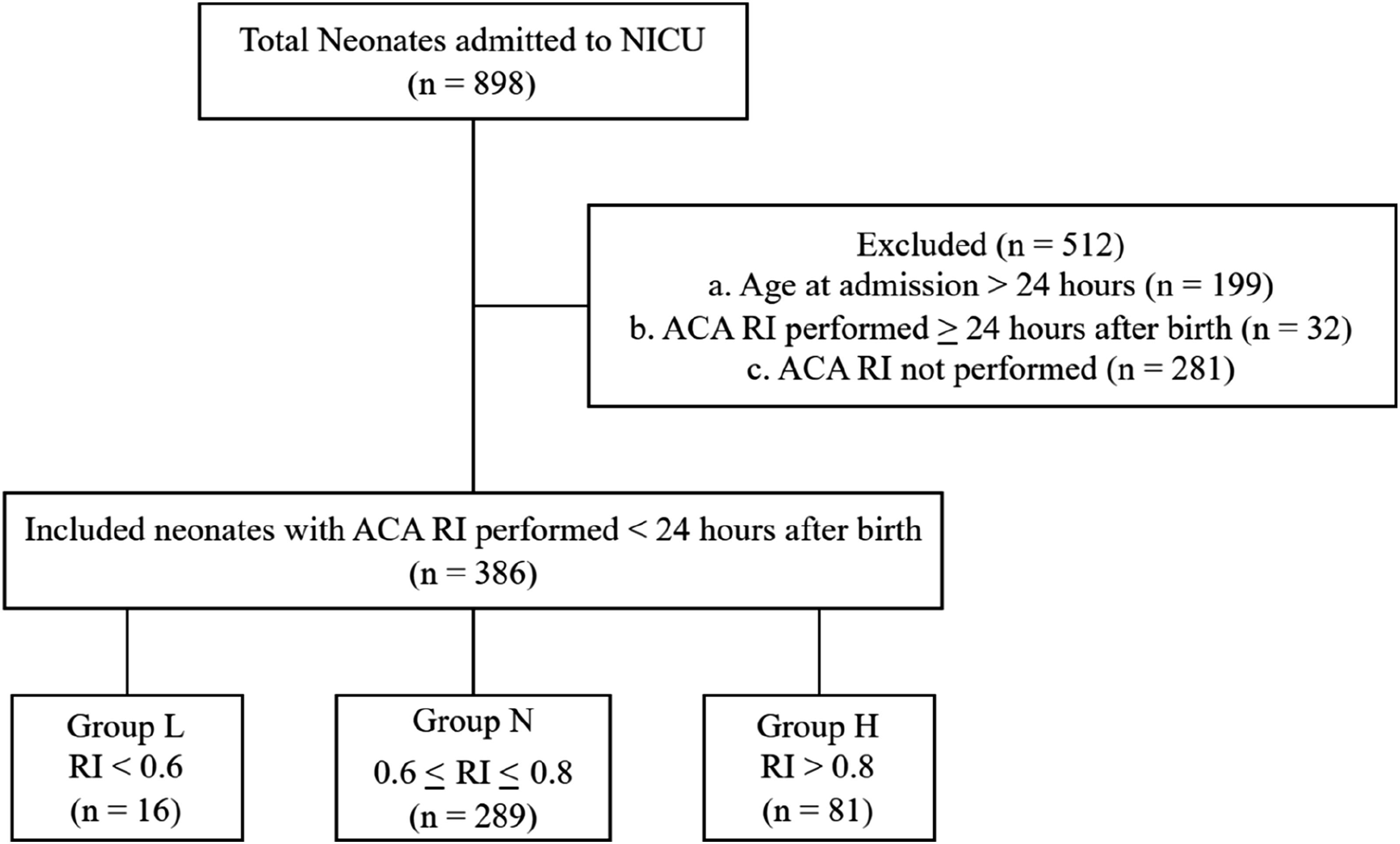
Preterm versus term subgroup analysis
Patients’ characteristics by gestational age (preterm vs full-term).
