
Abstract
Urogenital diseases, such as hypospadias, incontinence, urethral obstruction, and pelvic organ prolapse, are common conditions that often require treatments at specialized health care providers. All these conditions can have a negative effect on quality of life, but due to issues of taboo and shame, treatment of urogenital disorders has received less attention and has perhaps undergone less development than desirable. Reconstructive surgery of the lower urinary tract is not without complications, and the functional results may be clinically suboptimal and not meeting with patient expectations. Recent advancements in tissue engineering (TE), material sciences, and disease modeling may create new treatment solutions to diseases of the lower urinary tract. To reach constructive advancement of urogenital TE, we created an interdisciplinary network with European scientists, from different backgrounds and research traditions, to identify knowledge gaps and to stimulate further interactions. In this study, we describe the unmet medical need, the advances in new materials and technologies, and the need for preclinical disease models. We concluded that recent developments offer hope for future treatment options, and with this review, we argue that an interdisciplinary network is essential for the transition from bench to bedside. However, for real progress in the field to manifest, we should further integrate patient representatives, as well as representatives of regulatory bodies.
Impact Statement
The unmet needs in urogenital tissue engineering (TE) are affecting the quality of life for many patients. Interdisciplinary networks are essential for the identification of relevant research and the development of new treatment options. Recognizing and integrating clinical need, the patient’s voice, and the technological advancements are essential for delivering holistic, patient-centered urological and urogynecological care in the future. Integration of regulatory bodies early in our networks is essential to ensure that the TE field is ready to move forward toward treatment options for the ongoing medical challenges in urogenital diseases.
Keywords
Introduction
The need for tissue reconstruction in urogenital diseases is an area of interest in medicine. Current treatments for conditions of the lower urogenital tract such as pelvic organ prolapse (POP), urinary incontinence, urethral strictures, and hypospadias may fail to be successful. For example, conventional treatments for POP range from conservative management to various surgical options aimed at repairing and supporting the prolapsed organs. With surgical interventions using patient native tissue repair (NTR), there is a risk of recurrence and complications. 1 For POP repair involving synthetic transvaginal meshes, surgical treatment recurrence rates may be reduced; however, permanent transvaginal meshes have been associated with severe complications. 2 An example of a method that failed for long-term clinical applications in POP treatment was the use of nondegradable synthetic polypropylene (PPL) meshes. These meshes resulted in high complication rates leading to high morbidity and are therefore now banned by the U.S. Federal Drug Administration (FDA) for this application. 3 Urinary incontinence using midurethral slings leads to complications in 5–10% of patients. 4
In reconstructive surgery for urethral stricture and hypospadias, the main clinical issues are shortage of healthy autologous grafting tissue for the repair and proper postoperative graft vascularization. Moreover, current grafts replace the urethra, but not the surrounding corporal tissue (i.e., the corpus spongiosum). Currently, no autologous tissue grafts are known to sufficiently replace this integral part of the urethra, securing its important function to protect the urethra. Where traditional surgical treatment fails, tissue engineering (TE) and regenerative medicine have emerged as potential solutions to address these issues by combining the body’s own abilities for repair with innovative bioengineering. This approach opens new treatment opportunities in complicated cases with POP, incontinence surgery, and in urethral reconstruction.
One example of a well-recognized application for TE was the development of an engineered urinary bladder in 2006 at the Wake Forest Institute for Regenerative Medicine, involving a decellularized biological scaffold in the first cases and later a synthetic scaffold. 5 Unfortunately, despite initial enthusiasm from both urologists and patients, in a multicenter phase II clinical trial, the cell-seeded biodegradable scaffold failed to significantly improve bladder function. 6 In addition, serious adverse effects were encountered, surpassing acceptable safety standards and leading to preliminary trial termination, with all patients needing rediversion. 7
Before TE of the bladder can become a future reality, preclinical long-term studies in diseased animal models, simulating human pathophysiology, must be conducted to determine optimal replacement methods.8,9 A major challenge in TE is the understanding of key properties related to native human tissues. A comprehensive understanding of the native tissue structure and function is essential for successful outcomes, serving as the foundation for developing implants and grafts by TE that can effectively mimic the properties of the targeted organs, thereby reducing the risk of complications and improving overall treatment efficacy. In the case of PPL meshes for POP surgery, the properties of the first-generation mesh implants did not match the properties of the native tissue, as they were dense and mechanically stiffer than the vaginal tissue, and these factors consequently led to serious complications such as erosion and pain. 3 Furthermore, regulatory authorities from the FDA and the European Medicines Agency (EMA) have set the standards for good manufacturing products (GMPs) in TE to the level of pharmaceutics manufacturing, which clearly restricts its implementation to common clinical practice even further.10,11
In response to these challenges in advancing new treatments for lower urogenital diseases, our workshop aimed to bring together diverse stakeholders, including patient representatives, clinicians involved with reconstructive surgery, and basic scientists within the field of regenerative medicine, to constructively move from the failed application of biomaterials in urogenital diseases toward a path of successful applications of novel technologies by formulating a consensus statement to align our future research agendas in the direction of our common goals. The aim of this narrative review was to present the outcomes and experiences from an interdisciplinary workshop focusing on urogenital TE.
