
Abstract
Background
Lung recruitment maneuvers (LRM) during high-frequency oscillatory ventilation (HFOV) lack bedside standardized monitoring.
Aim
To evaluate the efficacy and safety of FiO2-guided LRM in preterm infants with moderate-to-severe respiratory-distress syndrome (RDS) using integrated functional echocardiography (FE) and lung ultrasound (LUS). Also, we hypothesized that a standardized LUS score can accurately guide successful recruitment.
Methods
This a prospective, single-arm, protocol-driven cohort study that was conducted at a tertiary NICU (Alexandria University), and 70 preterm infants (GA 32–37 weeks) requiring HFOV within 24 h of life were included. Integrated LUS and FE were performed at three phases: pre-initiation, maintenance pressure (opening), and pre-weaning. Lung aeration was quantified using a standardized 12-zone LUS protocol (0–3 points per zone) based on international consensus. Hemodynamics were assessed via tricuspid regurgitation (TR) gradient, superior vena cava (SVC) flow, and right ventricular myocardial performance index (RV-MPI).
Results
LRM led to significant improvements in oxygenation and lung aeration. Mean LUS scores decreased significantly from 23.13 ± 1.33 (pre-initiation) to 19.94 ± 1.67 (maintenance) and 3.70 ± 2.49 (pre-weaning) (p < 0.001). FE demonstrated a significant reduction in TR gradient (p < 0.001), while SVC flow and RV-MPI remained stable, indicating preserved myocardial function. Pre-weaning LUS scores were significantly associated with weaning success from HFOV.
Conclusions
FiO2-guided LRM is effective and safe in late-preterm infants with RDS. Integrated bedside imaging confirms that recruitment improves lung aeration without compromising hemodynamics. A standardized LUS score is a reliable tool for identifying optimal lung opening and guiding the weaning process.
Keywords
(1) FiO2-guided lung recruitment has been shown to enhance lung aeration and oxygenation in preterm infants. Nevertheless, there is a paucity of studies employing point-of-care ultrasound monitoring during this procedure. (2) In the present study, the integration of functional echocardiography (FE) and lung ultrasound facilitated a more comprehensive understanding and monitoring of patients by determining optimal opening and maintenance pressures, and the most appropriate timing for weaning. (3) FE confirmed that hemodynamics and myocardial function were preserved throughout the lung recruitment process. (4) Post-recruitment lung ultrasound score acts as a highly sensitive, independent predictive metric of mechanical ventilation weaning failure.Impact statements
Introduction
Mechanical ventilation is a cornerstone in managing neonatal respiratory distress syndrome (RDS), yet ventilator-induced lung injury (VILI) immediately after birth significantly drives neonatal morbidity and mortality. 1 To mitigate VILI (such as atelectotrauma and volutrauma), protocolized lung recruitment maneuvers (LRMs) can be applied using high-frequency oscillatory ventilation (HFOV), which maintains an “open-lung” state via ultra-small tidal volumes delivered around a constant continuous distending pressure. 2 Preclinical animal data, particularly utilizing premature lamb models of surfactant deficiency, confirm that systematic, stepwise adjustments in airway pressure successfully optimize functional residual capacity and protect the lung parenchyma from cyclical shearing injuries. 3 These animal models demonstrate that achieving homogeneous alveolar opening significantly reduces lung inflammatory markers compared to conventional volume-controlled strategies. 3
Historically, non-physiological strategies like sustained lung inflation (SLI), applying a prolonged, static high pressure immediately at birth, were introduced to establish functional residual capacity; however, large multi-center trials halted this practice after proving that SLI fails to reduce bronchopulmonary dysplasia and paradoxically increases early mortality due to focal volutrauma and acute circulatory arrest. 4 Consequently, modern open-lung ventilation has shifted away from static, unmonitored inflation maneuvers toward dynamic, stepwise LRMs nested within an active HFOV framework.
Because an LRM modifies intrathoracic pressure, it acts as a cardiorespiratory intervention that interacts dynamically with the immature transitional circulation across three distinct pathophysiological milestones: Phase 1 (Baseline Disease State): Widespread alveolar atelectasis induces localized hypoxia, triggering hypoxic pulmonary vasoconstriction and driving up pulmonary vascular resistance (PVR), which heavily increases right ventricular (RV) afterload. Phase 2 (Acute Intervention State): During active step-up pressure titration, elevated pressures present an acute mechanical risk, potentially compressing the vena cava and transiently compromising venous return and cardiac output. Phase 3 (Resolved Stabilization State): Once uniform recruitment is structurally established, the relief of atelectasis reverses hypoxic vasoconstriction and drops PVR, optimizing RV mechanical efficiency and enhancing left-heart filling, systemic blood flow, and cerebral perfusion.
Conventionally, neonatologists guide LRMs strictly by oxygenation responses (FiO2). 5 However, oxygenation markers can be delayed and unreflective of regional tissue mechanics. Bedside lung ultrasound (LU) has emerged as a reliable, radiation-free tool to monitor real-time, regional lung aeration kinetics and structural tissue recruitment directly at the bedside, 6 though its systematic combination with functional hemodynamic safety tracking during an HFOV-LRM has not been thoroughly established.
Study hypotheses
Primary hypothesis
In preterm infants requiring HFOV for moderate-to-severe RDS, a protocolized lung recruitment maneuver will achieve superior structural alveolar recruitment that is more accurately identified, tracked, and verified by serial 12-zone LUS across consecutive clinical phases than by standard operational oxygenation indices.
Secondary hypothesis
The lung recruitment maneuver will maintain a safe central hemodynamic profile, where functional echocardiography (FE) acts as a sensitive safety monitor for transient venous return compression during Phase 2 (acute intervention), and ultimately documents significant improvements in right ventricular efficiency (RV TD-MPI), and systemic blood flow (SVC flow), and during Phase 3 (resolved stabilization) due to the successful reduction of pulmonary vascular resistance.
