
Abstract
Fecal incontinence (FI) severely affects physical and psychological well-being. Artificial anal sphincters (AASs) provide a reconstructive option for patients with severe sphincter damage or congenital dysfunctions, but their clinical application is often limited by complications stemming largely from poor biomechanical compatibility with host tissues. This review examines the physiological mechanisms of defecation as the basis for bionic AAS design and classifies existing devices into two main types: those simulating anorectal angle regulation and those mimicking direct sphincter occlusion. A comparative analysis reveals distinct biomechanical failure modes associated with each approach: angle-modulating devices face challenges like tissue hyperplasia around moving parts, while direct occlusion devices, particularly high-pressure circumferential cuffs, frequently lead to tissue erosion, infection, and mechanical breakdown due to ischemic pressure. Addressing this core issue of biomechanical incompatibility is paramount. Novel mechanical designs, such as constant-force mechanisms, aim to mitigate pressure-induced injury. Furthermore, future optimization directions include enhancing device intelligence through smart sensing and AI algorithms, and exploring biohybrid designs that integrate tissue-engineered components to potentially achieve superior long-term integration. This review underscores that harmonizing mechanical function with the biological environment is critical for improving the safety, efficacy, and longevity of AASs in FI treatment.
Impact Statement
Artificial anal sphincters (AASs) represent a promising solution for fecal incontinence (FI), but their clinical utility is limited by poor biomechanical integration with soft tissues. This review analyzes current bionic AAS designs and highlights biomechanical compatibility as a key barrier to long-term success. It proposes engineering solutions—such as constant-force output and rapid feedback control—that could improve the safety, efficacy, and clinical applicability of future AAS systems.
Keywords
Introduction
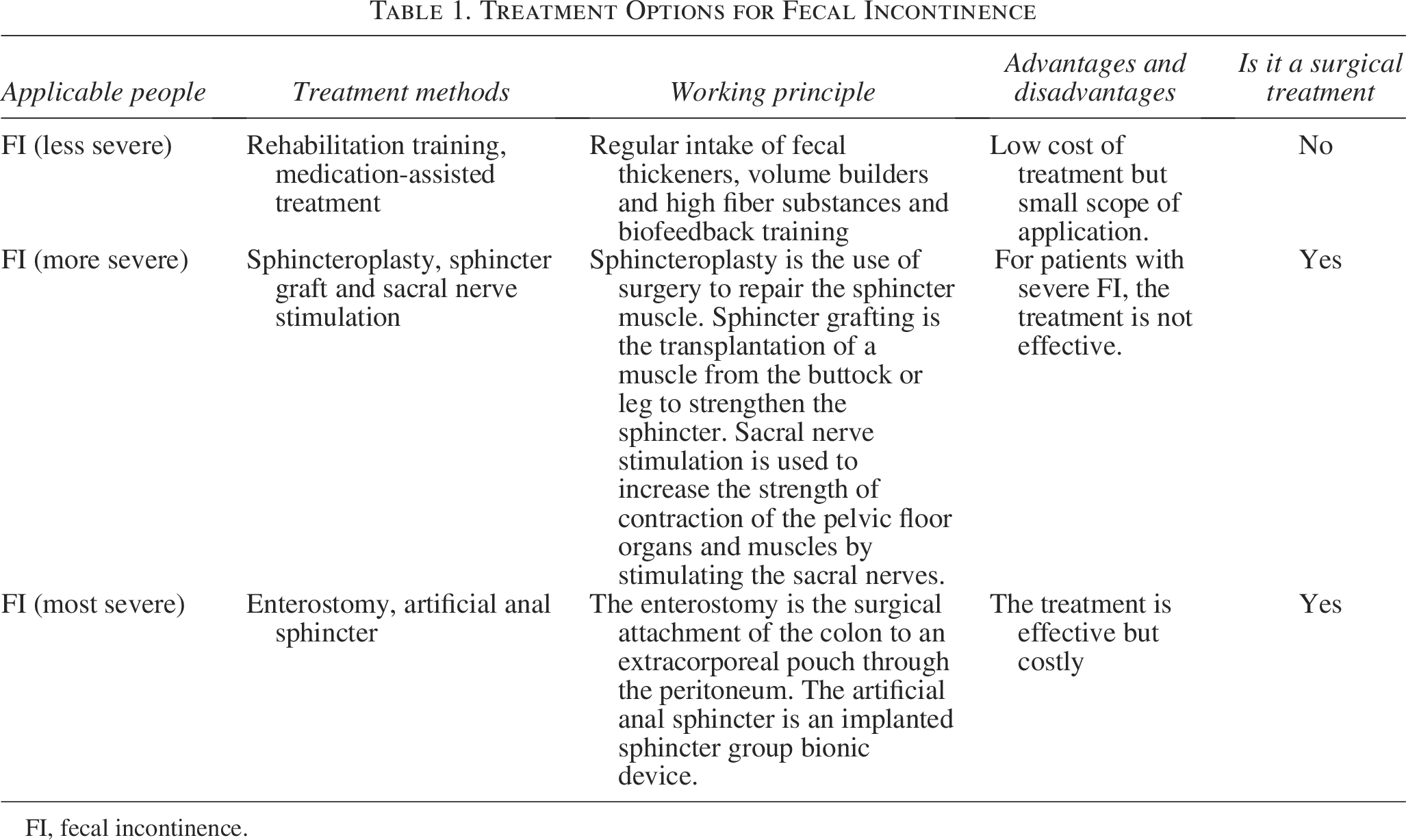
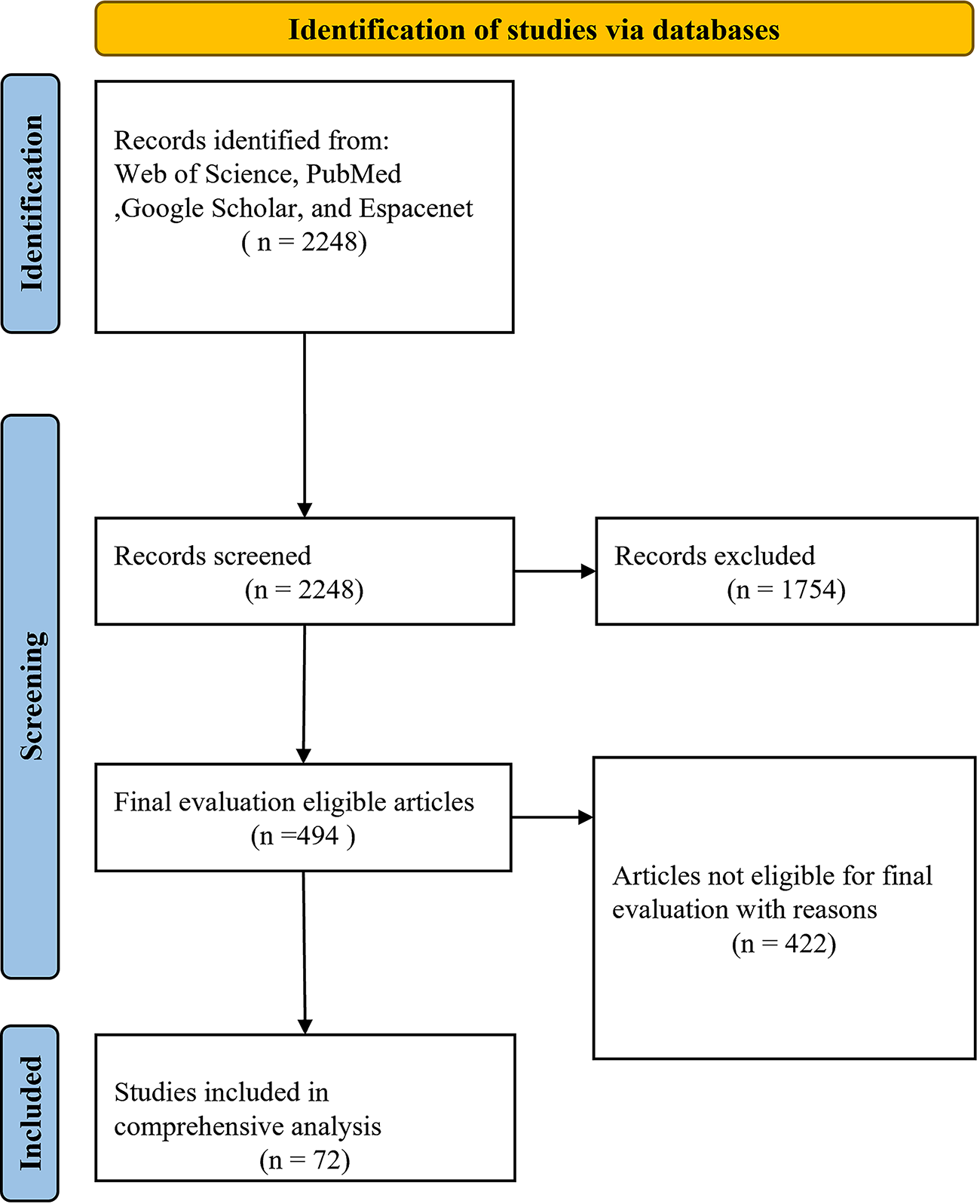
Fecal incontinence (FI) is characterized by the uncontrolled excretion or leakage of intestinal contents. 1 FI is a widespread condition that not only reduces quality of life but also causes significant psychological distress. 2 FI is most prevalent among middle-aged and older adults, yet its prevalence is often underestimated. The overall prevalence in adults is estimated to be about 15% and increases with age. It is more common in women and the elderly, affecting approximately 16% of younger women and up to 40% of older women.3–5 FI has complex and multifactorial causes, primarily including injury to the sphincter or its innervation, and sphincter atrophy (Fig. 1). The most common risk factors are sphincter injuries during childbirth or surgery.6,7 Other contributing factors include older age, frequent diarrhea, certain intestinal and congenital diseases, and diabetes.8–10 Treatment options for FI include both conservative and surgical approaches. Conservative treatment includes medication, biofeedback, and lifestyle interventions.11–13 Surgical treatment includes sacral nerve stimulation, enterostomy, and artificial anal sphincter (AAS) implantation.14–17 Conservative treatment is typically the first-line option for patients with mild symptoms. If conservative treatment fails, surgical intervention becomes necessary. Sacral nerve stimulation is usually considered for patients with a history of septicemia and an intact sphincter. In cases of severe sphincter damage or absence, enterostomy or AAS implantation is required (Table 1). Compared with AAS, enterostomy can significantly disrupt daily life, limiting social participation, and physical activity. Therefore, an AAS is a more suitable option for patients with severe FI, particularly those with congenital sphincter defects or rectal sensory loss. An AAS functions by sealing the biological lumen to replicate the role of the natural sphincter. Currently, experimental AAS systems primarily employ hydraulic, magnetic, or other actuation mechanisms 18 (Fig. 2).