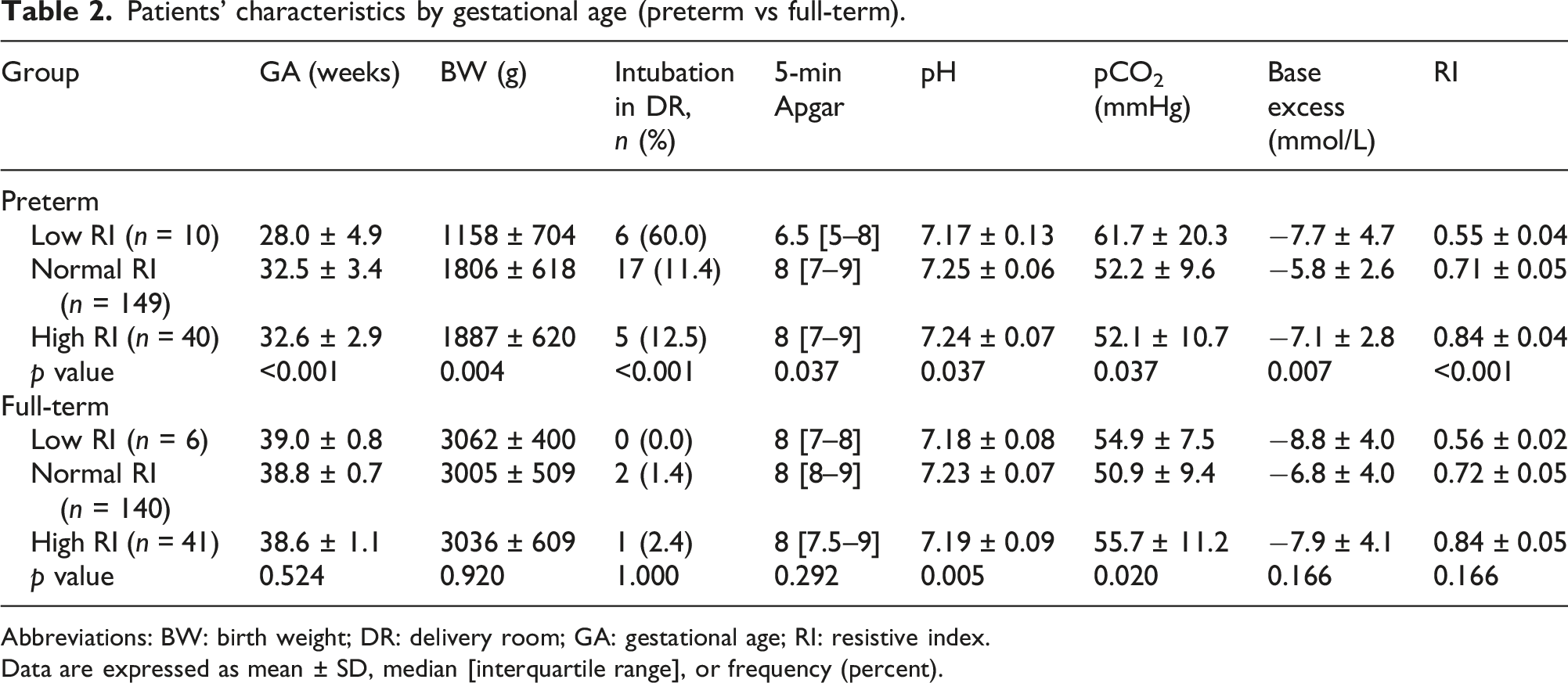
Abbreviations: BW: birth weight; DR: delivery room; GA: gestational age; RI: resistive index.
Data are expressed as mean ± SD, median [interquartile range], or frequency (percent).
Short-term and long-term outcomes
Short- and long-term outcomes by RI classification.
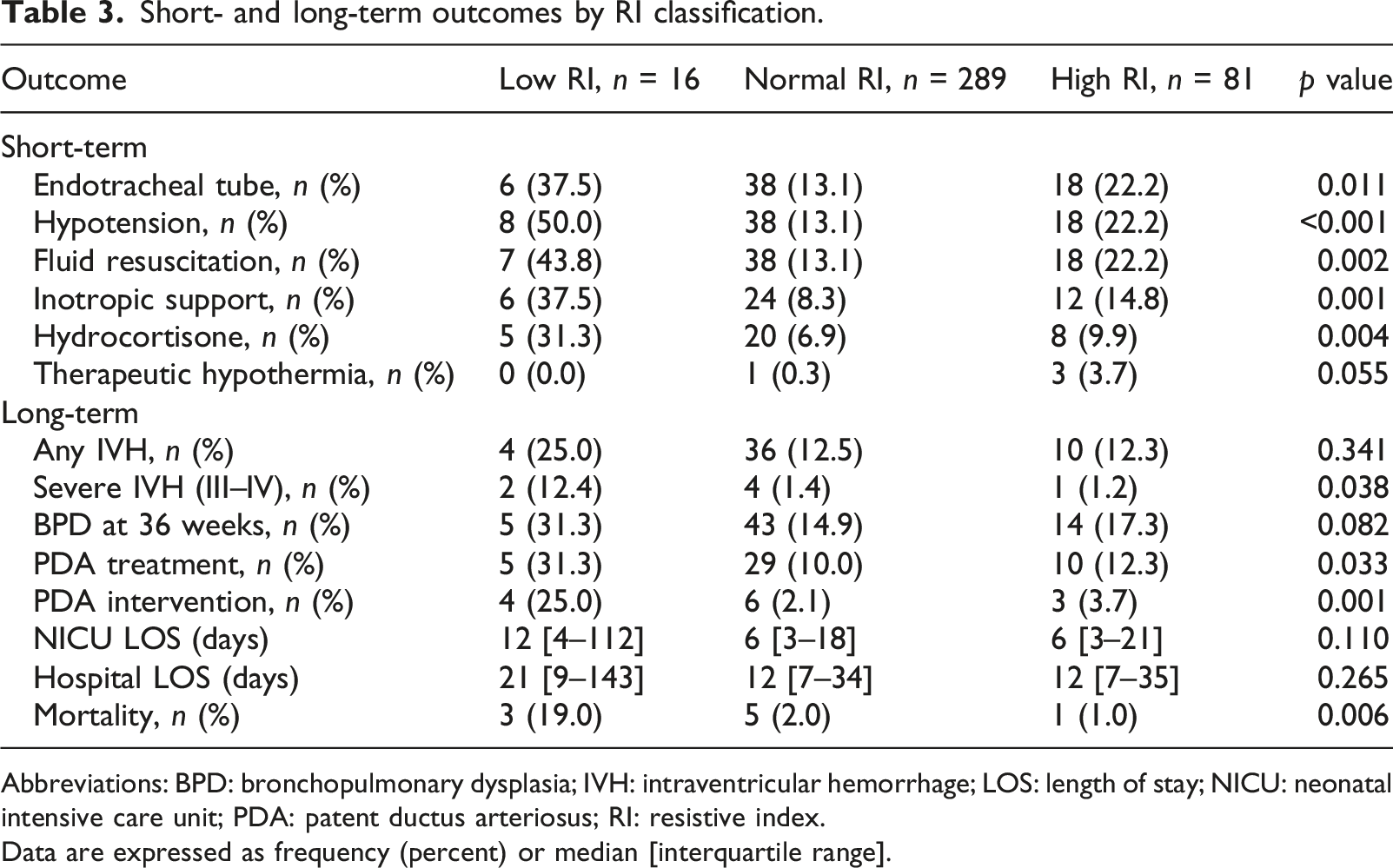
Abbreviations: BPD: bronchopulmonary dysplasia; IVH: intraventricular hemorrhage; LOS: length of stay; NICU: neonatal intensive care unit; PDA: patent ductus arteriosus; RI: resistive index.
Data are expressed as frequency (percent) or median [interquartile range].
Regarding long-term outcomes, severe IVH (IVH grade III–IV) was more frequent in the low RI group (12.4%) compared with the normal (1.4%) and high RI (1.2%) groups (p = 0.038). Treatment for PDA was also more common among infants with abnormal RI (p = 0.033), with a notably higher rate of surgical or catheter-based intervention in the low RI group (25.0% vs 2.1% in normal RI; p = 0.001). Mortality was significantly higher in neonates with low RI (19%) compared to those with normal (2%) or high RI (1%) (p = 0.006).
