
Abstract
Background
To assess the feasibility and efficacy of Vayu continuous positive airway pressure (vCPAP) for preterm and term infants with respiratory distress in the delivery room.
Methods
Feasibility study of infants of any gestational age presenting with respiratory distress defined as a Silverman–Anderson Score (SAS) ≥4 in the delivery room, who were started on vCPAP prior to transfer to the NICU and maintained during transport. Efficacy was assessed by comparing SAS, FiO2, and SpO2 before initiation of vCPAP, 1 min after initiation, and at the time of NICU admission. Secondary outcomes were feasibility accessed by a survey applied to all health care professionals (HCP), and safety (pneumothorax or clinical deterioration). Descriptive analysis and parametric and non-parametric tests were applied (alpha of 5%).
Results
10 preterm and 10 term infants were initially enrolled, but one term was excluded because of a protocol deviation. The median gestational age was 37.6 ± 1.1 weeks for preterm and 34.2 ± 1.6 weeks for term infants. A significant improvement in SAS from five prior to vCPAP initiation (IQR 4–6) to three 1 min after initiation (IQR 2–4, p < 0.01), to two on NICU admission (IQR 1–3, p < 0.001). No significant differences in FiO2, SpO2, or CPAP pressure over these time periods were identified. Among HCP, ease of use and satisfaction were highlighted. No complications were observed.
Conclusion
In neonates with respiratory distress after birth, a clinical improvement was noted after initiation of vCPAP in the DR and during transport to the NICU.
Keywords
Introduction
Neonatal respiratory distress accounts for 30% to 40% of all admissions to the Neonatal Intensive Care Unit (NICU) globally. 1 In premature infants (<37 weeks of gestational age), several randomized clinical trials have demonstrated that initiation of nasal continuous positive airway pressure (CPAP) in the delivery room was associated with decreased duration of mechanical ventilation, mortality, and the combined outcome of death/bronchopulmonary dysplasia (BPD). 2 Initiation of CPAP in the delivery room and during transport to the NICU maintains functional residual capacity and pulmonary reserve resulting in less need for intubation and mechanical ventilation. 3 However, the availability of CPAP systems that can be used in the DR and during transport in low- and middle-income countries (LMICs) is small. 4 CPAP systems require electricity, compressed air, oxygen blenders, heaters, and humidifiers making them expensive to maintain and impractical for use in much of the world.
The Vayu bCPAP (Vayu Global Health Innovations, Boston, MA, USA) is a low-cost system that does not require electricity or compressed air. 5 It does not have a heater, and humidification is provided by the use of an extra water chamber. The oxygen is mixed with room air by using a venturi, allowing provision of oxygen (O2) concentrations between 30% and 100%. Therefore, vCPAP can be easily placed in the DR and used during transport to the NICU. The objective of this pilot study was to assess the feasibility of vCPAP in infants with respiratory distress immediately after birth and during transport to the NICU.
Methods
Study design
Site
This feasibility study was performed at the Santa Casa de São Paulo level III NICU, between November 2022 and March 2023. In the delivery room, as the standard of care, CPAP is provided with a T-piece device and face masks, which is also used for transportation to the NICU. During the study, the unit had 4 manual T-piece devices (Babypuff®) and one bubble CPAP (BabyPAP; FANEM, SP, Brazil). The institution follows a CPAP protocol without specifications on which type of CPAP to use. Therefore, there were no previous experience with the Vayu system. Patients were enrolled, and as soon as possible, the family was informed of the study and advised of the option to withdraw or consent for continued participation. 6 The study, including the deferred consent process, was approved by the ethics board of the Institution. Written consent was obtained. No families later refused or withdrew from the study.
Inclusion and exclusion criteria
Preterm (<37 weeks) and/or term (≥37 weeks) infants presenting with respiratory distress immediately after birth, with Silverman–Anderson Score ≥4. Infants with major congenital malformations, or extremely low birth weight infants (<1000 g) were excluded of this study.
Outcomes
The primary outcome was feasibility of the vCPAP system use. Feasibility was determined by the ability to initiate vCPAP in the DR, the time between the decision to initiate CPAP and when the device was effectively applied and functioning, and responses to a specific survey developed for the study. Secondary outcomes were efficacy by comparing changes on the Silverman–Anderson Score (SAS), fraction of inspired oxygen (FiO2), oxygen saturation (SpO2), and CPAP pressures between three specific points: before vCPAP initiation, 1 min after starting vCPAP, and at the time of NICU admission and safety defined by the occurrence of pneumothorax diagnosed at admission by CXR or sudden clinical deterioration (SpO2 <80% and/or HR <100 bpm) occurring only while on the vCPAP.
