
Abstract
BACKGROUND:
Bone cements aid in bone regeneration; however, if the handling time is not well established for the material to harden, complications may arise.
OBJECTIVE:
This work investigates the effect of using polyethylene glycol (PEG) and characterize it in brushite bone cement in order to obtain desirable handling times as well as its regeneration in vivo to analyse if addition of this polymer may significantly modify its properties.
METHODS:
PEG 4000 was synthesised with wollastonite by phosphorization reaction in order to form brushite which was further cured by oven drying. They were further characterised and tested in vivo as tibial bone defect model using rabbits.
RESULTS:
Addition of PEG exhibited handling times of 60 min with a low increase in temperature when curing. Brushite phase of ∼71% was obtained after cement hardening with good compressive strength (25 MPa) and decent values of porosity (33%). In vivo presented that, at 40 days postoperatively, accelerated bone neoformation with partial consolidation at 30 days and total after 60 days when using bone cement.
CONCLUSIONS:
Addition of PEG does not disrupt the beneficial properties of the bone cement and can be a potential alternative to control the time-temperature profile of hardening these materials.
Introduction
Bone cements are used in biomaterials applications such as orthopaedic and dentistry, and by mixing a ceramic powder, usually calcium phosphates [1], with aqueous solution phase, such as acids [2,3], a viscous mass is formed. This material is then spontaneously hardened at room or body temperature, presenting biodegradability and osteoconductive properties [4,5].
Calcium silicate is the main component of wollastonite/brushite bone cement, in which the wollastonite powder (CaSiO3) reacts with a phosphoric acid solution, obtaining a homogenous mass, that after drying, forms the brushite phase [6]. The bioresorbable mechanism of brushite cements have been reported to be due to macrophages and giant cells, osteoclastic activity and simple dissolution; therefore, possessing faster bioresorbable rate as they decompose by active and passive processes compared to hydroxyapatite [7,8].
In particular, brushite cements still presents challenges, such as short handling period and inflammatory reactions that have been reported in the first weeks [9]. This could have been attributed to partial transformation of brushite to hydroxyapatite, and/or calcium-deficient hydroxyapatite that releases phosphoric acid [2]. Addition of Polyethylene glycol (PEG) can alter the curing time, and also improve the handling period of this material [10]. However, the in vivo effect is not yet thoroughly understood, but previous work by Vahabzadeh et al. suggests that PEG is biocompatible, and significantly enhances cells proliferation and differentiation. Nevertheless, the amount of PEG added can negatively alter the cellular behaviour [11]. Therefore, evaluation of clinical and histological analyses for PEG, synthesised within the brushite bone cement, may provide important evidence of the potential usefulness of this polymer.
Therefore, in this work, we evaluate the effect of using brushite bone cement together with PEG polymer to increase its handling time and adjust the temperature of exothermic reaction within safe limits of usage. This material was characterised and further studied in vivo.
Materials and methods
Production of brushite cements
The methodology used for the bone cement synthesis (Fig. 1) was adapted from [12]. Initially, phosphoric acid (9.95 mol/L) and polyethylene glycol - (PEG) 4000 (0.075 mol/L) aqueous solutions were prepared. Consequently, corresponding amounts were manually mixed for 90 seconds, using 2.9 mL of phosphoric acid solution and 5 g of wollastonite powder (sizes of <38.1 μm), and PEG 4000 solution (0.075 mol/L) that was added (0.3% wt of wollastonite). Afterwards, the paste was added in Teflon moulds in order to form cylindrical specimens (5.8 ± 0.1 mm in diameter and 12.3 ± 0.1 mm in length) that were submitted to curing (drying) for 24 h at 25 ± 5 °C and relative humidity of 80 ± 10%.
