
Abstract
Pelvic organ prolapse (POP) is a common yet complex condition affecting women, characterized by the descent of pelvic organs due to weakened pelvic floor structures. While several treatment strategies exist, their efficacy is often limited, and complications such as surgical failure or recurrence can hinder long-term success. Hydrogels, due to their unique properties such as high-water content, biocompatibility, and flexibility, offer promising potential in the management of POP. This review summarizes various animal models of POP including abdominal wall weakness model, sustained pressure method (vaginal ball stretching), ovariectomy (OVX) model, and gene knockout model. This review further provides a comprehensive overview of the role of hydrogels in POP, highlighting their applications in tissue engineering, drug delivery, and as coatings or injectable materials for prolapsed organs. Furthermore, the challenges in their development were discussed, including material selection, degradability, mechanical properties, and long-term biocompatibility. The strategies to optimize hydrogel performance to better meet clinical needs, with an emphasis on personalization and multifunctionality, were outlined. In conclusion, while hydrogels offer significant promise, further research into their design, application methods, and clinical outcomes is crucial to fully realize their potential in the treatment of POP.
Impact Statement
This review highlights the transformative potential of hydrogels in treating pelvic organ prolapse, a condition with limited long-term therapeutic success. By systematically analyzing animal models and exploring hydrogel applications in tissue repair and drug delivery, it identifies critical challenges and future directions. The insights offered lay the groundwork for personalized, multifunctional hydrogel systems, guiding future research and accelerating clinical translation.
Introduction
Pelvic organ prolapse (POP) is a multifactorial condition characterized by the descent or protrusion of one or more of the pelvic organs, including the bladder, uterus, or rectum, through the vaginal canal. 1 It is a prevalent condition, particularly affecting women in their postreproductive years, with an estimated 50% of women over the age of 50 showing some degree of POP, though the severity can vary widely. 2 While POP is not always associated with significant symptoms, it can lead to a wide range of distressing symptoms such as pelvic pressure, urinary and bowel incontinence, vaginal bulging, and sexual dysfunction. 3 In severe cases, it may even result in physical deformity and profound psychological distress. 4
Given the significant impact of POP on the health and well-being of affected women, its management is a major focus in gynecology and urogynecology. Traditionally, the treatment options for POP include pelvic floor muscle training (PFMT), pessary use, and surgery. Among these, surgery, such as pelvic floor repair or hysterectomy with vaginal vault suspension, remains the most definitive treatment for moderate to severe prolapse.5,6 However, surgery is not without risks, including infection, bleeding, organ injury, and recurrence of prolapse. 7 Moreover, patients may experience long recovery times and complications related to the surgical procedure. 8 As a result, there is an increasing demand for less invasive alternatives that provide effective symptom relief with minimal side effects and faster recovery times. 9
One such alternative that has gained considerable attention in recent years is the use of hydrogel materials in the management of POP. Hydrogel, a water-based polymer material, has a unique set of properties that make it an attractive candidate for medical applications. 10 These properties include biocompatibility, flexibility, moisture retention, and the ability to conform to the anatomical structures it interacts with. 11 Hydrogels have been utilized in a variety of therapeutic areas, including wound healing, drug delivery, and tissue engineering.12,13 More recently, research has explored the application of hydrogel materials in pelvic floor disorders, particularly in conditions such as POP, where support and tissue regeneration are key therapeutic goals. The potential of hydrogel to act as a temporary support structure, filling the void left by weakened tissues, has sparked interest in its use as a nonsurgical adjunct or alternative to conventional treatment modalities. Hydrogel can retain large amounts of water, which helps maintain tissue hydration and promote healing, making it an ideal material for use in tissue repair and support in conditions like POP. 14
Hydrogels have been investigated for their ability to act as scaffolds that provide mechanical support to prolapsed organs, as well as their potential to promote tissue regeneration through their moisture-retaining properties. 15 The idea is that hydrogels, when strategically placed, could help to restore normal anatomical position of the prolapsed organs, or at the very least, alleviate symptoms by providing temporary structural support while the pelvic floor tissues regenerate. In addition, hydrogels have shown promise in improving the function of the pelvic floor muscles and soft tissues, promoting collagen synthesis, and reducing inflammation, all of which could contribute to the long-term success of nonsurgical treatments. 16 This review aims to provide a comprehensive analysis of the role of hydrogel in the treatment of POP, focusing on the biological mechanisms, clinical applications, and potential benefits of this innovative material. This review summarizes overview of POP, POP models, characteristics and application background of hydrogels, applications of hydrogels in POP, and challenges and future prospects of hydrogels (Fig. 1).
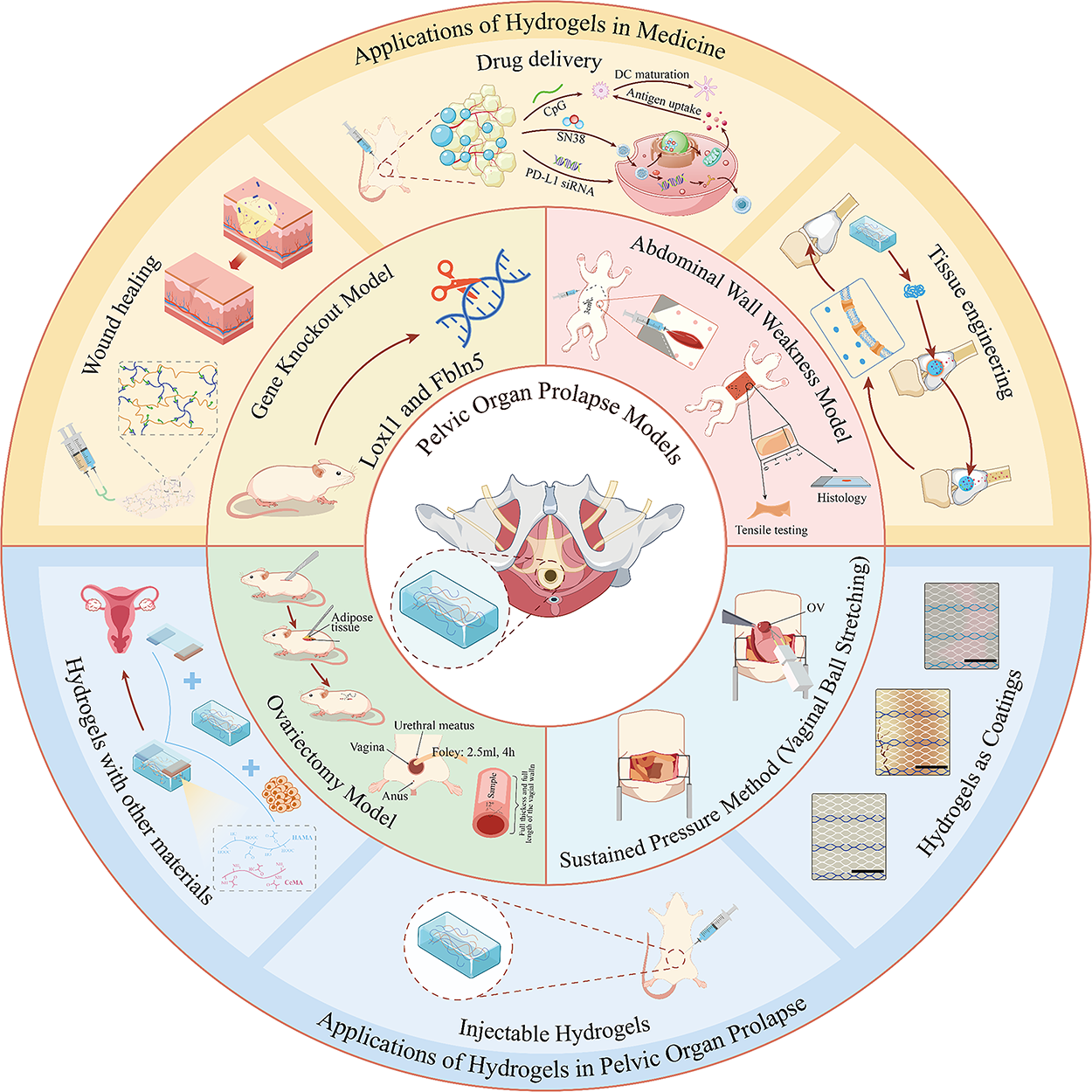
Hydrogels for POP: animal models and biomedical applications. POP, pelvic organ prolapse.
Overview of POP
Etiology and classification
POP is a condition caused by defects, degeneration, or damage to the pelvic floor support structures, with connective tissue weakness in these structures as the primary pathological basis, significantly affecting the quality of life of women.17–19 Epidemiological studies show that the incidence of POP is between 3–6%. 20 The pathophysiology of POP is complex and involves a combination of factors, such as advancing age, hormonal changes, genetic predispositions, obesity, and, notably, vaginal childbirth. As such, POP predominantly affects women after childbirth, and many will require treatment to alleviate the associated symptoms. While POP can occur in younger women, the highest incidence of POP symptoms is between the ages of 70 and 79. 21 Environmental factors contributing to POP include multiple childbirths, tissue trauma, obesity, aging, and others. 22 Genetic factors are currently widely recognized as key determinants in the progression of POP. Connective tissue disorders may be a potential cause of POP. 23
POP is often classified based on the extent of the descent of the pelvic organs, the specific organ affected, and the clinical presentation. There are several systems used for the classification of POP, which help guide the diagnosis, treatment, and prognosis of the condition. The most widely used classification systems for POP include the Baden–Walker system, the Pelvic Organ Prolapse Quantification (POP-Q) system, and the International Continence Society (ICS) Classification. Each of these systems provides different ways of evaluating and categorizing the severity and type of prolapse. The Baden–Walker system is divided into four grades, but it is considered less precise than the POP-Q system, particularly in the classification of organ-specific prolapse. 24 The POP-Q system is a more comprehensive and standardized method for classifying and quantifying POP. 25 It is widely considered the gold standard for the clinical assessment of POP and is endorsed by the ICS. The POP-Q system provides a detailed and reproducible way of measuring the extent of prolapse in relation to fixed anatomical landmarks, offering a consistent way to evaluate prolapse over time and in different settings. 26 The POP-Q system is particularly valuable in clinical trials and research because it allows for standardized, objective measurements and provides a framework for comparing treatment outcomes. 27 The ICS developed a classification system to describe the various types of prolapse based on the organ affected and the direction of descent. 28 The ICS system focuses more on the anatomical location of prolapse and helps identify specific organs that may be involved. Classifying POP accurately is essential for determining the appropriate course of treatment. The different classifications help in understanding the severity of the condition, the specific organs involved, and the most effective interventions. The classification systems also help in patient education, allowing both healthcare providers and patients to understand the severity of the prolapse and the expected outcomes of various treatment options.