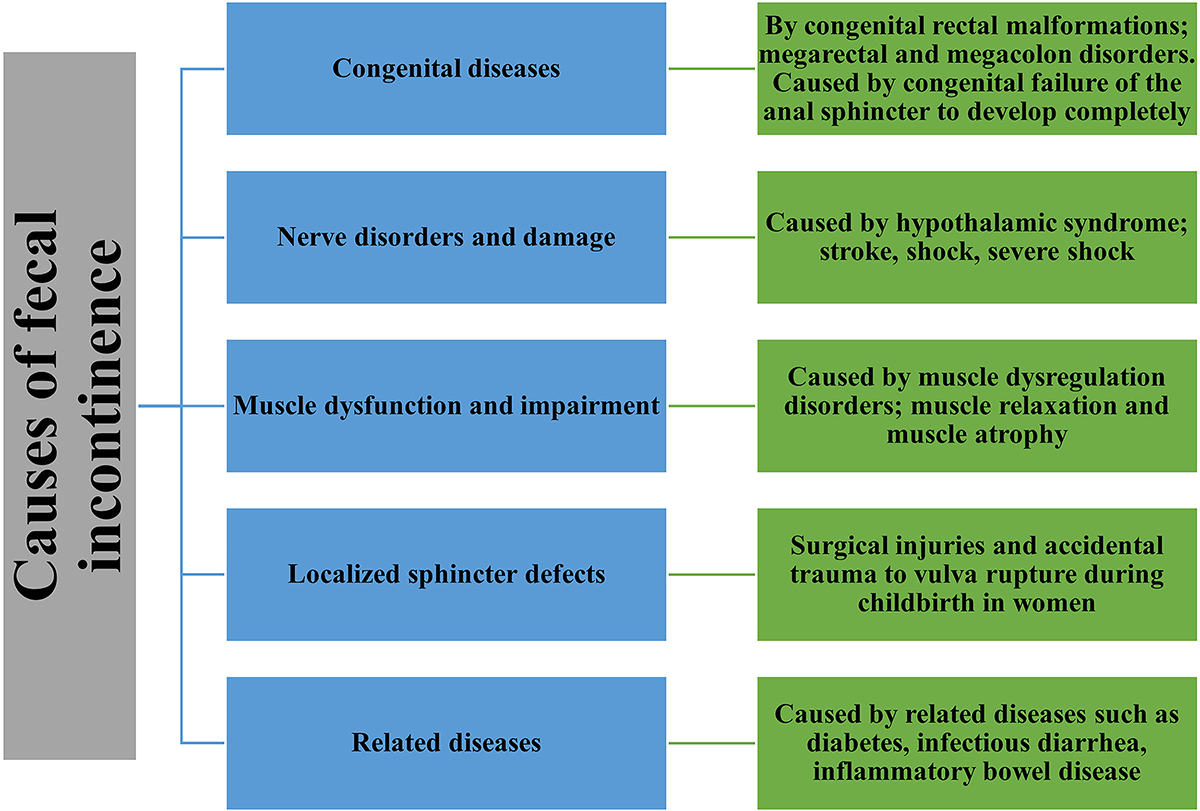
Causes of fecal incontinence.
Treatment Options for Fecal Incontinence
FI, fecal incontinence.
Activation methods of artificial anal sphincters.
To better understand the working principle of AASs and guide the design of an ideal system, this paper analyzes the physiological defecation mechanism in healthy individuals and reviews existing bionic AAS designs through the critical lens of biomechanical compatibility. We categorize devices based on their biomimetic principles, compare their respective biomechanical advantages and clinical failure modes, and discuss key engineering elements derived from current design experience. Recognizing that achieving long-term safety and effectiveness hinges on resolving the biomechanical mismatch between implants and host tissues, this review further explores advanced optimization strategies, including novel mechanical designs, the integration of smart sensing and artificial intelligence (AI), and forward-looking concepts in biohybrid engineering.
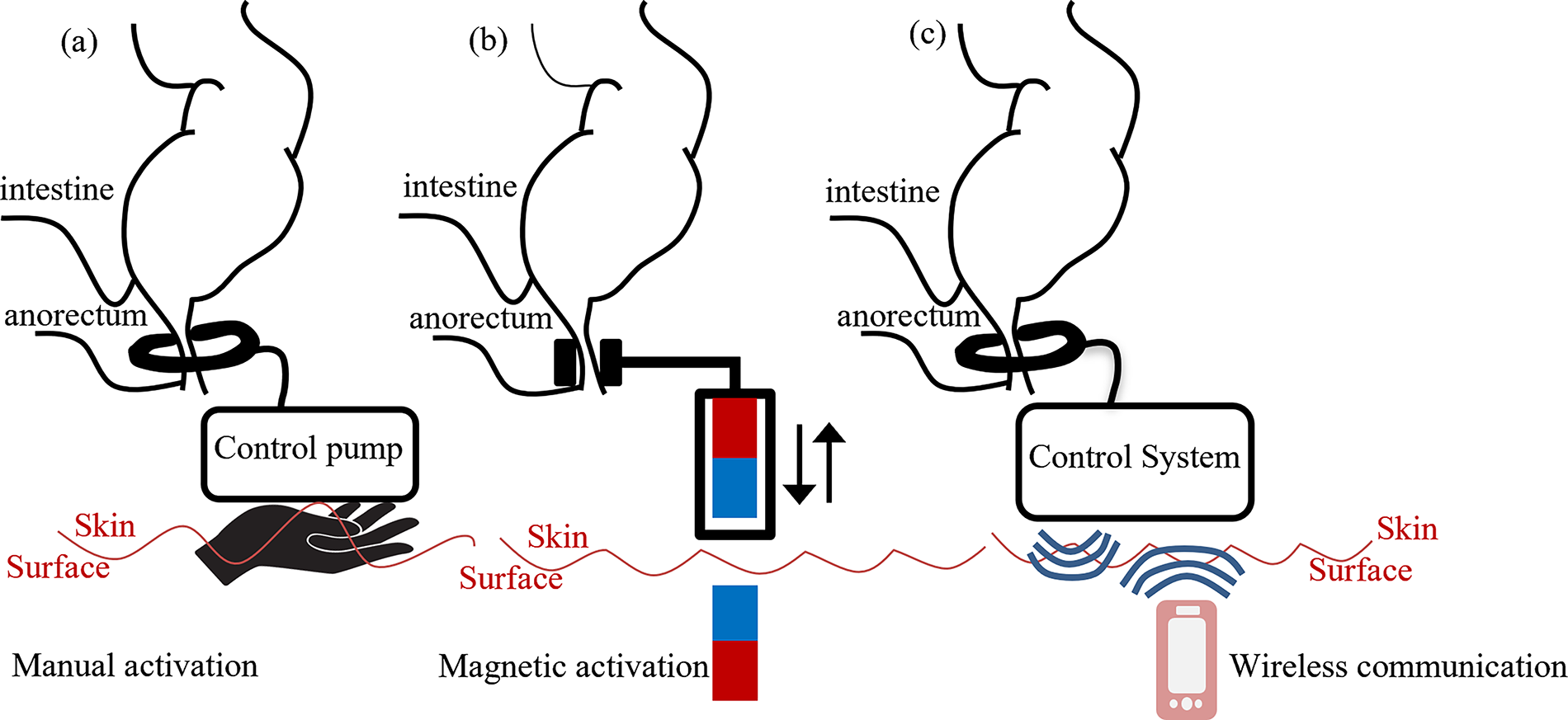
This review is based on an extensive literature search using PubMed, Web of Science, Google Scholar, and Espacenet-Patent. The search was conducted using keywords such as FI, defecation mechanism, AAS, and surgical treatment of FI. The most relevant English-language publications on FI and less-studied AAS systems were selected. Publications were chosen based on relevance and inclusion criteria, and reference lists were also screened for eligible studies. Of the initial 2248 records identified, 1754 were excluded for not meeting the inclusion criteria. The remaining 494 full-text articles were assessed for eligibility, and 422 were further excluded due to incomplete data or other reasons. Ultimately, 72 studies were included in the final analysis (Fig. 3).
