
Abstract
The repair and reconstruction of oral mucosal defects are critical for restoring both function and aesthetics of the oral cavity. Tissue engineering, which integrates principles from engineering and life sciences, has enabled the development of biological substitutes that closely mimic the native structure and function of oral mucosa, significantly reducing the risks and complications associated with autologous transplantation. With the rapid advancement of tissue-engineered oral mucosa (TEOM) technology, its applications in regenerative medicine and oral disease modeling have become increasingly prominent. In recent years, innovative strategies such as the development of organoids, prevascularization, immunomodulation, and dermal–epidermal junction biomimicry have emerged, providing effective solutions to challenges related to inadequate vascularization, immune dysregulation, and mechanical performance in TEOM constructs. In addition, the application of cutting-edge manufacturing technologies such as 3D bioprinting has accelerated the translation of TEOM toward clinical use. This review outlines the fundamental principles, design strategies, and potential applications of TEOM, and discusses novel approaches and challenges that must be addressed to facilitate its clinical implementation.
Impact Statement
This review provides a critical synthesis of recent advances in tissue-engineered oral mucosa, emphasizing cutting-edge methodologies in biomaterial development, cell engineering, and microenvironment modulation. By identifying unresolved challenges such as vascularization and immunomodulation, and proposing innovative strategies, including organoids and smart biomaterials, this article provides a valuable framework for researchers and clinicians striving to translate laboratory breakthroughs into effective regenerative therapies. This integrative perspective is poised to accelerate progress in oral mucosal repair across a variety of clinical applications.
Keywords
Composition and Function of Oral Mucosa
The oral mucosa is the soft, pink, moist tissue lining the entire inner surface of the mouth. Structurally and functionally similar to skin, the normal human oral mucosa consists of a stratified squamous epithelium anchored to a dense connective tissue layer by a specialized basement membrane. 1 However, the oral mucosa exhibits unique physiological characteristics, such as its pink color due to rich blood supply, a moist surface, higher permeability, and the absence of skin appendages such as hair follicles, sebaceous glands, and sweat glands. 1 The primary cells of the oral epithelium are keratinocytes, which are tightly connected by desmosomes and arranged in well-defined layers.2,3 Beneath the epithelium lies the lamina propria, mainly composed of blood vessels, nerves, fibroblasts, and macrophages, all embedded within an extracellular matrix (ECM) made up of type I and III collagen fibers and elastin. The deeper rete ridges of the epithelium interlock closely with the papillary projections of the lamina propria. 1 Between these two layers is the basement membrane, featuring a nanometer-scale ultrastructure and maintaining its integrity through hemidesmosomes. 4
The keratinization patterns of the oral mucosa vary according to anatomical location and function, with the epithelium classified as keratinized (masticatory mucosa), nonkeratinized (lining mucosa), or both (specialized mucosa of the dorsal tongue). 1 In contrast, the skin epithelium is generally keratinized regardless of its location on the body. 1 Subjected to greater mechanical stress, the hard palate and gingiva are covered by a keratinized stratified squamous epithelium, while the soft palate, inner lips, ventral tongue, buccal mucosa, and floor of the mouth are lined by a nonkeratinized stratified squamous epithelium, providing enhanced flexibility and resilience.