Clinical symptoms and diagnosis
POP can range from mild and asymptomatic to severe and debilitating, with a broad spectrum of symptoms that can significantly affect a woman’s quality of life. The main clinical manifestations of female POP include varying degrees of anterior and posterior vaginal wall prolapse, vaginal vault prolapse, uterine and cervical prolapse, and vaginal vault prolapse after hysterectomy. 29 These prolapses may occur individually or simultaneously. Although POP rarely leads to serious illness or death, the discomfort caused by the protruding mass and its impact on bowel and urinary function significantly affect the patient’s quality of life. 30 The diagnosis of POP is made through a combination of patient history, clinical symptoms, physical examination, and additional diagnostic tests. A thorough assessment is required to determine the severity of the prolapse, the organs involved, and any associated complications. The diagnosis also helps inform treatment decisions and guide surgical or nonsurgical management options. A pelvic exam is the cornerstone of the diagnostic workup for POP. 31 The examination allows the clinician to assess the degree of prolapse, the organs involved, and the presence of any associated complications. During the exam, the patient is typically asked to lie on an examination table in a lithotomy position (with legs in stirrups), and the clinician performs a vaginal examination while the patient is asked to cough, bear down, or perform a Valsalva maneuver (straining). If urinary symptoms such as incontinence or retention are present, additional tests may be performed to evaluate bladder function. If bowel symptoms such as constipation, incomplete evacuation, or fecal incontinence are present, defecography as a special X-ray study may be conducted to evaluate rectal function and the degree of rectal prolapse or rectocele. 32 In some cases, imaging studies such as magnetic resonance imaging or ultrasound may be used to further evaluate pelvic floor anatomy and identify areas of prolapse or muscle weakness. These are typically reserved for complex or recurrent cases of POP. Transperineal or transvaginal ultrasound can be used to visualize prolapsed organs and evaluate the extent of prolapse, especially in cases where vaginal examination alone does not provide enough information. 33 Early recognition and diagnosis are essential for determining the most appropriate management strategies.
Current treatment status of POP
Current treatment options for POP can be broadly categorized into nonsurgical treatments and surgical interventions, with a focus on providing symptom relief and improving pelvic floor function. Approximately 13% of women will undergo prolapse surgery in their lifetime. 34 Traditional prolapse surgeries use autologous fascia and ligaments for repair, but due to the weakness of the fascia and ligaments, the recurrence rate postsurgery can be as high as 30%. 35 The treatment of POP has evolved over the years, with a growing emphasis on individualized care, minimally invasive options, and improving patient outcomes. Treatment choices depend on the severity of the prolapse, the specific organs involved, the patient’s age, comorbid conditions, and their preferences regarding the desired outcome. For many women, nonsurgical treatments can be effective in managing symptoms, particularly in those with mild to moderate prolapse or those who are not candidates for surgery due to age, comorbidities, or personal preference. 36 These treatments aim to provide symptom relief, restore pelvic floor function, and prevent further progression of prolapse. PFMT is one of the most common nonsurgical approaches for managing POP. 37 Pessaries are first-line nonsurgical treatments. 38 In postmenopausal women, hormonal therapy (especially estrogen) may help improve pelvic floor muscle tone and vaginal tissue integrity.
Surgical intervention is typically considered for women with moderate to severe POP who have failed conservative management or who have significant symptoms that impair their quality of life. Surgical options aim to restore the anatomical position of the pelvic organs, reduce prolapse symptoms, and provide long-term relief. The type of surgery depends on the organs involved, the severity of the prolapse, and the patient’s preferences regarding the use of mesh or tissue repair. Vaginal surgery is a common approach for correcting POP. 39 It is typically less invasive than abdominal surgery and involves shorter recovery times. Vaginal surgeries are often used for prolapse of the bladder, rectum, or uterus. 40 In cases where vaginal surgery is not feasible or when the prolapse is severe, abdominal surgery may be required. This can be done either through an open incision or using minimally invasive laparoscopic or robotic-assisted techniques. Abdominal surgeries offer higher success rates for certain types of prolapse, particularly when the prolapse involves the vaginal apex or when there is a need for more extensive tissue repair. The use of mesh in POP surgery has been a topic of significant controversy. While mesh can offer a durable and effective solution for repairing prolapse, its use has been associated with complications, such as infection, erosion, and chronic pain. 41 As a result, there has been a shift toward using mesh more cautiously, particularly in vaginal surgeries. Advancements in minimally invasive surgery and robotic-assisted surgery have made it possible to treat POP with less trauma, smaller incisions, and quicker recovery times. Ultimately, personalized treatment plans that incorporate both conservative and surgical options are key to improving the quality of life for women with POP.
POP Models
POP research is essential for understanding the pathophysiology of the condition, developing effective treatments, and evaluating new therapeutic approaches. Various models are employed to replicate the anatomical, functional, and molecular aspects of POP. These models can be broadly categorized into in vitro models and in vivo animal models, each offering distinct advantages in terms of studying the condition’s mechanisms and testing interventions. It is necessary to use different animal models including abdominal wall weakness model, sustained pressure method (vaginal ball stretching), OVX model, and gene knockout model. 42 These animal models are classified based on specific injury methods, with each model simulating a different process of POP development and providing essential experimental data for clinical research.
Abdominal wall weakness model
The abdominal wall weakness model is designed to simulate POP by inducing structural defects or insufficient support in the abdominal wall. This model aims to replicate the mechanical and anatomical changes that occur when the integrity of the abdominal wall is compromised, thereby providing insight into the pathogenesis of POP and strategies for its prevention or treatment. Commonly used methods include partial excision of abdominal wall tissues, such as muscle and fascia, or the application of synthetic or biological materials to deliberately weaken the abdominal wall. These interventions result in decreased abdominal support, mimicking the descent of pelvic organs due to weakened musculature and connective tissue.
For instance, a representative study utilized adult female New Zealand white rabbits to establish a reproducible abdominal wall weakness model. 43 Under sterile conditions, and with the animals reared in single cages under standard care, a midline abdominal incision was made. The subcutaneous tissue was carefully separated while preserving the peritoneum and deep muscle layers with tissues between the superficial muscle layer and the dermis excised. A standardized defect measuring 10 × 40 mm2 was created at three distinct sites. Subsequently, the fascia and dermis were sutured layer by layer, and the wound was disinfected and bandaged. This procedure successfully led to the formation of a POP model, effectively replicating the loss of mechanical support observed in human POP.
In another study focusing on localized abdominal wall injury and material implantation, the surgical procedure was refined through pilot testing to determine the optimal muscle layers for injection, hydrogel volumes, cannula positioning, and wound closure techniques (Fig. 2). 44 The external oblique muscle (a superficial abdominal wall layer) was exposed by making a 30 mm skin incision, followed by muscle dissection. The muscle was then closed using five interrupted 4/0 Vicryl degradable sutures, while intentionally leaving a small opening at the incision site to allow for hydrogel injection. This model provides a controlled platform to test the efficacy of biomaterial-based reinforcement strategies in weakening or damaged abdominal walls, with potential translational value for POP repair. Together, these models provide critical tools for exploring how abdominal wall defects contribute to pelvic floor dysfunction, and for evaluating innovative therapeutic interventions that aim to restore structural support and prevent prolapse progression.
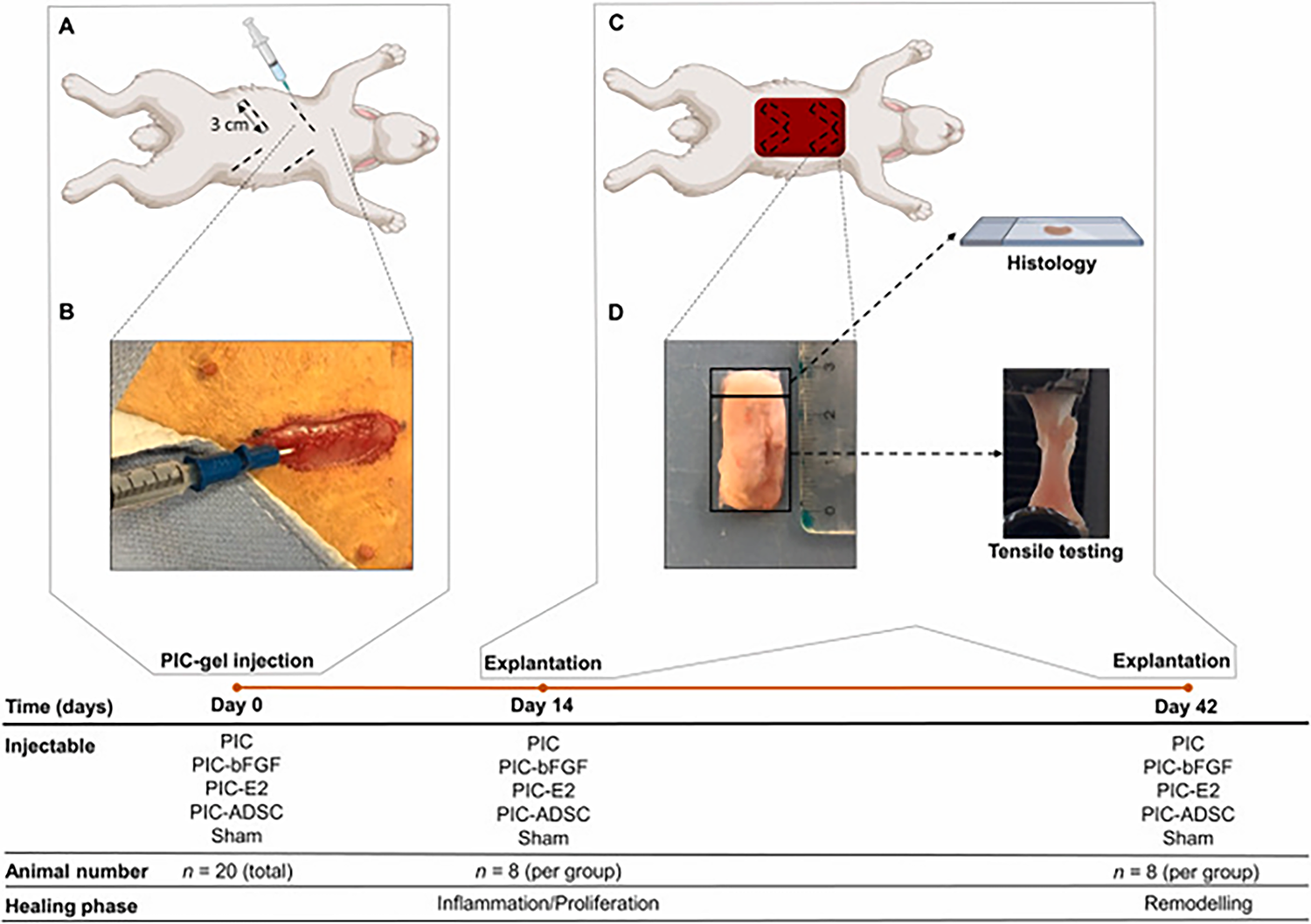
Abdominal Wall Weakness Model.
