
Abstract
The tendon–bone interface (TBI) possesses a highly intricate structure, making complete restoration of its native structure postinjury particularly challenging, which often leads to suboptimal healing outcomes. Metal ions, such as calcium (Ca2+), magnesium (Mg2+), zinc (Zn2+), copper (Cu2+), cobalt (Co2+), strontium (Sr2+), iron (Fe2+/Fe3+), and lithium (Li+), have attached significant attention in tissue regeneration research owing to the excellent roles in promoting angiogenesis, osteogenesis, and chondrogenesis. This review systematically elucidates a comprehensive overview of the current understanding of these bioactive ions’ mechanisms and their applications in TBI repair. Additionally, the review highlights the importance of incorporating metal ions into biomaterial scaffolds to enhance simultaneous multitissue regeneration while addressing current therapeutic limitations in TBI management. Finally, the review outlines future research directions for optimizing ion-based biomaterial strategies to advance TBI treatment paradigms.
Impact Statement
The tendon-bone interface (TBI) repair is challenging due to the structural complexity. While a lot of research has focused on restoring TBI functionally and structurally, there is no good strategy to achieve its complete repair. Metal ions play certain roles in promoting the repair of TBI. Therefore, this paper discussed the role of metal ions and materials applied to the TBI in the repair process and related mechanisms, aiming to provide reference for subsequent studies.
Introduction
The tendon–bone interface (TBI), a specialized transitional zone comprising four distinct yet continuous regions: fibrous, uncalcified and calcified fibrocartilage, and bone, plays a critical biomechanical role in completing complex movements and dissipating stress concentrations.1–4 Although traditional surgical reconstruction has remained the gold-standard treatment for TBI injury via simply fixing tendons or ligaments to bone for decades, it is difficult to achieve satisfactory therapeutic effect after anterior cruciate ligament (ACL) injury and rotator cuff tear (RCT). 5 Postoperative healing typically results in disorganized fibrous scar rather than the native TBI’s hierarchical architecture, significantly increasing the risk of reinjury.6,7 Consequently, impaired TBI healing, characterized by chronic pain and restricted mobility, is the major contributor to surgical failure.8,9 To address these limitations, other strategies have been developed to promote TBI healing in preclinical models and early-phase clinical trials, such as hydrogel, 10 exosomes, 11 bioprinting, 12 bioscaffolds,13,14 and mesenchymal stem cell (MSC)-based therapies15,16 (Table 1). However, achieving functional and biological tendon–bone regeneration is challenging because of the TBI’s inherently poor regenerative capacity. Those studies indicate that bioactive ions play key roles in restoring the native structural and compositional properties of the TBI.17,18 Notably, an increasing number of metal ions are gradually incorporated into tissue-engineered biomaterials and synthetic scaffolds to promote tendon–bone healing, including Ca2, Mg2+, Zn2+, and Cu2+.19–21 On one hand, ions can regulate bone regeneration by regulating osteogenic differentiation and osteoclastic resorption activities, such as Ca2+, Cu2+, and Ag2+. Notably, Cu2+ exhibits dual functionality: it induces collagen maturation while upregulating vascular endothelial growth factor (VEGF) expression to stimulate neovascularization.22,23 On the other hand, Mg2+ can not only promote fibrocartilage regeneration by recruiting MSCs to TBI and induce their differentiation into chondrocytes24,25 but also inhibit the early inflammatory response through AKT serine/threonine kinase 1-mediated polarization of M2 macrophages, thereby enhancing fibrochondrocyte differentiation of human bone MSCs. 26 Additionally, Zn2+ possesses antimicrobial effect by inducing bacterial reactive oxygen species production.27,28 Zn2+ stimulates fibroblasts to secrete collagen I and reduces tendon scar formation 29 and suppresses iNOS-mediated reactive nitrogen species (RNS) production via inhibition of M1 macrophage polarization 30 and suppression of iNOS-mediated RNS production via inhibition of M1 macrophage polarization. To maximize therapeutic efficiency, advanced delivery systems releasing bioactive ions into gradient structure are required to achieve spatiotemporal control over ion release for synchronized tissue regeneration. 14
