
Abstract
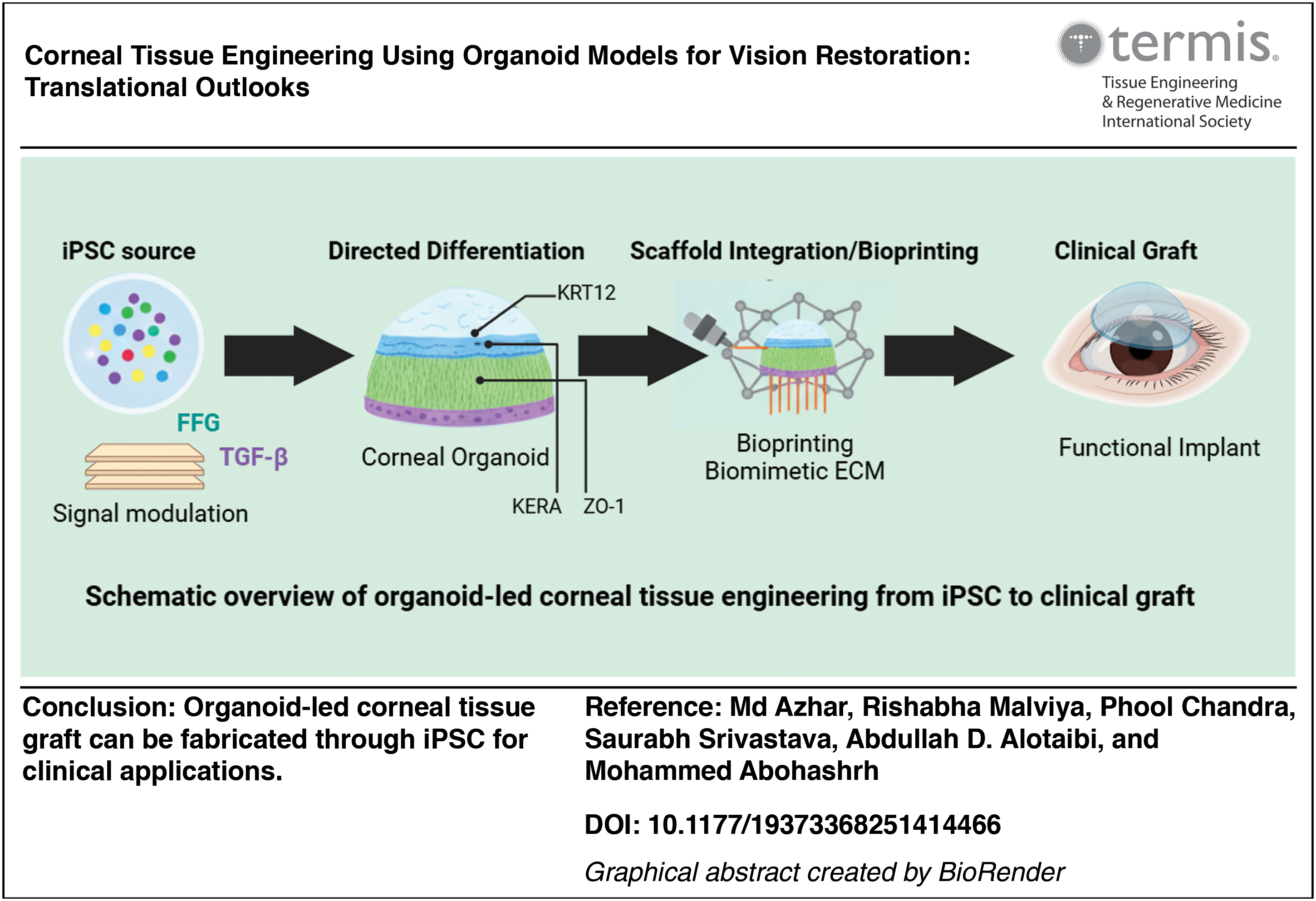
Corneal blindness has been a significant, in most cases, reversible cause of visual impairment worldwide due to donor deficiency and donor graft failure, which has encouraged the consideration of donor-independent techniques for regeneration. This review aims to discuss the advances in corneal organoid-based tissue engineering and its potential application in the translation to vision restoration. This review was conducted through an analysis of publications related to corneal organoids, biomaterials, bioprinting, preclinical models, and early human studies, published between 2005-2025 in Scopus, Web of Science, Google Scholar, PubMed, and WHO. In vitro corneal organoids from iPSCs and ESCs have a multilayered epithelium, stroma-like extracellular matrix, and intermittent endothelial phenotypes. In animal models and in vitro, they show lineage, light transmittance, and functional analysis indicators. Printing and microfabrication work with dECM gelMA bioinks. Despite batch variation, graft-scale production, endothelial pumps, and relevant aspects of translation, such as GMP-grade production, repeatability, biosafety certification, etc. It exhibited close to physiological transparency and biomechanics in quantifying with the original cornea, and demonstrates translational potential. The use of induced pluripotent stem cells and bioengineered corneal constructs has shown good first-in-human and preclinical trials. In conclusion, it is possible to say that the corneal organoid procedures are the potential solution to lessening reliance on donors and making therapeutic modalities as personalized as possible, but they demand standardized methodologies, GMP-level upscaling, solid safety data, and clinical trials before they can be adopted widely. This review presents a comprehensive overview of the progress in iPSC-derived corneal organoids, bio printing, and the development of biomaterials, and presents their respective advancements on their way to translation into the clinical setting in the field of corneal engineering and donor-independent restoration of vision.
Impact Statement
This review presents a comprehensive overview of the progress in induced pluripotent stem-cell-derived corneal organoids, bioprinting, and the development of biomaterials and presents their respective advancements on their way to translation into the clinical setting in the field of corneal engineering and donor-independent restoration of vision.