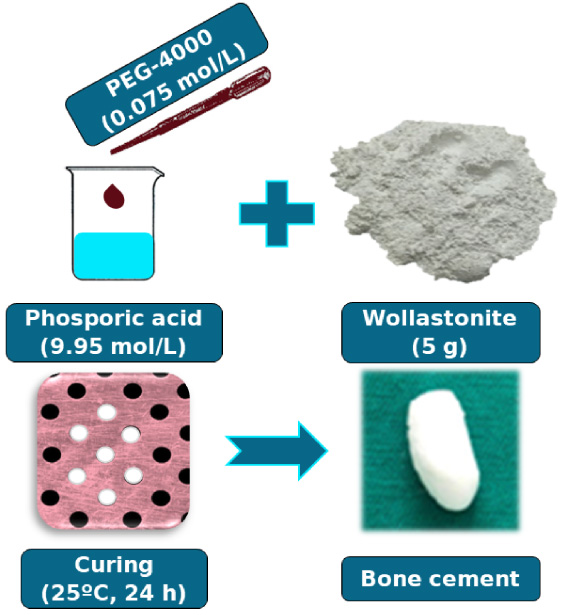
Synthesis of brushite bone cement.
X-ray diffraction (XRD)
The XRD was performed in grounded and sieved samples using an X-ray diffractometer X XRD-7000 (Shimadzu, Japan) as Cu–Kα radiation (k = 1.5418 Å), voltage of 40 kV, current of 30 mA; also, in the angular range of 10–70° (2𝜃) with scanning speed of 1°/min, Rietveld was performed with (GSAS II) software (NIST, USA).
Mercury intrusion porosimeter (PIM)
A mercury porosimeter AUTOPORE IV (Micromeritics, USA) was used to verify the pore diameter, pore volume and pore distribution.
Compressive strength
This test was performed according to the ABNT NBR ISO 5833 Standard at one, three and seven days after curing, using an Instron 3360 Series (Instron, USA), with load cell of 10 kN and speed of 1 mm/min using five samples.
Scanning electron microscopy
The morphology was obtained using an Electronic Scanning Microscopic from TM - 1000 (Hitachi, Japan). Cross-section of the bone cement and grounded powder were performed at 1500X and 3000X.
In vivo methodology
Surgery conditions
The experiments were carried out after approval by the Ethics Committee on the Usage of Animals of UFCG with protocol no. 0134/2018.
Characteristics of the animals studied
Twelve half-breed, young adults’ rabbits of the New Zealand breed (New Zealand (Oryctolagus Cuniculus), all clinically healthy as six males and six females, weighing on average 2.5 ± 0.3 kg were used. They were randomly divided into two experimental groups of six animals for the surgery, and each group subdivided into two other subgroups, according to observation periods of 40 and 90 days.
Anaesthesia and surgery procedure
Prior to operative period, the animals received ivermectin, in order to prevent scabies, (0.4 mg/kg), subcutaneously, and then were numbered and put in individual cages which were previously sanitized and suspended from the ground. They remained for 15 days for adaptation and through all the experimental period, in which they received a balanced feed ratio twice a day, and drinking waterad libitum.
In the preoperative period, the animals were anesthetized using zoletil (15 mg/kg), intramuscularly, which was followed by an anti-inflammatory, meloxicam (0.2 mg/kg), subcutaneously. About 30 minutes before the surgical procedure, prophylactic antibiotic therapy was administered intravenously, using cephalothin 20% at 25 mg/kg. After removal of the hairs from both pelvic limbs and lumbosacral region, anaesthesia was performed with 2% lidocaine (0.3 ml/kg), and tramadol 5% (1 mg/kg) via epidural route in all animals.
A 2-cm-long incision was made at the proximal and distal cranium-medial margin of each tibia, followed by a subcutaneous and muscular tissue divulsion until the periosteum was exposed. The bone defect was standardized as a 2 mm of diameter which was made medially on the proximal tibial diaphysis of each pelvic limb. An orthopaedic drill was used, with a 2 mm drill bit, under constant irrigation of 0.9% sodium chloride solution to avoid thermal injury on the edges of the defect. In the right limb, the bone defect was not filled with any material, used as control, and in the left limb the defect was filled with the brushite bone cement. Afterwards, the grafts were fixed to the receiving areas by suturing the musculature with “X” suture pattern using a polyglactin 910 3-0 which was also used for reducing dead space, and also the skin suture with standard nylon 3-0 thread using the Wolf suture pattern.