Patients and methods
This a A prospective, single-arm, protocol-driven cohort study was conducted in the Neonatal Intensive Care Unit (NICU) at Alexandria University Maternity Hospital (AUMH) from July 2024 to January 2025. It focused on preterm infants with a gestational age of 32 0/7 to 36 6/7 weeks who exhibited moderate to severe respiratory distress and intubated within the first 24 h of life (n = 70). The flow chart of the patients is presented in (Figure 1). Infants with major congenital anomalies, such as congenital heart defects, congenital diaphragmatic hernia, or fetal hydrops, were excluded from the study, as these conditions could confound the assessment of lung recruitment and cardiac function. Additionally, patients who were on non-invasive ventilation during the first 24 h or intubated due to central depression or hemodynamic instability (hypotensive despite use of > 2 inotropes) were excluded. Flow chart of patients.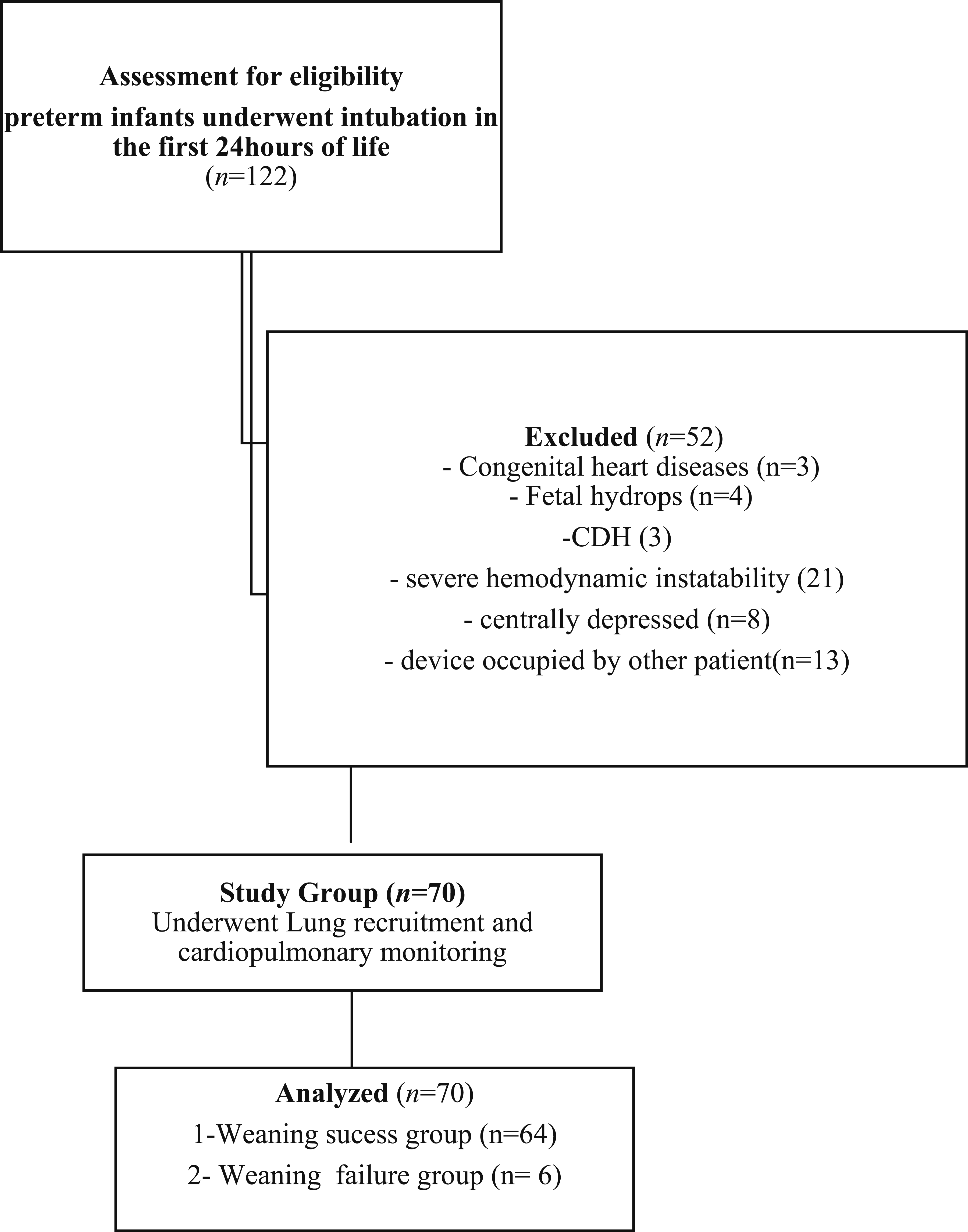
The study complied with the ethical standards established by the institutional review board and the 1964 Helsinki Declaration, together with its subsequent amendments. The ethics committee of Alexandria University approved the trial on 15/12/2022, with approval number 0201752, IRB no 00012098, and FWA no. 00018699. Informed consent was acquired from the patients’ guardians upon admission to the NICU.
The clinical objectives of this protocol were pre-specified as follows: • Primary Objective: The primary objective was to evaluate the physiological efficacy of an open-lung HFOV recruitment strategy in preterm infants with moderate-to-severe RDS, defined by improvements in systemic oxygenation parameters and a relative reduction in FiO2 requirements. • Secondary Objectives: The secondary objectives were twofold: first, to track real-time, regional structural lung tissue recruitment and aeration changes using a serial 12-zone LUS framework; second, to systematically evaluate cardiovascular safety, right ventricular mechanical efficiency (via tissue Doppler imaging), and central/cerebral perfusion stability using targeted functional echocardiography (FE) throughout the consecutive pressure transitions of the maneuver.
The LRM was initiated using HFOV, starting with a mean airway pressure (MAP) of 8 mbar, Frequency 15HZ, delta pressures of 18 mbar and FiO2 1. The procedure involved stepwise increases in MAP to open collapsed lung units, with MAP increased every 5–15 min by 2 mbar. FiO2 was reduced stepwise, maintaining oxygen saturation (SpO2) at 94–96%. The target FiO2 was <30%, or 40% if persistent pulmonary hypertension (PPHN) was confirmed by a tricuspid regurgitation (TR) gradient >40 mmHg, right to left duct shunting and/or right ventricular dilatation. The increase in MAP was halted when SpO2 could no longer be maintained by decreasing FiO2 to <0.30 (<0.40 if PPHN was present). At this juncture, the patient was considered to be at the opening pressure. Subsequently, MAP was gradually decreased every 5–15 min by 2 mbar until there was a persistent drop in SpO2 below 88%, at which point the MAP was termed the closing pressure. The reapplication of the opening pressures for 15 min and descends in a quicker pattern. Then, 2–4 mbar was added to closing pressure to have maintenance pressure. Surfactant was administered after application of LRM.