Introduction
Corneal disease has been one of the major causes of the loss and impairment of vision globally. As reported by the World Health Organization (WHO) and global blindness statistics, approximately one billion individuals experience the impairment of vision that can be prevented with corneal opacities, taking up more than five million cases each year.1–3 In global surveys and eye-bank statistics, there is a fundamental mismatch between demand and available corneas (about one donated cornea per dozen patients in some areas), which perpetuates long waiting lists and curable vision loss across the world.4–6 The persistent mismatch between supply and demand of the donors, which is exacerbated by the occurrence of graft failure and immunological rejection, underlines the necessity of donor-independent regenerative therapies. Owing to the reestablishment of the tissue hierarchy of the cornea in vitro, tissue engineering and stem-cell-based organoids are immunocompatible and repeatable transplant options that avoid dependency on donors. Routine treatment, penetrating and lamellar corneal transplantation, can restore vision but is limited by donor shortages, surgical difficulty, tissue-handling logistics, and immunologic failure. Rejection and long-term graft failure have been reported by the indication and risk profile, with huge proportions of patients experiencing rejection episodes or delayed graft loss, especially in high-risk beds or repeat procedures.4,7–9 Limbal stem-cell transplants and cell therapies offer an alternative in the treatment of select epithelial disorders, but are limited by scaling, durability, and manufacturing uniformity restrictions.10–12 As a result, there is a growing urgency to use regenerative strategies that do not rely on cadaveric tissue. 13
The solutions to these challenges include tissue engineering and organoids. Organoids: 3D self-assembling tissues of stem cells and pluripotent or mature progenitor cells that reenact multicellular organization, developmental signaling, and some extracellular matrix (ECM) properties unavailable to 2D cultures. They are chemotactic agents of disease modeling, drug discovery, and potentially in autograft generation.14–16 Preclinical and first-in-human trials involving stem-cell-derived corneal cells and bioengineered corneal constructs show both the feasibility of functional restoration and less dependence on donors. Although they are feasible, organoid platforms have significant translational issues such as absence of vascularization and neural integration, small-scale, and immune compatibility issues that hinder direct clinical application.17–19 Altogether, corneal organoid systems provide a physiological three-dimensional capability to the translational pipelines that connect the bench discoveries with vision restoration in the clinics.
This review discusses the morbidity of corneal blindness, the constraints of organ transplantation, and why organoid-based tissue engineering is rational. It addresses the recent developments in the field of corneal organoids and their integration with biomaterials and the translational capabilities of vision restoration. The search approach involved in this of the literature (2005–2025) of articles in Scopus, Web of Science, Google Scholar, PubMed, and WHO, on the topic of corneal organoids, tissue engineering, and regenerative medicine.
Corneal Anatomy and Physiology of Tissue Engineering
The cornea is a highly ordered multilaminar tissue, the structure and physiological processes of which provide rigorous tissue engineering goals. It consists, anterior to posterior, of the stratified, nonkeratinized epithelium (basal, wing, and superficial cells), the thin acellular Bowman layer, the thick collagenous stroma (keratocytes embedded in regularly arrayed type I collagen lamellae), the Descemet membrane, and the monolayered endothelium that conveys deturgescence and pump functions.20–22 The stroma constitutes approximately 90% of the corneal thickness, and its transparency relies critically on the consistency of the collagen fibril diameter, even interfibrillar separation, and orthogonal lamellar arrangement, which are visualized and measured with nonlinear optical imaging, including second-harmonic generation (SHG) and other methods.23,24 The membrane of Descemet is an exclusive basement membrane that is composed and biomechanically regulated differently, whereas the endothelium sustains stromal dehydration by an active system of pumps and leaks (Na+/K+-ATPase, bicarbonate/anion transporters, and aquaporins) to maintain transparency and refractive characteristics.25–27
The goals of engineering a functional corneal substitute would hence be (i) optical transparency (high coherent light transmittance and minimum scattering), (ii) proper anterior curvature and thickness to recreate refractive power, (iii) epithelial barrier properties and the right innervation to sustain hydration and trophic support, (iv) stromal biomechanics (tensile modulus and lamellar alignment), and (v) endothelial pump activity.20,26,28 Quantitative measures are used to assess constructs such as central corneal thickness (usually ∼500–550 µm in humans), percent light transmittance over visible wavelengths, stromal substitute elastic/tensile modulus, collagen architecture (SHG coherence/anisotropy indices), and lineage-specific molecular markers (e.g., KRT3/12 corneal epithelium, KERA/ALDH3A1 keratocytes, ZO-1, and Na+/K+-ATPase for epithelium).20,29,30
The engineering design of the cornea is informed by the structural and physiological structure of the eye. The guided scaffold surface porosity and wettability under the influence of the epithelium-layered barrier facilitate epithelial adhesion and renewal. 31 The uniformly oriented collagen fibrils that make up the stromal lamellae provide design features of anisotropy and transparency of scaffolds. 32 Hydrogel permeability and ion exchange conditions to retain deturgescence are determined by the presence of an endothelial layer that supports the ionic and osmotic balance by the activity of NA+/K+-ATPase. It is thus important that these biomechanical and biochemical cues are integrated when recreating the functions of the native corneal tissue in tissue-engineered constructs. 33 This is because such structural–functional relationships are important in designing physiologically viable corneal substitutes.
These features are not easy to reproduce in engineered models. To achieve low scattering, the stromal lamellar architecture on a submicron scale is required, which is difficult to print with most bulk hydrogels and with the majority of printing technologies.23,30,34 The organoid-derived stromal matrices and gelatin methacryloyl (GelMA)/decellularized corneal ECM (dECM)-based bioprinted constructs have, however, demonstrated partial collagen alignment and optical transmittance of 85–88% of the clear range of the cornea in nature of 0.3–0.7 MPa tensile modulus. 35 Second, to maintain a sustained, functional endothelial monolayer with stable pump activity without stimulating edema or fibrosis, cell phenotype and tight junction formation must be regulated.36,37 Third, the capacity to integrate innervation with a stable epithelial barrier (such as mucin/tear film interactions) is seldom considered in simple constructs but is critical to physiology and graft survival. 38 Fourth, biofabrication strategies, including aligned matrices, controlled crosslinking, and low light scattering additives, are in line with natural mechanics (anisotropic tensile strength and curvature) and retain transparency.27,39 Last, the functional assays that correlate in vitro measures (e.g., transmittance, pump assays) with in vivo graft clarity and refractive outcome are yet to be standardized, hindering head-to-head comparison across studies.20,25,40 Figure 1 compares the native cornea’s microanatomy with the engineered organoid.