The oral mucosa provides essential protective, sensory, and secretory functions. When the oral mucosa is damaged, the disruption of barrier function can lead to tissue fluid loss, increase the risk of infection, and may result in functional limitations. 5 Therefore, it is necessary to reconstruct its anatomical and physiological characteristics in time to prevent the occurrence of complication. 6 The healing process of oral mucosa follows stages similar to skin: hemostasis, inflammation, proliferation, and remodeling. The concrescence of epithelium around the teeth after periodontal treatment or tooth extraction is completed after 7–14 days, 7 whereas the formation of biological width around the implant and the maturation of barrier function take 6–8 weeks. 8 Compared with the skin, the wound of oral mucosa usually heals faster with minimal scarring, which is attributed to the rich blood supply, active regulation of stem cells, and a moist environment, which is more favorable for mucosal healing. In addition, the involvement of keratinocytes in epithelial remodeling and proinflammatory responses in the oral cavity also contributes to wound healing. 9
Limitations of Conventional Oral Mucosa Grafts
Oral mucosal reconstruction is necessary due to gum recession, infection, trauma, radiation therapy, and congenital or pathological lesions that result in incomplete oral mucosal structure and function. The results of reconstruction will depend on appropriate therapy, defect size, and the quality of soft tissue present at the injury site. 10
Autologous transplantation and allogeneic tissue transplantation, as important approaches for oral repair and regeneration, are widely applied in oral mucosal defects, scar repair, and complex maxillofacial soft tissue reconstruction.11,12 Despite donor-site morbidity and limited availability, autologous transplants remain the gold standard for oral mucosa repair. 12 Autografts taken from different sites of the oral cavity, such as free gingival grafts, buccal mucosal grafts, and palatal mucosal grafts, are commonly used for repairing oral soft tissue defects without rejection reactions. However, studies have shown that autologous tissue transplantation is often associated with postoperative pain, sensory abnormalities, infection, scar formation, and surgical complications. 13 Moreover, flap transplantation is often accompanied by tissue swelling in the operated area, which affects aesthetics and occlusal function. Despite its effectiveness, these limitations highlight the need for alternative reconstruction methods.
Allografts become essential when autografts struggle to meet the demand, especially for treating large or severe wounds. 14 Freeze–dried allogeneic skin grafts were one of the earliest products introduced for gingival mucosal surgery. They were initially used as substitutes for free gingival grafts and combined with coronally advanced flap to enhance keratinized tissue. 15 However, the source of allogeneic skin or mucosal flaps is not inexhaustible. The characteristics of exogenous substitutes are different from the real oral and maxillofacial skin and mucosa, 16 which means even if the flaps are successfully transplanted, it is difficult to maintain the secretion and lubrication functions of the oral mucosa.
Therefore, enhancing tissue regeneration capabilities or developing functional biological substitutes represents a critical breakthrough for future oral mucosal defect repair and regenerative therapies.17,18 Tissue-engineered oral mucosa (TEOM) holds great promise to effectively promote tissue reconstruction while avoiding the risks and complications of autologous tissue harvesting.
The Tissue Engineering Principles of Tissue-Engineered Oral Mucosa
Tissue engineering is an approach that combines biomaterials, cells, and bioactive factors to create tissue or organ substitutes. 19 The unique structural and functional characteristics of the oral mucosa, such as its rapid healing ability, low scar formation rate, and specialized immune regulatory environment, provide important design principles for tissue engineering.19,20
Cells
The natural repair process of the oral mucosa involves the synergistic actions of multiple cell types. 20 Keratinocytes, as the main cellular components of the mucosal epithelium, are responsible for forming the stratified epithelial structure. 21 They rapidly proliferate and migrate to cover the damaged area, thereby restoring the barrier function of the mucosa. Fibroblasts, located in the lamina propria, participate in the synthesis and remodeling of the ECM, while also regulating keratinocyte proliferation and differentiation through the secretion of growth factors. 22 Mesenchymal stem cells (MSCs) not only differentiate into epithelial cells and fibroblasts to replenish damaged tissue but also modulate the local immune environment by secreting various cytokines and promoting inflammation resolution and tissue regeneration.23,24
In the field of tissue engineering, introducing these cells or exogenous stem cells into injury sites simulates the cellular dynamics of natural healing and enhances the repair effect. 25 Intercellular communication mechanisms, especially the transfer of miRNAs and bioactive molecules via extracellular vesicles, regulate immune responses, cell migration, and differentiation, further improving the microenvironment and promoting coordinated advancement of the repair process. 26 Precise regulation of cellular behavior and their interactions form the foundation for successful oral mucosal tissue engineering.