All patients were positioned supine. LUS was performed at three time points (phases): initially (Phase 1; baseline disease state), at the maintenance pressure (acute interventional pressure) to assess the degree of lung recruitment (Phase 2), and just before weaning to nasal continuous positive airway pressure (NCPAP), (Phase 3: post-recruitment stabilization). Lung aeration was assessed using the 12-zone 0–3 point scoring system as defined by the ESICM-ESPNIC 2025 international expert consensus 7 was utilized to evaluate patients, as well as the number of zones affected. FE was performed simultaneously to evaluate hemodynamic parameters, myocardial function, and pulmonary artery pressure. The following markers were used: SVCF, right ventricular myocardial performance index using tissue Doppler (TD-RV-MPI), TR gradient, patent ductus arteriosus (PDA), and patent foramen ovale (PFO), including shunt direction and size. Echocardiographic studies were conducted using the 12S-RS probe with a frequency range of 5–11 MHz of the machine model GE Vivid iq premium, WUXI, China (M, 2D, color Doppler modes, pulsed wave Doppler, and tissue Doppler). During scans, patients were sleeping or quietly resting in a supine position on a flat surface.
SVC-diameter was assessed through parasternal view with the beam angled to the right of the ascending aorta. Minimal and maximal diameters (in cm) were averaged from three cardiac cycles, using M-mode. Velocity Time Integral (VTI) was measured using low subcostal view, using PW Doppler. The mean velocity was averaged from five consecutive cardiac cycles. Calculation of the SVC-flow = (SVC VTI × (π × (mean SVC diameter2/4) × heart rate)/body weight. The resulting figure was expressed in mL/kg/min.8–10 Annular pulsed TDI recordings was obtained from an apical 4-chamber view to measure RV-MPI. TD RV MPI = IVCT + IVRT/RVET.
11
The echocardiographic scans were done at the three phases (time points) of the study, representing three distinct pathophysiological milestones: 1. Phase 1 (The Disease State/Baseline): The hemodynamic parameters captured here represent the baseline circulatory effects of severe, active RDS and generalized alveolar collapse, characterized by high pulmonary vascular resistance [evidenced by TR gradient] due to hypoxic pulmonary vasoconstriction) and its effect on right ventricle and COP represented by SVC flow. 2. Phase 2 (The Acute Intervention State): The parameters captured here represent the acute mechanical and cardiovascular effects of the LRM itself, where FE was utilized strictly as a safety tracking tool to monitor right ventricular (RV) function and systemic blood flow against increased intrathoracic working pressures. 3. Phase 3 (The Resolved Stabilization State): The parameters captured here represent the stabilized hemodynamics after the successful resolution of RDS and the establishment of uniform lung recruitment.
The imaging of all patients were done by single operator experienced in neonatal echocardiography >5 years. All images of LUS and echocardiography were revised by consultant cardiologist and consultant neonatologist experienced in point of care ultrasound to minimize bias.
Clinical parameters such as oxygen saturation index (OSI), inotropic support, and blood gas measurements (e.g., pH, PaO2, PaCO2, base excess) were regularly recorded. Chest X-rays were taken alongside LUS to correlate findings and assess lung aeration. Pneumothorax, pulmonary hemorrhage and intraventricular hemorrhages were documented.
Statistical methods