PRISMA flow diagram of literature search.
Physiological Defecation Mechanism
Defecation is a highly complex neural reflex process (Fig. 4). 2 The primary muscles involved in defecation include the anal sphincter and the puborectalis muscle. 19 The anal sphincter surrounds the rectoanal canal and consists of an internal and an external component. The internal anal sphincter is composed of smooth muscle and maintains tonic contraction to keep the anus closed when defecation is not required. It relaxes during defecation. The external anal sphincter surrounds the internal sphincter and provides voluntary control to temporarily close the anal canal. 20 Bowel control at rest primarily depends on the internal anal sphincter, which requires minimal energy and can sustain prolonged contraction without fatigue. The puborectalis is a U-shaped muscle that loops around the lower rectum. During defecation, it relaxes to increase the anorectal angle, playing a key role in continence.21,22 Defecation is initiated when rectal distension reaches a certain threshold. When rectal volume reaches approximately 300 mL and intrarectal pressure increases to about 7.3 kPa, the defecation center in the spinal cord is activated, triggering rectal contraction. During defecation, the puborectalis muscle relaxes, increasing the anorectal angle, while the anal sphincter also relaxes, allowing the intestinal contents to be expelled by peristalsis. After defecation, the anal sphincter complex gradually contracts to reclose the anal canal.23,24
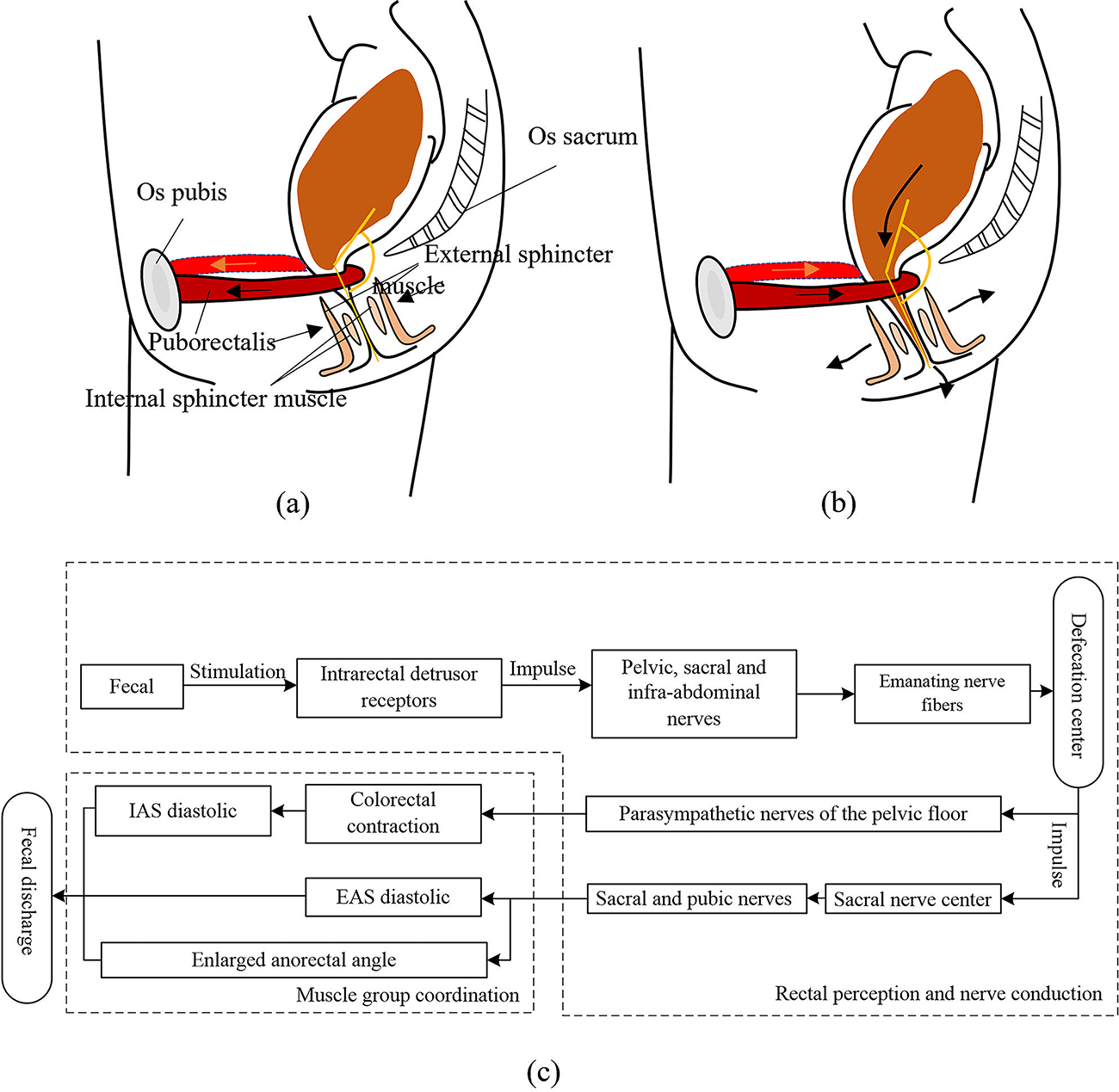
Defecation process.
Current Research on AASs
In 1987, Christiansen et al. proposed modifying the American Medical Systems 800—originally developed for treating urinary incontinence—for use in managing FI. The device was later adapted by the American Medical Corporation into an implantable AAS, which was approved by the Food and Drug Administration (FDA) in 2001. 25 Since then, numerous bionic AASs have been developed. These devices are generally classified into two categories based on their bionic principles: those that simulate changes in the anorectal angle via puborectalis muscle action, and those that replicate the contraction–relaxation function of the anal sphincter.
AASs based on bionic principles mimicking the puborectalis muscle
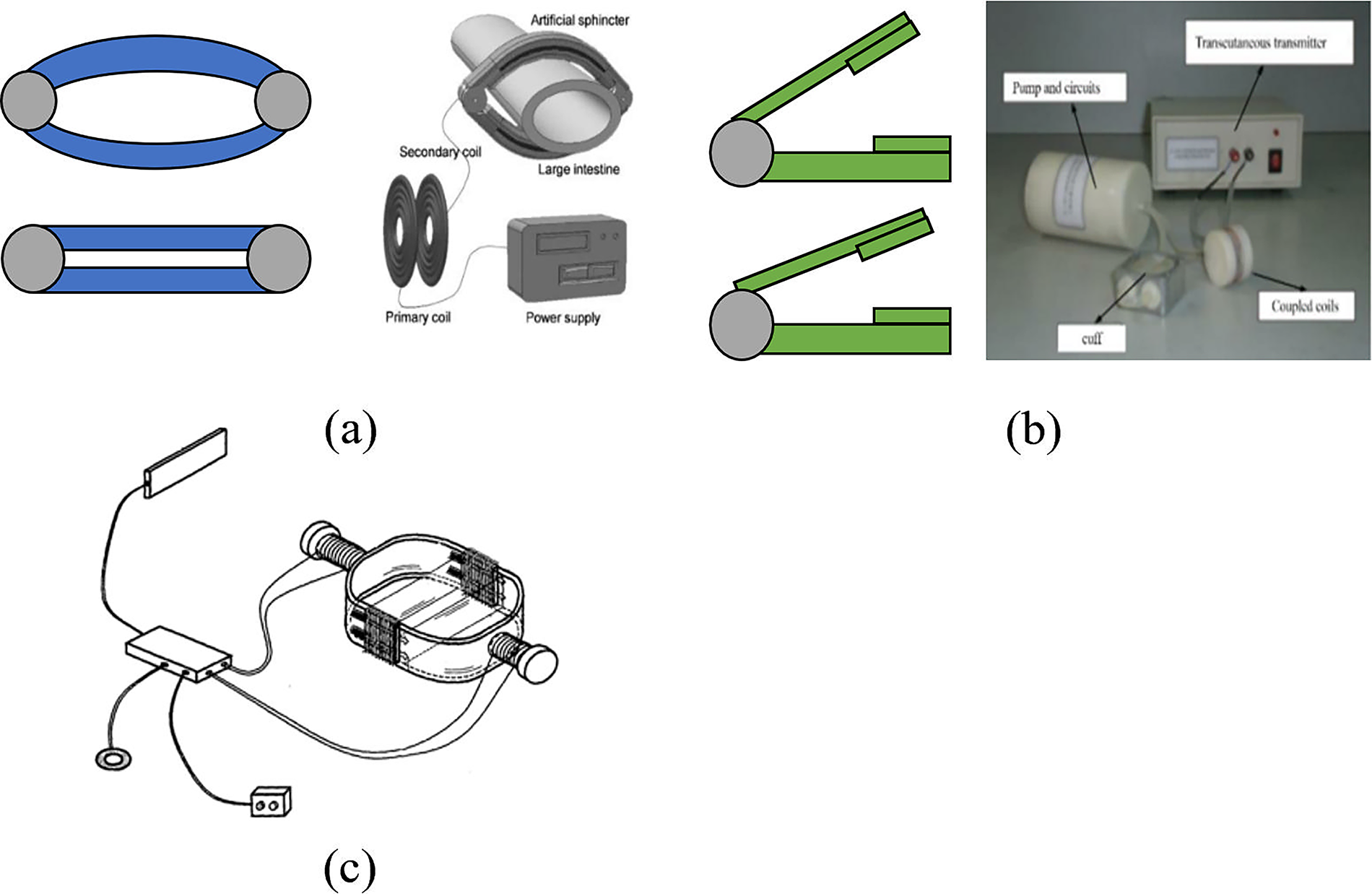
The bionic principle of AASs based on the puborectalis muscle is to reproduce anorectal angle modulation in order to maintain fecal continence during normal defecation. When activated, the prosthesis pulls the rectum to form an anorectal angle of approximately 90°. During defecation, the prosthesis gradually releases the rectum, increasing the anorectal angle and restoring normal evacuation function. Currently, such devices include the prosthetic anal sphincter (PAS), the shape memory alloy—based PAAS (PAAS-SMA), the puborectalis-type AAS (PAAS), and the newer version, N-PAAS (Fig. 5).