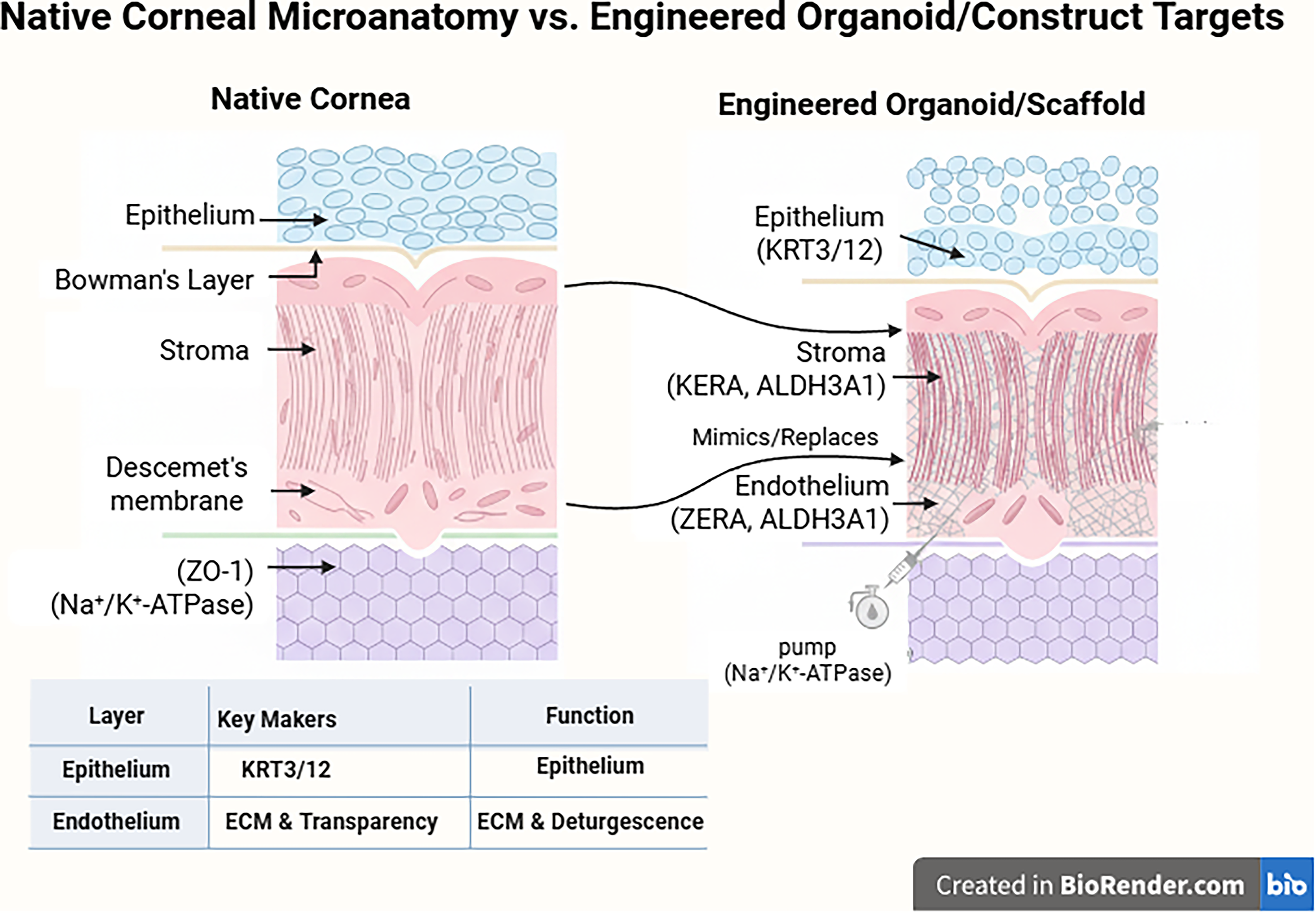
Native cornea versus engineered organoid targets. ECM, extracellular matrix.
As there are mechanical, biological, optical, and anatomical limitations to corneal organoids and grafts, high fidelity objectives can be reached through multicellular and layer-based native ECM 3D organoid models.
Overview of Corneal Tissue Engineering Strategies
There are three major types of tissue engineering approaches for the cornea: scaffold-based constructs, cell-based therapies, and hybrid techniques that utilize a combination of cells, scaffolds, and biological signals. 41 Scaffolds are based on natural ECM (decellularized corneal matrix, collagen, gelatin, recombinant human collagen) or plastic polymers (PEG, PLGA, PCL). Synthetic polymers can be engineered to have their mechanical properties and degradation behavior adjusted, although often they must be functionalized on their surface in order to form corneal cell phenotypes and minimize light scattering. Natural ECM scaffolds are bioactive and native ligands to facilitate cell adhesion and phenotype, but lot-to-lot changes might exist.41–45 Recent developments have been recombinant and dual cross-linked collagen structures, which are intended to be more transparent and easier to work with during surgery. 32
Cell-based strategies are intended to restore specific compartments of the corneas. Limbal stem cell transplantation (autologous or allogenic), such as cultivated limbal epithelial transplantation and simple limbal epithelial transplantation, has demonstrated efficacy in ocular surface reconstruction in limbal stem cell deficiency, but consequences vary based on etiology, immune status, and graft management.46,47 One cell type of interest, mesenchymal stem/stromal cells (MSCs), has been explored as supporting epithelial cells, stromal repair, and endothelial rescue through the actions of paracrine and immunomodulatory, preclinical, and early clinical evidence. It suggests that MSCs reduce inflammation, support wound repair, and have the potential to enhance endothelial recovery, although longer safety and standard dosing remain unresolved issues.48–50 The induced pluripotent stem cell (iPSC)-derived corneal lineages provide a limitless autologous source of cells and have expedited translational interest. 10
New hybrid approaches incorporate cell populations with engineered scaffolds and regulated release of growth factors or extracellular vesicles to speed up maturation and integration. Methods comprise cell-seeded decellularized matrices, bioactive collagen implants, and 3D bioprinting that incorporates lamellar architecture and curvature, as well as locating cells in spatially defined layers.44,45,51,52 The first translation breakthrough was a new translational breakthrough of a minimally invasive cell-free recombinant collagen implant in preclinical feasibility trials. Bioengineered stromal substitutes have been proven to have viable paths to decreased donor reliance with Phase I trials (NCT04653922).19,32
Although improvements have been made, the constraints remain: scaffold optical clarity versus mechanical strength trade-offs, variability in cell survival/function following implantation, immunological risk of allogeneic cells, and scalable genetically modified organoid (GMO) manufacturability. These limitations, especially the inability to recreate multicellular 3D microarchitecture and deposit native ECM, lead to organoid-based approaches that more accurately mimic the complexity of corneal tissues for modeling, screening, and potentially creating autologous grafts.