Postoperative evaluation from in vivo
In the postoperative period, the surgical wound was cleaned daily using 0.9% sodium chloride solution, with subsequent application of a dressing with the help of a gauze and adhesive tape, and meloxicam (0.1 mg/kg) every 24 h for three days. The process of clinical evaluation of the surgical wounds occurred following ten postoperative days. Animals that presented such conditions were counted as indices (%) from the total observed group.
Radiograph evaluation
Plain radiographies of craniocaudal and middle-lateral projections were performed in the immediate postoperative period, and at 30, 60 and 90 days, in order to analyse the bone regeneration. Animals with presence, or absence, of periosteal reaction, periosteal reaction with consolidation and total consolidation from the radiographic evaluation were counted as indices (%) from the total observed group.
Euthanasia
The animals were euthanized after 40 and 90 days, using xylazine 2% (5 mg/kg) intramuscularly. After 15 min, thiopental sodium (20 mg/kg) was administered intravenously and, straight after the loss of the reflexes, potassium chloride 19.1% (1 ml/kg) intravenously.
Processing of in vivo samples
After euthanasia, 40 and 90 days, the tibias were removed and sectioned around 1 cm above and below in relation to the implant. The bone fragments were submitted to fixation using 10% Neutral buffered formalin for 10 days. Afterwards, it was washed in running water and decalcified using 5% formic acid solution + 5% hydrochloric acid for five days; afterwards, the pieces were included in liquid paraffin and, subsequently, cut in transversal slices of 5 μm thickness from the blocks mounted on glass slides. From each block, four slides were obtained, and these were stained using haematoxylin-eosin for the histological visualization.
Statistical analysis
The differences in the clinical and histological results with the Brushite biomaterial and control treatment were tested using the Wilcoxon signed rank test. The analyses were performed using the R 3.5.0. program (R Core Team, 2018).
Results and discussion
Time-temperature curing profile
The brushite cement with PEG (BR/PEG) presents no cure in the first 60 min (Fig. 2). Subsequently, there is a fast increase in temperature reaching a peak at 49.7 °C; considering this as an adiabatic system, it will be lower during actual in vivo application. In addition, there is an exothermic cure reaction that occurred with a peak at 77 min, followed by a fast temperature decrease reaching again the stable value of 25 °C at 80 min.
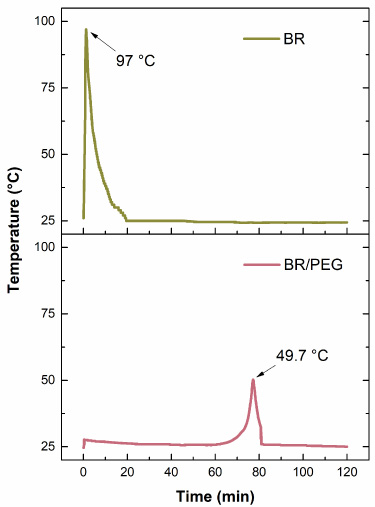
Time-temperature curing profile for the studied brushite cement with (BR) or without addition of PEG (BR/PEG).
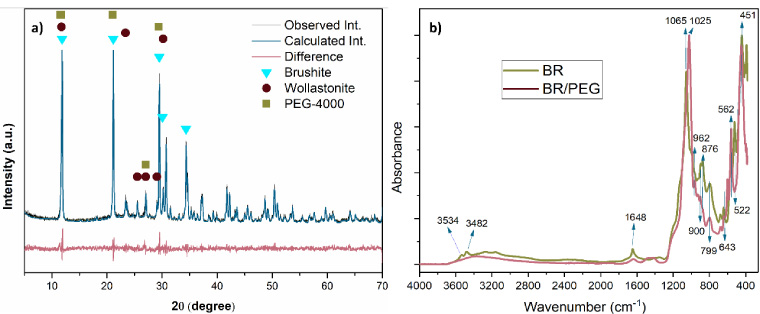
(a) XRD spectra of brushite BR/PEG cement and (b) FTIR for the brushite bone cement with (BR) or without (BR/PEG) PEG.