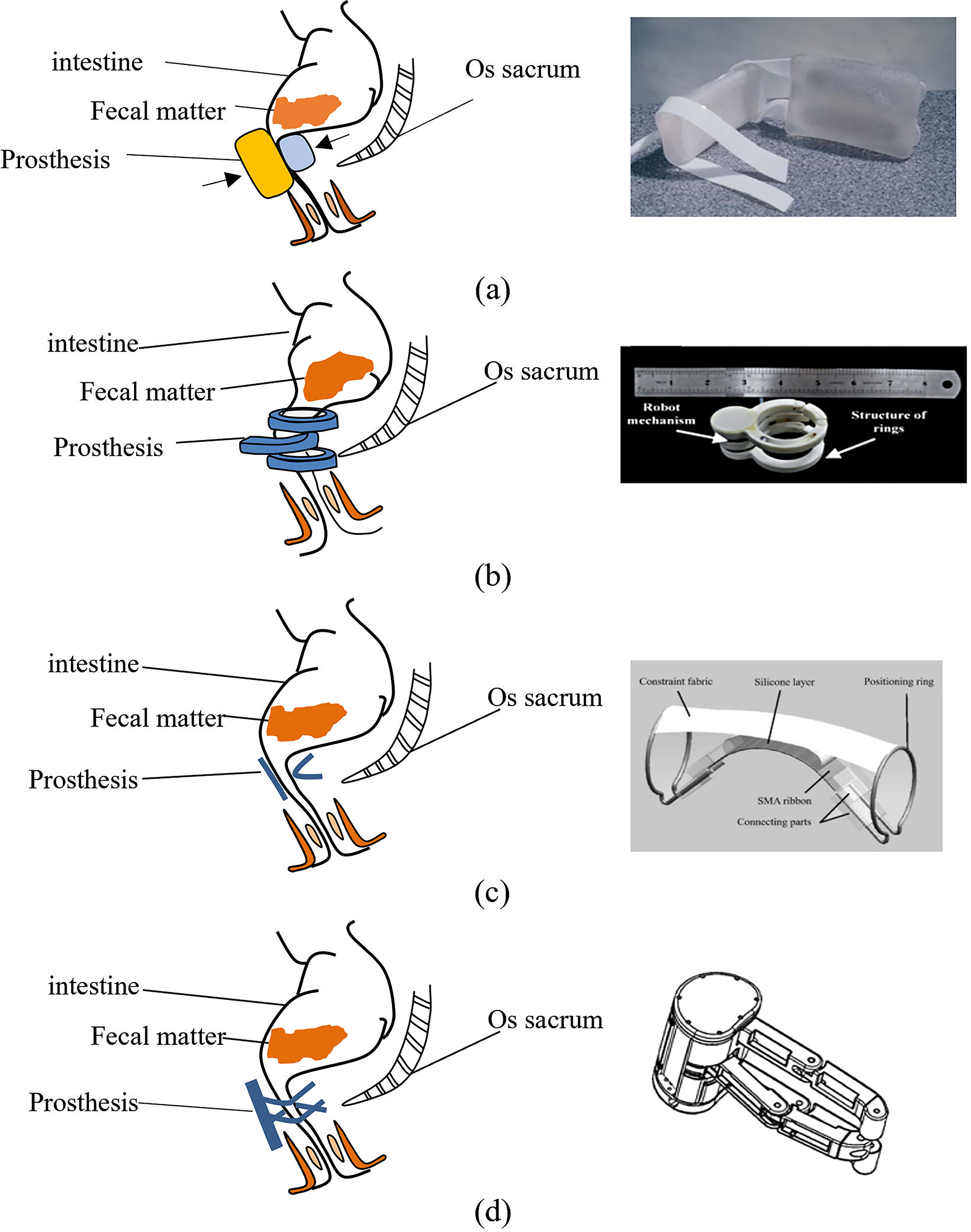
AASs mimicking the puborectalis muscle.
In 1997, Professor Finlay in the United Kingdom developed the PAS, which consists of a cuff prosthesis, a spherical reservoir pocket, and a water pump. 26 The cuff prosthesis comprises an expander and a pillow block filled with soft gel. This design’s core principle was to avoid localized high-pressure points by flattening and angulating the bowel. 27 During defecation, the patient presses the pump button, causing the fluid in the cuff to return to the reservoir. After defecation, the patient presses the button again, allowing fluid from the reservoir to refill the cuff, thereby clamping the bowel. 27
In 2012, Yue Wu et al. designed PAAS-SMA. 29 The device consists of Ti-51at%Ni SMA tapes, a silicone insulation layer, two positioning rings, and a restraint fabric. This device utilizes the shape memory effect of the Ti-Ni SMA as an actuator to provide functional assistance that mimics the puborectalis muscle’s action. 29 At normal body temperature (37°C), the SMA tapes remain bent, forming an anorectal angle that prevents the expulsion of intestinal contents. When the temperature is increased to 60°C, the SMA tapes straighten, enlarging the anorectal angle. As a result, the rectum is released, and the intestinal contents can be discharged. Upon cooling back to 37°C, the SMA tapes return to their bent shape, re-establishing the anorectal angle and closing the rectal outlet.
In 2017, Guozheng Yan et al. developed PAAS system, consisting of four components: an in vivo control module, an ex vivo control module, a transcutaneous energy transfer module, and a driver module. 28 The system integrated pressure sensors to provide feedback for reconstructing rectal sensation. 24 During normal operation, the prosthesis clamps the rectum and alters the anorectal angle to inhibit defecation. When intestinal pressure exceeds a preset threshold, the internal control module wirelessly transmits this information to a handheld remote-control device. If conditions are appropriate for defecation, the patient can activate the sphincter prosthesis using a handheld remote control. 24
In 2020, Guozheng Yan et al. designed N-PAAS based on PAAS. 30 N-PAAS differs from PAAS by replacing the two retaining rings with two movable operating arms. When the patient needs to defecate, the middle operating arm rotates to one side, allowing defecation to occur at the maximal anorectal angle. After defecation, the middle operating arm rotates to the opposite side, driven by a motor. The upper and lower operating arms then move in the opposite direction to the middle arm, reducing the anorectal angle and reclosing the anal canal. This biaxial, mechanically actuated design concept has been the basis for several subsequent advanced prototypes, such as the AAS based on a Novel Clamping Mechanism (AASNCM) and the Biaxial Actuated Artificial Sphincter (BAAS).31,32 Further refinements have included improving the transmission structure from traditional gears to a cam-follower system to enhance positional accuracy and self-locking capabilities, 33 and investigating materials with better biocompatibility, such as polyetheretherketone (PEEK). 21
AASs based on bionic principles mimicking the anal sphincter complex
AASs that mimic the movement of the anal sphincter complex are designed to reproduce the function of the natural sphincter, thereby achieving fecal continence and controlled release, ultimately restoring normal defecation. According to their occlusion mechanisms, such AASs can be categorized into circumferential occlusion and planar occlusion types.
AASs with circumferential occlusion
AASs with circumferential occlusion include a variety of designs, such as the artificial bowel sphincter (ABS), German AAS (GAAS), soft anal band (SAB), elastic-scale AAS (ES-AAS), magnetic-type AAS (MAS), water-pumped AAS system (WP-AASS), constant-force clamping AAS (CFC-AAS), as well as several novel patented concepts (Fig. 6 and Fig 7).