Conventional scaffold-based and cell-based systems are useful in part to do reconstruction, but are incapable of producing the initial heterogeneity of cells or the self-assembly of the ECM. Organoid systems address these issues by allowing multicellular differentiation to proceed naturally, self-assembly of ECM, and increased physiological reminisce. They represent the regenerative model of the cornea’s next generation.
Organoid Technology: Principles and Relevance to Corneal Tissue Engineering
Organoids are tissue surrogates (three-dimensional and multicellular) that can be formed through the intrinsic self-organization of progenitor cells under specified culture conditions. They differentiate the important features of organ architecture, cell-type diversity, and developmental signaling by integrating cell-intrinsic programs alongside ECM signals and lax culture conditions. They are qualitatively distinct from simple cell aggregates or monolayered cultures. This hallmark of biology, self-organization, multilineage differentiation, and emergent 3D architecture, provides organoids with high fidelity to model-level interaction and development.53–57
Practically, 3D cornea constructions are easily differentiated. Three-dimensional cell groups are known as spheroids. They are physically more relevant and organized than 2D cultures, but not as complex as organoids, which are more capable of self-assembling and performing organ-like functions. 58 The organoids are three-dimensional structures constructed using the stem cells that self-organize and resemble organs. Explant cultures are sections of original tissue that have retained their form and cell content. Full-thickness structures that have been biofabricated resemble the structure of the eye but do not self-organize. They are constructed through scaffolding or additive constructions. To sum up, an engineering aggregation is a spheroid, a self-organizing mini-tissue is an organoid, and a native tissue fragment is an explant.58–60
There are two main methods for producing organoids: Uninstructed or self-organizing techniques let pluripotent stem cells (PSCs) or tissue fragments develop naturally (e.g., cerebral organoids from embryoid bodies in Matrigel), while directed-differentiation approaches use developmental signals, such as wingless-related integration site (WNT), bone morphogenetic protein (BMP), fibroblast growth factor (FGF), and transforming growth factor-beta (TGF-beta) modulators, to guide PSCs into specific lineages before 3D culture and maturation. 61 Culture formats include ECM-based gels such as Matrigel and collagen, air–liquid interfaces (ALI), spinning bioreactors, and microfluidic platforms; using microfabrication and bioreactor control improves consistency and efficiency.53,54,59,62,63
In the context of corneal tissue engineering, organoids are more advantageous. They are capable of forming a multilayered epithelial network, stromal-like compartments, secretory of native ECM (collagens, proteoglycans), and a primitive posterior layer, allowing more physiological cell–ECM interaction than 2D culture or single scaffolds. AD iPSC organoids enable autologous modeling of genetic eye disorders (e.g., PAX6-related aniridia) and screening of personalized therapies, whereas organoid-derived material (cells, secretome/exosomes) can provide novel cell sources and regenerative constructs. Disease modeling and drug testing are also faster on organoid platforms, with increased predictive validity.64–66
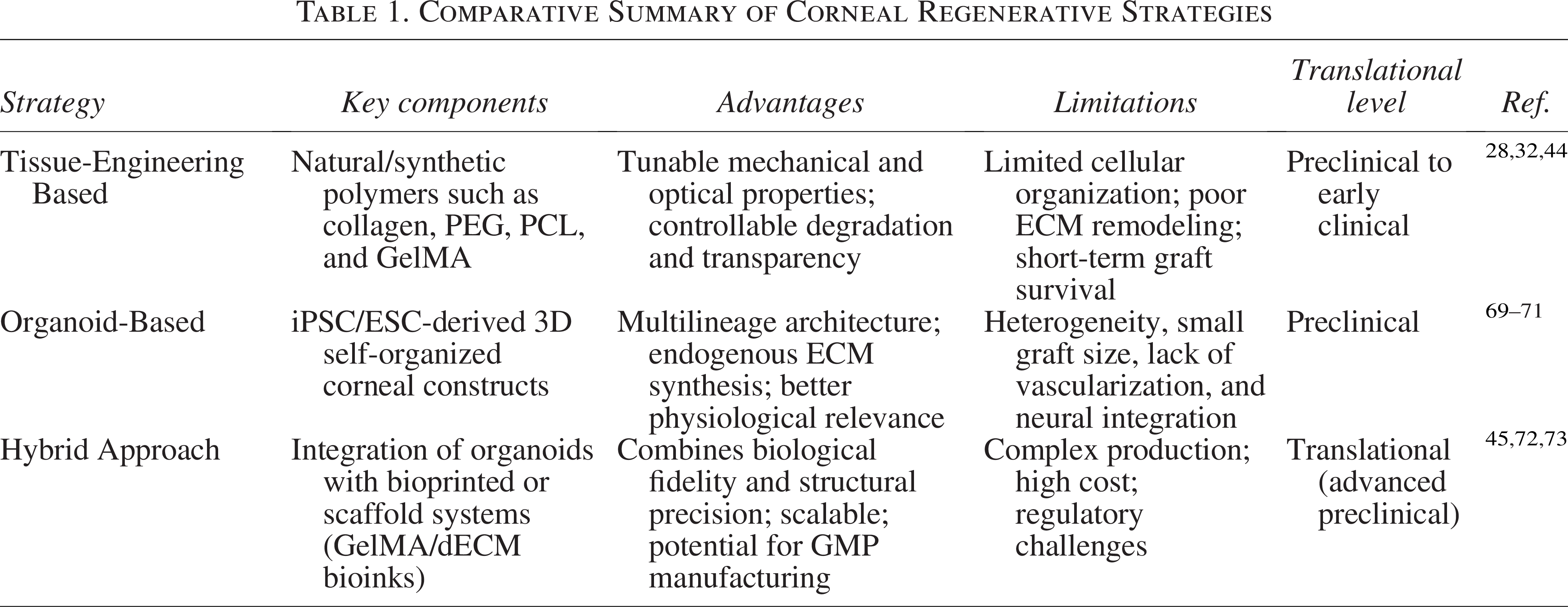
Restrictions are still significant to be considered. Organoids tend to be batch-heterogeneous, with patterning and size, generate small-scale, rather than clinical-scale grafts, and do not naturally vascularize and lack the immune system and stromal functions altogether. 67 This inhibits maturation, long-term survival, and in vivo predictability. Microfluidics, endothelial network coculture, scaffold guiding, and standardized bioprocessing reduce the variability and also support the corneal healing research. 68 Overall, organoid technology provides a physiological 3D platform for corneal biology, disease modeling, and a potential autologous source for regenerative therapies once engineering and scale-up challenges are addressed.59,63 Table 1 provides a comparison between the standard tissue engineering models and organoid and hybrid methods in regenerative strategies. Although the applications of tissue engineering and cell-based therapies have succeeded partially, organoid and hybrid systems offer structural and biological fidelity to next-generation corneal models.