The first event that occurred prior to exothermic reaction, commonly known as handling period, are generally longer in comparison to mixture and curing periods [9,13]. The target-application aimed at bone cements will require different handling periods, such as shorter periods in dentistry, and longer for the orthopaedic; however, the sample BR/PEG presented a reasonable safe handling period, 60 min, in order to use as bone implant. Therefore, the sample BR/PEG formulation was used for further characterizations and in vivo studies.
The X-ray diffraction (XRD) with Rietveld refinement for BR/PEG cement (Fig. 3a) presents the characteristic peaks and crystalline phases from brushite synthesis, wollastonite and polyethylene glycol (PEG-4000). The crystalline phase of brushite was monoclinic centred from spatial group I 12/a1 (JCPDS 96-900-7305) at angles (2𝜃) of 11.84°, 21.14°, 29.48°, 30.07° and 34.34°. In addition to a crystalline phase of triclinic wollastonite as spatial group P-1 (JCPDS 00-027-1064), at angles (2𝜃) of 11.72°, 23.36°, 25.48°, 27.03°, 29.05° and 30.18°. These identifications are in agreement with previous works [8,14,15]. Furthermore, there is presence of characteristic peaks from polyethylene glycol (PEG-4000) as orthorhombic, pccn space group, (COD 400-1603 and JCPDS 00-049-2095) which was identified at angles (2𝜃) of 11.53°, 11.66°, 21.00°, 27.01° and 29.44°. The quantification of present phases for the brushite cement calculated by the Rietveld refinement reported 70.95% of brushite and 29.05% of wollastonite phases with a Rwp confidence factor of 14.5%.
The FTIR was used in this work in order to investigate the main functional groups from the bone cements, whether with or without PEG 4000 (Fig. 3b). The spectra present a low intensity broadband, whereas pure brushite bone cement presents peaks at 3534 and 3482 cm−1 assigned to stretching of hydroxyl groups (O-H) and vibrations of water molecules in the network. In addition, vibration of water bending with a maximum at 1648 cm−1 was detected, while a decrease occurs with PEG 4000 addition [16].
The high intensity vibrations between 1000–1100 cm−1 are characteristic of symmetrical vibrations from covalent bonds present in the hydrogenated phosphate ions (P=O), as presented by their bands at 1065 and 1025 cm−1 with or without PEG in their profiles. The presence of bands at 962, 876 and 799 cm−1 are assigned to the asymmetric stretching vibrations of the ionic groups (ortho) phosphates P-O(H). All bands mentioned previously are characteristic of groups between phosphorus and oxygen, which corresponds to the brushite phase in agreement with XRD results. Shifting of the bands are due to the vibrations caused by the addition of the polymer into the bone cement [17–19].
The bands around 562 and 522 cm−1 are assigned to the bending vibrations (O-P-O) of brushite phosphate groups (P-O), whereas addition of the polymer had variation on its intensity. Characteristic bands of covalent bonds assigned to silicate ion (SiO3 2−) in 900, 643 and 451 cm−1 were also identified, with strong intensity, confirming the presence of wollastonite [20–22].
Physical properties
The cumulative porous volume as function of pore-size distribution graph for the bone cement containing PEG (Fig. 4a) presents a narrow distribution of pore size. According to Guan et al., this effect may be related to the PEG that, when mixed with the brushite, occupies the brushite void-rich regions forming anchoring groups on the surface. The polymeric solvent chain is then extended in the medium, creating a steric hindrance layer in which, besides delaying the reaction curing time, it also prevents aggregation of solid particles [23]. This material presented to be highly selective in the region of 1200 nm, a profile similar to what has been reported before [13]. In addition, porosity values presented to be at 33%, which is ideal for its application as a load bearing for bone tissue injuries. Furthermore, values of average diameter presents to be in micrometre region with apparent density and further values similar to calcium phosphate bone cements reported in literature [7,24].