To ensure the study is adequately powered, a sample size calculation was performed for a single-arm, pre-post interventional design using a paired Student's t-test framework, with the primary outcome defined as the improvement in the Oxygenation Saturation Index (OSI) following lung ultrasound and echocardiography-guided lung recruitment maneuvers. Based on clinical parameters established in the literature for infants managed with an ultrasound-targeted recruitment protocol (the LUSTR cohort), 6 the baseline starting OSI was estimated at 16.9 +/- 8.1, which was expected to improve significantly to a final post-recruitment mean of 8.8 +/- 6.8, yielding an expected mean clinical delta of 8.2 points with a standard deviation of the change score of 6.8 To detect this physiological effect size with 90% statistical power, a minimum sample size of 8 infants is required. To ensure a robust data distribution for parametric testing and to accommodate an anticipated 15% to 20% sample attrition or drop-out rate due to acute clinical complications or technical scanning limitations, a final cohort of 10 to 12 preterm infants will be targeted for prospective enrollment. Expanded final enrollment to 70 infants based on your unit’s standard clinical admission rate over a 6-month period.
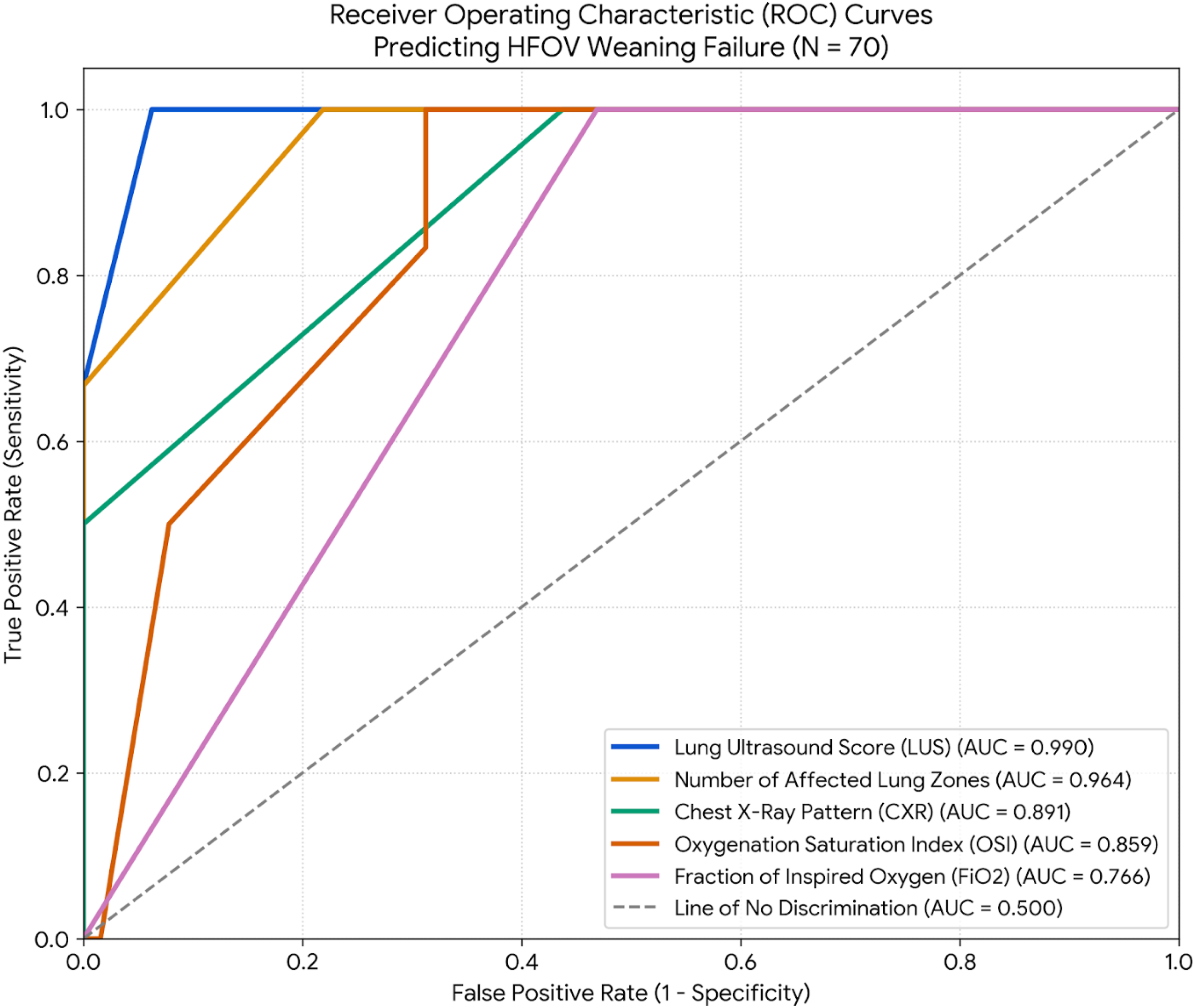
Data were fed into a computer and analyzed with IBM SPSS software version 26.0. Qualitative data were presented as numbers and percentages. The Kolmogorov-Smirnov test checked the normality of distribution. Quantitative data were described using the range (minimum and maximum), mean, standard deviation, median, and interquartile range (IQR). The significance of the results was assessed at the 5% level. ANOVA with repeated measures and the Friedman test were applied to normally and abnormally distributed variables, respectively. Pairwise comparisons were conducted using the Post Hoc Test (Bonferroni adjusted). Spearman and Pearson coefficients were employed for correlations between abnormally and normally distributed variables, respectively. To evaluate the clinical magnitude of cardiorespiratory, ventilatory, and hemodynamic changes across consecutive protocol phases (Phase 1 vs. Phase 2; Phase 2 vs. Phase 3), paired Cohen’s d effect sizes were calculated. Effect sizes were interpreted using standard clinical thresholds: trivial (<0.20), small (0.20–0.49), moderate (0.50–0.79), and large (≥0.80). Receiver Operating Characteristic (ROC) curve analysis was executed to evaluate the performance of pre-weaning (Phase 3) parameters, including LUS, number of affected zones, CXR grading, OSI, and FiO2 in discriminating HFOV weaning failure from successful weaning. Sensitivity, specificity, positive predictive value (PPV), and negative predictive value (NPV) were calculated.
Finally, patients were categorized into groups based on successful or failed weaning. Univariate screening was executed across all clinical and hemodynamic parameters to identify unadjusted risk factors for HFOV weaning failure. Relevant chronological covariates, including maternal antenatal steroids, active neonatal sepsis, pre-weaning global Lung LUS >7.0, and Phase 3 OSI, were then entered into a multivariate logistic regression model. To preserve model reliability against cardiorespiratory multicollinearity and zero-cell mathematical separation constraints, parameters were stabilized using a Haldane-Anscombe exact continuity correction framework and cross-validated via Fisher’s Exact test at an alpha level of 0.05. Inotropic circulatory support was intentionally retained in the final multivariate logistic regression model, despite its lack of statistical significance in univariate screening, to serve as a vital baseline cardiorespiratory covariate. This demonstrates that the predictive power of the pre-weaning global LUS is a true reflection of primary pulmonary structural derecruitment, remaining completely independent of the infant’s underlying hemodynamic or circulatory support status.
Results
During the study period 122 infants with gestational age between 32 0/7 and 36 6/7 weeks were admitted to NICU of Alexandria University hospital and intubated in the first 4 h after birth due to pulmonary causes. Seventy preterm infants with moderate to severe RDS were eligible for the study and had FiO2 guided LRM, as well as cardiopulmonary monitoring using LUS and FE, Figure 1.
Descriptive analysis of socio-demographic data, clinical characteristics and fate of studied patients.
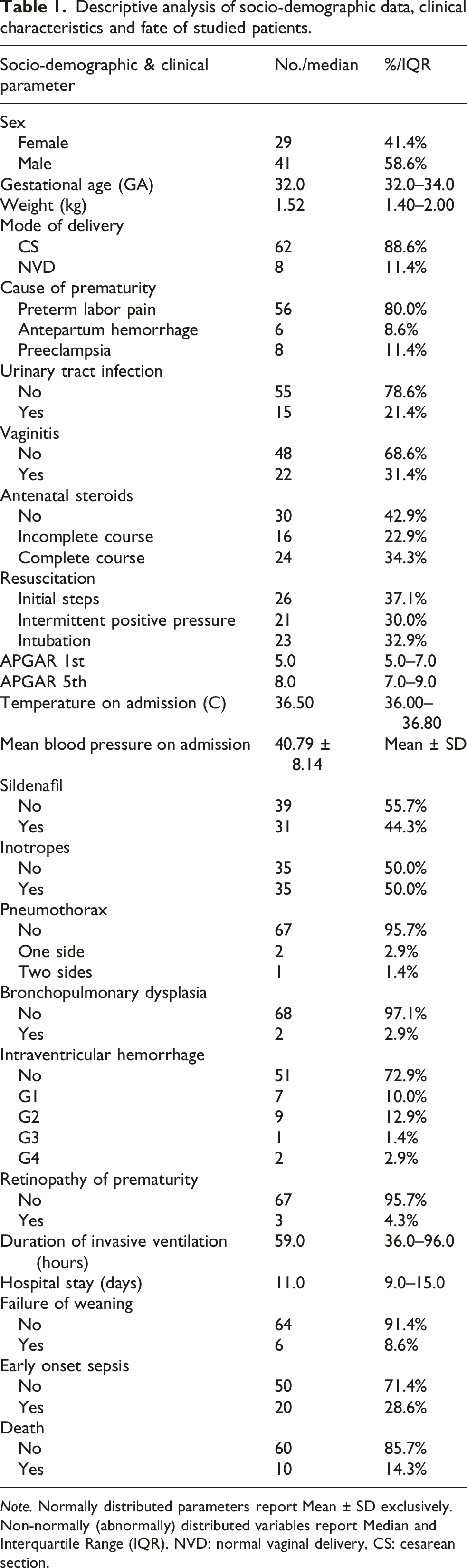
Note. Normally distributed parameters report Mean ± SD exclusively. Non-normally (abnormally) distributed variables report Median and Interquartile Range (IQR). NVD: normal vaginal delivery, CS: cesarean section.