Signaling molecules
Oral mucosal healing depends on various growth factors such as epidermal growth factor, basic fibroblast growth factor, transforming growth factor-β (TGF-β), as well as bioactive molecules such as endogenous vesicles.27–30 These signaling molecules regulate cell chemotaxis, proliferation, and differentiation by activating endogenous repair mechanisms, thereby promoting repair at different stages of the injury site.29–31 Although multiple signaling factors act synergistically during wound healing, a single growth factor can still activate complex signaling networks to trigger downstream regeneration-related cellular responses and matrix remodeling.31,32 Effective tissue engineering strategies need to incorporate these natural regulatory mechanisms, mimicking and enhancing the signaling networks involved in the natural healing processes of oral mucosal wounds. By exogenous release or scaffold-mediated delivery of these signaling molecules, endogenous cells can be activated and targeted to promote their migration and functional expression. Traditional direct injection methods often fail to maintain effective concentrations due to short half-lives and rapid diffusion. To address this, various carrier systems have been developed. The decellularized ECM (dECM), rich in natural signaling factors and possessing a complex 3D structure, is widely used to construct highly biomimetic repair scaffolds. 33 Its naturally retained ligand–receptor binding sites promote cell adhesion and migration, while also modulating the local immune environment to reduce inflammation and fibrosis. Moreover, the combined use of nanocarriers, hydrogels, and porous materials enables synergistic delivery of multiple factors, regulating cell behavior while enhancing tissue regeneration efficiency. 34
Scaffolds
Scaffolds can not only provide support for tissue cells, but also offer a favorable space for cell adhesion and growth, which is very important to the construction of TEOM. An ideal scaffold should have good biocompatibility, biological stability, and appropriate porosity to allow for culture medium perfusion, intrinsic vascularization, sufficient fibroblast infiltration and proliferation, and intercellular communication. 35 The physiological characteristics of the oral mucosa require scaffolds to not only meet basic mechanical strength but also to mimic the unique flexibility and elasticity of the mucosa. In terms of material types, scaffolds can be made from natural polymers, synthetic polymers, or their composites. Natural materials such as collagen and fibrin are commonly chosen scaffolds due to their close resemblance to the physiological environment, but their mechanical properties are relatively weak.36,37 Synthetic polymer materials such as polyglycolic acid, polylactic acid, and trimethylene carbonate possess controllable mechanical properties and degradation rates but lack bioactivity, necessitating surface modification or combination with natural materials for improvement.38,39
In recent years, the application of dECM has overcome the limitations of traditional scaffold materials. This material removes cells while preserving ECM components, providing a more authentic extracellular environment due to its natural structure and bioactivity, effectively promoting cell adhesion and signal transduction.33,40,41 Combined with 3D bioprinting technology, researchers can manufacture customized scaffolds with complex multiscale porous structures and bioactivity on demand, showing great promise for precise repair of the oral mucosa.41,42 Moreover, the development of smart responsive materials enables scaffolds to respond to environmental stimuli (such as pH, enzyme activity, temperature), dynamically regulating cell behavior and molecular release, greatly enriching the control of the microenvironment in oral mucosal tissue engineering. 43
Tissue engineering strategies
As mentioned above, tissue engineering strategies can be mainly divided into two categories: cell-mediated strategies and signaling molecule-driven strategies. Cell-mediated strategies involve seeding living cells onto scaffolds to reconstruct complex interactions between cells as well as between cells and the ECM, thereby mimicking the healing process of autografts. Signaling molecule-driven strategies, on the contrary, utilize scaffolds loaded or soaked with specific signaling factors to activate the repair potential of host endogenous cells. Many commercially available biological products are based on this second principle, simplifying the operational procedures and effectively reducing treatment costs.
Potential Application of Tissue-Engineered Oral Mucosa
Disease modeling
TEOM can serve as a disease model for oral ulcers, cancer, and cleft palate, replacing animal testing in drug or vaccine development.12,44 As an in vitro model, TEOM should be reproducible, possess excellent handling properties and biodegradability, and its degradation rate should be adjustable according to specific needs.