Comparison of Various Strategies
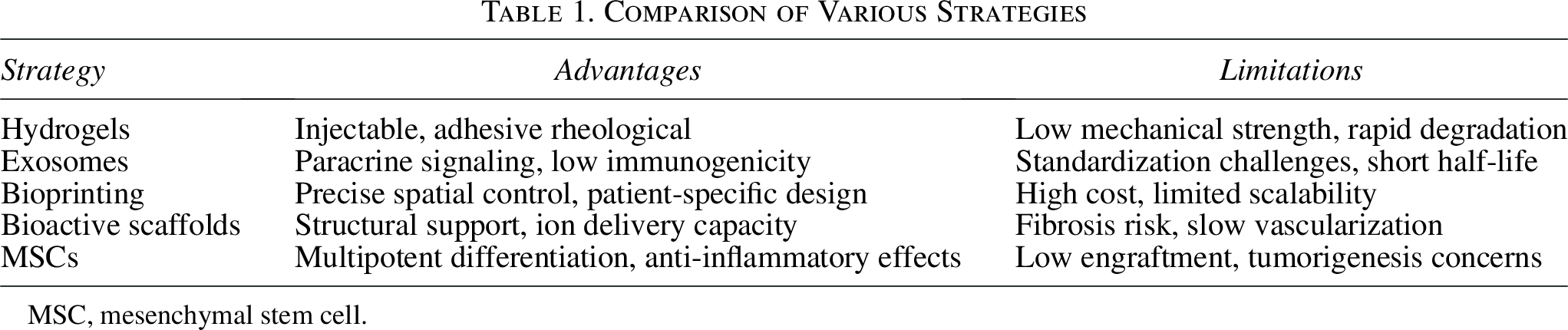
MSC, mesenchymal stem cell.
This review critically evaluates recent progress in the development and application of ion-incorporated biomaterials for TBI regeneration, with particular emphasis on the underlying therapeutic mechanisms and translational potential.
Application of Various Ions in TBI Healing
Calcium (Ca)
Calcium (Ca) is one of the most abundant inorganic elements in the human body, with approximately 99% stored as hydroxyapatite ([Ca10(PO4)6(OH)2], HA)—the primary component of bone, and a small fraction existing as amorphous calcium phosphate ([Ca2P2O7], ACP). 31 In the TBI, Ca is localized in the calcified fibrocartilage and bone regions, with a well-defined mineralization front demarcating the transition between nonmineralized and mineralized interface regions.32,33 Qu et al. found that elevated Ca levels in calcification solution-treated tendons promote tendon calcification and bone formation. 34 Due to their structural support and osteoinductive properties, various calcium-containing synthetic grafts (e.g., calcium phosphate [CaP], HA, β-tricalcium phosphate, and calcium carbonate), as same as autografts, are increasingly utilized in tendon–bone repair. 35
Calcium phosphate
CaP material is extensively adopted in clinical orthopedic surgeons owing to the compositional similarity to native bone and excellent osteogenic ability, which enhance tendon–bone healing.36–38 A research demonstrates that CaP-based augmentation at the tendon–bone repair site facilitates early postoperative bone formation, fibrocartilage regeneration, and improved collagen organization in rotator cuff repairs. 39 Research further showed that the CaP-hybridized tendon grafts enhance knee healing by promoting cartilage layer and new bone formation during the TBI healing. 40 Mechanistically, CaP not only increases local calcium ion concentration to accelerate bone regeneration but also modulates cellular activity by stimulating osteoblasts while suppressing osteoclasts in the TBI.41,42 However, hybridization of CaP to the tendon grafts via alternate soaking enhanced tendon–bone healing by osteogenic activity in a goat ACL model, promoting new bone regeneration, yet it failed to restore native joint laxity or tendon loading capacity, suggesting that bone regeneration alone is insufficient for functional recovery. 43 In contrast, early time after RCT repair, Ca5(PO4)2SiO4 (CPS), a CaP-based bioceramic, not only improved tendon–bone insertion via osteogenic activity at the interface but also significantly expanded the fibrocartilage area while suppressing fibrous tissue formation, thereby reconstructing the native laxity and the biomechanical properties of the TBI. 44 These differential effects may be attributed to silicon, a component of CPS bioceramic, which serve dual roles: (1) as a bioactive sites facilitating bonelike apatite by Ca2+ and phosphorus ion recruitment and (2) as a structural scaffold creating a favorable microenvironment for fibrochondrocyte proliferation and extracellular matrix (ECM) deposition. 45 Collectively, these results suggest that restoring biomechanical stability and structural integrity is critical for TBI healing. Further studies should focus on how to restore the function of TBI, involved in contributing to the synchronous formation of osteogenesis, chondrogenesis, and tendon.