Compressive strength of bone cements was measured at three-time intervals (days) after curing the material (Fig. 4b). The compressive strength presented no statistically significant difference, presenting mean values of 21.4 ± 2 MPa. Calcium orthophosphate cements with applications in orthopaedics are comparable with the human spongy bone (trabecular) (10–30 MPa), as previously reported by other authors [7,25]. The values presented herein are in agreement with previous works [13,26], in which brushite cements have compressive strength within 25 MPa.
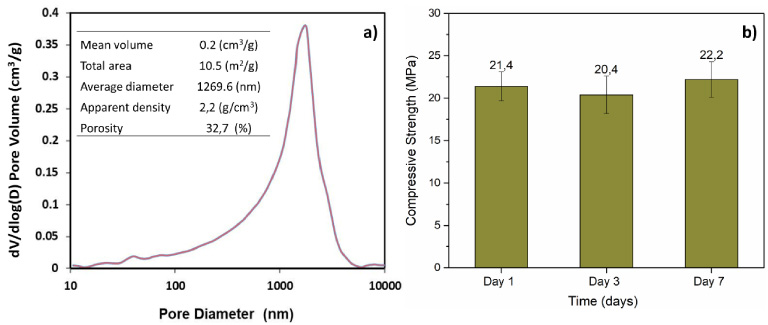
(a) BR/PEG cement cumulative volume distribution and (b) compression strength graph after one, three and seven days of the sample synthesis.
An irregular surface microstructure can be perceived in the bone cement containing the polymer (Fig. 5), characterized by clusters of different sizes and shapes that exhibited a growth of two types of particles. The majority of these particles are arranged in a lamellae or plate shape, that corresponds to the formation of brushite and amorphous silica in agreement with previous works [27,28]. Cross-section morphology of this material exhibits few aggregations of the bone cement particles (Fig. 5b), assigned to the hinder effect of PEG.
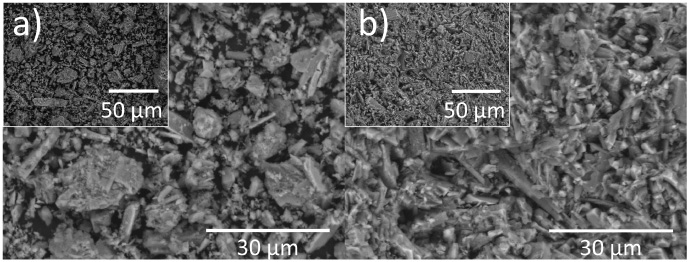
Morphology of the bone cement BR/PEG by SEM as (a) powder particles and (b) cross-section.
The clinical variables were not significantly different between the control and the brushite in any periods evaluated; therefore, indicating that tibial support was not compromised. The use of brushite bone cement, compared to control, resulted in a significantly higher incidence of local signs - such as erythema, on the first day, as well as for the fourth to the tenth day; drainage on the second, fifth and eighth to tenth day; and claudication on the sixth, seventh and tenth postoperative days (Fig. 6). Despite these clinical responses, no contamination of the product during its handling occurred, which was verified by the absence of microorganisms by histological evaluations.
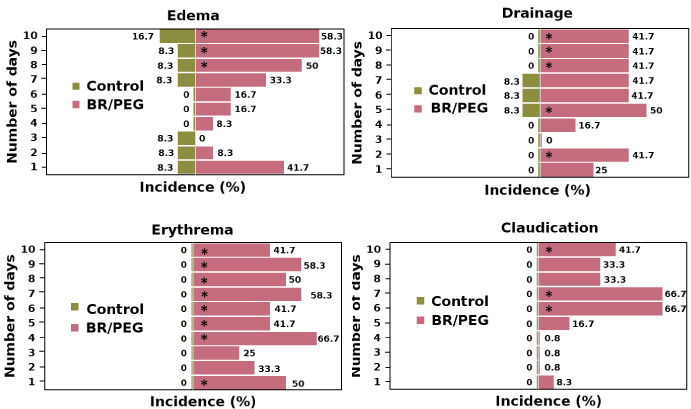
Incidence (%) of clinical variables during 10 days of recovery after surgical treatment for the right pelvic limbs (Control) and left pelvic limbs (BR/PEG). *Significant differences (p < 0.05) between control and BR/PEG cement at paired Wilcoxon test.