Interdisciplinary networking
During the workshop “Urogenital Tissue Engineering from bedside to bench and back: What do clinicians need and what has basic science to offer,” key themes for regeneration and treatment of urogenital diseases were discussed. The event was sponsored by the European Reference Network (ERN) and the European Joint Programme on Rare Diseases (EJP RD) and hosted by the Regenerative Medicine Center of Utrecht Medical University in the Netherlands, during September 4–5, 2023. 12 Participants were invited via the aforementioned organizations, forming a think tank consisting of individuals from different backgrounds and research traditions, including clinicians (specialized in gynecology, pediatric surgery, pediatric urology, and urology), tissue engineers, material scientists, chemists, animal model researchers, and molecular cell biologists. Patient representatives from the World Federation of Incontinence and Pelvic Problems (WFIPP) were also invited and they took part in the discussions, whereas male patients with urethral disease (such as hypospadias or strictures) were not represented but will be invited via the European Reference Network for rare urogenital diseases and complex conditions (ERN eUROGEN) registries and integrated in future meetings.
To enhance familiarity among participants, we began with an informal speed-dating session. Subsequently, lectures were given on novel technologies currently being developed in the field of regenerative medicine on the advantages and limitations of various disease models, unmet clinical needs, and the implementations and importance of patient involvement. Roundtable discussions were organized to identify knowledge gaps and stimulate interactions between the different specialties. As a starting point, we decided to limit our discussions to the clinical problems specifically related to urethral reconstructive surgery and POP. Our goal was to translate information from scientific research findings and outcomes to clinical experience and vice versa, thereby translating clinical experience to formulate scientific questions for laboratory-based researchers. Therefore, we finally summarized our conclusions and common statements by written communications within the working group. Below we report our outcome organized by topic.
The unmet need in urogynecology
POP is a prevalent problem, with about 40% of all women experiencing some kind of POP in their lifetime, involving symptoms of bulge, impaired micturition, defecation, sexual function, as well as psychosocial problems. 13 Of these women, 10–20% will undergo POP repair surgery, and subsequently, 20–40% will later undergo surgery again for recurrent POP. 14 The relatively high rates of recurrence after NTR have been frustrating for patients and gynecologists and we can foresee that; since the population ages rise and as women of higher age are more active, a growing number of women will seek care for POP in the future. This number may increase even more, as the existing taboos on POP and its associated symptoms decrease and expectations of health care increase. However, a shortage of health care professionals in Western countries is approaching, resulting in more women seeking care from relatively fewer professionals. 15
Preventing the occurrence of POP is a key goal. An important factor contributing to the development of POP is the damage caused during vaginal childbirth. Preventive measurements during delivery and innovative postdelivery treatments, such as stem cells or exogenic factors extracted from stem cell conditioned medium, could potentially reduce POP incidence. 16 Furthermore, a clinically recognized current praxis is to strengthen the weakened native pelvic diaphragm (supportive smooth muscle tissue), which is sutured back together during POP surgery to prevent recurrence. This desire to add additional supportive material was previously evident by the adoption of the PPL meshes for POP surgery from 2004 to 2012. 17 Although most of these meshes had not been tested in animal models, no legal restrictions prohibited human application despite limited knowledge on the mesh behavior in vivo. However, the initial PPL meshes were adopted from hernia repair, and the properties of these meshes, including their structure, size, being nondegradable, and location (migration over time), resulted in unacceptably high complication rates when implanted vaginally. These complications included mesh exposure into the vagina or erosion into other pelvic structures, such as the bladder or bowel, tissue ingrowth, as well as mesh shrinkage, leading to pain, bleeding, and/or infection. Consequently, these meshes were banned in several countries 3 or restricted to clinical trials, leaving an unsolved clinical problem and many women, who needed reoperation, untreated. Given these challenges, a pertinent need exists for better solutions, based on robust research and evidence, and encouraging innovation and rigorous clinical trials can help develop safer and more durable treatments for POP.