Amorphous calcium phosphate
ACP, a precursor of bone minerals, constitutes the primary inorganic phase in biomineralization. 46 During early biomineralization, matrix vesicles secreted by osteoblasts accumulate Ca and P, acting as precursors for ACP, which subsequently deposits into collagen. 47 Additionally mineralization tendon could induce osteogenic differentiation of MSCs. 48 The osteogenic properties of ACP scaffolds stem from their ability to modulate extracellular Ca2+ and P concentrations in MSCs, either through Ras/Raf/Erk-dependent signaling pathways or ATP-adenosine regulatory mechanisms.47,49 During the process of TBI healing, the physical forms of ACP influence its functional outcomes. Research shows that the ACP nanoparticles exhibit dual osteogenic and angiogenic activity in vitro, enhancing tendon–bone integration, through the regeneration of a functional fibrocartilaginous transition zone and promoting tendon maturation. 50 Biomechanical analyses further reveal that ACP nanoparticles improve the ultimate failure load and stiffness at the TBI, thereby enhancing overall biomechanical performance. Studies indicate that ACP promotes TBI repair mainly via contributing to tendon mineralization.
Hydroxyapatite
Treatment with octacalcium phosphate (OCP), a precursor of HA, enhances osteogenic differentiation in tendon stem/progenitor cells (TSPCs). This is evidenced by increased alkaline phosphatase activity and upregulated expression of genes (RUNX2, Col1a1, OCN, AND OPN), which collectively accelerate mineralization. 51 Beyond osteogenesis, OCP may also induce fibrocartilaginous differentiation of TSPCs, thereby increasing the Sharpey’s fibers formation in the TBI.52,53 During TBI healing, OCP initially enhances osteoblast-mediated mineralization on the bone side, whereas fibrocartilage-like cells dominate later stages by stimulating collagen and Sharpey’s fibers production. 54 These findings suggest that biological scaffolds (e.g., HA, hydrogel, and ECM), incorporating temporally regulated molecule cues (e.g., cytokines and drugs), could effectively induce TSPCs differentiation to restore the native structure of TBI. For instance, while transforming growth factor β1 (TGF-β1) upregulation in bone MSCs (BMSCs) enhances tendon–bone healing via mitogen-activated protein kinase (MAPK) 1 signaling pathway, 55 its efficacy diminishes over time. Research shows that the HA encapsulated with TGF-β1 significantly improved the area of fibrocartilage formation and mechanical strength postrepair. 56 Adipose-derived ECM (AD-ECM) contains key components of the TBI, containing elastin, laminin, glycosaminoglycans (GAGs), and collagen, 57 but lacks sufficient calcium. 58 However, combining AD-ECM with calcium materials, such as HA gradient (HA-G scaffold), can mimic the native TBI structure and provide MSCs with a regenerative microenvironment. This approach promotes collagen deposition in tendon, cartilage-related GAG, and type Ⅱ collagen accumulation in the intermediate zone, and increased calcium mineralization in the osseous region. 59 Therefore, further studies should consider developing scaffolds that better replicate the native TBI structure and augmenting bioactive substances to achieve both structural and functional restoration.
Beta tricalcium phosphate
Beta tricalcium phosphate (β-TCP) is a synthetic osteoconductive material that enhances bone regeneration. 60 When grafted into the bone-patellar tendon–bone site, β-TCP promotes the remodeling process of TBI structures. 61 What is more, β-TCP accelerates new bone formation and improves graft integration by contributing to osteoclasts resorption and osteoblast attachment to the junction. 62 Delivering recombinant human bone morphogenetic protein 2 via β-TCP further enhances fibrocartilage formation. 63 Filling bone tunnel with TCP improves ACL graft incorporation, yielding superior biomechanical properties and more mature histological organization. 64 However, current applications of TCP mainly focus on the osteogenic repair rather than TBI regeneration, as its bone formation effects require supplementation with additional bioactive substances. Additionally, its slow degradation kinetics limit its broader use compared with other calcium-containing materials.