The first Apgar scores ranged from 3.0 to 7.0, with a mean of 5.41 ± 1.34, and the fifth-minute Apgar scores ranged from 5.0 to 9.0, with a mean of 7.70 ± 1.16. Pneumothorax occurred in three patients; one case developed post-weaning following reintubation, while the remaining two cases occurred and resolved prior to the weaning process. The average duration of mechanical ventilation was 74.11 ± 52.58 h, with a mean hospital stay of 13.17 ± 9.19 days. The mortality rate was 14.3%, with sepsis being the primary cause of death.
STable 1a and STable 1b demonstrate ventilatory settings (MAP, delta pressure and frequency, as well as chest X-ray findings, LUS, number of affected zones, OSI at the three time points of the study, initially at the opening pressure and pre-weaning. Chest X-rays and LUS assessments showed significant improvements in lung aeration over time.
S-Table 1c shows distribution of hemodynamic parameters and right ventricular global function at the three-time phases of the study. FiO2 guided LRM using HFOV led to significant improvements in various clinical parameters over time.
Comprehensive paired Cohen’s d effect size matrix across phases of the study regarding ventilatory settings, oxygenation parameters, lung ultrasound score, and echocardiographic parameters (N = 70).
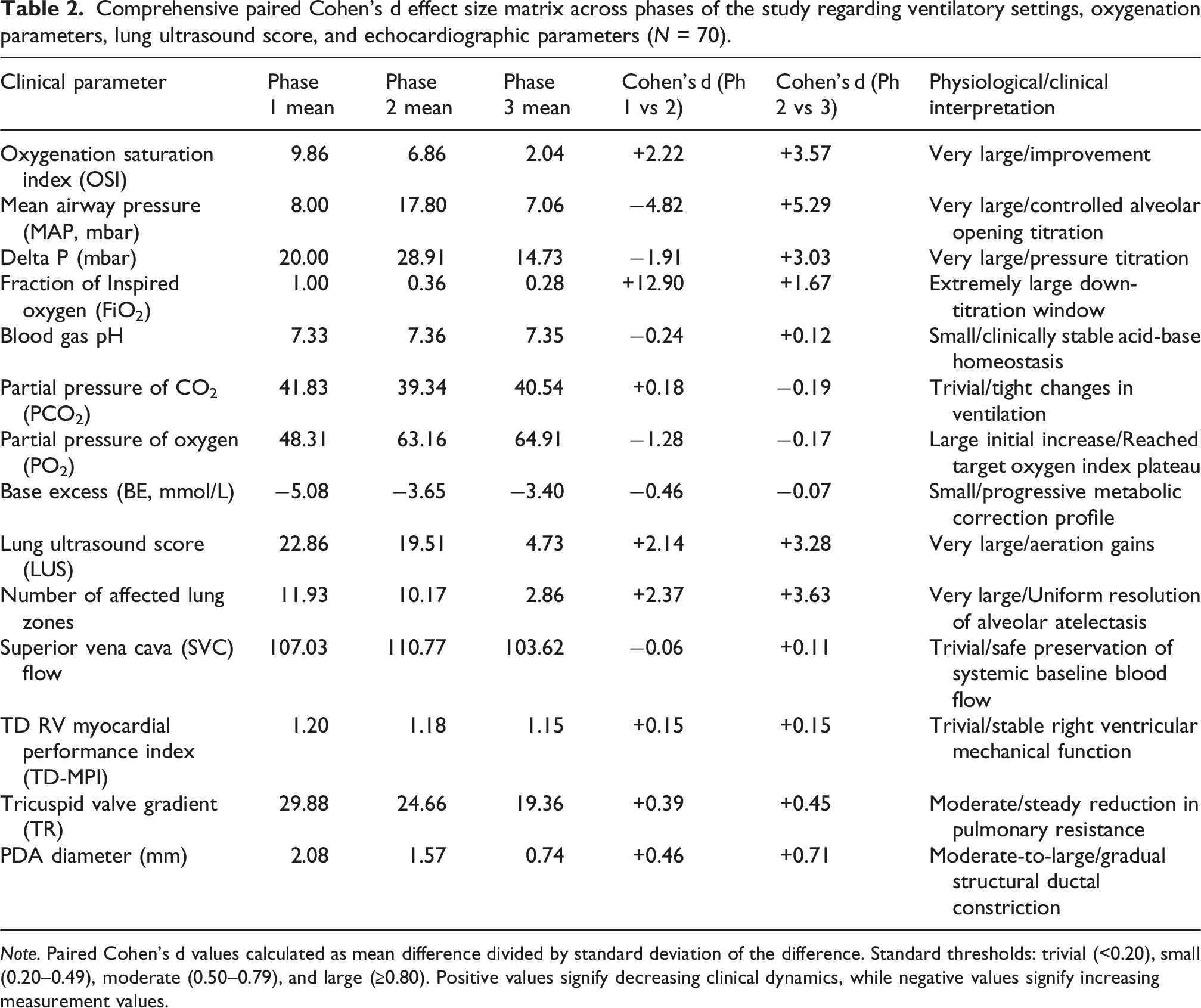
Note. Paired Cohen’s d values calculated as mean difference divided by standard deviation of the difference. Standard thresholds: trivial (<0.20), small (0.20–0.49), moderate (0.50–0.79), and large (≥0.80). Positive values signify decreasing clinical dynamics, while negative values signify increasing measurement values.
ROC curve parameters and predictive indices for HFOV weaning failure after LRM.