In the early years, monolayer cell cultures (2D culture models) were commonly used for cytotoxicity detection, but the models always fail to capture critical cell–cytokine interactions that influence experimental outcomes. More biologically relevant 3D models have since emerged, enabling investigation of periodontal or mucosal infections through microbial integration to study host–pathogen interactions, epithelial damage, and therapeutic approaches.45–47 In 2013, Colley et al. utilized the TEOM model to investigate the effects of radiotherapy on oral mucosa. The model was irradiated with 20 Gy of radiation, and observations at 21 days postirradiation revealed a significant thinning of the TEOM epithelial layer and an increase in cell apoptosis. Compared with the nonirradiated group, there was a notable increase in the secretion of interleukin-6, chemokine-8, and granulocyte-macrophage colony-stimulating factor. These changes are consistent with the histological manifestations of radiation-induced stomatitis. 48 In addition, 3D TEOM models facilitate implant–soft tissue interaction studies. In 2012, Chai et al. tested machined, polished, sandblasted, and Ti Unite implant surfaces, observing hemidesmosome-like structures under scanning electron microscopy, indicating the formation of an epithelial connection between the implants and the oral mucosa. 49
While 3D TEOM models better replicate in vivo conditions, limitations still persist, including the drop of seed cells from the scaffold, the absence of mucin in saliva, the insufficient presence of bacteria and immune responses, as well as a relatively static culture environment. These constraints hinder clinical translation of in vitro findings. Future efforts should leverage advanced technologies to better mimic physiological microenvironments.50–52
Regenerative medicine
TEOM can be used to treat epithelial or mucosal wounds outside the oral cavity, such as reconstruction of the urethra 53 and genital tract, 54 or repair of esophageal contracture. 55 As early as 2004, Nishida et al. used cultured autologous oral mucosal epithelial cell sheets for the treatment of bilateral limbal stem cell deficiency and discovered their clinical applicability in restoring vision. 56 In the same year, Nakamura et al. designed a bilayer TEOM composed of autologous oral mucosal keratinocytes and exfoliated human amniotic membrane (hAM), and demonstrated in later clinical trials that its derivative products can be effective in treating severe ocular surface diseases. 57 After that, some researchers have successfully established autologous tissue-engineered buccal mucosa by simultaneously inoculating oral keratinocytes and fibroblasts onto the dermis for urethral reconstruction.58,59 Due to its excellent anatomical and physiological properties, such as strong regenerative ability, abundant vascularity, and good operability, oral mucosa is considered advantageous for cell-based tissue engineering and has guiding significance for the reconstruction of other epithelial tissues.
While extraoral applications have advanced, the primary objective of TEOM remains addressing intraoral tissue deficiencies—particularly for periodontal regeneration around implants/teeth and postsurgical maxillofacial reconstruction. Despite progress, most TEOM research remains in the laboratory or preclinical stages, with no commercial products yet available for clinical mucosal repair. A 2015 clinical study by Amemiya et al. shows success using a bilayer TEOM (autologous keratinocytes with hAM) to repair minor oral defects. 60 In recent years, a new method has been proposed to directly produce an osteo-mucosal engineered construct, and it has been proven to have the potential to improve cell ingrowth and tissue integration. However, the author suggests that this kind of construct still needs further optimization to become a common graft in clinical practice. 61
Novel Strategies and Challenges of TEOM
Organoids
Regenerating oral mucosa is challenging due to the complex tissue architecture, diverse cell types, and dynamic interactions within the oral environment, which traditional 2D culture systems fail to replicate accurately. Therefore, oral mucosal organoids have emerged as promising models that can better mimic the native tissue structure and function, addressing these limitations and advancing both fundamental research and clinical applications. Oral mucosal organoids can faithfully replicate the tissue architecture and physiological functions of the oral mucosa. By combining oral epithelial cells with basal layer connective tissue cells and using 3D in vitro culture techniques, researchers have successfully constructed oral mucosal organoids featuring typical stratified structures and complex cell-to-cell interactions.62,63 These organoids include KRT14+ stem cells in the basal layer, KRT13+ differentiated cells in the spinous layer, and keratinized cells in the superficial layer. Their transepithelial electrical resistance reaches as high as 413 ± 138 Ω·cm2, providing strong evidence of a functional barrier. In addition, the organoids express molecular markers similar to native oral tissues, such as the antimicrobial peptide HBD3 and the pattern recognition receptor TLR3, and are capable of responding to pathogenic stimuli. 63 Some oral mucosal organoids even have the ability to reconstruct specialized functional units, such as taste bud organoids, further expanding their application potential. 64
Oral mucosal organoids not only serve as ideal models for studying the development and repair mechanisms of the oral mucosa but also have become important tools in regenerative medicine. Their remarkable tissue regenerative capacity holds promise as an ideal source for future oral mucosal regeneration and transplantation therapies. However, the research and application of oral mucosal organoids still face some limitations. Although the research and application of oral mucosal organoids have shown great potential, there are still some limitations in this field. First, the establishment and maintenance of oral mucosal organoids require sophisticated techniques and conditions, limiting their promotion and widespread application. Second, we have seen studies on the pathological mechanisms and drug evaluation of oral diseases, however, less research has been done in practical oral tissue repair and regeneration. Further exploration is still needed to effectively transform these organoids into clinical applications.