Preterm and term outcome comparisons
Outcomes in preterm and full-term infants according to RI classification.
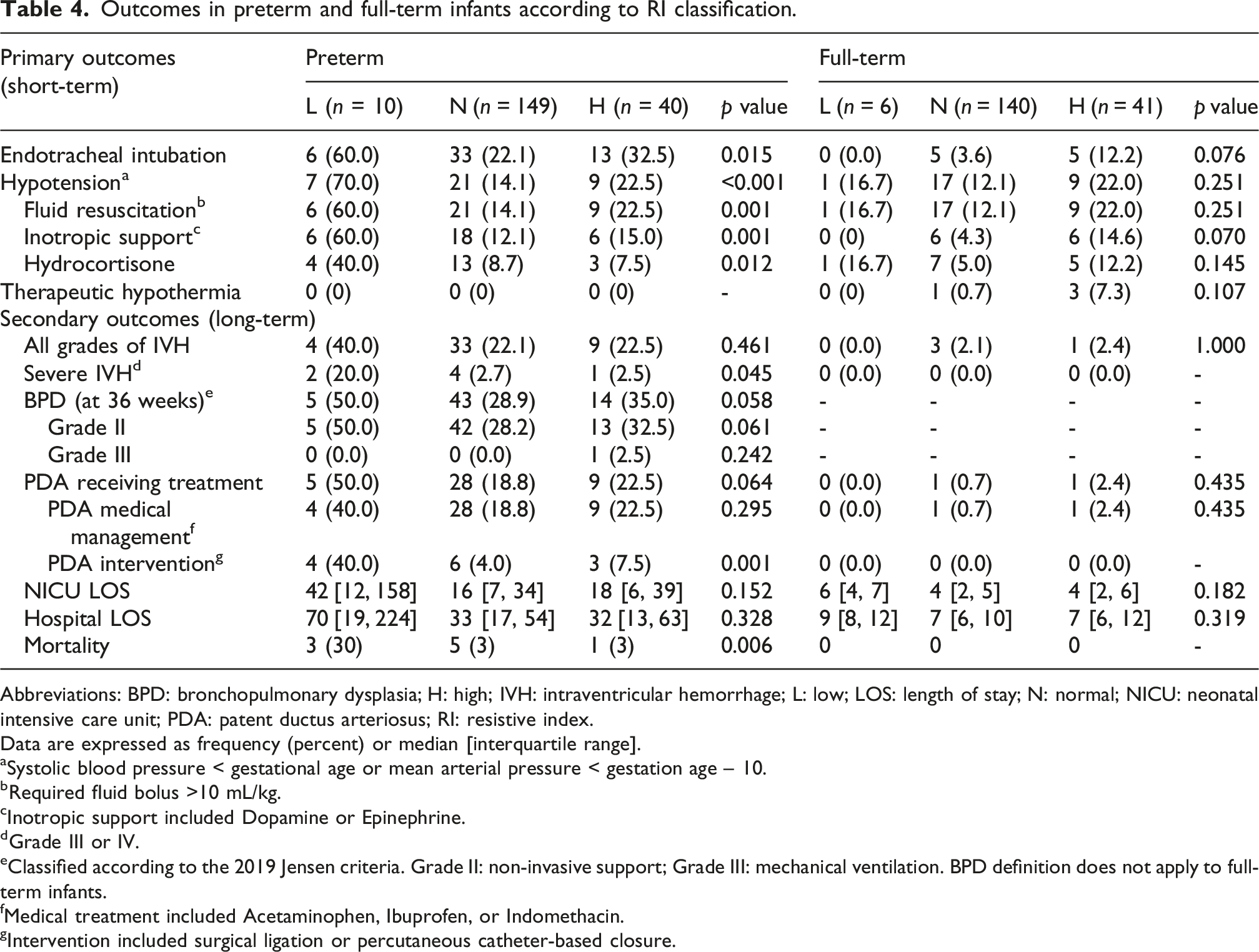
Abbreviations: BPD: bronchopulmonary dysplasia; H: high; IVH: intraventricular hemorrhage; L: low; LOS: length of stay; N: normal; NICU: neonatal intensive care unit; PDA: patent ductus arteriosus; RI: resistive index.
Data are expressed as frequency (percent) or median [interquartile range].
aSystolic blood pressure < gestational age or mean arterial pressure < gestation age – 10.
bRequired fluid bolus >10 mL/kg.
cInotropic support included Dopamine or Epinephrine.
dGrade III or IV.
eClassified according to the 2019 Jensen criteria. Grade II: non-invasive support; Grade III: mechanical ventilation. BPD definition does not apply to full-term infants.
fMedical treatment included Acetaminophen, Ibuprofen, or Indomethacin.
gIntervention included surgical ligation or percutaneous catheter-based closure.
In contrast, among term infants, the differences between RI groups were less striking. Although some variation in pH and pCO2 persisted, short-term outcomes such as intubation, hypotension, and PDA treatment did not differ significantly across RI categories. No deaths occurred among term infants during the study period.
Independent predictors of clinical outcomes
To determine whether RI acts as an independent predictor beyond the confounding effects of prematurity and clinical timing, a multivariate logistic regression was performed (Table 5). After adjusting for gestational age, birth weight, and age at first RI evaluation, low RI remained significantly associated with an increased risk of hypotension (aOR 4.904; 95% CI 1.509–15.935; p = 0.008) and the need for fluid resuscitation (aOR 3.600; 95% CI 1.109–11.687; p = 0.033). However, the associations with severe IVH and mortality were no longer significant after adjustment, suggesting these outcomes are more closely linked to the degree of prematurity than to RI alone.
Non-survivor characteristics
Univariate and multivariable logistic regression analysis of RI groups for clinical outcomes.