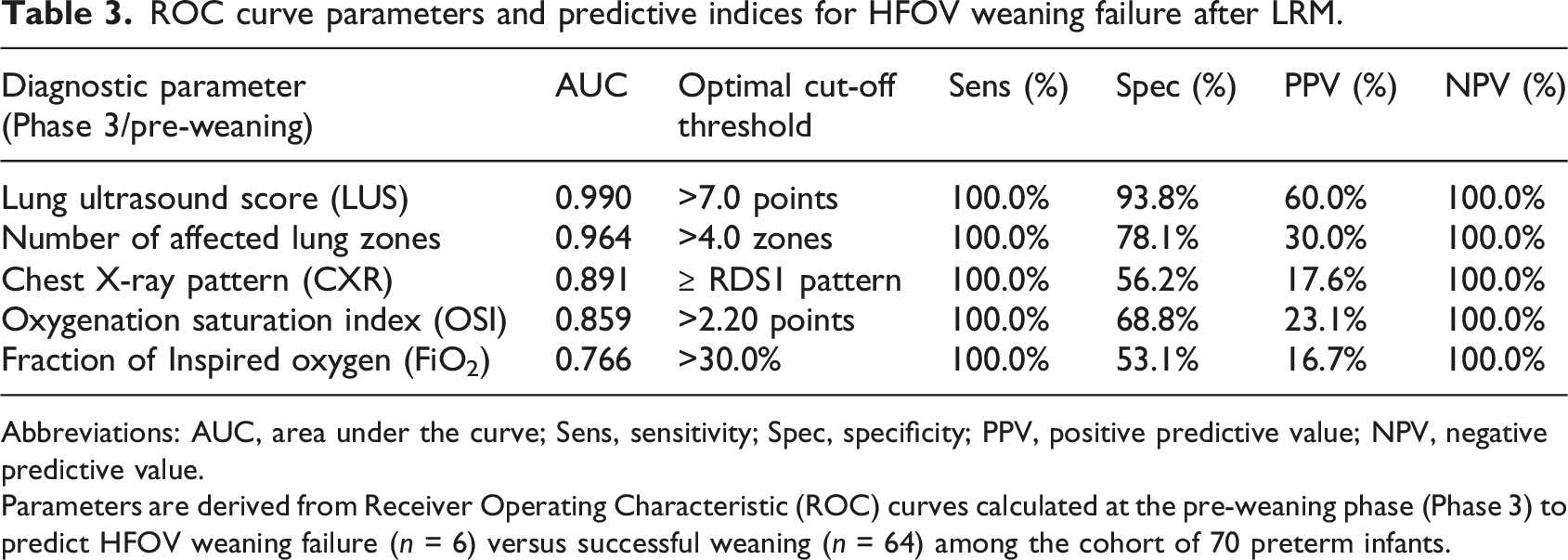
Abbreviations: AUC, area under the curve; Sens, sensitivity; Spec, specificity; PPV, positive predictive value; NPV, negative predictive value.
Parameters are derived from Receiver Operating Characteristic (ROC) curves calculated at the pre-weaning phase (Phase 3) to predict HFOV weaning failure (n = 6) versus successful weaning (n = 64) among the cohort of 70 preterm infants.
ROC curve parameters and predictive indices for HFOV weaning failure after LRM.
Multivariate logistic regression analysis for the parameters affecting weaning failure in studied group.
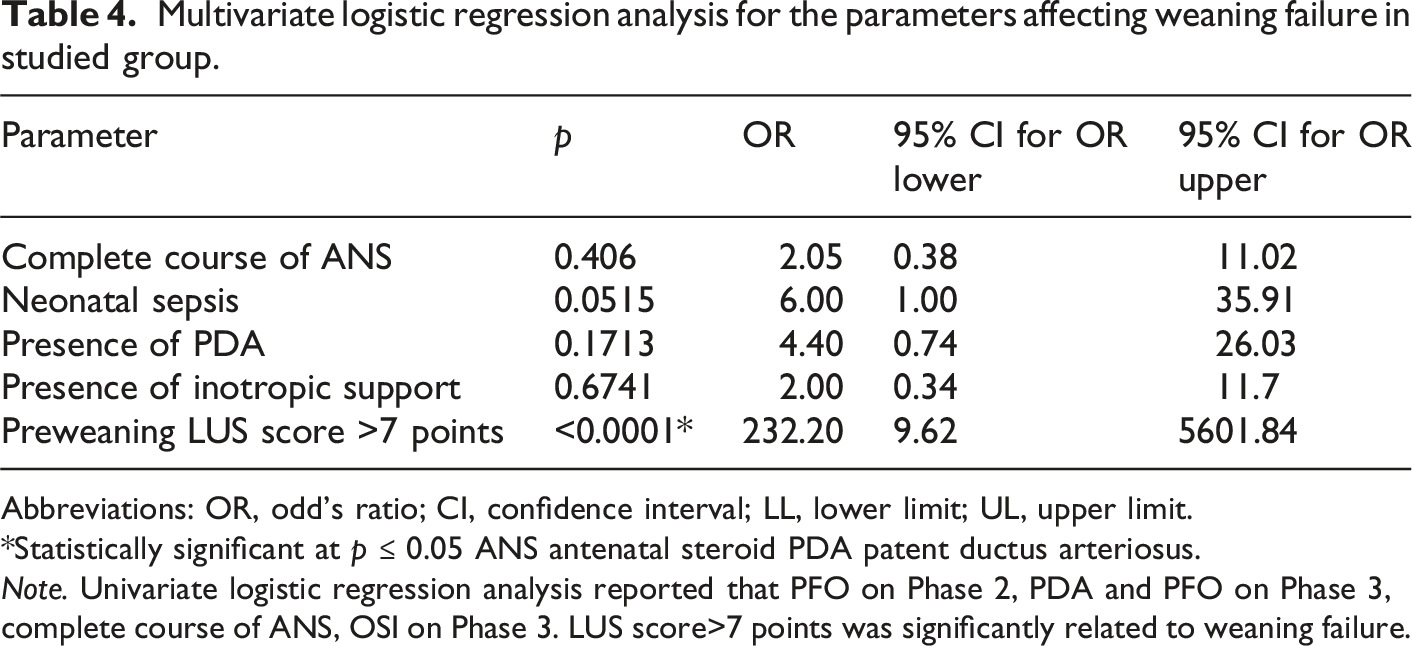
Abbreviations: OR, odd’s ratio; CI, confidence interval; LL, lower limit; UL, upper limit.
*Statistically significant at p ≤ 0.05 ANS antenatal steroid PDA patent ductus arteriosus.
Note. Univariate logistic regression analysis reported that PFO on Phase 2, PDA and PFO on Phase 3, complete course of ANS, OSI on Phase 3. LUS score>7 points was significantly related to weaning failure.