Training on Vayu CPAP
Prior to study initiation, training on the system was provided in person, by the vCPAP professional team, to 10 neonatologists and nine respiratory therapists (RT). Each session lasted 3 h and covered several technical and practical aspects of the device and its components. It included training in system assembling and installation, use in the DR and during transport, monitoring, cleaning, and troubleshooting.
Procedures
Delivery room stabilization
The delivery room team consisted of two neonatologists, one RT, and one NICU nurse, all trained on neonatal resuscitation. After birth, all interventions followed the Neonatal Resuscitation Program Guidelines.7,8 If needed, positive pressure ventilation was provided by using a T-piece device (BabyPuff®, FANEM, SP, Brazil) and FiO2 adjusted to keep the SpO2 within the NRP target range. After the decision to initiate an infant on vCPAP was taken by the resuscitation team in infants with SAS ≥4 were considered for CPAP initiation; once the decision was made the vCPAP was assembled by the RT and placed on the infant. The duration in minutes between the decision to initiate CPAP and the successful application of the vCPAP device was recorded.
Transport to the NICU
Transport was conducted by the same team attending the DR, and FiO2 levels were adjusted to maintain the SpO2 target. Upon admission to the NICU, patients still requiring vCPAP support were transitioned to the unit’s CPAP system.
Survey
To elicit feedback from health care providers (HCP), a 14-question survey was developed (see Appendix A). The survey consisted of 14 questions in a numerical 4-point Likert scale format. It included first and/or previous experiences with vCPAP, and general satisfaction when compared to other non-invasive respiratory devices. Regarding the DR context, there were questions about ease of use for assembling and placing the device on the newborn, verifying expiratory pressure and FiO2, and dynamic adjustments according to patient needs. About transport, questions ranged from ease of use when moving from the DR resuscitation unit to the transport incubator, and from transport to the NICU bed. SpO2 stability was also assessed in this step of the survey. The final question was about perceived clinical response and changes on SAS. The survey was administered to all HCP who participated in training and data collection. The full survey is provided as supplemental material in Appendix A.
Sample size and data analysis
This pilot study was not powered a priori, as its primary aim was feasibility. With a final sample of 19 infants and a large observed within-subject effect (median reduction in Silverman–Anderson Score from 5 to 2), post-hoc estimation suggests a high statistical power (>85%) for detecting the observed change. These findings support the presence of a strong physiological signal and provide effect size estimates to inform the design of adequately powered future trials. Descriptive analysis was performed for maternal and neonatal characteristics using frequency and normal distribution analyses.
The Student’s t-test was used to compare continuous data and the Wilcoxon rank sum test to determine differences in the medians using SAS. A significance level of p < 0.05 was used for all analyses. The Wilcoxon Rank Sum Test was used to determine differences in the medians [IQR] of SAS, FiO2, SpO2, and vCPAP pressures between baseline, 1 min after initiation, and at NICU admission. A p-value <0.05 was considered statistically different.
Results
Population demographics and clinical characteristics.