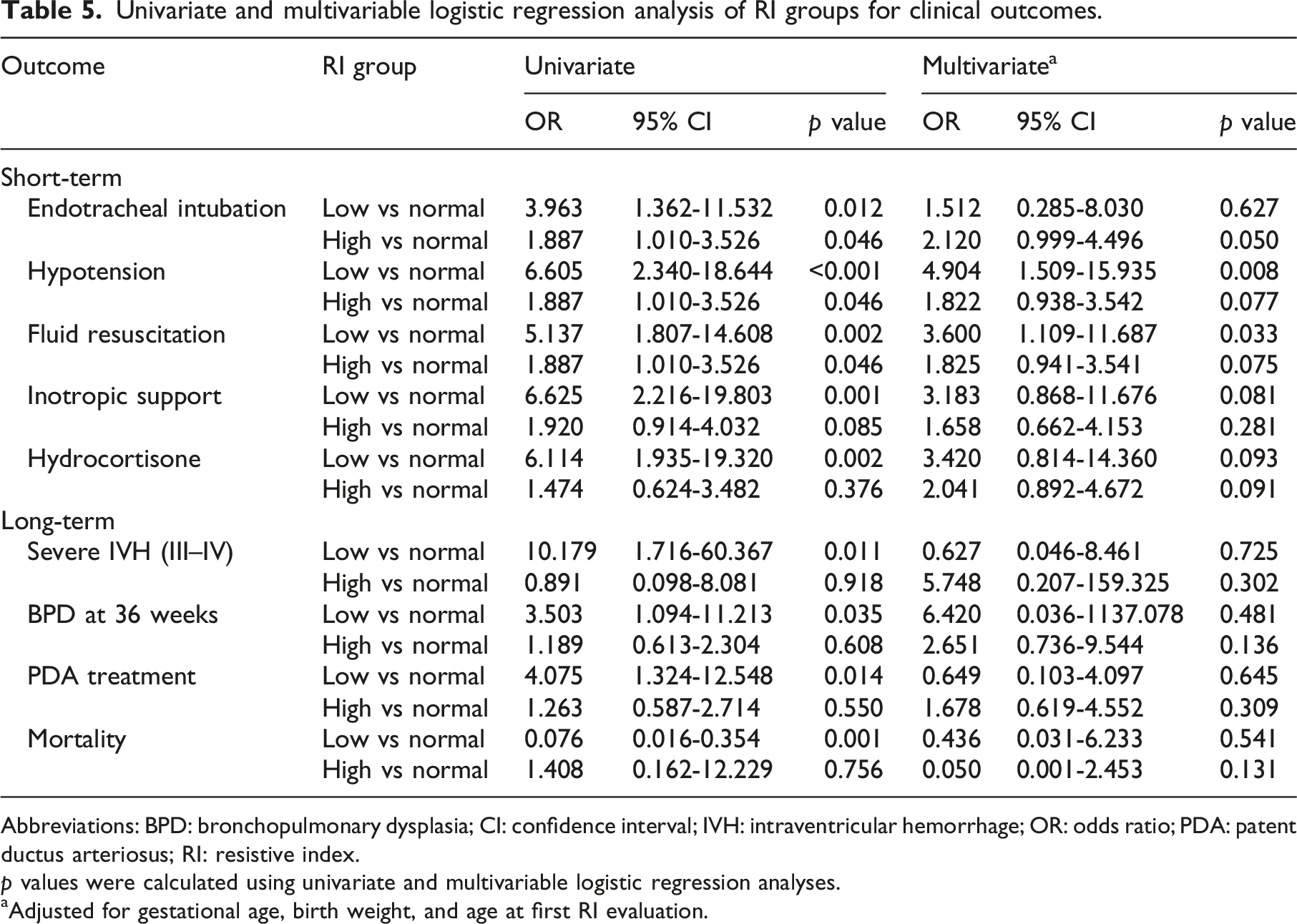
Abbreviations: BPD: bronchopulmonary dysplasia; CI: confidence interval; IVH: intraventricular hemorrhage; OR: odds ratio; PDA: patent ductus arteriosus; RI: resistive index.
p values were calculated using univariate and multivariable logistic regression analyses.
aAdjusted for gestational age, birth weight, and age at first RI evaluation.
Neonates treated with therapeutic hypothermia
Clinical and laboratory characteristics of non-surviving neonates (n = 9).