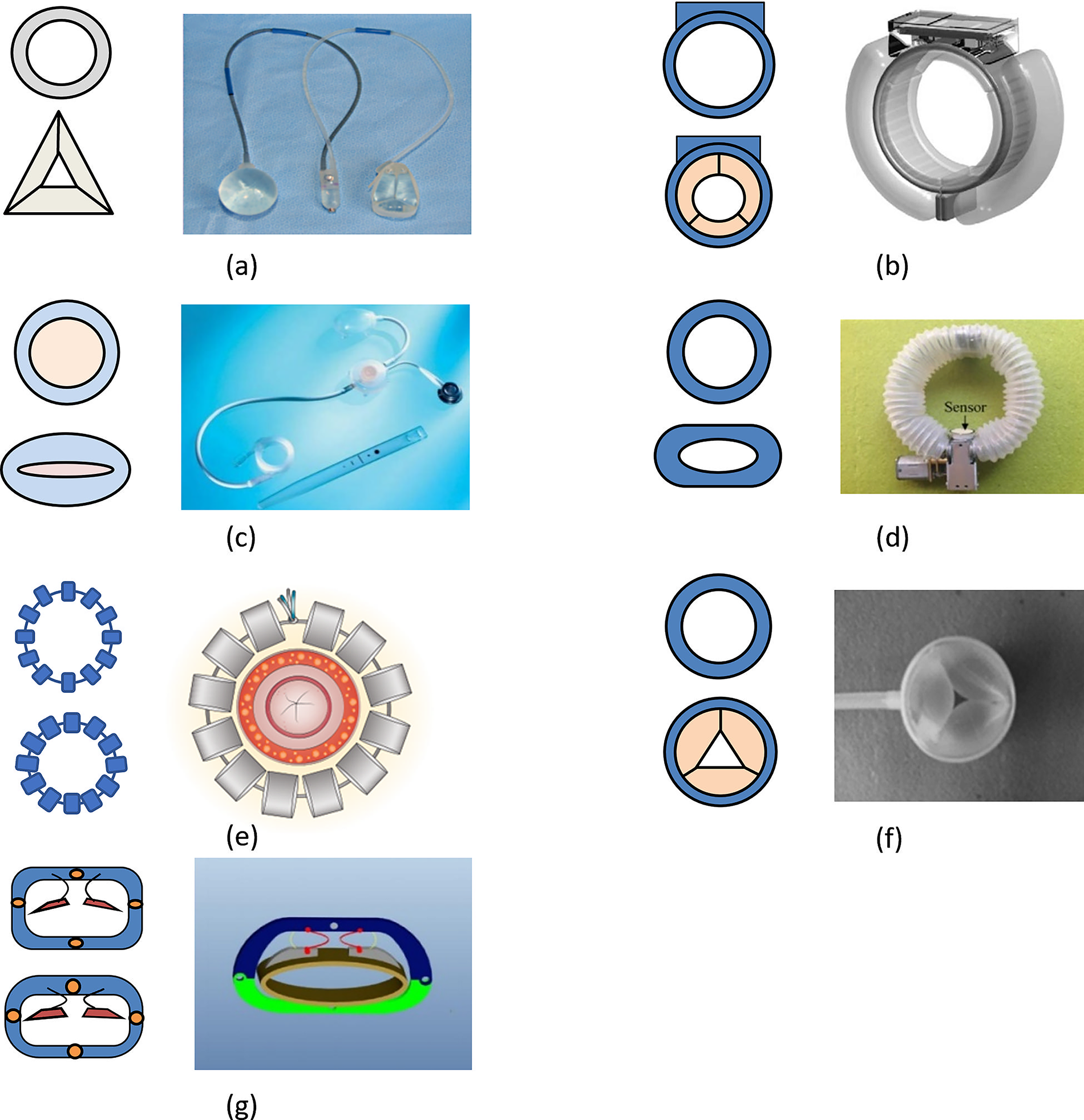
AASs with circumferential occlusion.
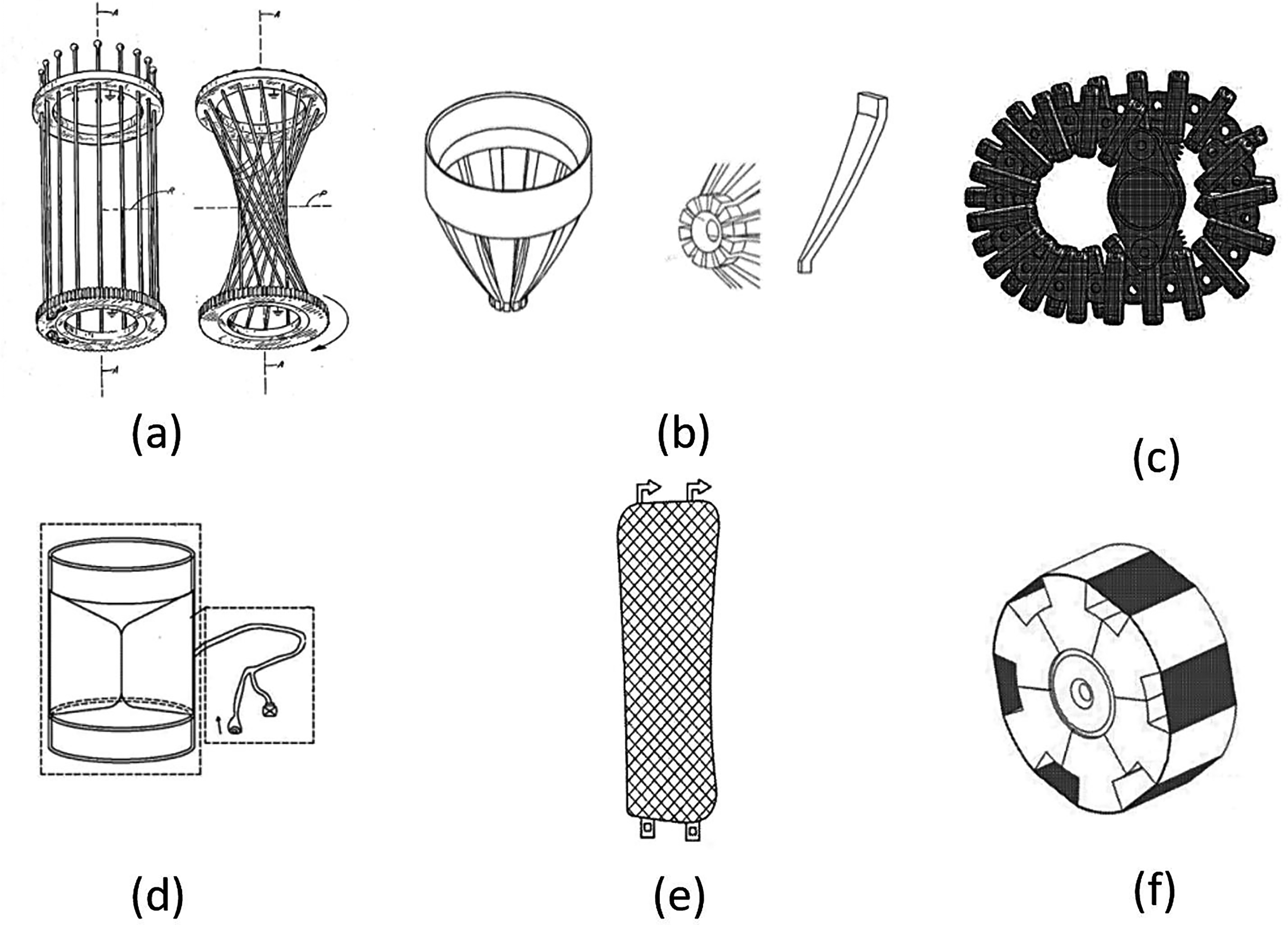
AASs with circumferential occlusion (patents).
In 1992, American Medical Systems designed the ABS, which consists of a cuffed prosthesis, a control pump, and a pressure-regulating balloon.34,35 This hydraulic system typically operates with a pressure-regulating balloon set between 91 and 110 cm H2O. 25 The device was approved by the United States FDA in 1999 and commercially released in 2001.25,36,57 To initiate defecation, fluid is transferred from the cuff to the pressure-regulating balloon, thereby opening the cuff. After defecation, the pressure-regulating balloon returns the fluid to the cuff, and the anal canal is closed again.36,58
In 2004, H. Schrag et al. proposed GASS (German Artificial Sphincter System) in Germany. This hydraulic AAS consists of an inflatable cuff, a fluid reservoir, and a bidirectional piezoelectric micropump. A key biomechanical innovation of GAAS is the use of this micropump for fluid transfer, with later versions utilizing multilayer piezo actuators to reduce the operating voltage to a safe level of <30 V. 38 It enables defecation by transferring fluid between the cuff and the reservoir. 38 The system’s components were later redesigned by Ruthmann et al. to meet the stringent requirements of implantable therapy and minimally invasive implantation. The updated design integrates all electrical and mechanical components into a compact unit. 38
In 2005, the SAB was developed in Austria. It consists of a cuff prosthesis, a reservoir balloon, a control valve, and a water pressure port. 39 From a biomechanical perspective, the SAB offers two potential advantages over the ABS. First, the occlusive pressure is not constant but is actively controlled by the patient. Second, patients can leave the cuff deflated for extended periods. 39 During defecation, the patient presses the valve button, allowing fluid to flow from the cuff into the reservoir balloon, thereby releasing the intestine. After defecation, the patient squeezes the subcutaneous reservoir balloon to pump saline back into the cuff, reclosing the intestine. Between 2005 and 2009, 43 patients underwent treatment with the SAB. Clinical trials showed that the SAB significantly improved patients’ symptoms. However, 48.8% of patients experienced complications such as infection and pain, and the devices had to be completely removed in nine cases. 40
In 2015, Guozheng Yan et al. developed the ES-AAS, 42 which consists of an annular elastic mechanism and an actuator. This device is mechanically, rather than hydraulically, driven. A key biomechanical design feature is the integration of a biological pressure sensor within the worm gearbox to provide feedback control. 42 The annular elastic mechanism consists of a spring encapsulated in a medical silicone corrugated tube. One end of the spring is anchored to the worm gear—worm transmission assembly. The actuator includes a steel cable, a worm gear and gearbox, and a micromotor. The ES-AAS controls spring contraction via worm gear transmission, ensuring that feces are securely clamped under appropriate pressure.