The unmet need in urethral reconstruction
The male urethra transports urine from the bladder, through the prostate, to the meatus at the top of the penis. Furthermore, during sexual activity, the urethra also transports semen from the seminal ducts entering the prostate. Hypospadias, a common congenital urethral anomaly, has seen an increase in prevalence and often requires complex reconstructive surgery. Some 5–10% of patients with hypospadias present with a severe form, requiring intricate and often repeated surgical interventions using autologous flaps or grafts. 18 In these cases, donor side morbidity and shortage of healthy, well-vascularized tissue may lead to undesired results. 19 Another common disease of the urethra is the presence of a urethral stricture. Strictures can happen at any point from the bladder to the tip of the penis, highest prevalence is in the bulbar region. 20 Common causes are trauma to the urethra, damage from endoscopic treatment, or infection such as sexually transmitted infections or lichen sclerosus. In many cases, no cause can be found.
Addressing the complex needs of urethroplasty requires a dual-perspective approach, encompassing both the clinician’s focus on restoring urethral function and the patient’s broader concerns, including cosmesis, sexual function, and psychological well-being. When native autologous tissue is insufficient, TE strategies may offer a solution to the challenges of urethral reconstruction. These challenges not only include creating a scaffold that replicates the distinct structure of the urethra but also ensures robust graft vascularization and long-term functionality within the host body, hereby preventing stricture formation. The promise of tissue-engineered urethras lies in their potential to provide a more compatible (i.e., potentially offering better integration and reduced fibrosis compared with conventional nondegradable synthetic grafts), less invasive, and long-term durable alternative to traditional grafts, which often fail due to fibrosis and poor integration. 21
Traditional measures of success, such as unobstructed urinary flow and the absence of infection, are crucial yet insufficient, as they fail to address the entirety of the patient’s experience postreconstruction. For patients, the psychological impact of the surgery, potential impairment of sexual performance, and the cosmetic appearance of the genitalia significantly influence their quality of life.18,22–24 Altogether, definitions of success vary among stakeholders—including researchers, surgeons, regulators, and patients—emphasizing the importance of integrating patient-reported outcome measures (PROMs) to bridge this gap.
Development of new biomaterials
The ideal material for urogenital reconstructive surgery should allow for tissue regeneration, extracellular matrix (ECM) production, neo-angiogenesis, and cell ingrowth.25,26 Importantly, the material should in addition be mechanically compliant with the target tissue. As an example, for application on the pelvic floor, a biomaterial should be elastic to cope with the increased abdominal pressure during coughing and sneezing. 27
As a result of the growing safety concerns, current TE approaches focus on degradable materials for pelvic repair.28–30 Tissue-engineered synthetic degradable materials can eliminate or limit adverse events and may outperform unmodified synthetic or natural materials in terms of biomechanics and host response. For example, polylactic acid (PLA) was compared with cadaveric dermis, porcine dermis, PPL, and porcine small intestinal submucosa to assess the suitability as a bladder neck sling for stress urinary incontinence (SUI) surgery. PLA exhibited the greatest increase in metabolic activity in terms of cell proliferation and collagen and elastin production compared with the other materials. 31 In another promising example, degradable silk fibroin scaffolds seeded with adipose-derived stem cells (ADSCs) were implanted into mice, and PPL was used as a control. 32 The silk scaffold showed favorable production of collagen and resulted in a comparable elastic modulus to native tissue. In another study on murine pelvic floor reconstruction, poly(lactic-co-glycolic acid) scaffolds reseeded with ADSCs resulted in collagen-abundant tissue regeneration convincingly mimicking native fascia. 33 Altogether, synthetic tissue-engineered degradable materials show promising results based on in vitro and in vivo small-animal studies; however, for further advancement toward clinical translation, future research is required to focus more on large animal studies and human trials.