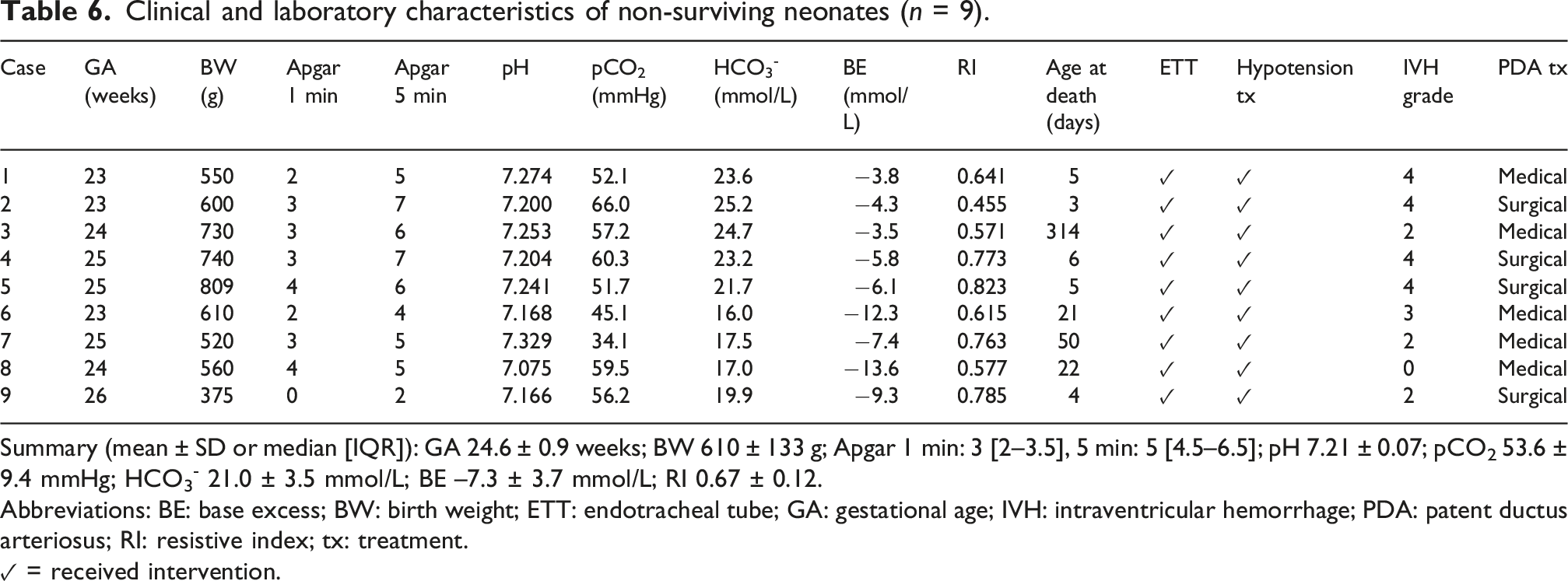
Summary (mean ± SD or median [IQR]): GA 24.6 ± 0.9 weeks; BW 610 ± 133 g; Apgar 1 min: 3 [2–3.5], 5 min: 5 [4.5–6.5]; pH 7.21 ± 0.07; pCO2 53.6 ± 9.4 mmHg; HCO3- 21.0 ± 3.5 mmol/L; BE –7.3 ± 3.7 mmol/L; RI 0.67 ± 0.12.
Abbreviations: BE: base excess; BW: birth weight; ETT: endotracheal tube; GA: gestational age; IVH: intraventricular hemorrhage; PDA: patent ductus arteriosus; RI: resistive index; tx: treatment.
✓ = received intervention.
Discussion
In this study, we evaluated the cerebral RI of the ACA within the first 24 h of life in a large cohort of NICU-admitted neonates and investigated its association with perinatal characteristics and clinical outcomes. We found that approximately one-quarter of neonates exhibited abnormal RI values (<0.6 or >0.8). Both low and high RI were associated with adverse vital signs, metabolic derangements, and increased risks of short- and long-term complications compared with neonates with normal RI. Recent reviews have emphasized that impairment of cerebral autoregulation places neonates at heightened risk for brain injury because both hypoperfusion and hyperperfusion can occur when the normal vasoconstrictive and vasodilatory responses to arterial blood pressure fluctuations fail.5,6 These disturbances have been described across a range of neonatal conditions, including prematurity, IVH, HIE, and systemic hemodynamic instability.6,7
Our results demonstrate that abnormal RI is closely linked with impaired transition at birth, as evidenced by lower Apgar scores, higher need for delivery room intubation, and acidosis with elevated pCO2. These findings are consistent with the prior study reporting that cerebral hemodynamics are highly sensitive to perinatal hypoxia, ventilation status, and systemic circulation disturbances. 8 The neonatal cerebral vasculature is exquisitely sensitive to pCO2, a reactivity that further complicates hemodynamic stability in this vulnerable population. 5 Comparative findings from other studies also support that cerebrovascular autoregulation is uniquely vulnerable during the immediate postnatal transition, when fluctuations in perfusion pressure and gas exchange can readily disrupt cerebral blood flow control. 8
Importantly, our study demonstrates that low RI is a potent and independent predictor of early hemodynamic instability. After adjusting for gestational age, birth weight, and age at first RI evaluation, infants with low RI remained at a significantly higher risk for systemic hypotension and the requirement for fluid resuscitation. These findings support the hypothesis that low RI reflects cerebral hyperperfusion.