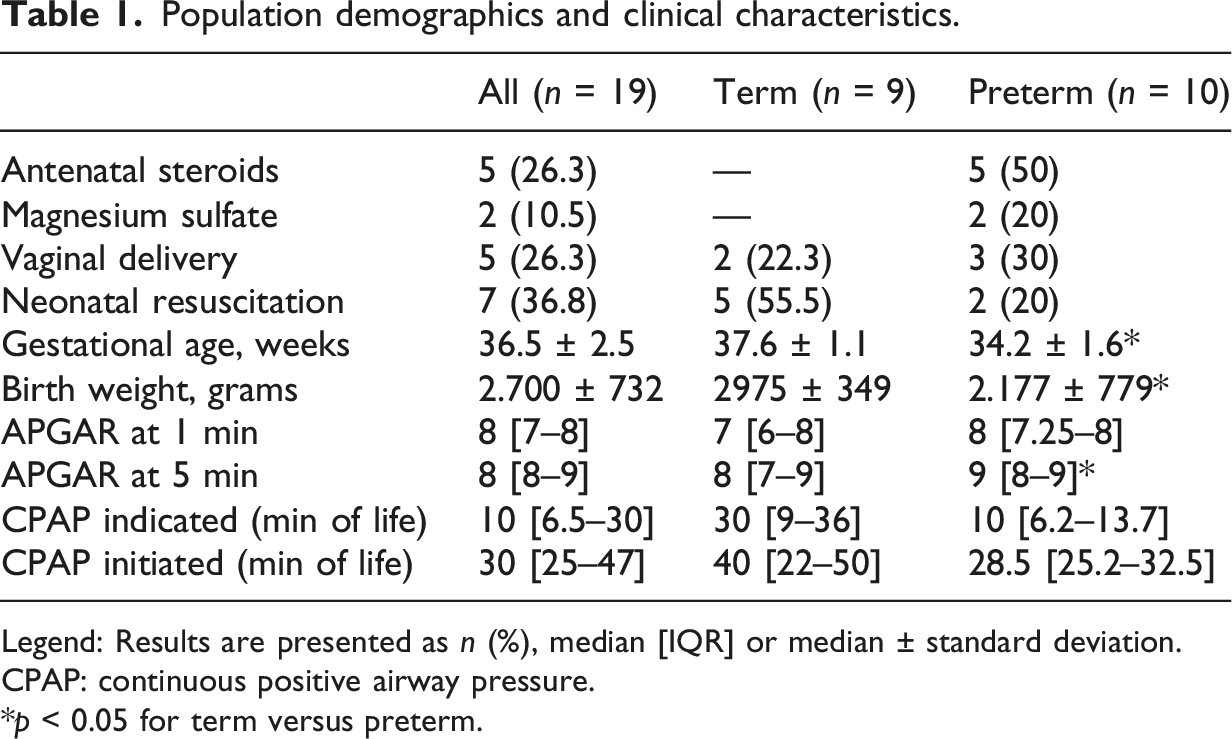
Legend: Results are presented as n (%), median [IQR] or median ± standard deviation.
CPAP: continuous positive airway pressure.
*p < 0.05 for term versus preterm.
Efficacy
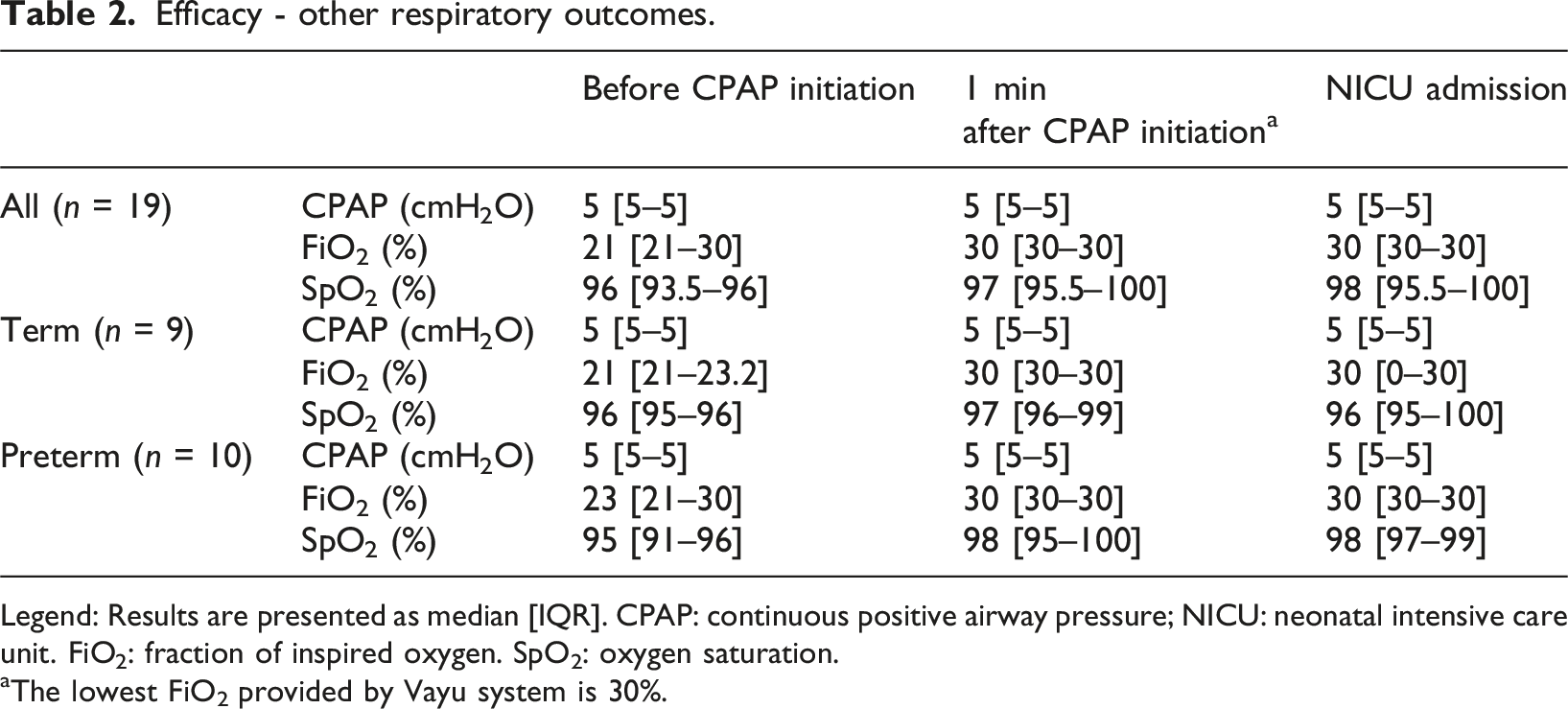
As shown in Figure 1, the SAS had a significant decrease from five (IQR 4–6) prior to vCPAP initiation to three (IQR 2–4) 1 min after initiation (p = 0.002). There was a further decrease to a SAS of two (IQR 1–3) at the time of NICU admission (p < 0.001). No differences were observed for FiO2, SpO2, or vCPAP pressure (Table 2). Efficacy—the Silverman–Anderson score trajectory from the DR to the NICU. Legend: CPAP: continuous positive airway pressure; NICU: neonatal intensive care unit. Each filled circle is a patient score. Results are presented as median and IQR; *p = 0.002; **p < 0.001; ***p = 0.006. Efficacy - other respiratory outcomes. Legend: Results are presented as median [IQR]. CPAP: continuous