Recently, another novel material based on polyisocyanide (PIC) hydrogels has been studied for application in the pelvic area. PIC hydrogels are synthetic yet strongly biomimetic hydrogels. In addition, PIC gels are thermosensitive (i.e., they switch from aqueous solution to a hydrogel form at temperatures above 15°C), which allows for minimally invasive applications through injection. 34 PIC gels reproduce many of the architectural and mechanical properties of ECM proteins, such as collagen and fibrin, but their synthetic nature makes them highly tailorable to various applications. 35 Furthermore, PIC gels stimulate cell proliferation and collagen deposition in vitro.36,37 The first in vivo results revealed how PIC gels demonstrate favorable characteristics in reducing certain factors linked to poor wound healing outcomes in NTR following POP, 38 and the results mimic the 2D and 3D in vitro studies where the same PIC gels were used as a tunable matrix for improved disease models. 36 Considering the initially successful application in POP, we expect that PIC gels may find similar applications in the treatment of SUI. As previously mentioned, biomechanical properties must match those of native tissues to ensure biomimetic performance. As a reference, biomechanical properties from human urogenital organs relevant to the scope of this article are provided in Table 1.39–41 Furthermore, a selected overview of additional promising biomaterials suitable for lower genitourinary repairs has been compiled in Table 2.42–74
Overview of Biomechanical Properties of Human Lower Urogenital Organ Tissues
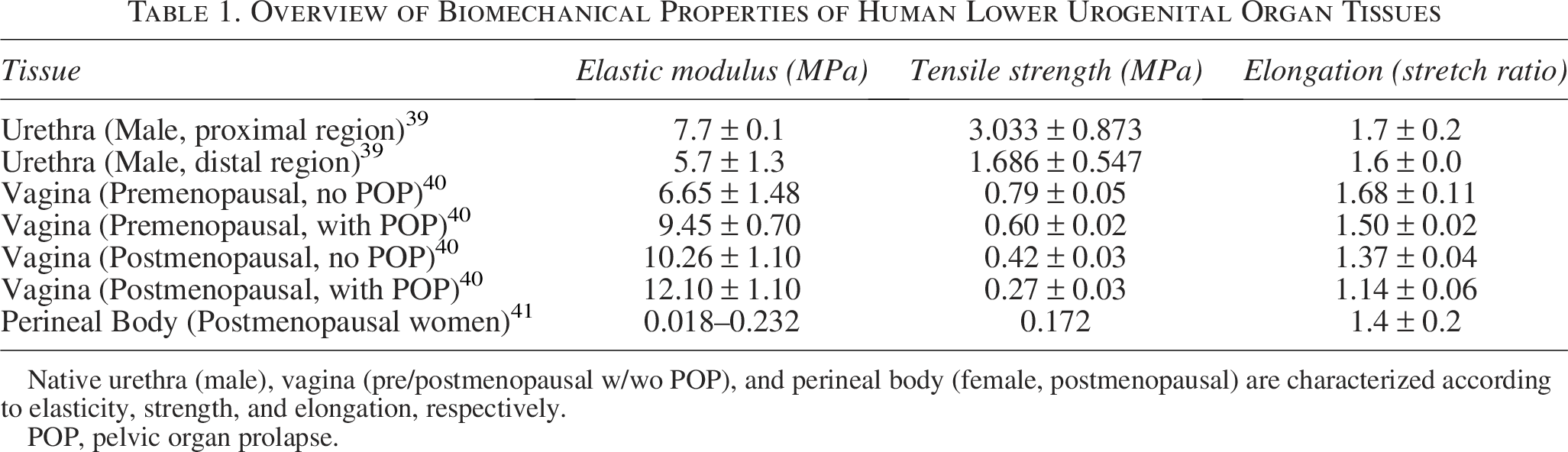
Native urethra (male), vagina (pre/postmenopausal w/wo POP), and perineal body (female, postmenopausal) are characterized according to elasticity, strength, and elongation, respectively.
POP, pelvic organ prolapse.
Overview of Potential Biomaterials Relevant to Lower Urogenital Tissue Engineering
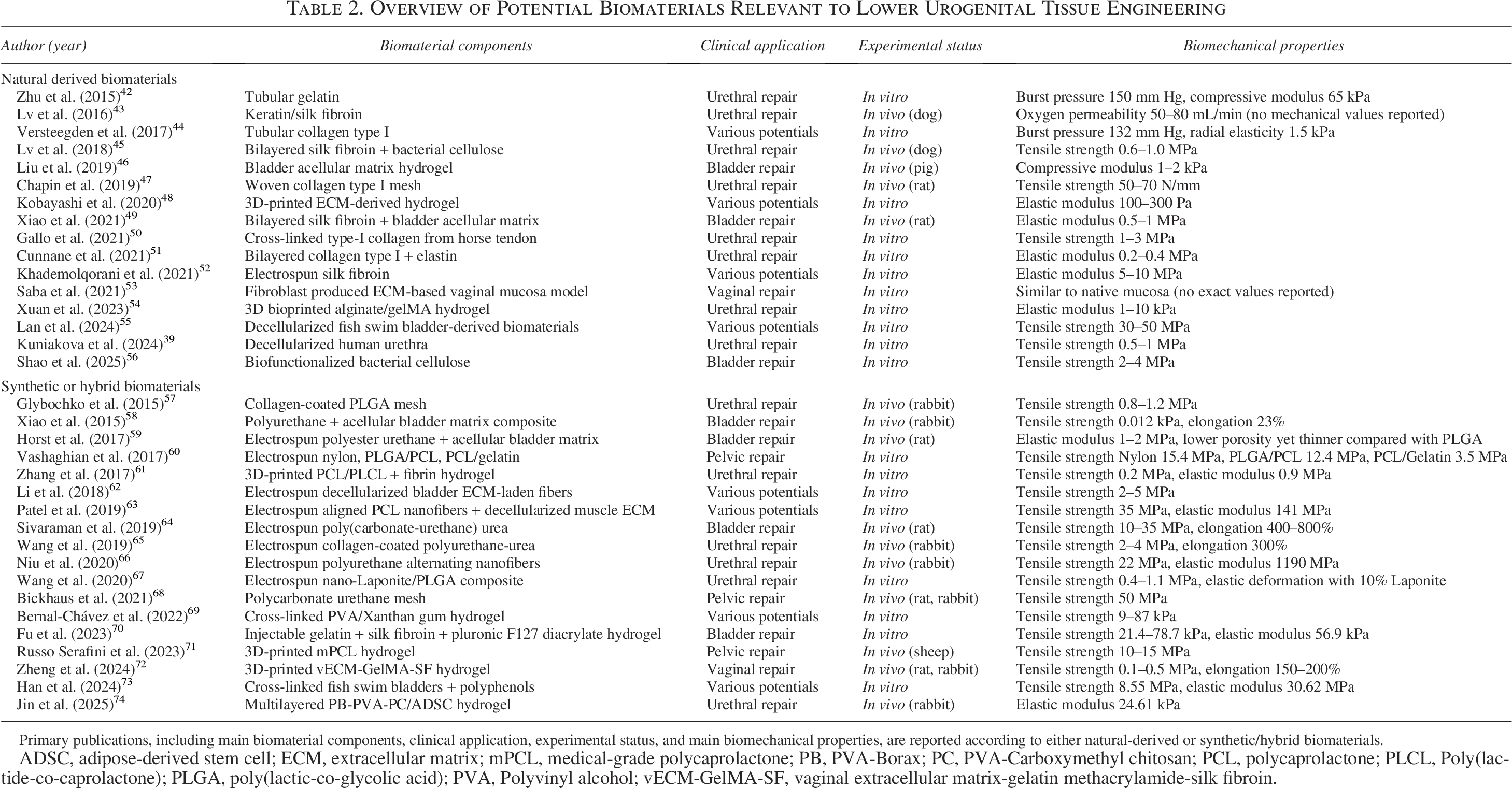
Primary publications, including main biomaterial components, clinical application, experimental status, and main biomechanical properties, are reported according to either natural-derived or synthetic/hybrid biomaterials.
ADSC, adipose-derived stem cell; ECM, extracellular matrix; mPCL, medical-grade polycaprolactone; PB, PVA-Borax; PC, PVA-Carboxymethyl chitosan; PCL, polycaprolactone; PLCL, Poly(lactide-co-caprolactone); PLGA, poly(lactic-co-glycolic acid); PVA, Polyvinyl alcohol; vECM-GelMA-SF, vaginal extracellular matrix-gelatin methacrylamide-silk fibroin.
Appropriate disease models