Prevascularization
Since oral mucosa is a highly vascularized tissue, most of the TEOMs reimplanted into the body rely on the vascular bed of the recipient site to supply oxygen and nutrients. When the area of the defect is large, the vascular bed cannot provide sufficient blood supply in the initial stages of reimplantation, leading to graft necrosis and ultimately resulting in transplantation failure. 65 To address this issue, researchers have explored the use of prevascularization strategies to enhance the nutrient and oxygen supply of TEOM. This approach involves coculturing endothelial cells (ECs) with supporting cells such as fibroblasts, MSCs, or pericytes derived from stem cells within the biological scaffold to promote the self-assembly of vascular progenitor cells into functional vascular networks.44,66 Supporting cells not only construct the structural framework by secreting ECM components such as collagen but also create a proangiogenic microenvironment by releasing various angiogenic factors, including VEGF, FGF-2, and TGF-β. 44 Zhou and colleagues constructed vascularized TEOM using ECs, human gingival fibroblasts, and human gingival epithelial cells in combination with a scaffold, and successfully promoted the repair of tissue damage.67,68 Building upon this foundation, researchers have further developed scaffolds with large pores to accelerate the growth of fibrovascular tissue, or utilized injectable 3D scaffolds to release potent angiogenic factors, thereby promoting blood vessel formation.69,70 Moreover, Tra et al. demonstrated that hyperbaric oxygen therapy posttransplantation upregulated key growth factors (KGF, VEGF, PIGF), emphasizing microenvironmental influences on vascular integration. 71 Despite progress, most approaches remain unvalidated in animal models, and clinical translation is still distant. Tissue engineering progress has been hindered by the lack of deep infiltration of vascular networks, insufficient functional maturity, and inefficient integration with host vasculature.
Electrospinning, 72 3D bioprinting, 73 and microfluidic organ-on-a-chip technology, 74 as innovative approaches for prevascularization in tissue-engineered organ models, enable precise regulation of the vascular microenvironment and the high-fidelity replication of complex spatial structures. Future research must integrate vascular induction principles into functional tissue design, thereby promoting the field to a new level.
Immunomodulation
The regulation of the immune microenvironment in TEOM is shifting from traditional inflammation suppression to precise immune modulation, emphasizing precise control over the functions of immune cells and their spatiotemporal dynamics.75–77 Currently, although the regulation of macrophage polarization from M1 to M2 has been extensively studied, deeper exploration into its epigenetic and metabolic regulatory mechanisms, such as the role of histone-modifying enzymes during polarization, is more promising.78,79 Moreover, the construction of the immune microenvironment has transcended the limitation of single cell types and is gradually integrating the functions of adaptive immune cells such as regulatory T cells and dendritic cells. By using gene editing and immune engineering technologies to activate specific immune clusters, dual goals of immune tolerance and regenerative promotion are achieved.80,81 This multidimensional and multicellular collaborative regulation, especially combined with the spatiotemporal release capabilities of smart biomaterials, can effectively avoid the side effects and relapse risks associated with traditional immunosuppression. Cutting-edge manufacturing technologies such as 3D printing can construct layered and multicellular microenvironments, enabling spatial arrangement and functional interactions between immune cells and repair cells, thereby promoting immune regulation and tissue remodeling.82,83 Metal-organic framework materials, with their high-specific surface area and tunable structural characteristics, can achieve efficient encapsulation and controlled release of immune regulatory factors, precisely modulating local immune responses and enhancing immune tolerance and anti-inflammatory effects. 84
Future directions should focus on elucidating nonclassical signaling pathways and intercellular metabolic coupling mechanisms between immune cells and oral mucosal tissues, driving immune-regulating materials toward dynamic and adaptive systems to achieve intelligent autonomous regulation of the immune microenvironment.