44
Sustained pressure method (vaginal ball stretching)
The sustained pressure method applies chronic mechanical stress to pelvic organs to simulate tissue stretching and displacement, mimicking the pathophysiological process of POP. The most common approach is the vaginal ball stretching model, which involves prolonged expansion or traction of the vaginal canal and adjacent support structures. This model replicates the gradual descent of pelvic organs under persistent pressure or overload, thereby reflecting clinical scenarios such as multiple childbirths or chronic intra-abdominal pressure. Such models are invaluable for understanding the biomechanical impact of sustained pressure on pelvic support structures, including muscles, fascia, and connective tissues. They also provide a platform to investigate tissue remodeling, inflammatory responses, and cellular changes resulting from mechanical loading, contributing to our knowledge of POP pathogenesis and potential therapeutic strategies.
A representative example is a rat prolapse model developed using a specially designed vacuum suction device tailored to the anatomy of the rat’s vagina (Fig. 3). 45 The device was fully inserted into the vaginal canal, and negative pressure was applied to pull the cervix and part of the fornix tissue outward through the vaginal opening. The traction standard was defined as the cervix protruding 5 mm beyond the external vaginal introitus. The exposed cervix was secured using 3–0 Prolene sutures in a cross pattern, with a 2-cm suture tail reserved for repeated traction. The rats underwent nine traction cycles per day, each lasting 2 min with a 1-min interval, for a total of 7 consecutive days. This was followed by 7 days of recovery before undergoing pelvic surgery (unilateral presacral suspension). The prolapsed cervix remained visible outside the introitus with the sutures retained in place, facilitating postoperative evaluation of prolapse repair. This model not only simulates sustained mechanical loading on pelvic organs but also enables dynamic assessment of tissue repair capacity and treatment response under real-world mechanical stress conditions, making it a robust platform for both mechanistic studies and therapeutic evaluations in POP research.
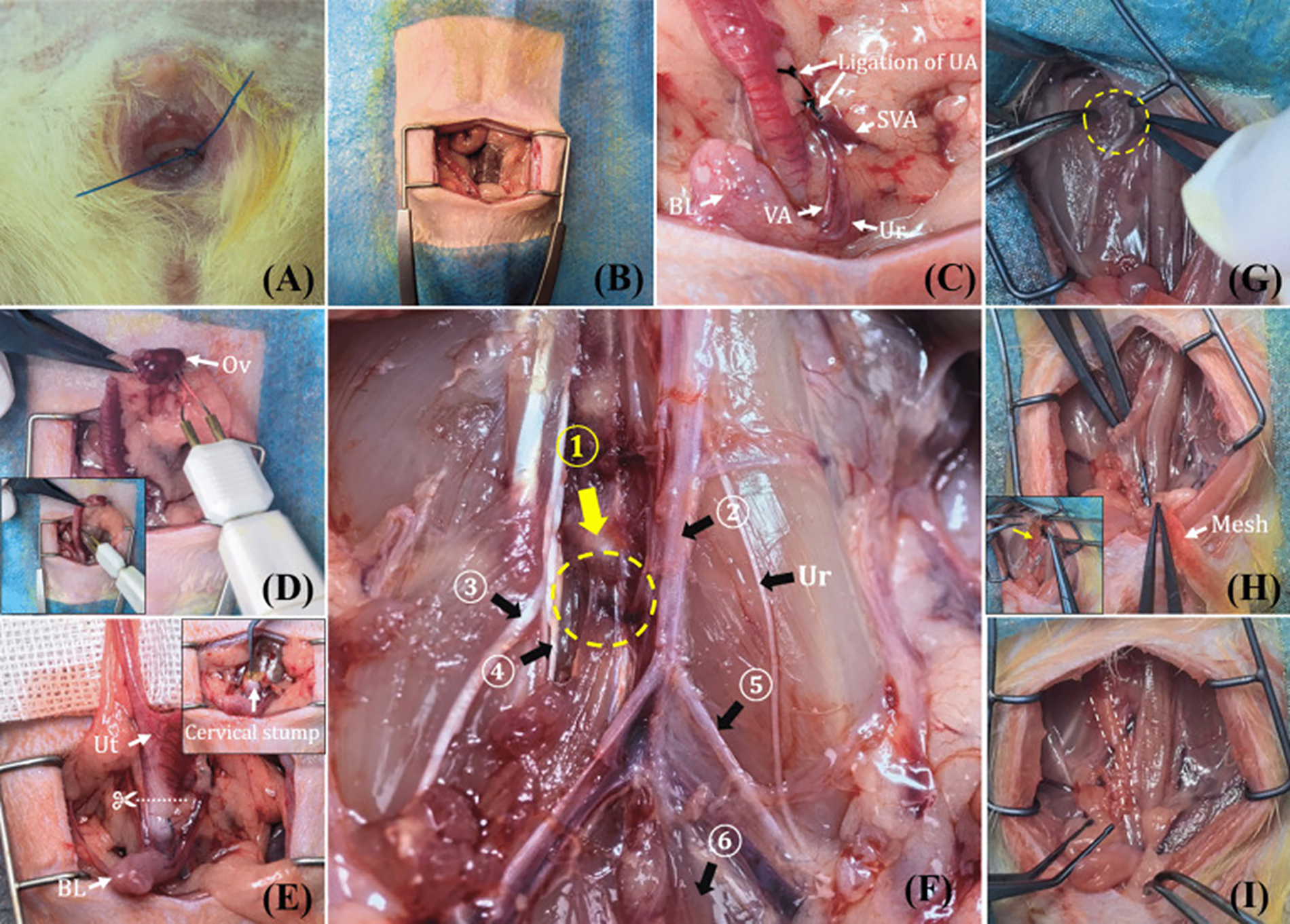
Sustained pressure method (vaginal ball stretching). The procedure of unilateral presacral suspension
OVX model
The OVX model is widely used to simulate the postmenopausal hormonal state in female animals. Surgical removal of the ovaries results in a sharp decline in estrogen levels, which subsequently leads to atrophy of pelvic floor muscles, degradation of connective tissue components such as collagen and elastin, and overall weakening of pelvic support structures. This model serves as a reliable preclinical platform to study the pathophysiological effects of estrogen deficiency and to evaluate hormone-based interventions for POP. In a typical OVX procedure performed in rats, bilateral abdominal incisions are made to access and excise the ovaries (Fig. 4). 46 To further enhance the relevance of the model, simulated vaginal delivery can be incorporated to mimic birth-related mechanical injury. This combination of hormonal deprivation and mechanical trauma provides a more comprehensive model for exploring the multifactorial etiology of POP.