The use of animals in translational research remains controversial, but is still required by regulatory authorities for the approval of many medical devices or drugs. Their use must always meet several requirements as follows: use the minimum number of animals; involve animals with the lowest capacity to experience pain; and cause the least suffering, distress, or lasting harm. The choice of animal model will therefore be a balance between anatomical fidelity and discrimination to meet the above requirements. 75 Unfortunately, human urogenital anatomy differs from most model animals. There is no ideal animal model that can simulate all human features. Therefore, we must choose the animal species depending on the mechanism of action, which we intend to investigate. Based on common practice, the animal models described in the following section are rodents, rabbits, pigs, and sheep. Mice and rats are substantially similar to humans regarding embryological, cellular, and molecular biology features. Their main advantages include low cost, availability, easy handling and management, available transgenic mice, and the possibility to use animals from the same litter to reduce the genetic noise. The drawbacks of rodents are small size, highly concentrated urine, differing penile anatomy, no vaginal birth trauma, and, most importantly, general differences in immune response from humans. Rabbits are more similar to humans in the sense that males lack a penile bone and females have a proportionally large vagina. They usually serve to bridge the gap between rodents and larger animals. Larger animals often allow for a better translation into a clinically relevant human scenario. The EMA, the FDA, and the International Society for Stem Cell Research recommend the use of large animal models to evaluate efficacy, creation of a critical size defect, durability, dose–response, degradation, and safety of advanced therapeutic medicinal products. 76 In this regard, pigs and sheep show anatomical and physiological similarities, useful for chronic studies. For example, the size and physiology of the pig organs are very similar to humans. Pigs and humans have comparable systemic and mucosal immune responses, with up to 80% of similarity in the immune system, highly in contrast to only 10% in mice. 77
The rabbit model is the most common animal model for the study of urethroplasty techniques, due to its anatomical characteristics, yet an ideal animal model resembling human congenital urethral defects remains to be established. 78 Sheep and pig models offer a platform for testing the biocompatibility, functionality, and integration of engineered tissues for the pelvic floor and the urethra before considering clinical trials in humans.79,80
Current in vitro disease modeling using organ-on-a-chip technology could in some respects propose a viable alternative to animal models. 81 However, to obtain essential data on the safety and effectiveness of new TE methods, it remains crucial at some point to progress to studies involving large animal models, to guide improvements and ensure the intended grafts function when eventually applied for human use.