Calcium silicate (CS)
The calcium silicate (CS) nanowires/alginate composite hydrogels significantly enhance tissue regeneration across the TBI, especially fibrocartilaginous transitional tissue. 65 In the rat and rabbit RCT models, CS-fish scale (CS-FS) promoted TBI regeneration through activation of the bone morphogenetic protein-2 (BMP-2)/Smad/Runx2 signaling pathway in BMSCs. This led to complete fibrocartilage layer regeneration, neo-tendon and bone formation at the junction, and improved biomechanical strength, with higher ultimate failure load than without CS-FS. 66 Notably, CS-based bioactive materials exhibit superior biodegradability and osteogenic activity relative to CaP-based biomaterials (HA, β-TCP, etc.), 67 as they release Ca and Si ions, synergistically enhancing TBI repair.
Magnesium (Mg)
Magnesium (Mg) is a promising biodegradable biomaterial for orthopedic application, owing to the favorable biocompatibility and mechanical characteristics. 68 Magnesium ions (Mg2+), a cofactor for enzymes, could facilitate the proliferation of human umbilical vein endothelial cells (HUVECs) to promote neovascularization while simultaneously stimulating fibrocartilage regeneration and reducing bone loss through BMSCs aggregation and osteogenic differentiation.69–72 Beyond tissue regeneration, Mg2+ could modulate inflammatory/immune microenvironment by polarizing macrophages toward anti-inflammatory M2 phenotype.17,73–75 Furthermore, Mg2+ entering BMSCs through the TRPM7 channel protein could facilitate cartilage matrix synthesis by upregulating hypoxia-inducible factor-1α (HIF-1α) and stimulating Sox9 secretion. 76 Given these properties, Mg-based biomaterials are increasingly being investigated for their therapeutic potential in TBI regeneration, with promising clinical applications.
Magnesium-based screw
Magnesium alloys including magnesium screws have attracted significant clinical interest owing to their bioactive and biodegradable properties. 77 Mg screws could not only improve biomechanical properties of tendon graft by increasing collagen fiber density, upregulating collagen II expression and suppressing MMP-13 expression, 78 but also modulate the inflammatory microenvironment of TBI by promoting macrophage polarization toward M2 phenotype. 79 Released from Mg interference screws, these ions enhance fibrocartilaginous entheses regeneration via upregulating BMP-2 and VEGF secreted by M2 macrophages.26,80,81 Despite these advantages, clinical application of magnesium-based screws in rotator cuff reconstruction remains limited duo to the unique anatomical structure.
Other magnesium-based materials
The composite hydrogel enables localized Mg2+ release, effectively promoting RCT tendon–bone healing via enhancing BMSCs adhesion, migration, and chondrogenic differentiation.19,82 Although current hydrogel systems exhibit improved ion release efficiency, achieving sustained delivery of bioactive ions (e.g., Mg2+) remains challenging. Citrate-based mussel-inspired magnesium whitlockite composite adhesives have shown potential to enhance initial TBI fixation strength, facilitate bony ingrowth from the bone tunnel, and promote both chondrogenic and osteogenic differentiation at the repair site. 83 Magnesium-based bone adhesive can improve the initial biomechanical properties of flexor tendon–bone repairs. However, in vivo application results in diminished mechanical performance over time, which is ascribed to allergic response and chronic inflammation. 84
Above all, Mg2+ shows great application in the TBI healing ascribing to its ability to enhance BMSCs migration, strengthen cell adhesion, and promote osteogenic differentiation. 85 However, the degradation of Mg-based materials generates hydrogen gas, which may compromise its biocompatibility. 78 Therefore, current research focuses on leveraging the synergistic effects of biomaterials and Mg2+’s biological properties to achieve sustained local ions release while avoiding its disadvantages in TBI healing.
Zinc (Zn)
Zn2+ is predominantly localized in the transition region between uncalcified and calcified fibrocartilage of TBI.86,87 Research shows that Zn2+ could regulate osteogenesis and inhibits osteoclasts by activating RANKL/RANK/OPG and Smad2/3/TGF-β signaling pathways in vivo and vitro.88–91 Considering these biological functions, several Zn containing materials have emerged as promising candidates for TBI healing application.