Comparative Summary of Corneal Regenerative Strategies
Corneal Organoid Generation: Method and Protocol
The most commonly used cell-source options in corneal organoid projects include human iPSCs, embryonic stem cells (ESCs), and adult corneal progenitors. iPSCs are suitable for autologous approaches because they provide patient-specific, unlimited growth and genetic matching, but they need stringent pluripotency purges and directed differentiation to eliminate undifferentiated remnant cells.74–76 ESCs demonstrate strong differentiation and developmental capabilities and raise ethical and allogenicity concerns. 77 Mature progenitors of the cornea (limbal epithelial stem cells, stromal keratocytes, or donor-derived endothelial cells) are lineage-committed and less complex to differentiate, but constrained by the supply and proliferative potential of donors.77–79
The differentiation of corneal lineages follows a developmentally mimetic process: pluripotent cells are first patterned to form surface ectoderm, then specified to become corneal epithelial progenitors, with optional parallel signals that can induce neural-crest-derived stromal or endothelial progenitors. 80 Simple signaling pathways and short descriptions of simple roles of direct fate are BMP, which is ectodermally patterned, epidermal/ocular surface fated; WNT, which is temporally regulated, to balance the anterior eye field with the neural retina; FGF, which is proliferative, and TGF-b, which is selectively inhibited, in epithelial specification, to prevent mesenchymal transition, but is used to induce stromal ECM where needed. On a protocol timescale (days to weeks), these signs replicate embryonic windows.80–84 Figure 2 provides a visual timeline of corneal organoid differentiation, from PSC to mature organoids.
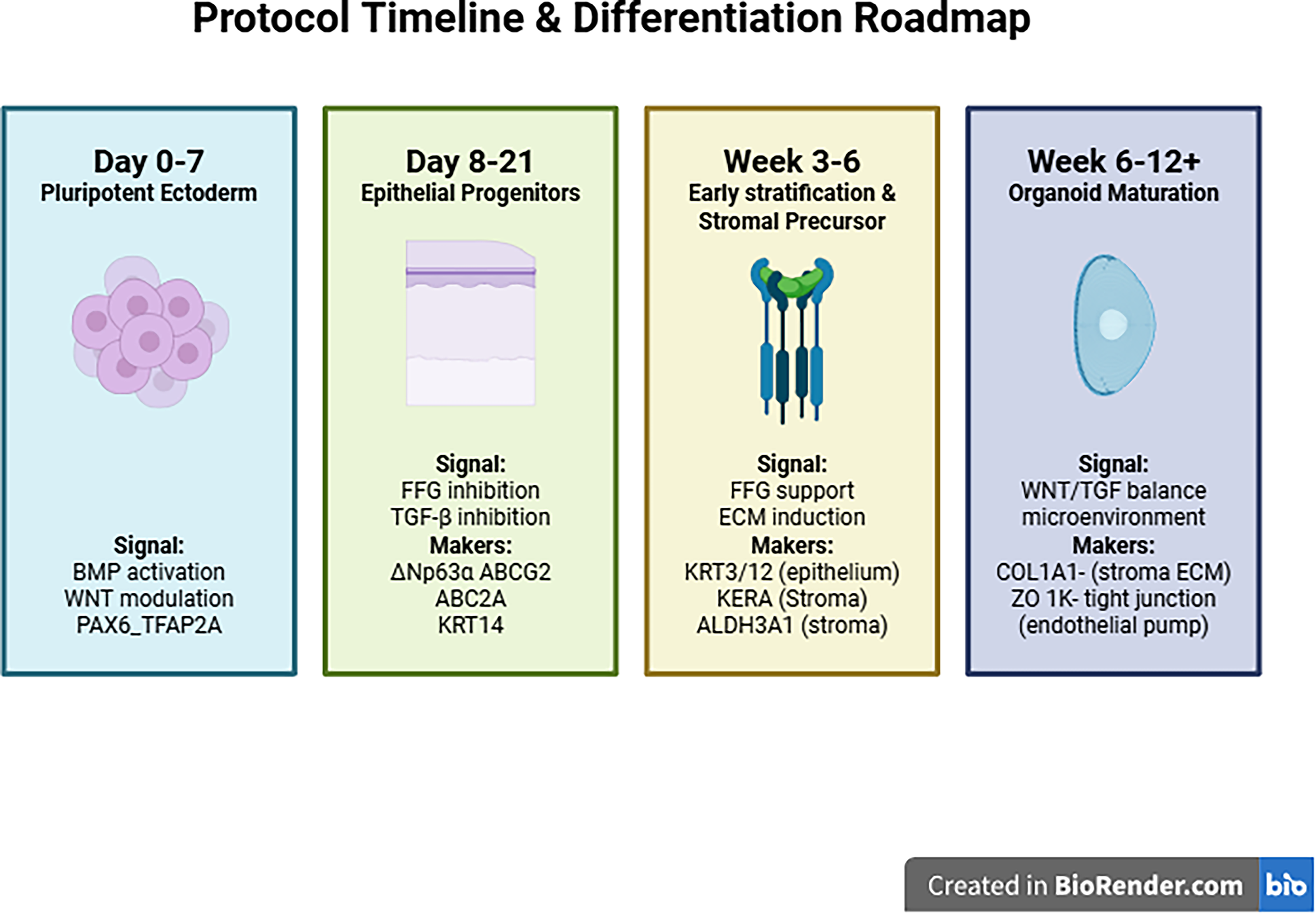
Protocol timeline for corneal organoid differentiation.