In preterm infants, impaired autoregulation of fragile vasculature predisposes the brain to hemorrhagic complications. 9 The autonomic nervous system in preterm infants is inherently immature, significantly elevating the risk of low CBF during episodes of systemic hypotension. 10 Consistent with previous studies that found no significant link between brain RI and IVH, 11 our cohort also showed that low RI may not be the sole independent driver of IVH. However, its strong association with systemic hypotension—which we found to be independent of GA—suggests that low RI serves as a crucial clinical “red flag” for an imminent breakdown in circulatory homeostasis. This systemic instability, as evidenced by the increased need for inotropic support and fluid boluses in the low RI group, likely creates the fluctuating cerebral blood flow patterns that ultimately exceed the tolerance of the fragile preterm brain.
Conversely, high RI was associated with increased cardiopulmonary support and adverse outcomes, albeit with lower mortality than the low RI group. Elevated RI may reflect increased cerebrovascular resistance due to hypoxia, hypoperfusion, or raised intracranial pressure. This pattern has been described in neonates with perinatal asphyxia and correlates with poor neurodevelopmental prognosis. The four neonates with hypoxic-ischemic encephalopathy in our study demonstrated markedly abnormal RI prior to therapeutic hypothermia, with partial normalization following treatment. These observations suggest that RI may also serve as a non-invasive biomarker of treatment response.
While a low RI (<0.6) is traditionally associated with poor prognosis due to loss of autoregulation in HIE, 12 early high RI may serve as a precursor or an alternative marker of severe injury. 13 Our observation is consistent with the findings of Kumar et al. (2021), who demonstrated that neonates with low 5-min Apgar scores exhibit high RI in the early postnatal phase (mean 3.6 h). 13 This phenomenon has been previously characterized as a primary insult stage, reflecting a transient period of intense vasoconstriction or reduced diastolic flow before the onset of secondary energy failure. 13
The timing of measurement is critical for interpreting these findings, as neonatal cerebral hemodynamics are highly dynamic during the first 24 h of life. On a general population level, the High RI group in our study was evaluated at a significantly earlier time point (mean 4.1 h) than other groups. This aligns with the physiological transition of immediate postnatal life, where cerebral vascular resistance is typically at its peak during the initial adaptation to extrauterine circulation, followed by a gradual decline as systemic and pulmonary circulations stabilize. 14 The clinical relevance of this temporal evolution in specific disease states is further demonstrated by the neonates in our cohort who received therapeutic hypothermia (Table 7). In these HIE cases, initial RI values within the first 24 h were notably high (mean 0.84 ± 0.12), but subsequently declined to lower levels (mean 0.67 ± 0.09) following clinical stabilization. This transition explains the disparity between our data and reports of low RI, as earlier assessments are more likely to capture the transient high-resistance phase.
Clinical and laboratory characteristics of neonates treated with therapeutic hypothermia (n = 4).
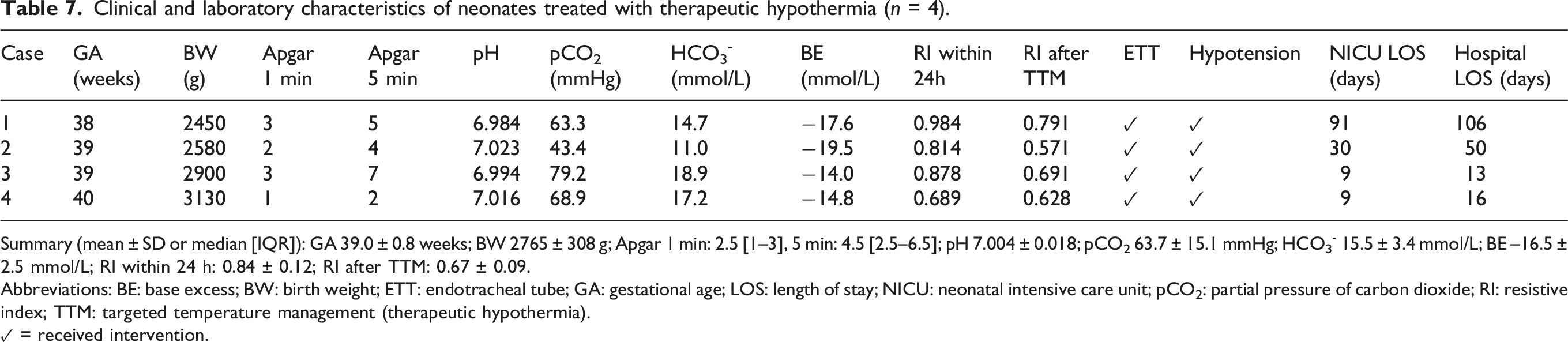
Summary (mean ± SD or median [IQR]): GA 39.0 ± 0.8 weeks; BW 2765 ± 308 g; Apgar 1 min: 2.5 [1–3], 5 min: 4.5 [2.5–6.5]; pH 7.004 ± 0.018; pCO2 63.7 ± 15.1 mmHg; HCO3- 15.5 ± 3.4 mmol/L; BE –16.5 ± 2.5 mmol/L; RI within 24 h: 0.84 ± 0.12; RI after TTM: 0.67 ± 0.09.