In 2008, Lehur et al. in France developed MAS, which consists of 12 connected magnetic beads typically placed around the anal canal. 43 To distribute pressure and prevent tissue damage, the titanium beads are designed with a “Roman arch” shape. 44 Under normal conditions, the magnetic beads attract one another, keeping the anal canal closed. When intestinal contents accumulate and intrarectal pressure rises beyond a threshold, the magnetic attraction is overcome, allowing the anal canal to open for defecation.44,59
In 2013, Guozheng Yan et al. designed the WP-AASS, which consists of a fluid-filled cuff, a transcutaneous energy transmission system, and a control unit.47,48 This system is driven by an electric micropump that controls the inflow and outflow of fluid, allowing for automated control rather than manual pumping. 48 The device achieves bowel clamping and relaxation by controlling the inflow and outflow of fluid within the cuff. In addition, the system is equipped with a pressure sensor to detect intestinal pressure, enabling reconstruction of fecal perception.47,48
In 2019, Minghui Wang et al. developed the CFC-AAS, a mechanical AAS featuring a constant-force clamping mechanism. 49 This device was specifically designed to enhance long-term biomechanical compatibility. Its core component is an optimized C-shaped superelastic SMA sheet that leverages the material’s stress plateau to deliver a nearly constant force.49,60 Building on this concept, a subsequent iteration introduced a flexible bionic design, which integrated the constant-force SMA element with a PEEK-based flexible frame and a bistable locking mechanism. 61
In 1983, Terry M. Haber et al. filed a patent for an AAS. 51 The device consists of a fixed ring, a rotating ring, and a connecting rod. During operation, rotating the ring drives the connecting rod to contract, thereby achieving bowel control.
In 2013, Hualing Chen et al. 52 filed a patent for an AAS, which consists of a sphincter prosthesis, a signal generator, and a pressure sensor. As fecal accumulation increases pressure on the sphincter, the pressure sensor transmits the signal to the signal generator, which then applies a positive voltage to the ionic polymer—metal composite (IPMC) actuator. The IPMC actuator generates an inward bending force to resist the pressure of intestinal contents, mimicking the self-sealing function of the anus and preventing fecal leakage. When the anal canal pressure reaches the defecation threshold and conditions permit defecation, the signal receiver applies a reverse voltage to the IPMC actuator. This causes the actuator to bend outward and open the canal, allowing feces to be discharged. After defecation, the power supply is cut off, and the IPMC actuator elastically returns to its initial state.
In 2014, Zhiwu Wang et al. 53 applied for a patent for an AAS with a finger buckle—type structure. The device consists of multiple flexible knuckle elements and a retractable actuator composed of a driving rope, two winch wheels, and a micromotor. During defecation, the winch wheels retract the driving rope, causing radial contraction of the knuckle elements and opening of the anal canal.
In 2015, Chunyuan Liu filed a patent for a circular blocking AAS. 54 The device comprises an artificial rectal lumen, an inner silicone rubber membrane that controls sphincter opening and closing, a sphincter capsule lumen, an intermediate silicone rubber sheet, and an outer three-dimensional woven polyvinyl mesh. When intestinal contents accumulate, pressure changes are transmitted through the inner silicone membrane to a pressure-sensing alarm device, which signals the need to defecate.
In 2018, Wenbai Li et al. 56 applied for a patent for a circumferential occlusive-type AAS, which consists of a sphincter prosthesis and a dielectric elastomer artificial muscle integrated with a flexible electrode block. The sphincter prosthesis is composed of several fan-shaped segments connected by an expansion spring, and the dielectric elastomer artificial muscle is positioned around these segments. When voltage is applied to the flexible electrode region, the dielectric elastomer artificial muscle relaxes accordingly. The elastic restorative force of the expansion spring causes the sphincter prosthesis to open. After defecation, the device automatically returns to a closed state.
In 2019, John R. Frigstad, St et al. 55 proposed a circumferential occlusion—type AAS characterized by multiple mesh openings. The device regulates the degree of anal canal expansion by adjusting the mesh size, thereby allowing or preventing defecation.
AASs with planar occlusion
AASs with planar occlusion include the magnetically controlled AAS (MC-AAS), the AAS with shape memory alloys (AS-SMA), and the novel mechanically driven AAS (NMD-AAS) (Fig. 8).
AASs with Planar Occlusion.
In 2002, LEE Hoon-Bum et al. patented the MC-AAS, which consists of a sphincter prosthesis, a sensing device, an actuator, and an on/off switch. 62 When the sensing device detects a defecation signal, the on/off switch adjusts the direction of current flow to activate or deactivate the electromagnet. This magnetic control enables closure or release of the anal canal.
In 2006, Yun Luo et al. at Tohoku University in Japan developed AS-SMA, which utilizes the shape memory effect of shape memory alloys. 63 A key biomechanical feature of this device is its “sandwich” mechanism, which compresses the bowel from two sides rather than radially squeezing it. 63 The device consists of two shape memory alloy plates connected by a central hinge. The SMA plates, which surround the anal canal, have a deformation temperature range of 47–52°C. At normal body temperature, the device remains closed, sealing the anal canal. When the SMA plates are continuously heated to their deformation range, they bend outward, opening the anal canal. AS-SMA was tested in animals for 3 months and demonstrated effective defecation control. 64
In 2010, Peng Zan et al. designed the NMD-AAS, which uses a mechanical clamping structure. 65 The device consists of a movable plate, a fixed plate, a micromotor, a silicone pad, and a telescopic mechanism. To inhibit defecation, the micromotor moves the movable plate toward the fixed plate until the anal canal is fully closed. When defecation is required, the micromotor runs in reverse, retracting the movable plate and releasing the anal canal. 66 Subsequent research from the same group has focused on optimizing this planar clamping actuator through finite element analysis (FEA) to ensure better biomechanical compatibility.67,68
Discussion
With advances in medical technology, AAS systems have emerged as a promising treatment for FI. Despite rapid progress, significant challenges remain in theoretical modeling, technical implementation, and especially clinical application. In the following, the advantages and disadvantages of different types of AAS will be summarized and compared, and engineering design considerations for future systems will be analyzed (Table 2).