Veterinary research
Besides animal disease models, we can also learn from veterinary medicine, for example, in dogs. Years of selective breeding during domestication of canines tremendously reduced genetic heterogeneity within breed populations, making them magnifying glasses for genetic disorders. 82 Different diseases occur in extraordinarily high prevalence within specific breeds selected for phenotypic extremes. Selective breeding has also resulted in an increased prevalence of more complex genetic disorders, including urogenital disorders like ectopic ureters, 83 hypospadias, 84 and urothelial cancer. 85 These underestimated yet naturally occurring canine veterinary-patient populations have the potential to function as human preclinical models. Aligned with the societal call to decrease reliance on animal models, utilizing animal patients for the development of therapeutic interventions can fulfill a dual purpose as follows: providing remedies for both humans and pets while concurrently lessening the use of experimental animals.
Recent advancements in TE methods
A variety of existing methods are currently being applied to create tissue substitutes in the field of urogenital TE. 86 Most often, these methods include an expansion of donor cells ex vivo, to obtain sufficient cell numbers, which are then combined with suitable biomaterials to form tridimensional substitutes. The purpose of these strategies is to mimic the histological architecture of native tissue ex vivo before transplantation back into the patient. In addition, the biomechanics of the native tissue need to be met. Therefore, studying the native tissue is of specific importance before further developing new strategies for TE organ reconstruction.87–89
Micrografting, involving the autotransplantation of small skin or tissue fragments to promote regeneration, has emerged as a low-tech yet effective and autologous technique within the broader TE spectrum.90–93 Within urogenital tissue reconstruction, micrografting has been studied in preclinical animal models, as a single-staged surgical procedure for the creation of urinary conduits aimed at urinary diversion and recently also for vaginal reconstruction.94–99 Importantly, this method circumvents the high costs and stringent regulatory requirements associated with ex vivo-expanded cell products, including reduced GMP-related barriers, a shorter time to implantation, and greater clinical accessibility. While less complex than other biofabrication methods, micrografting complements advanced strategies by offering immediate clinical utility, especially in wound healing, and exemplifies the continuum of solutions being developed to address varying clinical needs in regenerative medicine.
On the other end of the spectrum, recent advances in the introduction of 3D bioprinting technologies have been particularly transformative in urogenital TE. 3D bioprinting enables precise spatial deposition of cells and biomaterials to recreate complex tissue architectures, offering high customization and scalability; using biocompatible materials, often in combination with cells, 3D bioprinting allows for a high precision in the construction of a complex and biomimetic scaffold ultrastructure, providing new opportunities for creating advanced templates for tissue growth. These scaffolds can be designed to degrade over time, leaving behind only the newly formed tissue integrating with the body.100,101 However, challenges remain in achieving full vascularization and mechanical stability in large constructs. Furthermore, there are unfortunately no current harmonized standards or regulatory frameworks from the FDA or EMA, applying specifically to 3D printing or bioprinting, for use in medical devices or in the TE environment. As such, innovation is currently moving faster than the U.S. and European Union regulators. In contrast, scaffold-free cell sheet technologies (e.g., MukoCell©) preserve cell–cell junctions and native ECM, promoting better integration and functionality upon transplantation. 102 These solutions are generally limited to thinner tissues due to lack of structural support, limiting their use in the reconstruction of load-bearing organs.
Recent advancements and translation to the clinic (see below) lead to a dynamic timeline visualized in Figure 1, based on Seyhan et al. 103
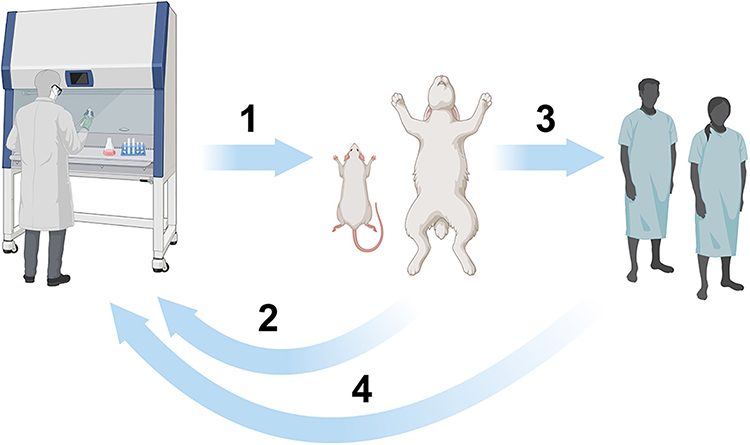
Visual representation of the timeline toward application of tissue engineering. In vitro experiments (left) precede preclinical trials. Hurdles in this step are ethical approval for animal experiments; go/no-go decisions on biocompatibility of the grafts generated in vitro need to be made beforehand, as well as the biomechanical properties, as these should match the properties of the native tissues (arrow 1). If the grafts are rejected in the animals or cause adverse events, in vitro redesigning is required (arrow 2). Only if preclinical trials are successful, research proceeds in phase 1 trials in humans. Hurdles include ethical approval and registration, which are still in development for these complex grafts, and the financing of translation to patients. If the clinical phase 1 trial fails, in vitro redesigning is required (arrow 4).