Zinc alloys
When Zn alloy-based screws are used for TBI suturing or fix ligaments, the released Zn2+ enhances graft integration by promoting osteogenesis and inducing tendon mineralization in rabbit ACL model. 92 Recent study indicates that Zn alloys facilitate BMSC osteogenic differentiation and HUVEC angiogenesis through SIRT4-mediated mitochondrial membrane potential and ATP production. 93
Zinc oxide
Zinc oxide (ZnO), when incorporated into bioactive ceramics, demonstrates osteogenic potential, acceptable biocompatibility, and sufficient mechanical strength, although these properties are less pronounced in zinc alloys. 94 The diverse morphological structures and functions of ZnO broaden its clinical applications. Both ZnO nanoparticles (nZnO) and ZnO films can improve osteogenesis, and nZnO exhibits additional antibacterial and angiogenic effects, whereas ZnO films display superior cell compatibility and improve chondrogenesis, fibrocartilage formation, and tendon healing.95,96 This suggests that both ZnO films and nanoparticles hold promise for TBI repair by facilitating regeneration of the TBI’s four-layer structure.
Collectively, Zn promotes bone regeneration and tendon healing. However, due to its inadequate mechanical qualities, Zn is typically combined with other materials to maximize its therapeutic efficacy.
Copper (Cu)
Copper (Cu) demonstrates multifunctional biological effects, including enhanced cellular migration and adhesion and promotion of osteogenic, chondrogenic, and angiogenic differentiation, while maintaining antibacterial properties. As a critical component for angiogenesis, Cu2+ promotes vascular endothelial cell tube formation and stimulates osteogenesis through the activation of HIF-1 pathway, thereby accelerating bone injury repair when Cu2+-incorporated biomaterials.97,98 Additionally, the release of Cu2+ further polarizes macrophages toward proinflammatory M1 phenotype through activation of Cu transport signaling pathways, including copper transporter 1 and ATPase copper-transporting alpha. 99 The activated M1 macrophages further enhance osteoblast maturation and exhibit increased bactericidal capacity against Staphylococcus aureus. 100 Moreover, recent studies have developed gradient bimetallic (Cu and Zn) ion-based hydrogel that simultaneously induces bone and tendon regeneration, thereby promoting fibrocartilaginous integration at the site. 20 To sum up, combining Cu2+ with other ions or biomaterials is a promising strategy to optimize its dual functions in supporting fibrocartilage organization and bone regeneration.
Cobalt (Co)
Cobalt dichloride (CoCl2) could promote neovascularization and enhance the migration and osteogenic differentiation of MSCs by activating BMP-9-HIF-1α circuit, thus accelerating bone defects repair when Co2+ incorporated into biomaterials.101–104 Cobalt nanoparticles exhibit good biocompatibility and favor osteogenesis by stimulating angiogenesis and biomineralization.105,106 Considering all these studies, Co2+ has significant potential for application in TBI due to its role in promoting angiogenesis and bone formation.
Strontium (Sr)
Approximately 98% of the body’s Sr resides in bone, where it exhibits similar characteristics with Ca2+ and can substitute for Ca2+ to enhance the osteogenic properties of bone graft.107,108 Sr could facilitate osteogenesis, calcium nodule formation, and matrix mineralization through activation of MAPK signaling and ERK1/2 phosphorylation in osteoblasts. 109 Conversely, it inhibits osteoclast differentiation and resorptive activity by suppressing carbonic anhydrase II and vitronectin receptor expression. 110 When incorporated into calcium phosphate cement, Sr accelerates bone tunnels healing by promoting rapid formation of Sharpey’s fibers and early remodeling of the graft–fibrocartilage–bone interface. 111 In ACL injury repair, silicate-substituted strontium (SrSiP)-coated ligament could facilitate bone formation. 112 Interestingly, newly formed bone area exhibits lower calcium concentration compared with previous findings, suggesting osteoblast on the ligament surface enhanced the consumption of Ca2+ for bone matrix synthesis. Beyond bone regeneration, Sr also supports cartilage repair with improved chondrocyte adhesion and maturation through the Notch and Wnt signaling pathways, though at much lower concentrations than required for osteogenesis.113,114 Excessive Sr2+ concentrations impair both cartilage regeneration and bone healing by suppressing Ca absorption. Given the dual requirements for cartilage formation and bone regeneration, precise control of Sr2+ release kinetics is crucial for the repair of TBI.