Three-dimensional culture formats induce tissue self-organization and maturation after induction into lineage. 85 Typical systems comprise ECM embedding (Matrigel or defined collagen/glycosaminoglycan [GAG] hydrogels) to allow lumenization and matrix deposition, ALI culture to enhance stratified epithelial differentiation and barrier function, and rotating or stirred bioreactors to enhance nutrient transport and scale-up; microfluidic culture and microfabricated wells can be used to improve uniformity and output.32,78,85–87 Important protocol variables include matrix composition and stiffness, oxygen tension, the timing and dosing of growth factors, and applied mechanical signs (shear, curvature): Softer matrices prefer epithelial stratification, and aligned/anisotropic scaffolds prefer stromal lamellar organization; hypoxia or low O2 phases can also regulate differentiation kinetics in some protocols.69,88
Bottlenecks, such as reproducibility and yield, remain viable. Different labs and protocols vary in their effectiveness. 89 Epithelial progenitor generation (ABCB5/ΔNp63α-positive) can be obtained in 2–4 weeks with feeder-free protocols, and corneal organoids with multilayered structure can be obtained in 6–12 weeks and demonstrate batch heterogeneity in size and proportions of cell types.74,84 Single-cell transcriptomics indicate that, after several months of culturing (∼3–4 months), organoids recapitulate fetal corneal cellular diversity. Although significant advances have been made in the production of organoids, there have been various problems in translational adaptation, like the absence of GMP-approachable pipelines of iPSC production, batch variation, potential of tumorigenesis, and risk of immune rejection. Unstandardized scalable bioprocessing, repeatability within regulatory quality frameworks. Clinical translation requires validated manufacturing processes, biosafety testing, and harmonization of regulatory regulations.70,77,90 For a quick reference, a practical timeline with stage-specific markers is summarized in Table 2.
Key Stages, Markers, and Features Observed during Stepwise Generation of Corneal Organoids from Pluripotent Stem Cells
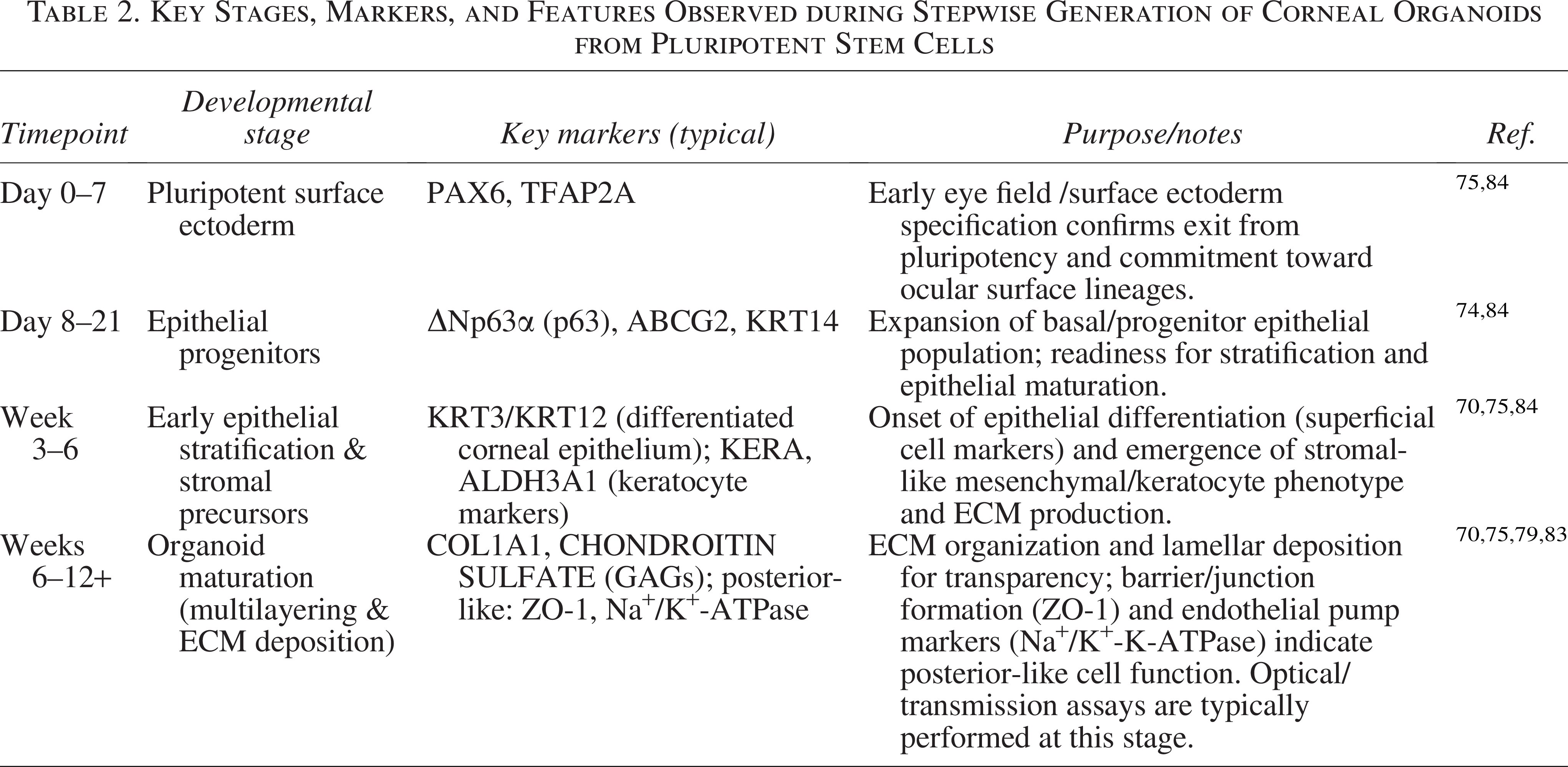
Layered epithelial organoids, stromal-like ECM, and infrequent endothelial-like cells are made in organoids derived from the iPSC system using protocols to isolate corneal organoids (Foster et al., Susaimanickam et al., and later optimized setups). They possess light transmittance, barrier formation, and lineage-specific marker expression, still with optical clarity like in the normal cornea, and an endothelial pump.70,74,75 Preclinical studies utilize small and large animal models to evaluate graft clarity, anatomic integration, epithelialization, stromal remodeling, endothelial control, and host response over time. Objective corneal clarity/scoring, graft–host aperture optical coherence tomography, histologic integration, endothelial cell density, functional deturgescence, and larger model behavioral/vision objectives are common.79,91,92
Functional Assessment of Corneal Organoids
The study focuses on the firm corneal organoid structure, optics, cellular identity, and fundamental physiology. Collagen organization is imaged using SHG microscopy, which is the gold standard for assessing collagen alignment and lamellar organization in terms of transparency and biomechanics. Multilayered epithelium and stromal compartments are checked by hematoxylin and eosin and immunofluorescence (IF).30,93 Quantitative measurements of visible-range light transmittance spectra, scattered measurements, and crude estimates of refractive indexes are all optical tests against human cornea standards (90% transmittance in the visible band; n ≈ 1.376).94,95
Cellular validation, marker panels, and function