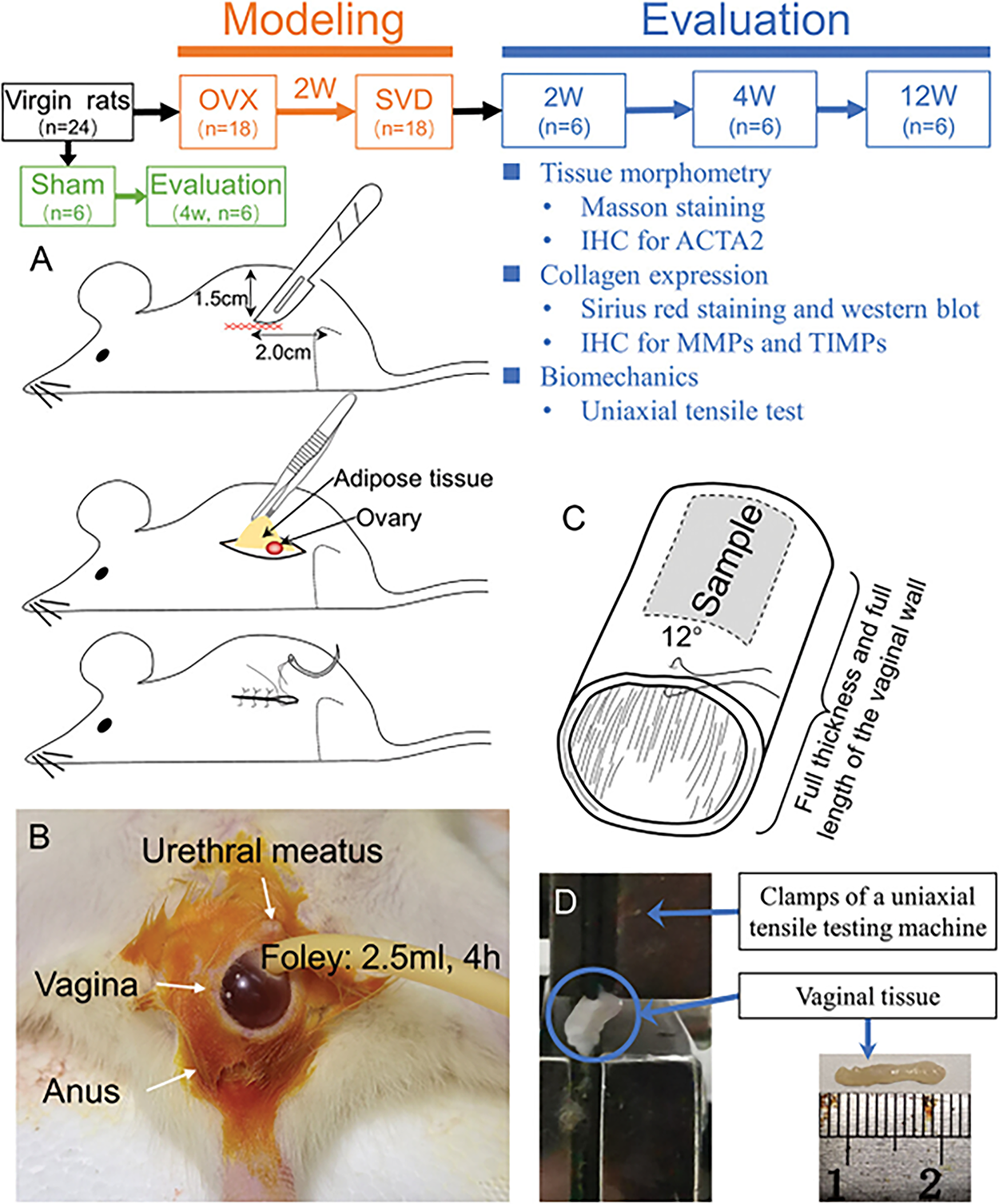
Establishment and evaluation of a POP ovariectomy model in rats. Modeling
In addition to animal models, clinical human-derived primary cell models provide further insights into the cellular effects of hormonal changes with the tissues collected during surgical procedures. These fibroblasts, derived from severely prolapsed tissues in postmenopausal women, offer a valuable in vitro platform to study the molecular and cellular consequences of estrogen deficiency, including impaired collagen synthesis, increased matrix metalloproteinase activity, and decreased tissue repair capacity. 47 Together, these models—from ovariectomized rodents to human-derived vaginal fibroblasts—enable in-depth exploration of postmenopausal POP pathogenesis and form a theoretical foundation for the development of targeted estrogen-related therapies.
Gene knockout model
The gene knockout model involves knocking out specific genes to simulate the impact of gene deletion on the development of POP. For example, knocking out genes related to connective tissue generation, elastin production, or pelvic floor muscle function leads to weakened tissue structures, making it easier for POP to occur. This model is useful for studying the genetic factors involved in POP, particularly at the molecular level, such as how genetic defects cause connective tissue degradation and elastin fiber damage, ultimately leading to POP. Gene knockout models enable researchers to explore the relationship between specific genes and POP, providing data to support personalized treatment approaches. Mice are especially useful for studying the POP. 48 Mice are genetically modified to study the role of specific genes involved in tissue remodeling, collagen production, and pelvic floor muscle function. For instance, knockout mice (KO) lacking genes encoding for collagen or extracellular matrix proteins can help researchers understand how these factors contribute to the development of prolapse, especially mouse KO models. 49
Among the enzymes responsible for elastin fiber assembly are LOX, LOXL1, fibulin-3, and fibulin-5. There are several mouse knockout models of POP, including Loxl1, Fbln5, Fbln3, Hoxa11, and Upii-sv40t. 50 The POP phenotype of Loxl1 and Fbln5 KO models were most reliable and predictable. It has been reported that the mice lacking Loxl1 could develop stable POP phenotype. 51 Tappy et al. utilized a mouse model of POP, fibulin-5 knockout (Fbln-5-/-) mice, to assess the ability of dasatinib and quercetin to prevent development of prolapse. 52
These animal models play a critical role in POP research. By simulating different injury methods, researchers can model various processes of POP development, study its pathogenesis, and evaluate the effects of different treatments. Ultimately, these animal models provide valuable experimental data for clinical treatments and promote the development of prevention, diagnosis, and treatment methods for POP.
Characteristics and Application Background of Hydrogels
Biomaterials have extensive applications in the medical field, including metals, ceramics, polymers, and composites. However, they have poor biocompatibility, which may lead to immune responses. Hydrogels, as a novel class of biomaterials, are a type of hydrophilic polymer matrices. 53 They possess excellent properties such as outstanding water retention ability, soft texture, stretchability, deformability, and good biocompatibility.54,55 Therefore, hydrogels play important roles in biomedical applications.
Basic structure and properties of hydrogels
The primary feature of hydrogels is their three-dimensional (3D) network of hydrophilic polymers, which interact with water molecules to form a gel-like structure. 56 The polymer backbone is responsible for the structural integrity of the hydrogel. 57 Cross-linking refers to the formation of covalent or ionic bonds between polymer chains, which creates a network structure. 58 Cross-links play a critical role in maintaining the structural stability and mechanical strength of the hydrogel. 59 The hydration capacity of a hydrogel refers to its ability to absorb and retain water in its structure, which is critical for hydrogels used in biological applications. 