positive airway pressure; NICU: neonatal intensive care unit. FiO2: fraction of inspired oxygen. SpO2: oxygen saturation. aThe lowest FiO2 provided by Vayu system is 30%.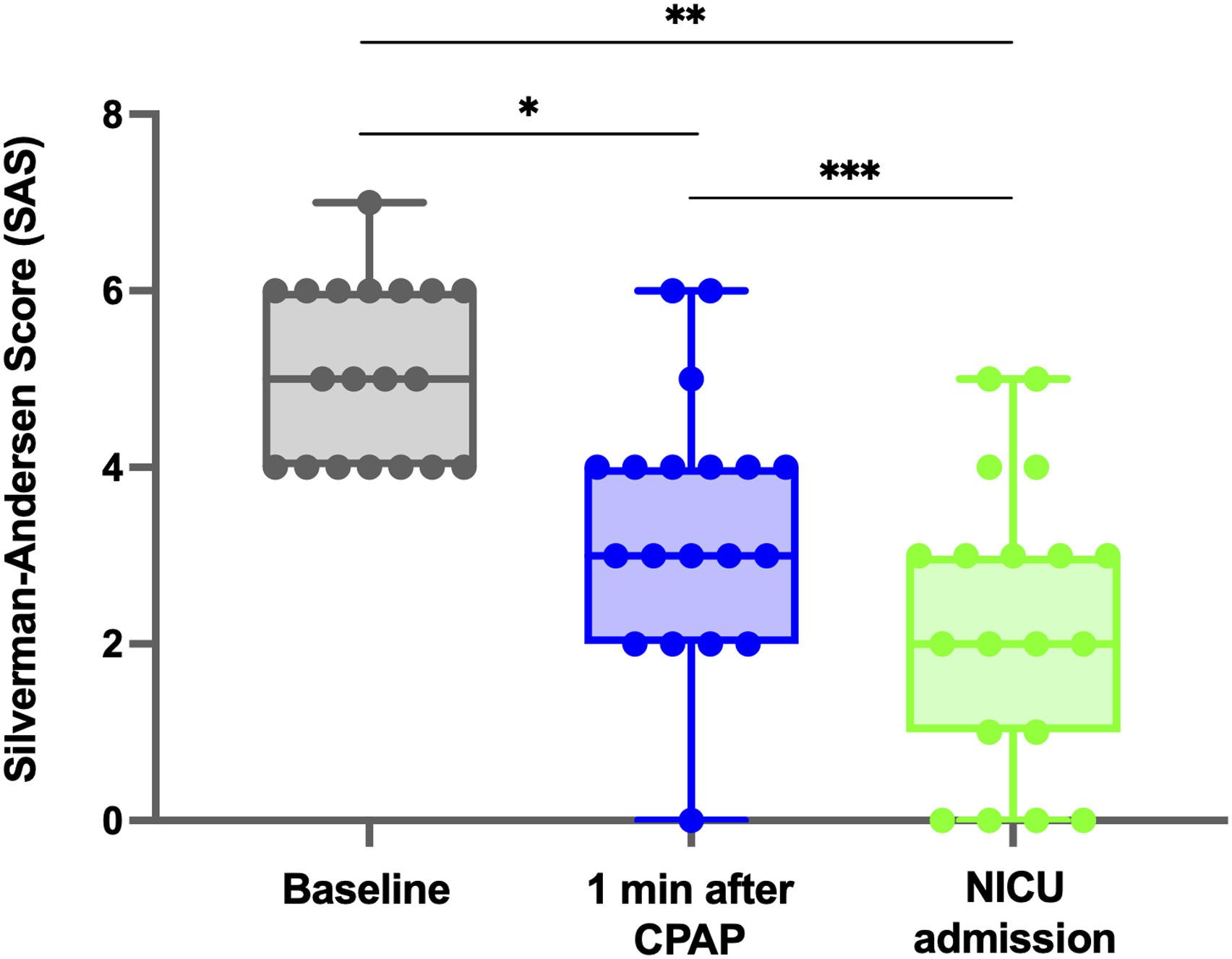
Feasibility and safety
The decision to start the vCPAP system was taken at a median age of 10 min (IQR = 6.5–30) and initiated at a median of 30 min (IQR 25–47). A total of 17 HCPs participated in the care of the 19 patients enrolled in the study. Survey evaluations were performed with these professionals, nine (53%) by physicians and eight (47%) by RTs. Assembly of the system was described as “easy” and “regular” by 12 (70.5%) and 5 (29.5%) professionals, respectively. Ninety-four percent of HCP reported an improvement in the infan’s respiratory symptoms after initiation of vCPAP.
During transport 88% of HCP described use of vCPAP as “easy” and 12% described it as “reasonable.” An improvement in SpO2 was perceived by 10 (59%) professionals, and