Comparison of Various Artificial Anal Sphincters
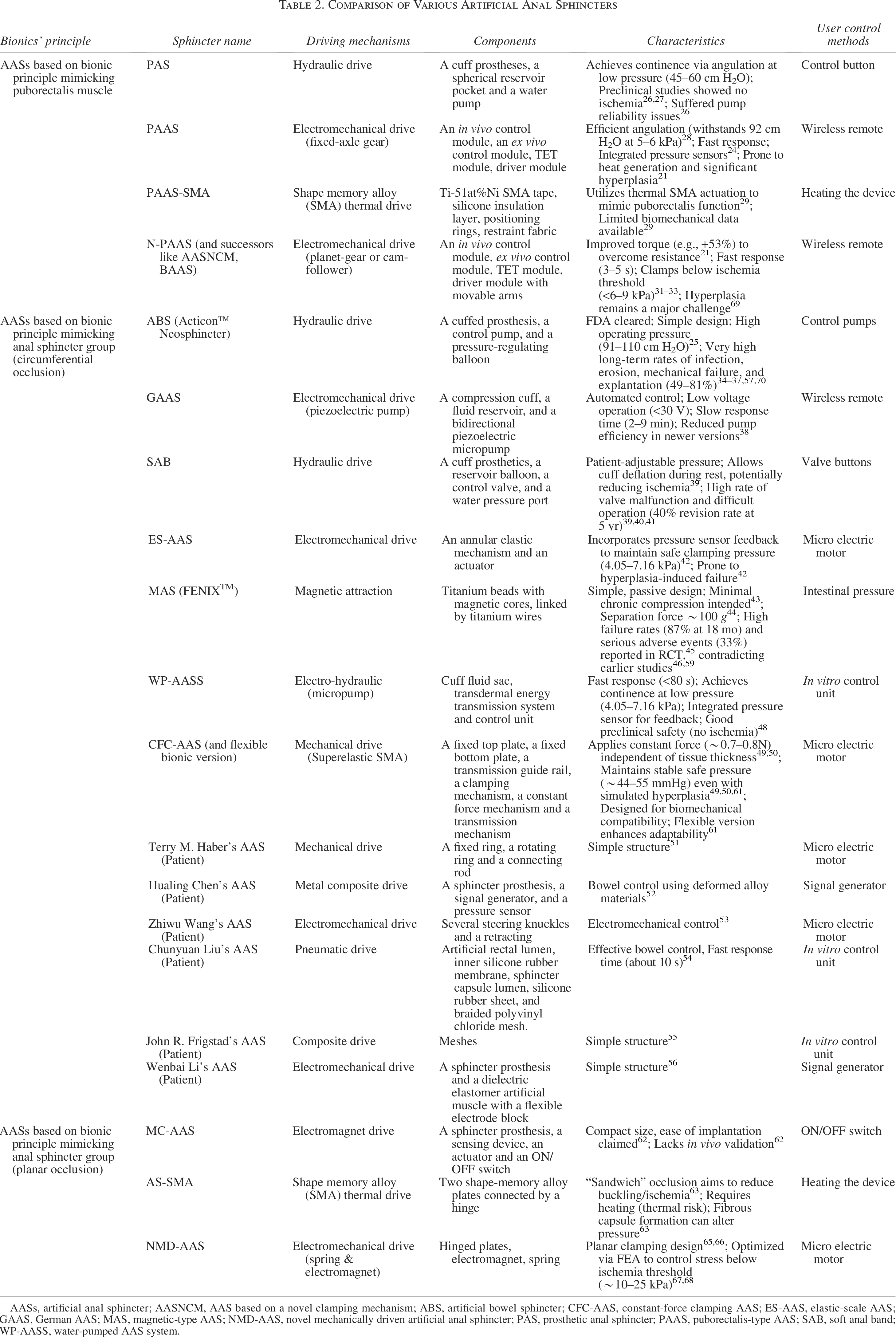
AASs, artificial anal sphincter; AASNCM, AAS based on a novel clamping mechanism; ABS, artificial bowel sphincter; CFC-AAS, constant-force clamping AAS; ES-AAS, elastic-scale AAS; GAAS, German AAS; MAS, magnetic-type AAS; NMD-AAS, novel mechanically driven artificial anal sphincter; PAS, prosthetic anal sphincter; PAAS, puborectalis-type AAS; SAB, soft anal band; WP-AASS, water-pumped AAS system.
A comparison of clinical performance
Comparing the prevalent failure modes reported in clinical studies reveals a direct link between a device’s underlying biomechanical design and its long-term clinical viability. Devices employing a high-pressure circumferential occlusion mechanism, such as the ABS, consistently demonstrate high rates of severe complications.34–36,57 Clinical manometric studies confirmed its biomechanical function, showing increased mean anal resting pressure, 70 but the high, constant pressure applied by the circular cuff (typically 91–110 cm H2O 25 ) is believed to be a major contributing factor to tissue ischemia and subsequent high rates of tissue erosion, infection, and mechanical failure.36,57 For instance, large cohort studies and systematic reviews report high explantation rates. A recent long-term study by van der Wilt et al. on 63 patients provided stark evidence of this biomechanical failure: after a median follow-up of 57 months, the device had been explanted in 49.2% of patients. The study reported a total of 101 reoperations, with the main reasons for revision being device failure and infection. At 5 years of follow-up, approximately 80% of the cohort had experienced a complication requiring surgery. 37 A study by Devesa et al. involving 43 patients reported functional issues, noting that 98% were unable to pass solid feces and 66% remained completely incontinent after ABS implantation. 71 These data strongly suggest that the fundamental design, relying on constant high pressure, leads to an unsustainable rate of clinical failure over the long term.
The SAB, another hydraulic cuff device, while reportedly having lower infection rates (9% in one series), 39 suffers from a high rate of technical revisions, primarily due to failures of its control valve, which patients often find difficult to operate.39,40 More recent long-term data confirm this failure pattern; in a cohort of 60 patients with a median follow-up of 5 years, the revision rate was 40%, mainly attributed to valve defects. Despite these technical challenges, 70% of patients retained a functioning implant at 5 years, with infection accounting for a 15% explantation rate. 45 This suggests that while its mechanical components are a point of weakness, the underlying biomechanical principle of adjustable, nonconstant pressure may lead to better long-term tissue compatibility compared to the ABS. Clinical manometry confirms its effectiveness, increasing mean resting pressure significantly. 40 However, initial trials also reported high complication rates (48.8% experiencing infection or pain, with 9 removals). 40
In contrast, devices based on noncompressive or alternative mechanical principles exhibit different failure patterns. The MAS, which uses passive magnetic force (requiring approx. 100 g separation force 43 ) initially showed a 5-year explantation or stoma creation rate of 23%, with pain and erosion still being notable complications. 46 Manometric studies showed increased anal resting pressure. 44 However, a more recent and large-scale randomized controlled trial (the sacral nerve stimulation versus the FENIXTM magnetic sphincter augmentation for adult faecal incontinence: a randomised investigation trial) reported a significantly higher rate of failure. In this trial, the MAS demonstrated a treatment failure rate of 87% at 18 months, and 33% of patients experienced a serious adverse event, including device erosion, pain, and defecatory dysfunction. Consequently, 30% of patients required device explantation. 45 These high complication rates strongly suggest that applying a constant, albeit passive, magnetic pressure carries a substantial risk of long-term tissue incompatibility and clinical failure.
For mechanically driven angulation devices like the PAAS and its successors (N-PAAS, AASNCM, BAAS), the primary clinical failure mode observed in preclinical studies is not pressure-induced necrosis but rather mechanical malfunction caused by the host’s biological response—specifically, hyperplasia formation around moving parts, which increases mechanical resistance and ultimately leads to device failure.21,69 Early animal studies with the PAS, however, showed no evidence of ischemic injury. 26 Subsequent iterations focused on improving torque output and material biocompatibility (e.g., using PEEK) to combat this hyperplasia. 21 Despite improvements, an 8-week in vivo study using the BAAS in piglets confirmed that severe hyperplastic wrapping leading to obstruction and device failure remains a critical hurdle, even though the fundamental defecation control function was verified. 69 SMA-based angulation devices such as PAAS-SMA, face potential thermal injury risks. 29
Planar occlusion devices such as AS-SMA, while aiming to reduce buckling risk, 63 also showed fibrous capsule formation in animal models, potentially altering occlusion pressure over time. 63 The heating required for actuation also presents thermal injury risks. 63
Hydraulic systems driven by electric micropumps, such as GAAS and WP-AASS, face their own challenges. While GAAS integrated components into a compact unit, its redesign reduced the effective fluid transport volume and resulted in slow inflation/deflation times (2–9 min). 38 The WP-AASS demonstrated good preclinical safety with no ischemic anomalies, but also experienced fibrous capsule formation and a mechanical failure (pressure sensor breakdown) during in vivo experiments. 47
A comparison of biomechanical design principles
The various AAS designs can be fundamentally distinguished by their core biomechanical strategies for achieving occlusion and actuation, each presenting unique advantages and challenges.
First, in terms of occlusion strategy, there is a clear dichotomy between high-pressure circumferential compression and low-pressure geometric modulation. The former, exemplified by the ABS and SAB, relies on applying fluid pressure—often in the range of 91–110 cm H2O for the ABS 25 —to physically squeeze the anal canal shut. This approach is powerful but inherently carries a high risk of inducing tissue ischemia, as the applied pressure often exceeds the capillary perfusion pressure of the anorectal tissue. 34 The latter strategy, employed by devices such as the PAS and PAAS family, uses angulation to create a mechanical kink, requiring significantly lower operating pressures (e.g., 45–60 cm H2O for the PAS), 26 and preclinical models demonstrated an absence of ischemic injury.26,27 In vitro tests on PAAS showed efficacy at low clamping pressures (5–6 kPa), 28 and later iterations such as AASNCM/BAAS demonstrated robust clamping forces (11.65–15.86 N) while maintaining clamping pressure within the safe range (<9.33 kPa), even during simulated defecation urges (e.g., 7.39 kPa).31–33 Other novel approaches, such as the planar “sandwich” compression of the AS-SMA 63 and the constant-force mechanism of the CFC-AAS, 49 represent further attempts to achieve a secure seal while minimizing tissue trauma. The NMD-AAS development involved significant biomechanical modeling, establishing a safety threshold of 4 kPa based on colonic blood flow analysis, 65 and subsequent FEA aimed to homogenize pressure distribution to stay below the 10 kPa perfusion threshold.67,68
Second, the actuation mechanisms directly influence device reliability and host response. Hydraulic systems (ABS, SAB, GAAS, WP-AASS) are prone to specific failures such as fluid leakage, cuff rupture, and valve/pump malfunction (e.g., SAB valve issues,39,41) and can have slow response times (e.g., 2–9 min for GAAS 42 vs. <80 s for WP-AASS 47 ). Electromechanical systems with moving parts (PAAS, N-PAAS and its successors, ES-AAS) offer faster, more precise control (e.g., 3–5 s for the AASNCM/BAAS family31,32) but introduce a dynamic interface with surrounding tissue, making them vulnerable to failure from fibrous capsule formation and hyperplasia, a failure mode explicitly observed in PAAS/BAAS animal studies.21,69 ES-AAS attempts to mitigate pressure risks via sensor feedback within a safe range (4.05–7.16 kPa). 42
Finally, devices driven by smart materials (MAS, AS-SMA, CFC-AAS) eliminate complex pumps and motors but introduce new biomechanical considerations. The MAS failure rates suggest issues with its passive magnetic pressure principle. 45 The AS-SMA faces challenges of thermal management (heating to 55°C 64 ) and pressure changes due to encapsulation. 63 The CFC-AAS, by using a superelastic SMA to deliver a constant force (∼0.8 N 50 ) independent of tissue deformation, directly targets the problem of pressure-induced ischemia. 49 Subsequent detailed FEA 60 and in vitro experiments on porcine intestine have validated this concept, showing that the device can maintain a stable clamping pressure (approx. 5.87 kPa or 44 mmHg, 50 later refined to 51.7 mmHg or ∼6.9 kPa 61 ) even when tissue thickness changes, a key feature for ensuring long-term biomechanical compatibility.50,60 The latest evolution of this design further incorporates a flexible PEEK frame to improve its bionic properties. 61
Future optimization directions for AASs
The clinical challenges faced by existing AASs, primarily rooted in biomechanical incompatibility and mechanical failure, demand a multipronged optimization strategy. Future designs must not only refine existing engineering principles but also integrate emerging technologies to create more intelligent and biologically compatible systems.