Discussion
Many neonatal diseases have cardiopulmonary interactions like RDS, BPD, and meconium aspiration syndrome.12,13 In the current research, cardiopulmonary interaction is anticipated both in lung pathology, like RDS and intervention, such as LRM. LRM enhances oxygenation and lung compliance, which in turn reduces the duration of invasive ventilation and the associated oxidative stress injury. The vulnerable lung, heart and hemodynamics in premature might be adversely affected by extra pressures applied acutely to recruited premature lung. Here comes the crucial role of point of care ultrasound using both FE to assess the cardiac function and hemodynamic changes, as well as LUS to aid in determining the ideal optimal opening and maintenance, pre-weaning pressures. Initial use of LUS in premature solely might be fallacious because the condition is confounded by both RDS and extensively retained lung fluids. In the current study, we implemented FiO2-guided LRM to recruit the lung, identified the optimal maintenance and pre-weaning pressures, and utilized LUS to find the corresponding LUS at those pressures. Additionally, cardiac function and hemodynamics were monitored with FE during the LRM process.
The multi-phase functional echocardiography (FE) and tissue Doppler data map a distinct three-stage cardiopulmonary trajectory during lung recruitment. In Phase 1 (Baseline), the hemodynamic profile reflects the raw pathophysiological burden of severe RDS, where generalized alveolar collapse drives up pulmonary vascular resistance (PVR) via hypoxic pulmonary vasoconstriction. In Phase 2 (Acute Intervention), metrics represent the immediate mechanical impact of the lung recruitment maneuver (LRM) itself; during this active pressure titration, FE serves strictly as a safety monitor to screen for transient reductions in venous return or right-heart compression from elevated mean airway pressures. Finally, in Phase 3 (Resolved Stabilization), the parameters capture the stabilized circulatory status following successful recruitment and subsequent RDS improvement. Once stable, ultrasound-verified alveolar expansion is secured, the relief of atelectasis reverses hypoxic vasoconstriction, drastically reducing right ventricular (RV) afterload. This optimizes RV mechanical efficiency, enhances left-heart filling, and ultimately improves systemic blood flow and cerebral perfusion metrics.
The obtained results from the current study showed that the use of FiO2 guided LRM using HFOV resulted in significant improvements in oxygenation, as indicated by the reduction in the FiO2 and the increased lung aeration seen on lung ultrasound. The mean FiO2 dropped from 100% in the initial phase to 35.86 ± 4.96% (at the maintenance pressure phase) and 27.57 ± 2.52% in the pre-weaning phases. In addition, LUS score improved along the three phases of study starting from median values 24 (initially), to 20 (at the opening pressure), then to 4 (pre-weaning). This suggests that lung recruitment using HFOV can successfully restore alveolar ventilation and improve gas exchange, reducing the need for high oxygen concentrations. At these three-time points hemodynamics did not significantly change.
This result is consistent with the findings of Fan et al. 14 who conducted a systematic review on recruitment maneuvers in patients with acute lung injury and RDS. Their study showed that LRMs, including HFOV, are effective in improving oxygenation and lung compliance in neonates with respiratory distress. Similarly, Miedema et al. 15 found that HFOV in preterm infants led to better oxygenation and more stable lung volumes by reducing intrapulmonary shunting, which is a hallmark of RDS.
However, contrasting results were reported by Gattinoni et al. 16 who highlighted that while HFOV may improve oxygenation, its long-term benefits remain unclear. Their study indicated that HFOV could lead to overdistension of the lungs in some cases, contributing to VALI. The current study carefully monitored FiO2 and pressure settings to avoid such complications, which may explain why the study did not observe such adverse outcomes. This difference in findings could be attributed to variations in study design, patient selection, and ventilator settings. In the current study, a gradual weaning from FiO2 was employed based on LUS and hemodynamic monitoring, which likely contributed to the better outcomes.
The current study demonstrated that LUS was a valuable tool for monitoring lung aeration, with a significant reduction in the number of affected lung zones over the three phases of ventilation. Initially, the mean number of non-aerated zones was 11.93 ± 0.26, which decreased to 4.73 ± 5.05 by the third phase. This increase in lung aeration corresponds with the reduction in FiO2, confirming the successful recruitment of lung units. The results also revealed a significant correlation between LUS and FiO2, supporting LUS as a reliable tool for monitoring lung recruitment.
These findings align with Lichtenstein and Mauriat 17 who reported that LUS provides real-time, non-invasive feedback on lung aeration and can be used effectively to monitor lung recruitment in critically ill neonates. Their work demonstrated that LUS could detect lung consolidation, atelectasis, and recruitment in neonates, which are crucial for adjusting ventilatory strategies.
On the other hand, Corradi et al. 18 suggested that although LUS is a promising tool for lung monitoring, its utility in assessing lung recruitment is still debated due to variability in interpretation and difficulty in visualizing deeper lung areas in certain patients. The current study minimized this limitation by employing a standardized ultrasound protocol and ensuring adequate visualization of lung zones. This methodological consistency could explain the more reliable results observed in the current study compared to previous studies that faced challenges with LUS interpretation in neonates.
The use of FE in this study revealed significant changes in hemodynamic parameters, such as systolic pulmonary artery pressure (PAP) and ductal shunting. PAP decreased significantly from 29.88 ± 13.43 mmHg in the first phase to 19.36 ± 11.53 mmHg in the third phase, while the PDA shunt flow decreased over time, indicating improved pulmonary circulation. These findings suggest that monitoring hemodynamic changes during lung recruitment is essential for optimizing treatment and avoiding hemodynamic instability.
These results are consistent with Tissot and Singh, 19 who emphasized the importance of FE in assessing right ventricular function and pulmonary circulation in critically ill neonates, especially those with RDS. Their study highlighted that right ventricular dysfunction is common in infants with severe RDS, and monitoring through FE can help guide therapeutic interventions, such as fluid management and inotropic support. However, FE in neonates remains underutilized due to the need for specialized training and the complexity of interpretation. 20
SVC Flow in neonates serves as an indicator of both cardiac output (COP) and cerebral blood flow, as described by Evans and Kluckow. 20 The utilization of SVC flow in the monitoring of preterm infants is expanding within neonatal intensive care units (NICUs).8,10 The present study demonstrated a non-significant difference in SVC flow across the three scan points, indicating stable hemodynamics throughout all stages of lung recruitment.
The study found a strong correlation between chest ultrasound scores and clinical parameters such as FiO2 and OSI, with statistically significant associations observed throughout the study. This supports the hypothesis that chest ultrasound can be used to guide ventilator settings and oxygenation strategies in real time, providing valuable information on lung aeration and recruitment.