Translation to the clinic
In common, most of the developments in urogenital TE face significant regulatory hurdles, as the rigorous process for Advanced Therapy Medicinal Products (ATMPs), particularly under the EMA in Europe, demands comprehensive clinical evidence and standardized manufacturing practices. 104 Regulatory approval of ATMPs varies significantly between the FDA and the EMA as follows: the FDA oversees ATMPs primarily through the Center for Biologics Evaluation and Research with mechanisms like the Breakthrough Therapy and Regenerative Medicine Advanced Therapy designations, whereas the EMA regulates them via the Committee for Advanced Therapies under a centralized procedure with incentives such as Priority Medicines status. These regulatory frameworks directly influence time to market and innovation by offering accelerated pathways, enhanced scientific advice, and financial incentives, which reduce development timelines and encourage investment in cutting-edge therapies, although regional differences in requirements and review processes can still create strategic complexity for global developers.
Moreover, clinical implementation of new technologies needs to take place in concert with patients’ advocacy groups to procure patient involvement and adequate measurements of success. Long-term clinical follow-up studies reveal that various outcomes for patients with adult hypospadias and urethral stricture, including a lower penile perception score, increased lower urinary tract symptoms, weaker urinary flow, and dissatisfaction with sexual life, indicate an ongoing demand for improved supportive care. Furthermore, psychological assessments highlight the cognitive and gender-role alignment with controls, yet semi-structured interviews uncover patients’ uncertainties about their condition, suggesting a need for accessible information and ownership of their own narrative. 105 A regular dialog should align TE innovations with ATMP regulations early in development, and potential timepoints for patient involvement could include focus-group interviews at early proof-of-concept stages, preclinical study design, and later scientific advice meetings. Finally, PROMs are invaluable in capturing the patient’s perspective on urinary function, cosmesis, and sexual health, promoting and ensuring a patient-centered approach.22,105
Broader implications for TE beyond the urogenital organs
Although the focus of our workshop was on the lower genitourinary tract, our interdisciplinary approach of inviting clinicians, basic scientists, and patient representatives lead to important insights extending beyond this anatomical region. This approach enables for the creation of clinically relevant, biologically grounded, and patient-centered tissue engineered therapies in the era of personalized medicine.