Abbreviations: BE: base excess; BW: birth weight; ETT: endotracheal tube; GA: gestational age; LOS: length of stay; NICU: neonatal intensive care unit; pCO2: partial pressure of carbon dioxide; RI: resistive index; TTM: targeted temperature management (therapeutic hypothermia).
✓ = received intervention.
Our findings suggest the potential clinical value of early cerebral Doppler assessment as a supplemental marker for the assessment of critically ill neonates. The identification of high-risk infants shortly after birth may support closer monitoring for hemodynamic stability. While ACA RI is a simple and non-invasive observational tool, it should be interpreted in the context of gestational age, hemodynamic status, and concomitant morbidities.
Looking forward, future research should prioritize establishing standardized clinical criteria for cerebral Doppler measurements in critically ill neonates, specifically tailored to gestational age and underlying pathologies. The substantial proportion of infants excluded from this retrospective cohort underscores the necessity of moving toward a comprehensive institutional protocol. Transitioning from a single assessment within the first 24 h of life to serial ACA RI monitoring through a prospective approach would ensure higher data completeness. Such longitudinal analysis would allow for a more robust understanding of the dynamic correlations between cerebral hemodynamics and clinical parameters throughout the neonatal course.
This study has several limitations. First, the single-center design and relatively small sample size may limit the generalizability of our findings. Specifically, the limited number of neonates in the low RI group (n = 16) may reduce the power of our multivariate analysis to detect independent associations for less frequent outcomes, such as severe IVH or mortality, after accounting for gestational age, birth weight, and age at first RI evaluation. Second, although the Doppler measurements were performed by neonatal fellows, who underwent standardized training prior to their participation, the involvement of multiple operators may still introduce inter-observer variability.
Third, the retrospective nature of the study led to a high exclusion rate, as early ACA Doppler screening was not a universal mandate during the initial phase of our study period. As shown in Table S1, infants excluded due to the lack of early ACA Doppler data had higher GA and BW. Clinically, it is likely that more stable near-term or term neonates did not undergo cerebral hemodynamic assessment immediately after birth, as the clinical urgency for such monitoring may be lower in this population. Therefore, their initial ACA Doppler scans are more likely to be performed beyond the first 24 h of life. While this ensures our study cohort strictly represents neonates requiring early-life monitoring, the findings may not be fully generalizable to the entire NICU population, particularly those who are more clinically stable at birth. Furthermore, while we performed subgroup and multivariate analyses to address the heterogeneity between preterm and term infants, the differing underlying pathophysiology in these groups remains a potential confounding factor that warrants further investigation in larger, prospective cohorts. Finally, long-term neurodevelopmental outcomes were not assessed, and thus the predictive value of RI for later impairment remains uncertain.
Conclusions
In conclusion, abnormal ACA RI within the first 24 h of life is common in NICU-admitted neonates and is independently associated with early hemodynamic disturbances. Specifically, after adjusting for potential confounders, abnormal RI values—particularly low RI—exhibited a significant independent association with systemic hypotension and the requirement for fluid resuscitation. Both low and high RI values reflect disturbed cerebral hemodynamics with distinct clinical implications. These findings suggest that early assessment of cerebral RI may serve as a supplemental clinical indicator to support risk assessment and hemodynamic monitoring in neonatal intensive care.
Supplemental material
Supplemental material - Early cerebral hemodynamic assessment using resistive index and its correlation with neonatal outcomes
Supplemental Material for Early cerebral hemodynamic assessment using resistive index and its correlation with neonatal outcomes by Ting-An Hsia, Chia-Sui Chou, Wei-Yu Chen, Pei-Chen Tsao, Yu-Sheng Lee, Mei-Jy Jeng in Journal of Neonatal-Perinatal Medicine
Footnotes
Ethical considerations
This study was performed in line with the principles of the Declaration of Helsinki. Approval was granted by the Institutional Review Board of Taipei Veterans General Hospital (Approval No. 2025-04-003BC).
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by a grant from Taipei Veterans General Hospital (Grant number: V115C-198).
Declaration of conflicting interests
The authors declare that they have no conflicts of interest related to the subject matter or materials discussed in this article.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.