no changes by 6 (35%). In comparison with other positive pressure devices used in DR and transport, the Vayu system was described as “better” than the other CPAP devices by 14 (82%) or indifferent by 3 (18%) professionals. Figure 2 outlines these feasibility outcomes as perceived by HCP who completed the survey. Feasibility—professional perspectives with Vayu CPAP use in the DR and during transport to the NICU. Legend: DR: delivery room, NICU: neonatal intensive care unit, SpO2: oxygen saturation. Results are presented as absolute values on the X axis for a total of 17 answers.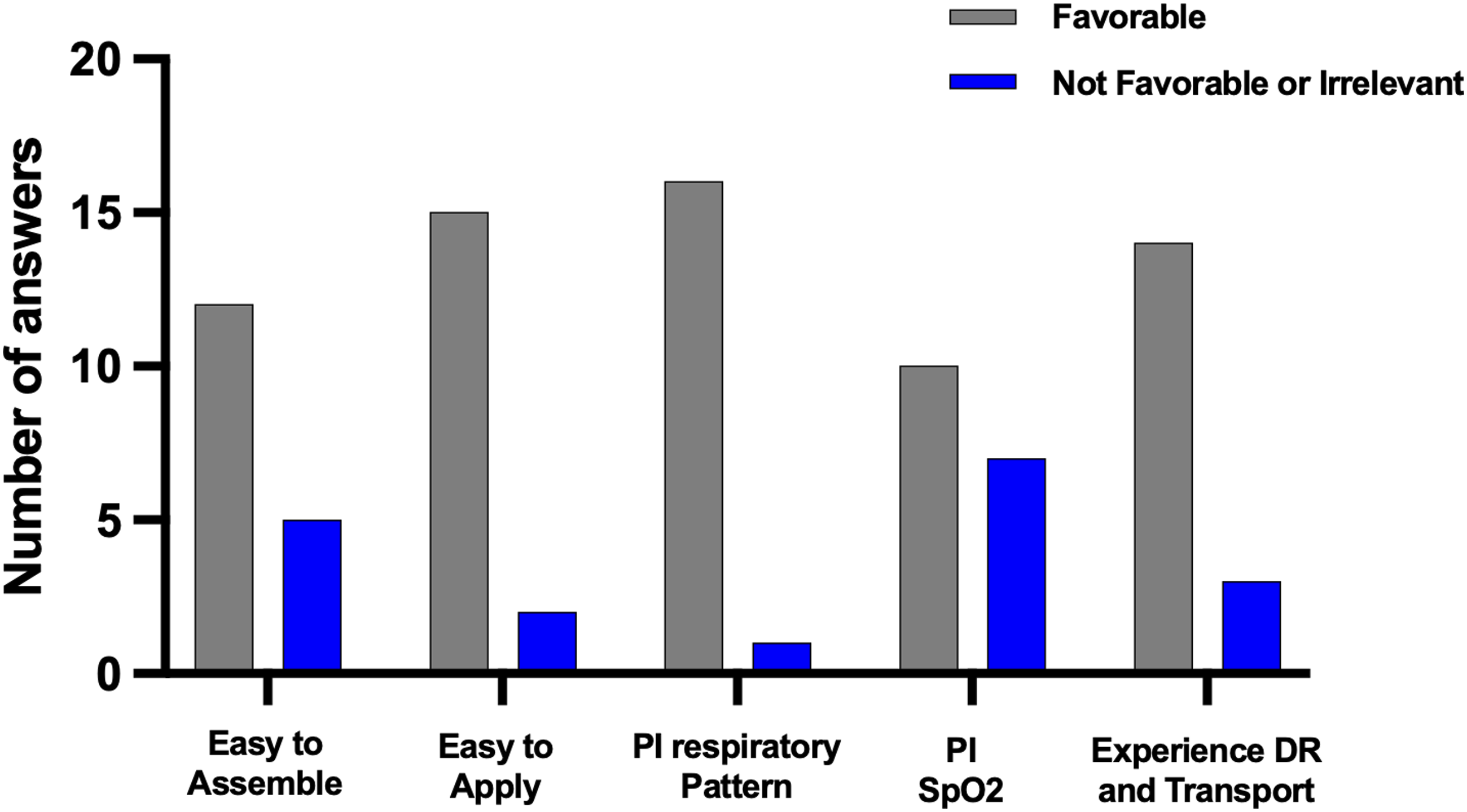
There were no cases of pneumothorax or clinical deterioration.
Discussion
This study is the first to evaluate the feasibility and efficacy of vCPAP for infants 31–40 weeks’ gestation presenting with respiratory distress in the delivery room defined as an SAS ≥4. We found the system to be feasible with 82% of HCP reporting a better experience with vCPAP over current standard of care using a t-piece or bubble CPAP device. Use of vCPAP resulted in a significant improvement in SAS both 1 min after initiation and at the time of NICU admission. No infants in the cohort were diagnosed with pneumothorax or required escalation of respiratory support during their birth hospitalization.
The use of CPAP for infants presenting with respiratory distress at the DR is a well-established clinical practice and a formal recommendation for neonatal global care. 9 There is strong evidence indicating a reduction in intubation rates, shorter length of hospitalization, decreased surfactant use, and a reduction in death and severe BPD, especially among preterm and extremely preterm infants.10–12 vCPAP does not require compressed medical air or electricity thus is an excellent option for LMICs.13–15 The compact and portable design of vCPAP allows it to be easily used during transport from the DR to the NICU.