60 The swelling behavior of hydrogels is often governed by osmotic pressure, which is created due to the affinity of the polymer for water molecules. 61 Biocompatibility is one of the most important properties of hydrogels. 62 Biocompatible hydrogel does not evoke a significant immune response when introduced into the body. 63 Biodegradability is another essential property for hydrogels used in drug delivery, wound healing, and tissue engineering. 64 The rate of biodegradation can be controlled by adjusting the cross-linking density, the type of polymer used, and the incorporation of degradable groups such as ester or amide bonds. 65 The mechanical properties are also essential for various applications. 66 Mechanical properties can be modified by controlling the degree of cross-linking, the molecular weight of the polymer chains, and by blending different types of polymers. 67 Incorporating nanoparticles or fibers into the hydrogel matrix can further enhance its mechanical strength, allowing hydrogels to be tailored for specific biomedical uses. 68
Applications of hydrogels in medicine
Hydrogels have a wide array of applications in medicine, particularly in wound repair, drug delivery, and tissue engineering. 69 Hydrogels are widely used in wound repair due to their extracellular matrix (ECM)-like characteristics. 12 Qian et al. developed a novel glycyrrhizic acid (GA)-based hybrid hydrogel dressing with intrinsic immunoregulatory properties for promoting rapid diabetic wound healing. 70 Biodegradable or easy-to-remove hydrogels can reduce secondary damage to wounds. 71 An injectable hydrogel is developed for emergency hemostasis and wound repair (Fig. 5). 72 Hydrogels for drug delivery can be designed to respond to specific environmental cues. A pH-responsive hydrogel is promising. 73 Wu et al. constructed a pH/reactive oxygen species (ROS) dual responsive injectable glycopeptide hydrogel. 74 Mosquera et al. used a synthetic hydrogel-based organoid for defining tumors undergo epigenetic reprogramming. 75 Wang et al. developed in situ vaccination with an injectable nucleic acid hydrogel for synergistic cancer immunotherapy, where immune checkpoint inhibitor programmed cell death ligand-1 siRNA is designed as a crosslinker to assemble with the cytosine-phosphate-guanine- and 7-ethyl-10-hydroxycamptothecin (SN38)-containing Y-shaped motif (Fig. 6). 76 Yang et al. constructed a multiple hydrogel for cartilage regeneration (Fig. 7). 77 The hydrogel could alleviate the inflammatory reaction and regulate oxidative stress in situ. Li et al. fabricated an injectable hydrogel microsphere for cartilage regeneration. 78
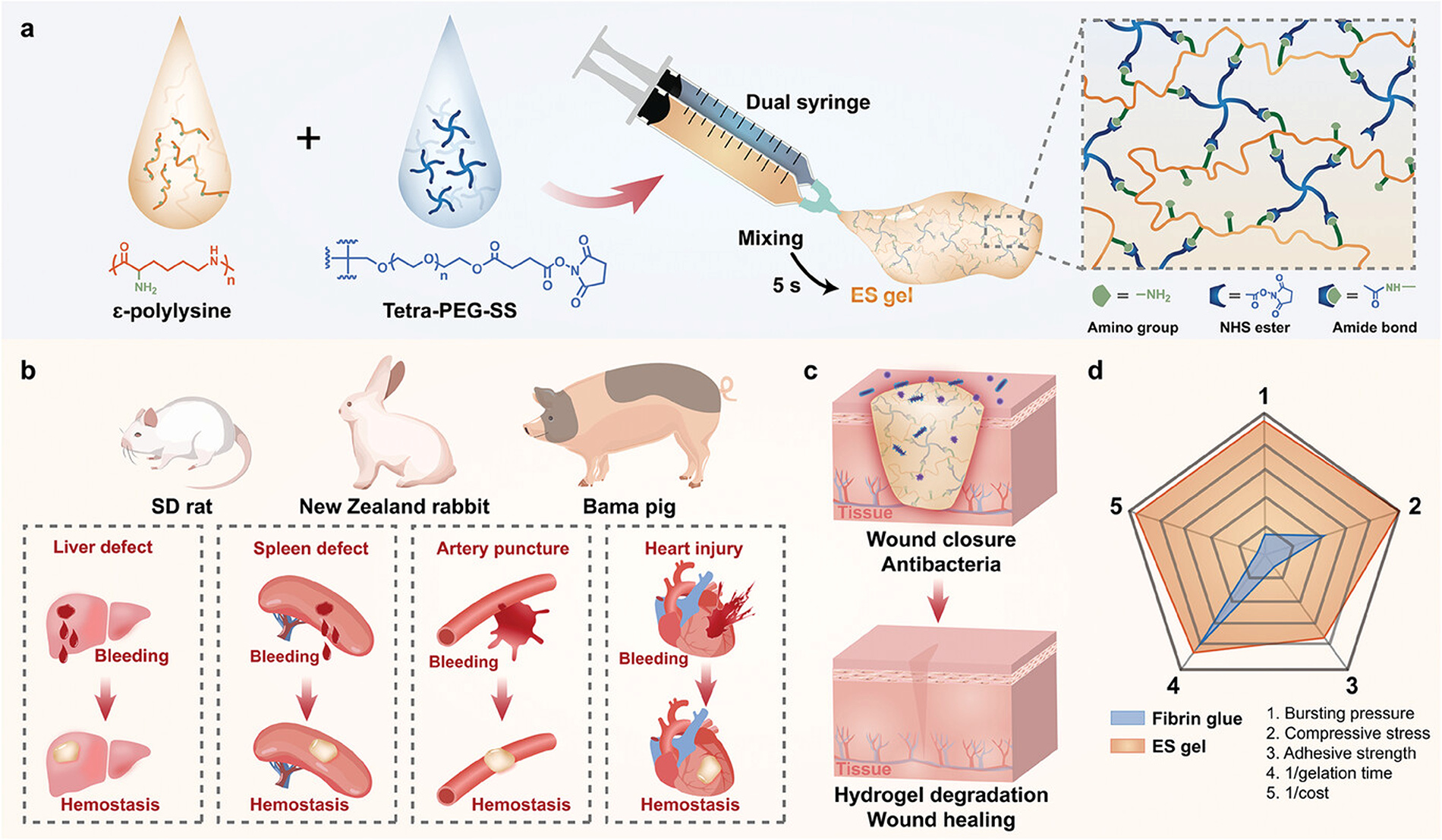
Design and application of the hydrogel for hemostasis and wound healing. Design
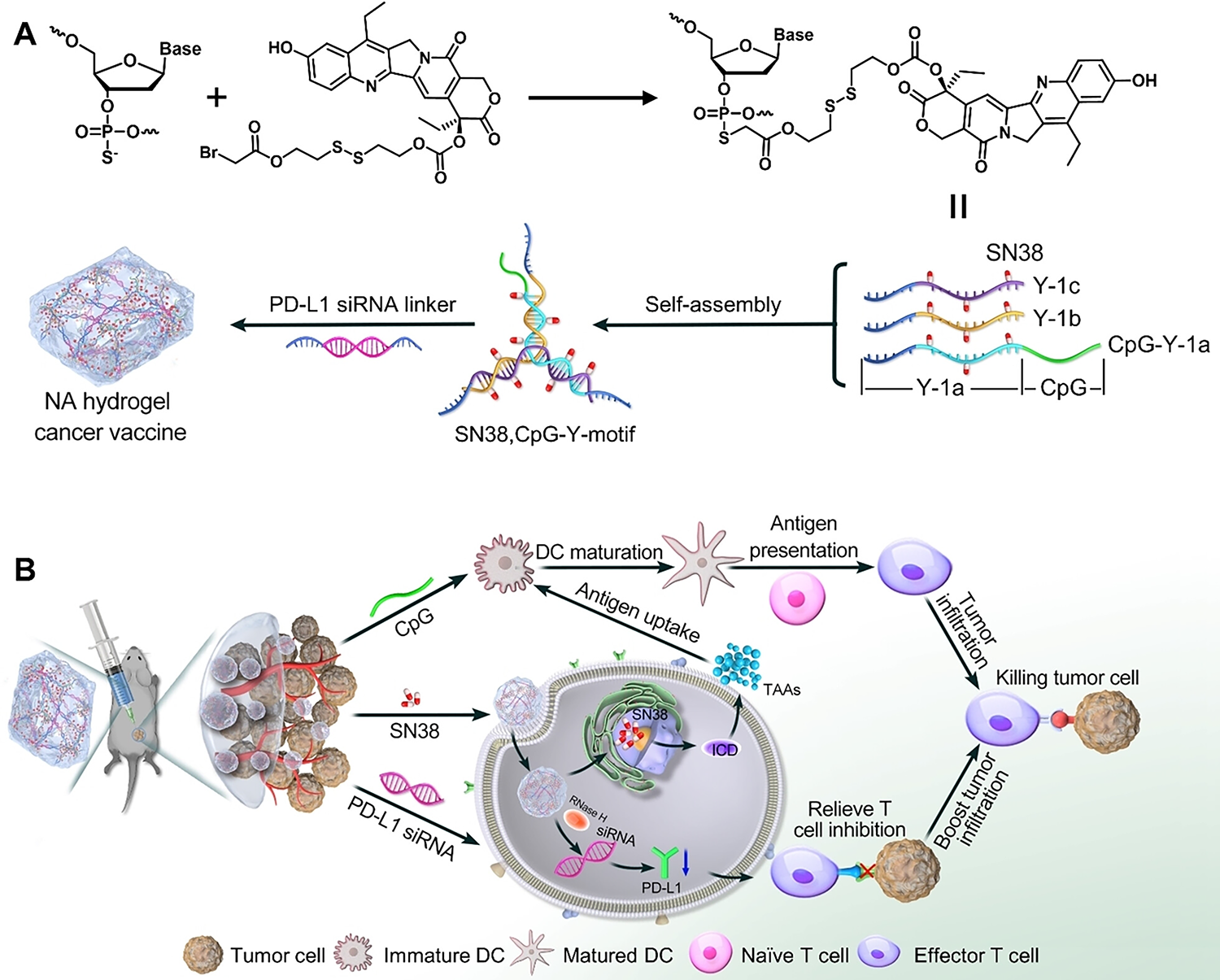
Schematic illustration of programmed self-assembly of the nucleic acid hydrogel tumor vaccine and its synergetic antitumor immunotherapy. Design
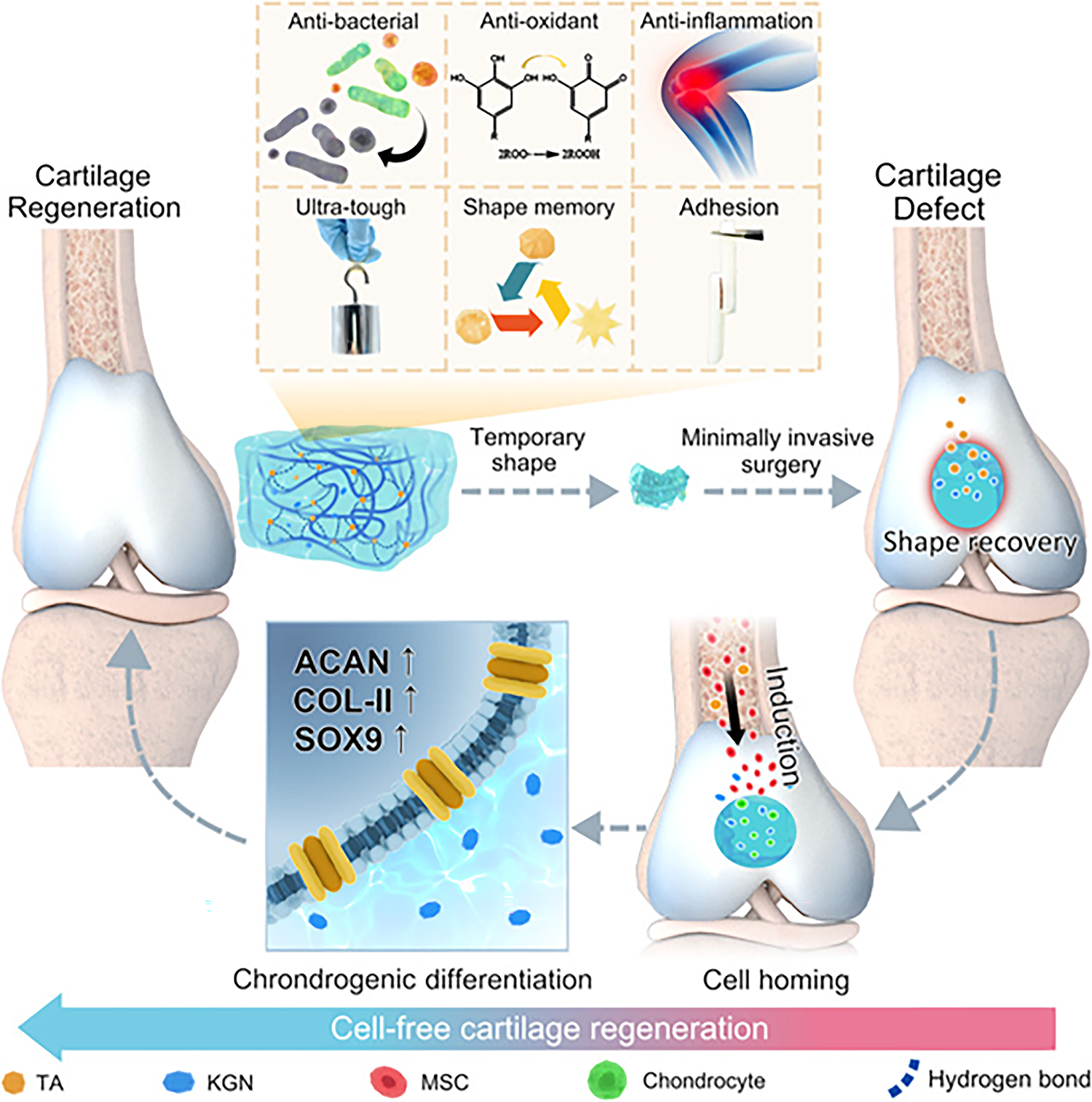
Hydrogel-induced cell-free cartilage regeneration. 77
Applications of Hydrogels in POP
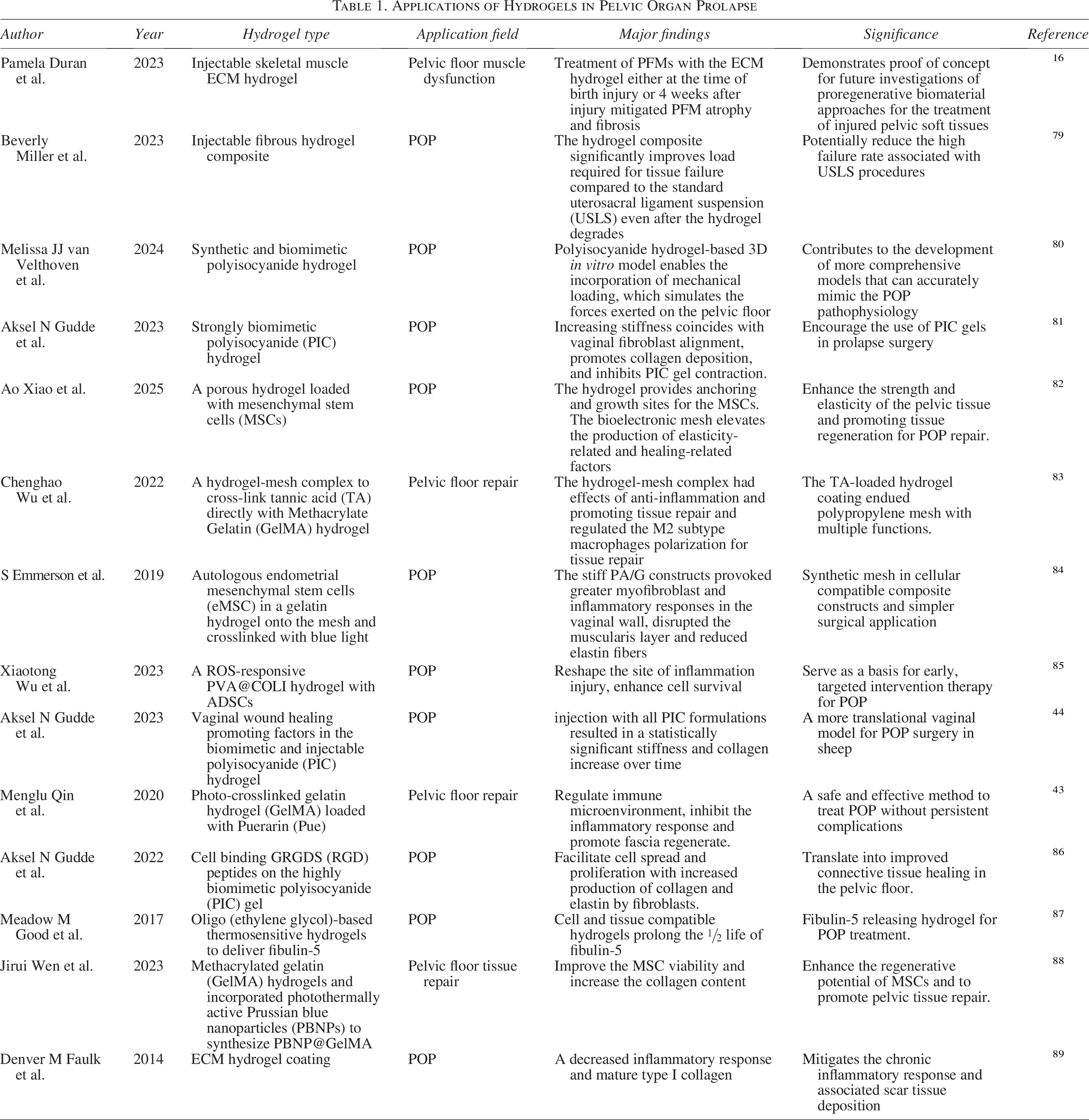
Current treatment options of POP range from conservative management to surgical repair, but there is growing interest in developing less invasive, tissue-engineering-based therapies to provide more effective and sustainable solutions. Hydrogels, whether natural or synthetic, exhibit varying properties that are crucial for their application in POP treatment. Biodegradability is a significant factor, with natural hydrogels like collagen degrading more quickly than synthetic ones. Synthetic hydrogels, such as polyisocyanide (PIC)-based materials, offer the advantage of tunable biodegradation, providing better long-term support. Mechanical strength is another essential property, as natural hydrogels often lack the necessary strength for prolonged use. In contrast, synthetic hydrogels can be engineered to match the mechanical properties of pelvic tissues, enhancing their suitability for POP applications. Immunogenicity plays a critical role in preventing adverse immune responses. Natural hydrogels tend to be biocompatible, mimicking the body’s extracellular matrix, while synthetic hydrogels may require modifications to improve biocompatibility and reduce immunogenicity. Lastly, scalability is a key consideration. While natural hydrogels face challenges in large-scale production, synthetic options are easier to manufacture consistently and in large quantities, making them more practical for clinical use. A careful balance of these properties is essential in selecting hydrogels for effective and sustainable POP treatment. This section focuses on the application of hydrogels in POP, particularly in their use as coatings, injectable hydrogels, and composite applications with other materials. The applications of hydrogels in POP have been listed in Table 1.