Dermal–epidermal junction mimics
An ideal full-thickness TEOM requires epithelial and connective layers interconnected by a basement membrane with characteristic dermal–epidermal junction (DEJ) architecture—a wavy interface of epithelial rete ridges and dermal papillae. 85 However, most TEOMs utilize flat scaffolds that fail to replicate the intricate undulating microstructure of DEJ, which adversely affects the directional proliferation and differentiation of cells as well as the biomechanical properties of the grafts, representing a critical technical challenge that needs to be addressed.
To address this challenge, researchers have utilized high-precision micronano fabrication techniques such as soft lithography and microelectromechanical systems to produce collagen scaffolds with micron-scale undulating patterns on a natural tilapia scale-derived type I collagen substrate, thereby achieving a biomimetic interlocking structure of connective tissue papillae and epithelial rete ridges.86–88 These micropatterned scaffolds significantly enhance keratinocyte proliferation, migration, and uniform distribution, while accelerating the deposition of basement membrane proteins, thus improving the maturity and stability of DEJ-like structures in TEOM models. Moreover, these scaffolds can withstand repeated tensile and shear stresses characteristic of the oral environment, preventing plastic deformation or rupture of the implanted tissue. Similar to the undulating microarchitecture, the basement membrane as a component of the DEJ plays a critical role in maintaining adhesion between the epithelium and the lamina propria, as well as mediating cellular signaling. The basement membrane exhibits a complex nanoscale architecture and unique biochemical composition, posing significant challenges for its replication. 89 In recent years, researchers have made important strides toward fabricating biomimetic basement membrane substitutes tailored for oral mucosa by utilizing porous polymer membranes, hydrogels, and electrospun nanofibers, combined with coculture strategies involving fibroblasts and keratinocytes.90–92 These DEJ-mimicking scaffolds thus offer a biomimetic platform for developing skin or mucosal substitutes, bridging experimental models and clinical regenerative applications.
3D bioprinting
Fibroblast infiltration is also a key challenge in oral mucosal tissue engineering.93,94 Fibroblasts seeded on scaffolds provide the foundation for epithelial cell attachment, but improper porosity severely compromises tissue quality. Low-porosity collagen membranes block fibroblast migration, disrupting essential fibroblast–keratinocyte cross talk, while excessive porosity permits keratinocyte invasion, creating aberrant epithelial islands. 93 Thus, scaffold porosity and pore size are critical for optimal cell infiltration. With the advent of 3D bioprinting technology, researchers can combine gelatin, elastin, and sodium hyaluronate to create a hybrid barrier membrane with tailored pore size on each side to guide osteoblast, fibroblast, and keratinocyte growth for tissue regeneration. 95 This technology offers a promising solution to balance scaffold properties for effective TEOM development. 96 As mentioned above, 3D bioprinting also enables precise spatial patterning of multiple cell types and bioactive factors, facilitating the integration of prevascularization and immunomodulation strategies within the scaffold design.73,82,83 This integrated approach holds great potential to overcome current limitations and accelerate the clinical translation of functional TEOM models.