The SAS provides a quick assessment of respiratory distress based on non-invasive clinical evaluation done at the bedside.16,17 Our findings that vCPAP initiation resulted in a significant decrease in SAS are consistent with prior literature.13,18 SAS ≥5 in the first hour of life are associated with increased need for respiratory support during the first 24 h of life. 17 A reduction in SAS, heart and respiratory rates, and FiO2 at one and 24 h after vCPAP initiation, has been demonstrated on a single center study. 18 While vCPAP has previously been shown to reduce heart rate, respiratory rate, and Fi02 requirement, we did not find a significant difference in similar physiologic parameters (Sp02 and Fi02). This may be explained by the overall normal ranges of Fi02 and Sp02 in our cohort prior to vCPAP initiation and the mild degree of respiratory distress with seven infants in the cohort not requiring CPAP at the time of NICU admission and all infants receiving a diagnosis of TTN.12,19,20
We found a median interval of 19 min between the decision to start vCPAP and its initiation. This is likely due to the study design, including not opening and setting up the vCPAP device prior to delivery, and would not be desirable in more urgent scenarios. . Therefore, assembly of the system prior to birth, in selected patients, could reduce this delay. 21 In addition, continuous training and development of standardized operating procedures may improve these results. 22
Most HCP in our cohort described the experience with Vayu as easy and overall better when compared to other CPAP devices used in DR and transport. Structured survey results from HCP participating in the study found vCPAP feasible to use in the DR and during transport. The clinical acceptance of a new device is a critical point for successful integration.14,21,22 Factors, such as ease of assembly and use, adequate application and monitoring, and affordability, are key points for positive outcomes.
The use of vCPAP was also safe, with no adverse events such as pneumothorax or clinical deterioration as reported before. 21 Safety is especially relevant for a low-cost and potentially widely applicable device. Our lack of safety events may both reflect the effective training session with proper use of the device and the overall health of the infants included in this study. 18
The study has several limitations. First, this was a small prospective study, and respiratory distress was assessed using SAS, which is prone to individual subjectivity. vCPAP can only deliver ≥30% oxygen. Since baseline FiO2 values were already close to this lower limit, FiO2 was a relatively insensitive outcome measure in this study. Additionally, there are several limitations of the vCPAP devices including lack of heat and humidification that may make its use challenging for smaller and sicker infants thus limiting the generalizability of our results to these populations. However, given the demographics of the population studied and the short period of exposure, both issues are likely to be not clinically relevant. At last, all final diagnoses of TTN might limit the generalizability to other causes of respiratory distress and since TTN is a self-limiting condition and the study does not include a control group, the observed clinical improvement cannot be solely attributed to vCPAP treatment. The effect of no heating in more immature infants prone to hypothermia, or unknown humidification for longer periods, needs to be evaluated in future studies. Further investigation is needed including larger sample size, multiple institutions, and higher-risk populations with other respiratory conditions, to confirm efficacy and safety, and enhance generalizability. Randomized controlled trials aiming for head-to-head comparisons with other established CPAP devices would also provide stronger evidence.
Conclusion
In conclusion, we found vCPAP to be feasible and efficacious in reducing SAS score from the DR to NICU admission in a small cohort of infants born at 31–40 weeks’ gestation with a final diagnosis of TTN. This simple, low-cost system is likely of high value for use in infants with respiratory distress when other forms of CPAP are not available. 23
Supplemental material
Supplemental Material - A simple, low-cost bubble CPAP system for use in the delivery room and during transport to the NICU for infants with respiratory distress: A feasibility study
Supplemental Material for A simple, low-cost bubble CPAP system for use in the delivery room and during transport to the NICU for infants with respiratory distress: A feasibility study by Danieli M. K. Leandro, Elisa S. B. Medeiros, Lidiaine N. Oliveira, Gabriel F. T. Variane, Mariana Werneck, Tayane do Vale Bertanha, Rafaela F. R. Pietrobom, Juliana Q. Teixeira, Anna K. S. Nazareth, Daniela P. Rodrigues, Maurício Magalhaes, and Guilherme Sant’Anna in Journal of Neonatal-Perinatal Medicine.
Footnotes
Acknowledgments
The authors would like to express gratitude to the clinical and nursing staff at Hospital da Santa Casa de Misericórdia de São Paulo for their invaluable cooperation and technical support during the data collection phase. We are also profoundly grateful to the families of the neonates included in this study for their participation.
ORCID iDs
Author contributions
The authors disclose that the Vayu Bubble CPAP equipment was kindly donated by Vayu Global Health Innovations. The manufacturer had no role in study design, data collection, statistical analysis, or the developing and submitting processes of this manuscript. The authors have no financial affiliation with Vayu Global Health Innovations.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.