From day eighth to tenth, edema was observed in most animals which was also observed in another work using a calcium phosphate-based bone substitute [29,30]. However, up to the tenth postoperative day, some animals still exhibited signs of inflammation; even though the healing of the surgical wound occurred by first intention and the suture was removed on the tenth day. Based on these evaluations, it can be stated that there is no rejection to the brushite bone cement, confirming its biocompatibility.
The histological examinations presented no significant differences between the bone histological analysis from the animals treated with brushite and the control (endosteal reaction, periosteal reaction, cicatrization tissue, bone differentiation and newly-formed bone), both at 40 days as at 90 days after the surgical procedures (Fig. 7).
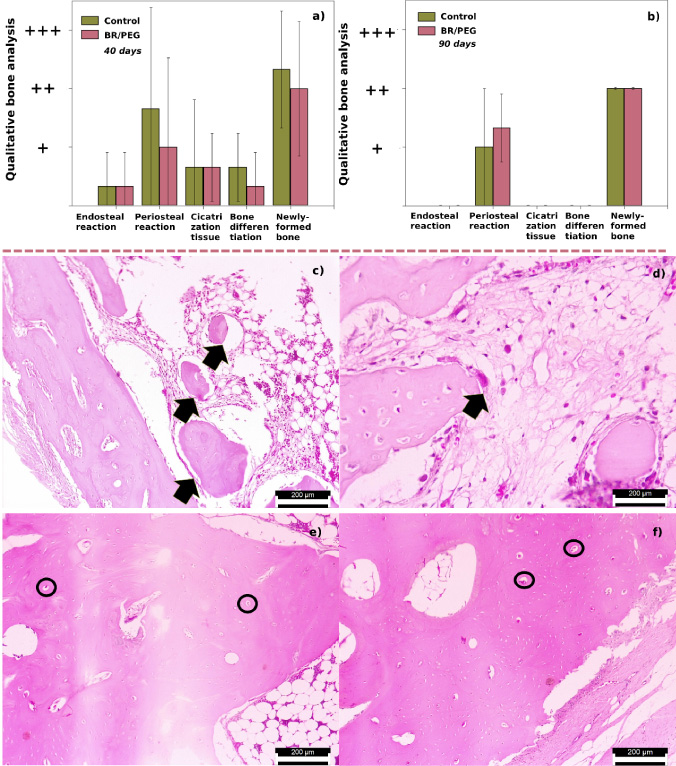
Histological qualitative bone analysis at (a) 40 and (b) 90 postoperative days for control and BR/PEG bone cement. Data presents no statistically significant differences between control and brushite. (c–f) Micrographs from histological section at (c,d) 40 postoperative days. (c) Control with rarefaction of bone trabeculae (arrows). (d) Brushite bone cement (BR/PEG) with formation of bone trabeculae, the arrow indicates osteoclastic activity (arrow). (e,f) 90 postoperative days whereas few osteocytes on (e) control while increased in (f) biomaterial group (circles). HE. 40 X objective 200 μm scale.
The bone-implant interface histological evaluation presents (Fig. 7b), at 40 postoperative days, no traces of the bone cement meaning that the biomaterial was completely absorbed. With the usage of the biomaterial, bone trabecula formation is perceived, and indicating osteoclastic activity (giant multinucleated cell in arrow Fig. 7d). The small gaps inside that bone trabecula, which are more numerous, contains osteocytes inside. It is possible to note, concomitantly, that the same trabecula is irregular. Thus, the sum of osteoclastic activity, abundant gaps with osteocytes inside and irregularities in the bone trabecula, represent components of bone repair. The PEG polymer used in this work presents low toxicity, good biocompatibility, and biodegradability without bone neoformation [31] whereas the bone neoformation observed in these histological images can be related to the brushite effect, which contains Ca–P phases that induces bone neoformation.