The IF/quantitative reverse transcription polymerase chain reaction lineage markers include KRT3/12 and ΔNp63α for the epithelium, KERA and ALDH3A1 for the stroma, and ZO-1 and Na+/K+-ATPase for the endothelium, along with single-cell profiling to assess cell-type diversity.71,96 Na+/K+-ATPase activity and fluid-height assays/physiological swelling/deswelling tests assess the endothelial pump capacity in ex vivo models, and TEER or tracer permeability assesses barrier integrity.83,96,97 It is believed that manufactured corneal constructs can be functionally equivalent when they have an optical clarity of not less than 85–90% across the visual spectrum, a refractive index of approximately 1.376 ± 0.002, and Na+/K+-ATPase activity 80–100% of that of capillary functionality. All these measurements demonstrate that the material is nearly as clear as the human cornea.32,98 Topical chemical permeability and response are typified by the Franz diffusion cell or imaging-based penetration technique.99,100
Physiological responsiveness improves translational relevance
Wound-healing assays, cytokine/inflammatory stimulation (e.g., hyperosmolar or lipopolysaccharide challenge), and live calcium/electrophysiology (where innervation is modeled) report dynamic responses that are observed in vivo. 101
Minimal publishing criteria (best practice)
(i) Cell provenance and quality control (karyotype, mycoplasma), (ii) marker panel protocols/reagents, representative figures, (iii) histology and SHG collagen imaging, (iv) quantitative optical data (transmittance, scattering, refractive index), (v) functional assays (TEER/permeability; Na+/K+-ATPase/pump), (vi) reproducibility (n, interbatch variance), and (vii) data on limitations (vascular/immune absence, heterogeneity) and ethical/regulatory compliance.102,103 These minimums were found to make organoid claims credible and similar in different labs.
Comparative analysis shows that the organisms and bioprinted structures are 85–88% clear and have tensile strength of 0.25–0.45 MPa, whereas natural human corneas are clearer than 90% (400–700 nm) and have a strength of 0.3–0.7 MPa. Na+/K+-ATPase pump activity in adult corneal organoids is 70–90% that of real corneas.94,95 There are still long-term biomechanical and endothelial stability issues, but these values demonstrate functionality and optical fidelity, which is extremely close to what the body would have.
Biomaterials, Bioprinting, and Integration
Corneal organoids require a favorable biomaterial; the fibril spacing and hydration of low light scattering are maintained by natural collagen, proteoglycan, and basement membrane signaling GAG-rich matrices (hyaluronate and chondroitin sulfate).104,105 The dECM–GelMA hybrid bioinks, GelMA-fabricated gels, and tunable GelMA hydrogel platforms retain the fibril spacing and hydration to allow low light scattering.72,106–108 Spatial control (3D) bioprinting creates anisotropic collagen orientation and dome-shaped refractive power potential using extrusion and microfluidic nozzles, print-path programming, and shear alignment. 109 Applications of microfabrication and microfluidics include cornea-on-a-chip technology, high-throughput printing, and multimaterial printing. The multilayer epithelia–stroma structures exhibit intriguing optical and mechanical activities.109–111
Microfluidic and microfabrication of cornea-on-a-chip systems creates the shear of the tear film, regulated flow of nutrients and compartmentalized epithelial–stromal interfaces, maturation of the barrier, and dynamic testing of drugs.112–114 This can be done by printing with supportive bioinks or by seeding cells onto mechanically supportive scaffolds, such as suture-retaining rings, fiber-reinforced hydrogels, or thin nets, and being transparent.113,115–117
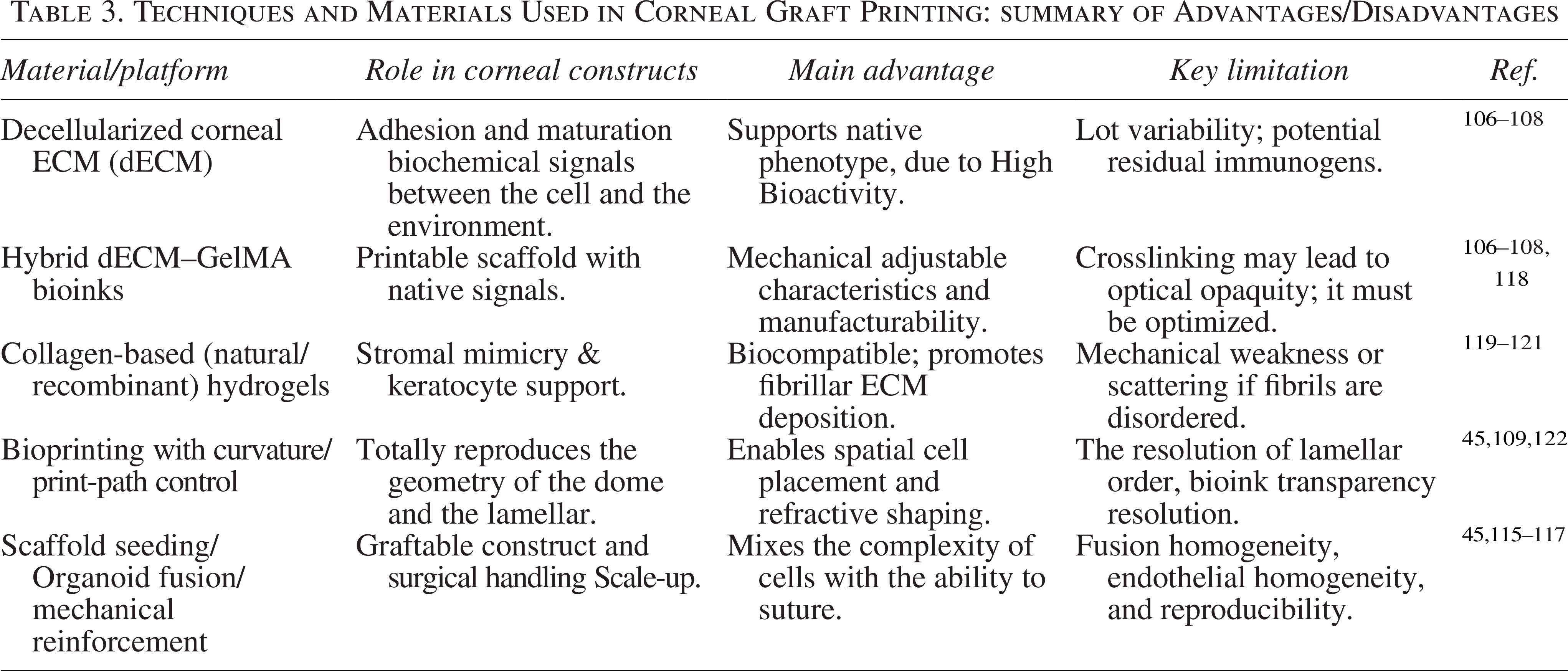