Iron (Fe)
Iron (Fe) serves essential physiological functions and accelerates osteogenesis through enhanced angiogenesis. 115 Studies demonstrated that Fe enhances mitochondrial activity and upregulates osteogenic markers (ALP and OCN) in BMSCs. 116 Fe-based biodegradable materials exhibit mechanical properties matching native bone tissue while demonstrating excellent cell compatibility. 117 In addition, iron oxide nanoparticles significantly improve wound healing by enhanced fibrogenesis and angiogenesis. 118 And BMSCs-derived exosomes preconditioned with Fe3O4 nanoparticles exhibit superior osteogenic and angiogenic effects compared with untreated exosomes. 119 Therefore, further research should investigate the therapeutic potential of iron in TBI healing and elucidate its underlying mechanisms.
Lithium (Li)
Lithium (Li), an essential element present in human bones, has emerged as a promising therapeutic agent for bone regeneration owing to its significant osteogenic properties. 120 Li promotes BMSC proliferation and osteogenic differentiation through activating both Sonic hedgehog and Wnt/β-catenin pathways. This effect is mediated through β-catenin stabilization by decreasing glycogen synthase kinase 3 activity.121,122 In addition, Li enhances angiogenesis by upregulating proangiogenic genes expression in BMSCs and HUVECs.123,124 While no studies have directly investigated Li’s role in TBI repair, its demonstrated dual capacity to stimulate both bone formation and angiogenesis suggests strong therapeutic potential for TBI repair application.
Summary and Outlook
TBI injury is a prevalent condition in sports medicine. Because of the complex structure of TBI and limited intrinsic healing capacity, TBI is characterized by poor functional recovery, posing significant challenges in clinical treatment. This review summarizes the numerous therapeutic potentials of various metal ions integrated into biomaterials, such as calcium, magnesium, zinc, copper, cobalt, strontium, iron, and lithium, and emphasizes their contributing roles and the potential mechanisms in TBI healing. Successful TBI healing requires coordinated regeneration of the four structures alongside functional integration between them. These metal ions can facilitate functional TBI healing by enhancing osseointegration, promoting fibrocartilage formation, angiogenesis, and modulating macrophage polarization.
Among the mentioned metal ions, Ca2+, Zn2+, Sr2+, and Li+ promote osteogenic differentiation of BMSCs, whereas Cu2+, Co2+, and Fe2+ enhance osteogenesis by promoting angiogenesis. Additionally, Ca2+, Zn2+, and Co2+ induce tendon mineralization, upregulating bone-related markers and facilitating the fusion tendon-to-bone. In contrast, Ca2+ alone exhibits limited chondrogenic potential but synergizes with other ions (e.g., in CS complexes) to enhance fibrocartilage regeneration. Mg2+ primarily promotes cartilage formation and modulates the inflammatory microenvironment. While Ca2+ alone exhibits limited chondrogenic potential, combining them with other inorganic ions to form new complexes such as CS has been found to promote fibrocartilage regeneration. Notably, combining Mg2+ with osteogenesis-related metal ions simultaneously promotes fibrocartilage and bone regeneration, demonstrating superior efficacy compared with single-ion treatments. However, simply integrating different ions together is inadequate for optimal TBI healing. At present, many studies have focused on the construction of rheological, biocompatible and biodegradable materials as carriers to release therapeutic drugs or ions, among which hydrogels and nano materials show great advantages.
Although we have some achievements in restoring the structural and functional integrity of TBI, current research and treating methods are unable to completely restore the normal mechanical properties of TBI. Therefore, further research is needed to advance TBI repair from both the mechanistic and therapeutic methods.
Authors’ Contributions
P.Y., J.G., and G.N. contributed equally to writing original draft and writing—review and editing; Y.H. and X.C. contributed significantly to article collection and analysis; T.P., L.L., Z.D., and W.X. provided critical revisions and final approval of the version to be published. All authors read and approved the final article.