Microscopic histological evaluation of the animals euthanized at 90 postoperative days (Fig. 7e,f), from the bone-implant interface, exhibits the periosteum totally structured with presence of fibroblasts, active conjunctive tissue and absence of the biomaterial, demonstrating its bioactivity and reabsorption capacity in the organism [30]. In the control group, (Fig. 7e), in the central gap (between the two circled areas, which is irregularly shaped), there is occasional fibrosis (in an area that typically had only bone marrow and fat in a normal bone) and a slight amount of osteoblasts in a small region.
Data regarding the presence, and absence, of the variables for the radiographic evaluation (Fig. 8) exhibited first that absence of periosteal reaction was not perceived in the rabbits, on any period of the evaluation days.
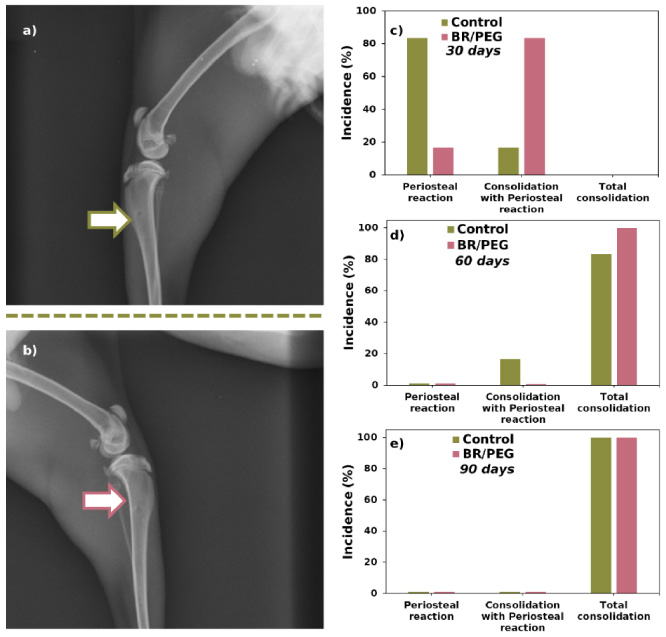
Radiographic image of the lateromedial projection of the tibia and fibula of rabbits at 30 postoperative days. (a) Control group. (b) BR/PEG group. The location of the bone orifice in (a) and (b) is highlighted (white arrow). (c–e) Radiographic evaluation indices, periosteal reaction; periosteal reaction with consolidation; and total bone consolidation.
In the evaluation at 30 days after surgery, 83.3% of the limbs from animals treated with brushite presented periosteal reaction on the borders of the lesion, with non-complete concentric consolidation, showing the presence of a defined radiopaque line at the defect site (Fig. 8a,b), thus indicating an osteointegration [32,33]. Whereas the majority of the control group presented reaction only at the borders, with only 16.6% demonstrating incomplete concentric consolidation, which may suggest that the brushite bone cement favours the bone healing process faster for being osteoinductive and osteoconductive.
These indices were reduced when evaluated at 60 and 90 days (Fig. 8c–e), since many animals already presented total bone consolidation. In the period of 60 days (Fig. 7d), all animals treated with bone cement already had total consolidation while only 83.3% from control had total bone consolidation. At the end of the experiment, 90 days, all animals had total bone consolidation (Fig. 8e).
By selectively specifying the content of polymer added in the liquid aqueous phase of bone cements it is possible to obtain a desirable handling curing time with little drawback in terms of its physical properties and morphology. These translates in good biocompatibility and regeneration when implanted having total consolidation after 40 days using rabbit tibial defect model, suggesting that the addition of PEG can be a useful coupling agent when forming bone cements.
Footnotes
Conflict of interest
None to report.