This finding is consistent with Chioma et al. 21 who developed a novel protocol for lung ultrasound-targeted recruitment (LUSTR), which showed that ultrasound scores can effectively guide ventilatory management and improve oxygenation in neonates with RDS. The study demonstrated that incorporating LUS into clinical decision-making can significantly optimize the recruitment strategy and reduce the need for prolonged high oxygen concentrations.
In contrast, Liu et al. 22 highlighted that while LUS can provide useful information on lung aeration, its predictive value for clinical outcomes, such as mortality or long-term lung function, remains unclear. The current study did not assess long-term outcomes, but the observed correlation between ultrasound findings and short-term clinical improvements suggests that LUS is a reliable tool for monitoring and guiding therapy in the acute phase.
Upon initiation of high-frequency oscillatory ventilation (HFOV), an open-lung strategy was systematically implemented via a protocolized, stepwise lung recruitment maneuver (LRM) prior to exogenous surfactant delivery. While immediate surfactant instillation upon intubation represents standard conventional care for neonatal RDS, this study utilized a sequential paradigm where surfactant was intentionally administered immediately after the completion of the LRM. 6
Physiologically, executing the LRM first establishes a uniform functional residual capacity (FRC) across the lung parenchyma, which avoids the patchy, non-uniform drug distribution and subsequent ventilation-perfusion mismatches frequently encountered when instilling surfactant directly into collapsed, atelectatic airways. Furthermore, recruiting the lung prior to delivery mitigates the high physical shear stress forces and mechanical inactivation that exogenous surfactant is subjected to when high inflation pressures are subsequently used to break alveolar surface tension. Opening the lung first allows the exogenous surfactant to immediately stabilize patent alveoli at lower, safer maintenance pressures, minimizing the risk of ventilator-induced lung injury (VILI). 6
This sequential recruit-first approach directly aligns with the validated clinical framework of the landmark multicenter IN-REC-SUR-E (Intubate-Recruit-Surfactant-Extubate) randomized controlled trial. This trial demonstrated that protocolized HFOV lung recruitment immediately preceding surfactant administration significantly reduces mechanical ventilation dependency within the first 72 h of life in preterm neonates without increasing adverse acute or long-term neurodevelopmental and respiratory outcomes.5,21
The results of this study are in agreement with Cucerea et al. 23 who found that early and effective management of respiratory distress syndrome, including the use of surfactant and mechanical ventilation strategies like HFOV, significantly reduced the incidence of severe complications such as BPD and ROP. Similarly, Corsini et al. 24 noted that the use of optimal ventilation strategies, guided by LUS, can reduce the risk of adverse outcomes in preterm infants. These findings indicate that HFOV, in conjunction with real-time monitoring of lung recruitment, can improve the clinical outcomes of preterm infants with severe RDS.
The clinical outcomes of the study showed that the majority of infants (91.4%) did not experience failure in the treatment protocol. However, the mortality rate of 14.3% observed in this study is higher than that reported in some other studies, with sepsis being the primary cause of death. For instance, Abbas et al. 25 reported a lower mortality rate of 5% in preterm infants with RDS who received similar interventions. This difference could be due to the varying severity of RDS in the studied populations, differences in the timing of intervention, or regional variations in healthcare resources. The current study was conducted in a single-center setting with a smaller sample size, which may limit the generalizability of the findings compared to multicenter studies.
In this study, three patients experienced pneumothorax: two were in the weaning success group, and one was in the weaning failure group. The patients in the weaning success group developed pneumothorax during the pre-weaning period, characterized by low LUS scores. The pneumothorax was effectively drained, leading to successful weaning. Conversely, the patient in the weaning failure group developed pneumothorax following reintubation. This patient, born at 34 weeks of gestation, had LUS score of 20, 22, and 18 at initial assessment, opening pressure, and pre-weaning, respectively. Despite a high pre-weaning LUS score, the patient was weaned to CPAP due to an FiO2 of less than 0.3. However, reintubation occurred 24 h post-weaning, resulting in bilateral pneumothorax.
Notably, one of the patients studied, a 32-weeker, initially presented with a LUS score of 24, which subsequently increased to 28 at the opening pressure. Despite a low FiO2, the pre-weaning score further escalated to 32. This patient was confirmed to have culture-proven sepsis, which may have adversely impacted lung condition. Additionally, this patient experienced weaning failure, further corroborating the role of LUS in predicting weaning failure.
In conclusion, this study validates the effectiveness of using FiO2-guided LRM with HFOV in treating patients with RDS who are between 32 and 36 weeks of gestational age. The integration of LUS and FE has shown that FiO2-guided LRM can improve lung aeration while maintaining hemodynamic stability and myocardial function (safety) in moderate and late preterm infants with moderate-to-severe RDS. Additionally, this research highlights the predictive capability of pre-weaning LUS in this age group, as it is notably higher in the weaning failure group compared to the weaning success group.
A limitation of this study is the absence of LUS-guided LRM application; nonetheless, we posit that the current findings may offer cutoff values for LUS score that could aid in determining the precise opening pressure. Gestational age is indicative of lung development status, affecting lung fluid content, gas exchange efficiency, RDS severity, hemodynamics, and relative myocardial dysfunction in preterm infants of lower gestational age, which may constrain the generalizability of the results. This approach might offer a viable solution for low-resource settings, allowing shorter duration of ventilation, unavailability of surfactant and nitric oxide (iNO) in some areas. Another limitation is the absence of inhaled iNO in the current research setting. Consequently, alternative treatments such as sildenafil are employed for the management of persistent pulmonary hypertension. In this study, we utilized two distinct devices, each equipped with a specific probe: a linear probe for conducting LUS and an echo probe for performing focused FE. Furthermore, the single-center nature of the study constitutes an additional limitation.
Supplemental material
Suppplemental Material - Integrated echocardiography and lung ultrasound assessment of lung recruitment in preterm infants using high frequency ventilation: A prospective, single-arm, protocol-driven cohort study
Suppplemental Material for Integrated echocardiography and lung ultrasound assessment of lung recruitment in preterm infants using high frequency ventilation: A prospective, single-arm, protocol-driven cohort study by Marwa Mohammed Farag, Mohamed Hazem Gouda, Aly Mohamed Abdel-Mohsen, Mohamed Hany Ahmed in Journal of Neonatal-Perinatal Medicine
Footnotes
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Clinical trial registration
This study was registered on clinical trial.gov with ID number: NCT05726578 on February 3, 2023 with URL: ![]() .
.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.