Discussion
Over the past few decades, regenerative medicine has continuously advanced, with research methods evolving from traditional 2D cell cultures to scaffold-based 3D cultures, followed by the development of tissue-engineered models. Nowadays, organoid and organ-on-a-chip technologies are widely adopted (Fig. 1). In recent years, strategies such as 3D bioprinting and prevascularization have significantly enhanced the structural complexity and functional performance of TEOM, accelerating its clinical translation. The advancement of TEOM not only offers new approaches for the repair of oral soft tissue defects but also facilitates the shift from conventional autografts toward functional biological substitutes.97,98
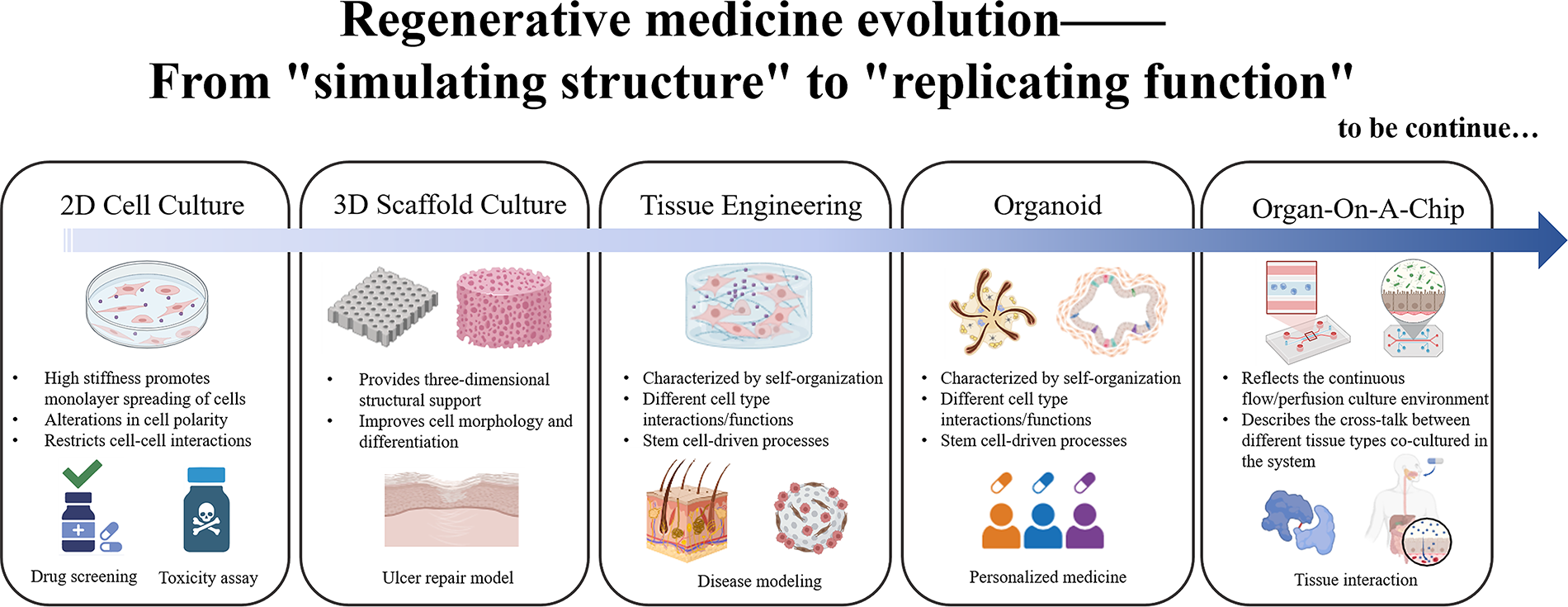
The development process of regenerative medicine.
Nevertheless, TEOM still faces considerable challenges.52,99 First, the complex tissue architecture and cellular heterogeneity limit the accurate replication of native oral mucosal functions, particularly in vascular network formation and integration of the immune microenvironment. Second, issues related to the biological stability, safety of biomaterials, and long-term functional maintenance of the models hinder clinical translation and application. Third, achieving precise immunomodulation to reduce rejection while promoting effective tissue integration remains a critical bottleneck. Future research should focus on integrating multidisciplinary technologies with precise regulatory strategies to expedite the clinical translation of TEOM and promote its practical application and scalable development in oral mucosal regeneration.100,101
Authors’ Contributions
Z.W.L. collected and summarized the references and wrote the article. S.T.W. prepared the literature and figures. S.Y., Z.L.W., and N.H. searched and analyzed the references and were involved in drafting the article. Q.S. and J.X. made substantial contributions to the conception, design, and critical revision of the article. H.C.L. conceived the idea of the review and revised the article. All the authors read and approved the final article.
Footnotes
Author Disclosure Statement
The authors declare that the article was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Funding Information
This work was supported by the National Natural Science Foundation of China (No. 82170985).