Clinicians contributed to translational relevance—the real-world patient needs and the practical details concerning anatomically implantable grafts. Their experience guided the discussion toward how to achieve practical outcomes. Basic scientists enriched the discussion by providing the molecular, cellular, and biomechanical understanding essential for creating functional tissues and in vitro models, such as organoids and organs-on-chip, as tools that help identify functional biological models. The inclusion of patient representatives was crucial to understand real-life experiences. The patient perspective, the insights on what is patient quality of life, esthetics, long-term integration, and personal values. The stakeholders, represented by the patient (representatives), clinicians, and basic scientists define the problem. Experiments and ultimately (pre)clinical trials redefine the problem and create new experimental ideas. The prototypes for grafts and solutions feed back into the project and the experiments. This entire nonlinear process is conceptualized in Figure 2, adopted from the design thinking process previously described by Lewis et al., which has mainly been used in education and social sciences. 106
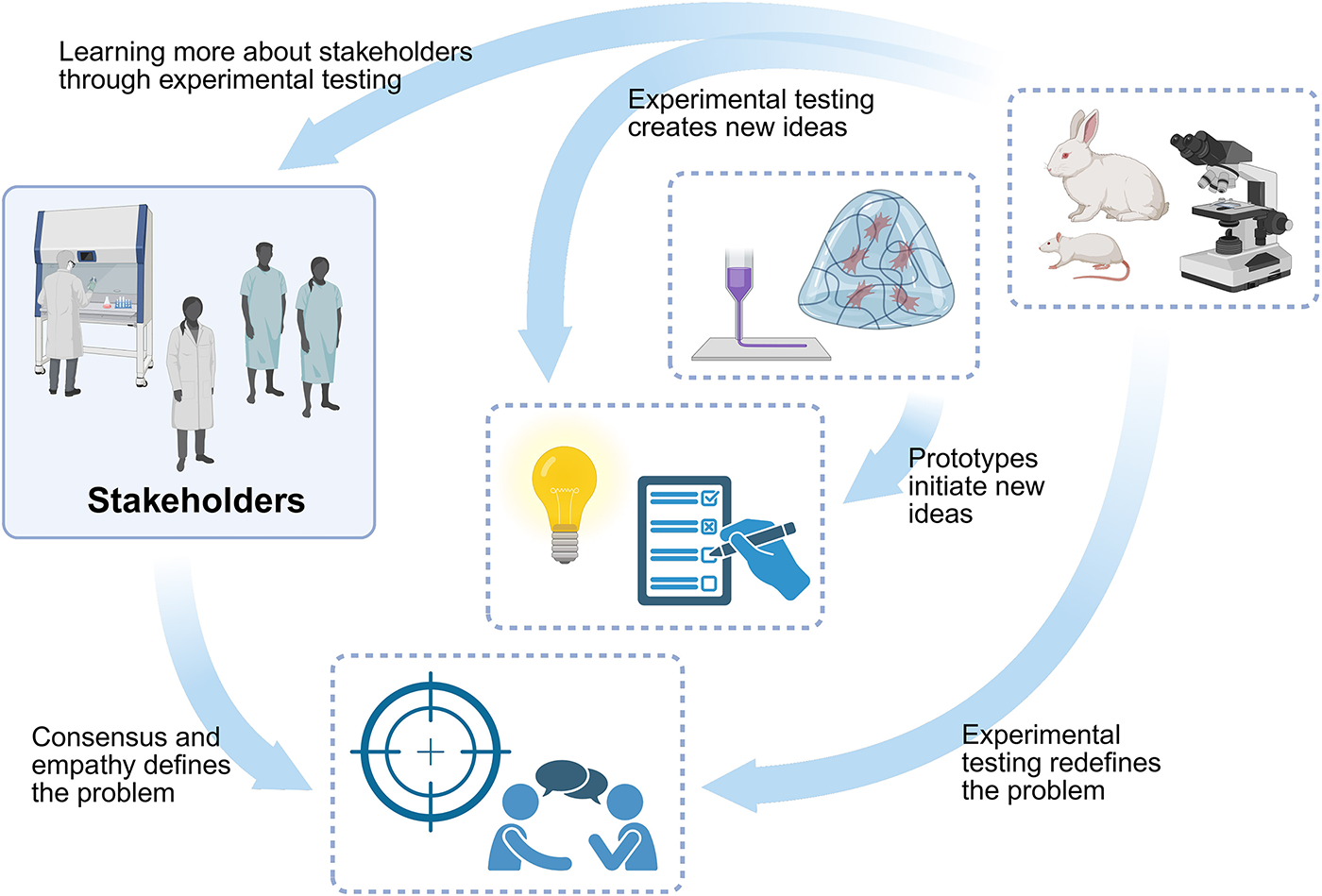
Visual representation of the process toward consensus. The stakeholders, specifically patient (representatives), clinicians, and basic scientists, define the problem. Experiments and ultimately (pre)clinical trials redefine the problem and create new ideas for the project. The prototypes for grafts and solutions feed back into the project and the experiments. The process is adapted for this context based on The Design Thinking Process mainly used in education and social sciences.
Ultimately, this interdisciplinary collaboration, patient-centered metrics, and preclinical model optimization offer a transferable framework for translational success in many TE fields, such as dermatology and in orthopedic, vascular, or gastrointestinal regeneration.
Conclusions
The unmet needs in urogenital TE, from both clinical and patient perspectives, range from functional voiding to esthetic and psychological consequences, whereas future treatment innovations entail navigating a complex regulatory landscape. New materials and technologies offer hope for future treatment options. Recognizing and integrating these factors into clinical practice is essential for delivering holistic, patient-centered urological and urogynecology care in the future. Creating interdisciplinary networks is essential for the identification of relevant research and development targets. The patients’ voice needs to be integrated further. Future meetings should involve representatives of the regulatory bodies to ensure that the TE field has matured and is ready to move forward toward treatment options for the ongoing medical challenges in patients with urogenital disease.
Authors’ Contributions
Drafting of the article: All the authors. Editing of the article: C.I.C., N.J., and P.D.G. Conceptualization, funding, and correspondence: P.D.G. Figures: P.D.G. Tables: C.I.C.
Footnotes
Acknowledgment
The authors acknowledge WFIPP.
Funding Information
HORIZON EUROPE Marie Sklodowska-Curie Actions: EJP RD COFUND-EJP N° 825575.
Disclosure Statement
C.I.C., N.J., K.B., T.O.E., M.F., L.d.K., M.W., and P.d.G. are employees of Healthcare Providers that are Full Members of ERN eUROGEN, the European Reference Network for Rare Urogenital Diseases and Complex Conditions. ERN eUROGEN is funded by the European Commission.