Applications of Hydrogels in Pelvic Organ Prolapse
Hydrogels as coatings
One of the most promising applications of hydrogels in the context of POP is their use as coatings on surgical meshes or implants. Meshes are commonly used in prolapse repair surgeries, but complications such as mesh erosion, infection, and chronic pain have been reported. Hydrogels, due to their lubricating properties and biocompatibility, can be used to coat these meshes, potentially reducing complications and improving patient outcomes. 90 The application of hydrogel coatings to surgical meshes reduces friction between the mesh and surrounding tissues, minimizing the risk of abrasion and subsequent irritation. 91 This is particularly beneficial in the vaginal and pelvic region, where the tissue is highly sensitive. Moreover, hydrogels can be incorporated with antimicrobial agents, helping prevent bacterial colonization and infection at the implant site. This antimicrobial capability can significantly reduce the risk of postoperative infections, which are a common complication in pelvic floor surgeries. 92 Certain hydrogels can be engineered to promote cellular infiltration and tissue regeneration. This feature is particularly valuable in promoting the integration of the mesh with the surrounding tissue, ensuring better long-term outcomes for patients. For example, Faulk et al. assessed the effects of an ECM hydrogel coating on the long-term host tissue response to polypropylene mesh, which mitigates the chronic inflammatory response to polypropylene mesh for POP. 89
Hydrogels provide a moisture-rich surface that can serve several functions in the context of POP treatment. Hydrogel coatings can enhance the biocompatibility of the underlying mesh, reducing the likelihood of the body’s immune response to the implanted material. 93 This can minimize issues such as chronic inflammation and fibrosis, which are often seen with mesh implants. Wu et al. fabricated a hydrogel-mesh complex using one-step coating modification (Fig. 8). 83 The hydrogel coating was important for facilitating pelvic floor repair.
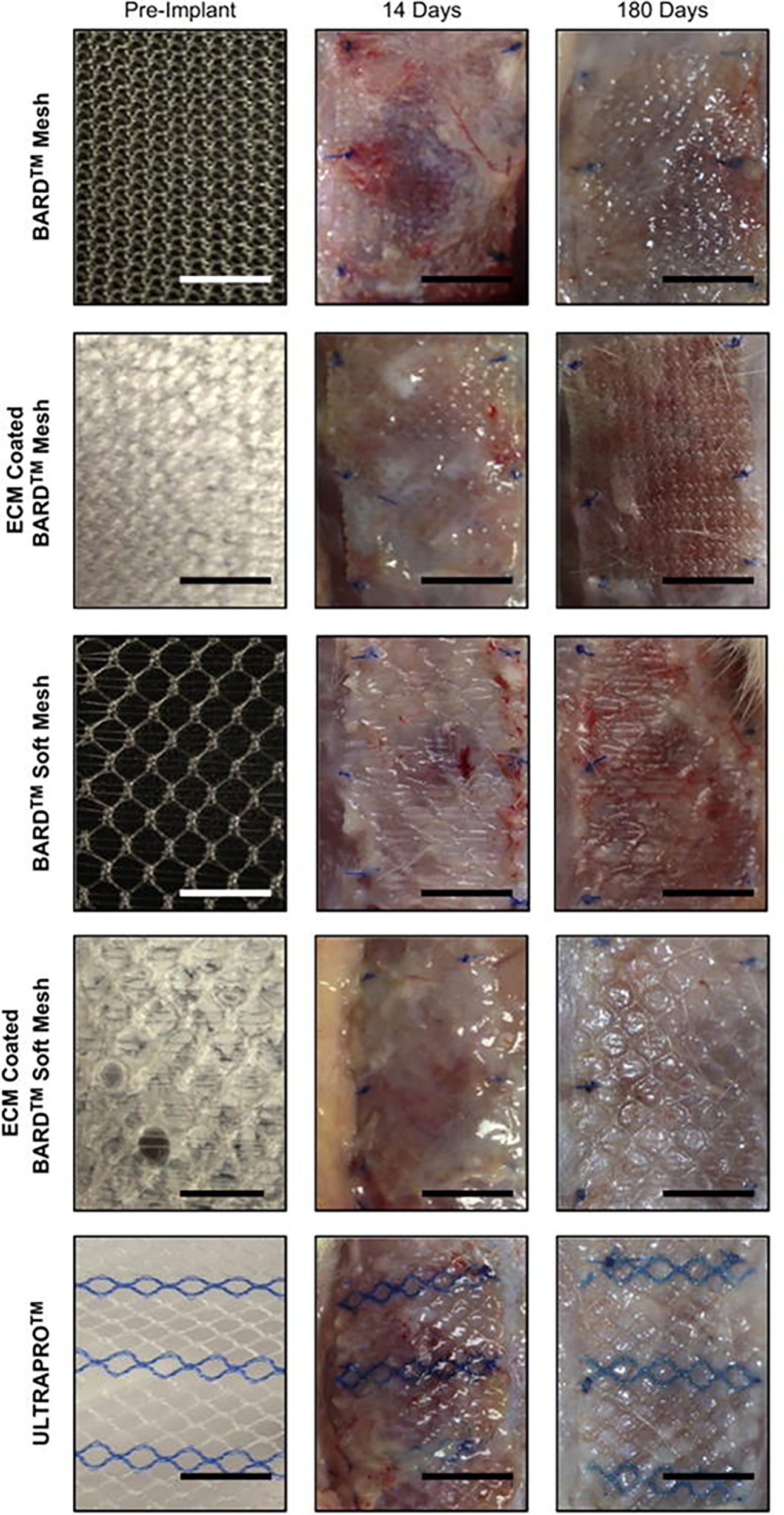
Extracellular matrix hydrogel coating mitigates the chronic inflammatory response to polypropylene mesh. 83
Injectable hydrogels
Injectable hydrogels are another innovative application in POP treatment, which can be injected directly into the pelvic tissues via minimally invasive procedures, offering a nonsurgical alternative to support weakened pelvic structures. Injectable hydrogels can be designed to provide mechanical support to the pelvic floor tissues. 94 They can be injected into the vaginal walls or surrounding tissues, helping to lift and support prolapsed organs. The hydrogels can be tailored to mimic the mechanical properties of native pelvic tissues, providing both strength and flexibility. Fibrin is a natural polymer derived from blood plasma and has been used in injectable form for tissue engineering. 95 Fibrin hydrogels have been shown to promote cell migration and tissue repair, making them an excellent candidate for use in pelvic floor regeneration. 96 Miller et al. found the injectable fibrous hydrogel composite significantly improves load. 79 The ability to inject these hydrogels minimally invasively is a significant advantage over traditional surgical methods, as it reduces the need for extensive incisions and can lead to faster recovery times. Thermosensitive hydrogels undergo a phase transition from liquid to gel at body temperature. This property allows for easy injection of the material, which then solidifies at the treatment site, providing structural support and promoting tissue regeneration. Good et al. found fibulin-5-containing oligo (ethylene glycol)-based thermosensitive hydrogels resulted in incorporation of fibulin-5 after injection. 87