Enhancing engineering design and intelligence
Fundamental engineering optimizations remain critical. AAS devices must continue to follow lightweight design principles, pursuing further miniaturization of components such as gearmotors and control circuits. Concurrently, power management is crucial for extending device longevity; this includes optimizing low-power operation modes and developing safer, more efficient wireless energy transfer (TET) systems that minimize thermal output. A key limitation, however, is that even a perfectly engineered mechanical device still relies on simplistic feedback and manual control. To overcome this, future AASs must become more intelligent. The integration of smart sensing and AI offers a promising path. By applying advanced algorithms such as long short-term memory networks to analyze real-time pressure sensor data, future systems could learn to accurately distinguish the true urge to defecate from other pressure events (e.g., coughing, body movement). This would enable a “perception reconstruction” module that transforms the AAS from a passive implant into an intelligent, adaptive system capable of automated control. 72
The biohybrid approach to biomechanical compatibility
While engineering refinements can mitigate issues, the ultimate solution to chronic foreign body response, tissue erosion, and mechanical wear may lie in replacing problematic mechanical components with living, biological substitutes. This biohybrid approach represents a convergence of bionic engineering and regenerative medicine, aiming to create an AAS that is part mechanical and part biological.
The feasibility of creating the “biological” component of such a hybrid system is supported by significant progress in tissue engineering. Studies have successfully demonstrated the creation of implantable, functional “biosphincters” using autologous smooth muscle cells and neurons on scaffolds. These bioengineered tissues have been shown to restore anal resting pressure in small and large animal models, including nonhuman primates, proving their long-term viability and function.73,74 Advanced fabrication techniques such as 3D printing are also being used to create patient-specific, cell-laden myo-structures for sphincter defects. 75 The concept for a future biohybrid AAS would be to integrate such a lab-grown, living cuff, which is inherently biocompatible and capable of self-repair, with a reliable mechanical control and power system. This would truly optimize the AAS, potentially offering a permanent and fully integrated solution.
In summary, the optimal engineering directions for future clinical application AAS systems are outlined in (Fig. 9).
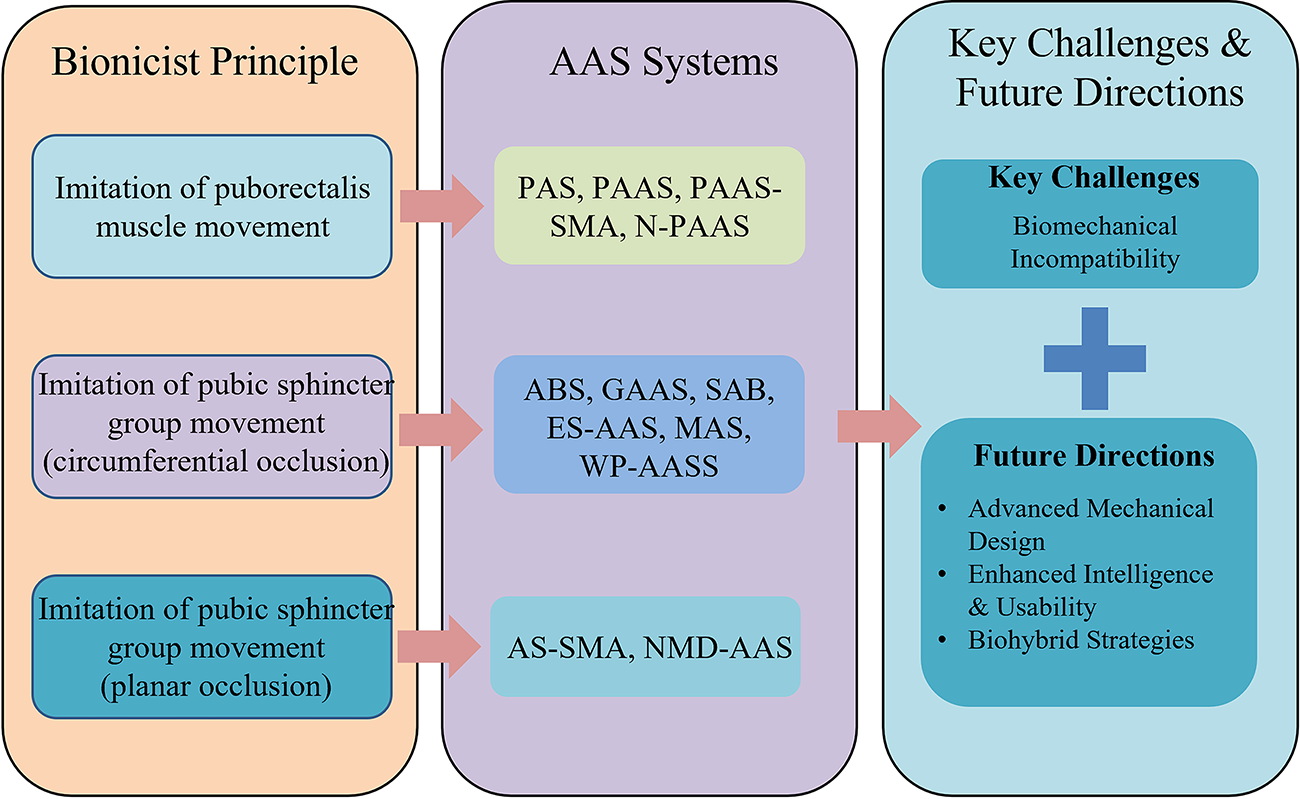
Future optimization goals for artificial anal sphincters.
Conclusion
FI significantly impacts patients’ lives, and while AASs offer a crucial reconstructive option for severe cases, their long-term clinical success remains hampered by significant limitations, primarily stemming from biomechanical incompatibility between the implant and the host tissue. This review analyzed various AAS designs through the lens of their underlying biomechanical principles and correlated these principles with observed clinical failure modes. High-pressure circumferential occlusion devices, such as the ABS, frequently lead to tissue damage and high explantation rates, highlighting the detrimental effects of sustained excessive pressure. Conversely, mechanically actuated systems mimicking puborectalis action, while operating at lower pressures, face distinct challenges related to the host tissue response, specifically hyperplasia formation around moving components leading to mechanical failure.
Addressing this fundamental issue of biomechanical incompatibility is therefore paramount for improving device safety and long-term effectiveness. Promising engineering strategies are emerging to mitigate these challenges. Advanced mechanical designs, such as constant-force mechanisms, aim to provide stable occlusion while minimizing the risk of pressure-induced tissue injury by adapting to tissue changes. Looking forward, the integration of smart sensing and AI holds potential for creating more adaptive, patient-responsive devices capable of reconstructing physiological perception. However, the ultimate path towards seamless, long-term integration may lie in biohybrid approaches. By converging bionic engineering with regenerative medicine principles, future systems could potentially replace failure-prone mechanical components with tissue-engineered constructs, such as lab-grown biosphincters. This strategy represents a paradigm shift towards achieving true biological harmony. Continued innovation focused squarely on enhancing biomechanical compatibility, through both advanced engineering and the integration of biological solutions, is crucial for advancing the clinical success of artificial sphincter systems in treating FI.
Authors’ Contributions
M.W.: Conceptualization, resources, formal analysis, supervision, writing—original draft, writing—review and editing, project administration, and funding acquisition. Y.Z.: Writing—review and editing, conceptualization, investigation, data curation, and visualization. Y.L.: Writing—original draft, formal analysis, data curation, and visualization. H.Y.: Writing—review and editing.
Footnotes
Disclosure Statement
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.