Many injectable hydrogels are bioactive and can release growth factors or other bioactive molecules over time to promote tissue regeneration. This can help strengthen the pelvic floor and prevent further prolapse. Duran et al. evaluated the acellular injectable skeletal muscle ECM hydrogel for the prevention of pelvic floor muscle dysfunction. 16 Furthermore, injectable hydrogels can be engineered to provide controlled, sustained release of therapeutic agents, such as collagen-stimulating factors or anti-inflammatory agents. This can enhance the long-term effectiveness of treatment. Gudde et al. used known vaginal wound healing promoting factors in the biomimetic and injectable PIC hydrogel, which improves regenerative capacity and healing. 44 Polyvinyl alcohol (PVA) is a popular hydrogel material due to its excellent water retention properties and ease of synthesis. 97 PVA-based hydrogels have shown promise in reducing friction and enhancing tissue integration when used as coatings for surgical meshes. 98 Wu et al. developed a ROS-responsive collagen hydrogel cell carrier for local injection to deliver adipose mesenchymal stem cells (MSCs) to the injured tissue site accurately (Fig. 9). 85 The gel could reshape the site of inflammation injury and enhance cell survival.
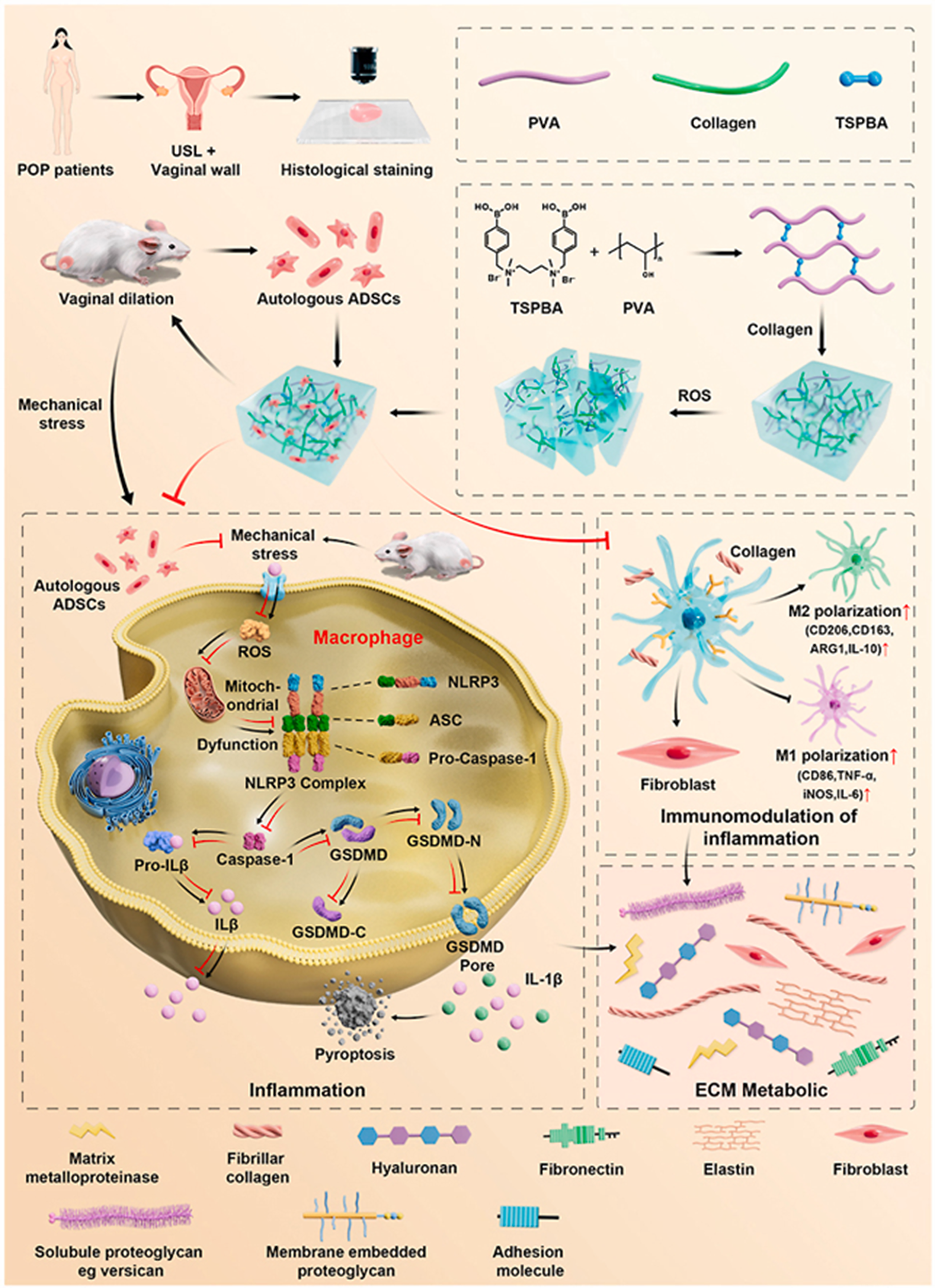
An ROS-responsive collagen hydrogel cell carrier for local injection to deliver adipose mesenchymal stem cells (ADSCs). 85 ROS, reactive oxygen species.
Composite applications of hydrogels with other materials
Researchers have explored combining hydrogels with other materials, such as biolayers, cellulose, and nanoparticles, to enhance their properties and extend their applications in POP treatment. Cellulose is a natural biopolymer that is widely used in biomedical applications due to its abundance, biocompatibility, and mechanical strength. 99 When combined with hydrogels, cellulose can provide additional structural support and improve the mechanical properties of the hydrogel, making it more suitable for use in prolapse repair. 100 Cellulose fibers reinforce the hydrogel matrix, improving its structural integrity and providing better support to the pelvic tissues. 101 The combination of cellulose with hydrogels can help maintain tissue hydration and improve biocompatibility, enhancing the overall therapeutic effect. 102 Gudde et al. found cell binding GRGDS (RGD) peptides on the highly biomimetic PIC gel facilitates and promotes the function of primary vaginal fibroblasts isolated from a POP patient. 86
Biolayers are thin layers of biological materials that can be incorporated into hydrogels to provide additional biological functionality. These biolayers may contain growth factors, stem cells, or extracellular matrix proteins, which can aid in tissue regeneration and repair. By incorporating biolayers into hydrogels, researchers can enhance the ability of the hydrogel to support tissue regeneration, particularly in the pelvic floor, where the support structures are weakened in prolapse. Emmerson et al. used autologous endometrial MSCs in a gelatin hydrogel onto the polyamide (PA) mesh and crosslinked with blue light, which provoked greater myofibroblast and inflammatory responses in the vaginal wall, disrupted the muscularis layer and reduced elastin fibres. 84 Biolayers can enhance cell attachment and growth within the hydrogel matrix, promoting faster and more efficient tissue integration. Xiao et al. designed a bioelectronic mesh consisting of a galvanic cell film and a porous hydrogel loaded with MSCs, enhancing the strength and elasticity of the pelvic tissue and promoting tissue regeneration for POP repair (Fig. 10). 82 The local stimulation strategy significantly reduces inflammation in pelvic tissues. Furthermore, the bioelectronic mesh completely degrades after in vivo application, eliminating the risks associated with surgical removal and demonstrating excellent biocompatibility.
Treating POP with the device, consisting of a galvanic cell film and a composite hydrogel loaded with MSCs.
82
Design
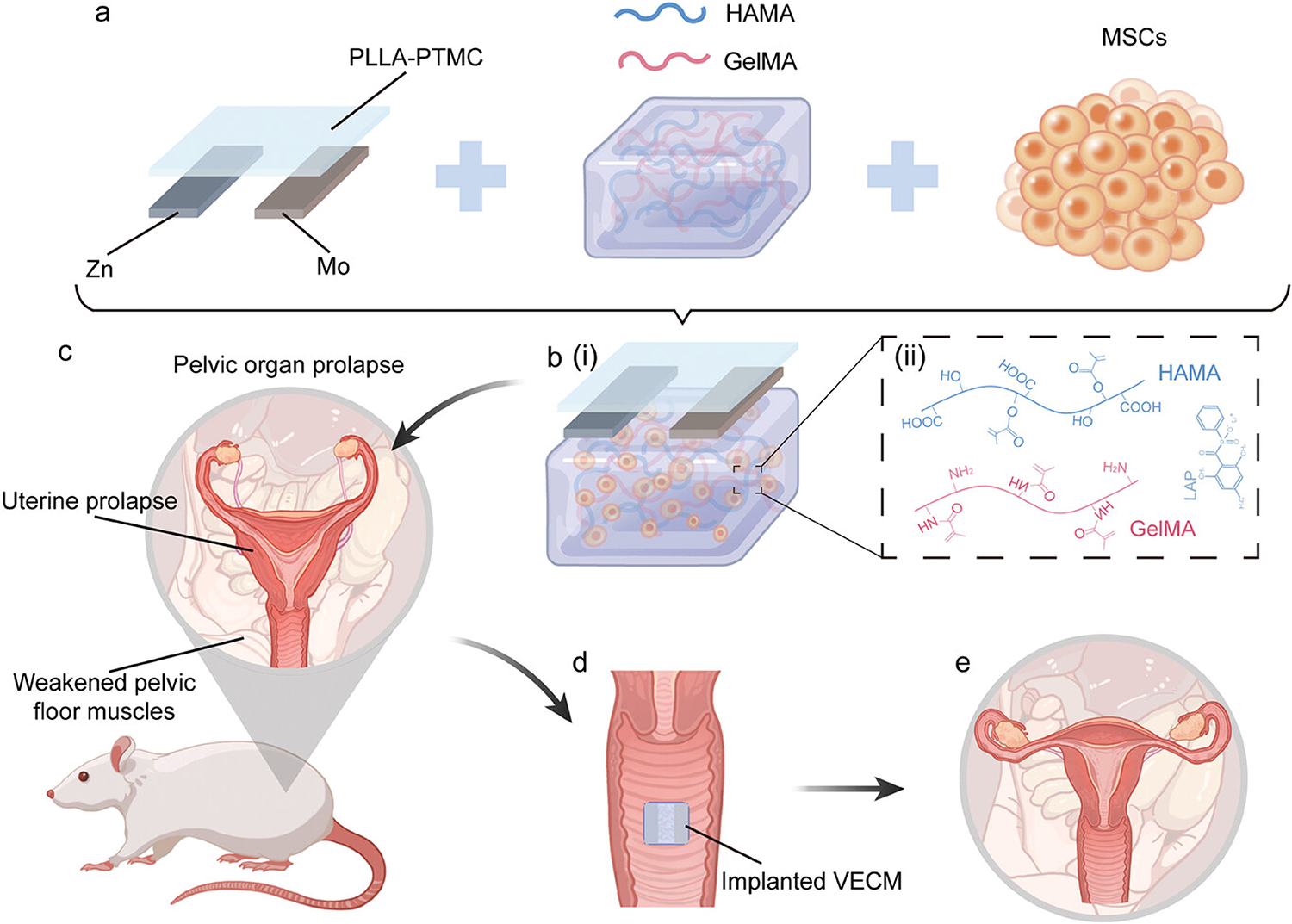
The incorporation of nanoparticles into hydrogels can further enhance their properties. Nanoparticles, particularly silver nanoparticles, have strong antimicrobial properties that can be leveraged to reduce the risk of infections in the postsurgical environment. 103 Nanoparticles can reinforce the hydrogel matrix, improving its mechanical strength and elasticity, which is particularly important for pelvic floor applications. Nanoparticles can be used to load and release therapeutic agents in a controlled manner, promoting tissue healing and regeneration over an extended period. 104 Wen et al. encapsulated MSCs in methacrylated gelatin (GelMA) hydrogels for promoting pelvic tissue repair. 88
Biological effects of hydrogels in POP treatment
Hydrogels play a crucial role in modulating cellular behavior and promoting tissue regeneration in the treatment of POP. They not only provide mechanical support to prolapsed organs but also influence key biological processes such as collagen remodeling, angiogenesis, and cellular differentiation, which are vital for tissue repair. By mimicking the extracellular matrix, hydrogels stimulate fibroblast activity, enhancing collagen deposition and organization, which strengthens the pelvic floor tissues. In addition, hydrogels can promote angiogenesis by releasing bioactive molecules like vascular endothelial growth factor, facilitating new blood vessel formation, and improving nutrient and oxygen supply to the affected tissues. Hydrogels also guide stem cell differentiation, helping progenitor cells become fibroblasts or smooth muscle cells, crucial for effective tissue regeneration. Furthermore, hydrogels can reduce inflammation by releasing anti-inflammatory agents, minimizing cytokine production, and preventing fibrosis, thus fostering a more favorable healing environment. Through these mechanisms, hydrogels offer a multifaceted approach to tissue repair in POP, contributing significantly to both structural support and functional restoration.
Challenges and Future Prospects of Hydrogels
Technical issues in the application of hydrogels
Several challenges remain in their application for POP management, primarily related to material selection, degradability, and long-term effects. Natural polymers have been explored due to their inherent biocompatibility, but they often suffer from low mechanical strength and rapid degradation rates. Conversely, synthetic polymers can offer better mechanical properties but may raise concerns regarding cytotoxicity and biocompatibility. Therefore, achieving a balance between mechanical properties and biological compatibility is key. While controlled biodegradability is beneficial for minimizing long-term complications and the need for surgical removal, an inappropriate degradation rate could either lead to premature loss of support or prolonged degradation, potentially causing chronic inflammation or fibrosis. The degradation process should ideally match the healing time and provide adequate support until the pelvic tissues regain their strength and functionality. Long-term biocompatibility is crucial for the success of hydrogels in POP treatment. Potential long-term effects such as immune responses, fibrosis, or interference with natural tissue regeneration need thorough investigation.
How to optimize hydrogel performance to better meet clinical needs
Hydrogels offer a versatile and promising platform for the treatment of POP. Their applications as coatings for surgical meshes, injectable hydrogels, and composite materials with other biopolymers and nanoparticles have the potential to address some of the limitations of current treatments. The mechanical properties of hydrogels must be finely tuned to mimic the biomechanical behavior of pelvic tissues. The stiffness of hydrogels has been shown to influence cellular behavior, with increased stiffness promoting collagen deposition and inhibiting gel contraction, which are beneficial for tissue repair. Tailoring the stiffness and elasticity of the hydrogel to match the surrounding tissues is crucial for maintaining the correct support for prolapsed organs. Optimizing the stiffness and elasticity of hydrogels is essential for their successful application in POP treatment, as these properties enable the materials to better mimic the native tissue environment, improving their clinical effectiveness. Besides, the degradation rate of hydrogels should be optimized to ensure that they remain intact long enough to provide support during tissue healing and remodeling. Incorporating bioactive molecules that enhance tissue regeneration and remodeling during degradation may also be a promising approach. Functionalizing hydrogels with biological signals or drugs that promote tissue healing could further enhance their therapeutic potential in POP treatment.
Clinical development and translational barriers in hydrogel-based POP treatments
The gap between preclinical research and human applications remains a primary barrier, as animal models do not always predict outcomes in humans due to anatomical and physiological differences. Moreover, the multifactorial nature of POP necessitates personalized hydrogel formulations, which complicates clinical implementation. Regulatory approval is another challenge, as hydrogels must undergo rigorous evaluations to meet safety and efficacy standards. This process can be lengthy, especially for hydrogels with bioactive molecules or those classified as drug-device combinations. Despite these barriers, ongoing human studies and clinical trials are exploring hydrogel-coated meshes, injectable hydrogels, and composite materials for pelvic floor repair. Early-stage trials have shown promising results in reducing complications like mesh erosion and chronic pain, though larger, multicenter studies are needed to validate these findings. 79 The future of hydrogel-based POP treatments depends on overcoming these challenges through improved biomaterial design, regulatory processes, and comprehensive clinical trials to ensure long-term safety and effectiveness.
Future research directions: Personalized treatment and development of multifunctional hydrogels
Each patient’s condition varies in severity, anatomical variations, and tissue responses. Future research should focus on developing personalized hydrogel-based treatments tailored to unique anatomical and physiological needs of an individual. By integrating 3D imaging and advanced biomaterial design, hydrogels could be customized to the specific dimensions and mechanical requirements of each patient’s pelvic region. Personalized approaches could lead to better clinical outcomes, reduced complications, and faster recovery times. To improve both the effectiveness and versatility of hydrogels in POP, future research should explore the development of multifunctional hydrogels. These hydrogels could integrate features such as drug delivery, antimicrobial properties, or even stimuli-responsive behavior. In addition, further investigation into the long-term biocompatibility and mechanisms of tissue integration will be essential to ensure that hydrogels provide durable and effective support over time.
Conclusion
Hydrogels have emerged as a promising therapeutic option for the management of POP, offering advantages in terms of biocompatibility, mechanical properties, and the ability to mimic the natural tissue environment. Through their use as coatings, injectable materials, or composite applications with other materials, hydrogels have demonstrated the potential to provide both structural support and promote tissue regeneration, addressing key challenges in current POP treatments. However, several technical issues still need to be addressed, including optimizing material selection, improving degradation rates, and ensuring long-term biocompatibility. Future developments should focus on customizing hydrogel properties to meet individual patient needs, incorporating multifunctionality such as drug delivery or antimicrobial properties, and enhancing the hydrogel’s performance within the body’s dynamic environment. With personalized treatments, hydrogels hold the potential to significantly improve the clinical outcomes of POP.
Footnotes
Author Disclosure Statement
The authors report no conflicts of interest in this work.
Funding Information
This review was funded by Jilin University 2024 Bethune Project (2024B34) and the Natural Science Foundation of Jilin Province (YDZJ202501ZYTS669).
Authors’ Contribution
H.L.: Conceptualization, methodology, software, writing—original draft preparation; M.J.: Methodology, software; Z.L.: Data curation; D.F.: Visualization, validation; L.F.: Supervision, writing—reviewing and editing.