GelMA/dECM mixes are selective in differentiating ocular cells and enhance vision as compared to Matrigel. dECM contains native collagen and GAG that stabilize epithelial and stromal lineages, orderly development of the ECM, and 90% visible properties.106–108 GelMA also offers mechanical stability and variable stiffness to keep the keratocytes in the sleep state and retain the vascular integrity to enable the pump to work. New research results show that dECM has a lower immune response to foreign substances and generates batches that are easier to work with than Matrigel, enhancing translational stability. Combinations of GelMA and dECM are clear to the naked eye and are useful in eye research and can help in corneal organoids in a range of applications.72,106,107 Table 3 summarizes the comparison of key biomaterials and strategies in bioprinting in terms of their role, main benefits, and key limitations to enable graft design and translational prioritization.
Techniques and Materials Used in Corneal Graft Printing: summary of Advantages/Disadvantages
Preclinical Translation, Safety, and Regulatory Considerations
Small and large animal models are used in preclinical studies to determine graft clarity, anatomic integration, epithelialization, stromal remodeling, endothelial control, and host response over time. Common are objective corneal clarity/scoring, graft–host ocular stem cell transplantation, histologic integration, endothelial cell density, functional deturgescence, and larger model behavioral/vision objectives.123,124
Safety issues include immune rejection on the use of allogeneic or xenogeneic materials, tumorigenicity of remaining pluripotent cells following the differentiation of iPSCs, and off-target differentiation or secondary ectopic development.79,125 The risk mitigation strategies can be encompassed in the following: complete undifferentiated cell removals, approved potency and identity panel tests, preclinical tumorigenicity in vivo, and preclinical immune surveillance.79,83,125,126
Producing GMP-compliant stocks of iPSCs, repeating differentiation, potency tests with a given result, scaling of the process, and remaining in the same batches, sterility, and product stability are all significant. 127 Food and Drug Administration and European Medicines Agency prefer detailed CMC (Chemical, Manufacturing, Control) dossiers, strong potency analysis, bio/toxicology information, and long-term follow-up of cell/advanced therapy medicinal product (ATMP) products. Based on composition and working mechanism, regulation applies to synthetic corneal constructions as medical devices, biologics, or ATMPs/cell therapies.127–129 The preliminary regulatory decisions must be based on nonclinical data (efficacy, biodistribution, tumorigenicity, and immunogenicity) and clinical trial design. Some ethical concerns are donor-derived iPSC informed permission, privacy of genomic editing, and transparency of genetic editing. Early GMP, frequent potency testing, and stringent preclinical safety may be considered beneficial to the responsible translation.130,131
Future Directions
Differentiation regimes, potency scales, scalable and transparent scaffolds of maturation, and surgical manipulation are all required demands.45,109 Innovations with high impacts include gene-edited autologous organoids that repair hereditary defects before grafting, combinatoric strategies to restore corneal innervation, and bio-assembled grafts that integrate organoids with bioprinter stromal architecture to make suturable implants.45,132 CRISPR of targeted correction, lamellar alignment of 3D bioprinting of curvature, cornea-on-a-chip dynamic maturation devices of microfluidics, and quality assurance will accelerate preclinical testing.133,134 The personalized therapeutic perspectives and pathology-specific medication testing can be offered by patient-derived iPSC patches and cell-seeded dECM implants.135,136 Clinical translation therapies founded on pluripotent-cell ocular therapy are in human trials, and in the near future, cell-level interventions are anticipated. Full-thickness organoid-based grafts require scale-up, GMO qualification, and longer safety records before they can be utilized on large scale.137 Figure 3 shows the integration of emerging technologies for future applications.
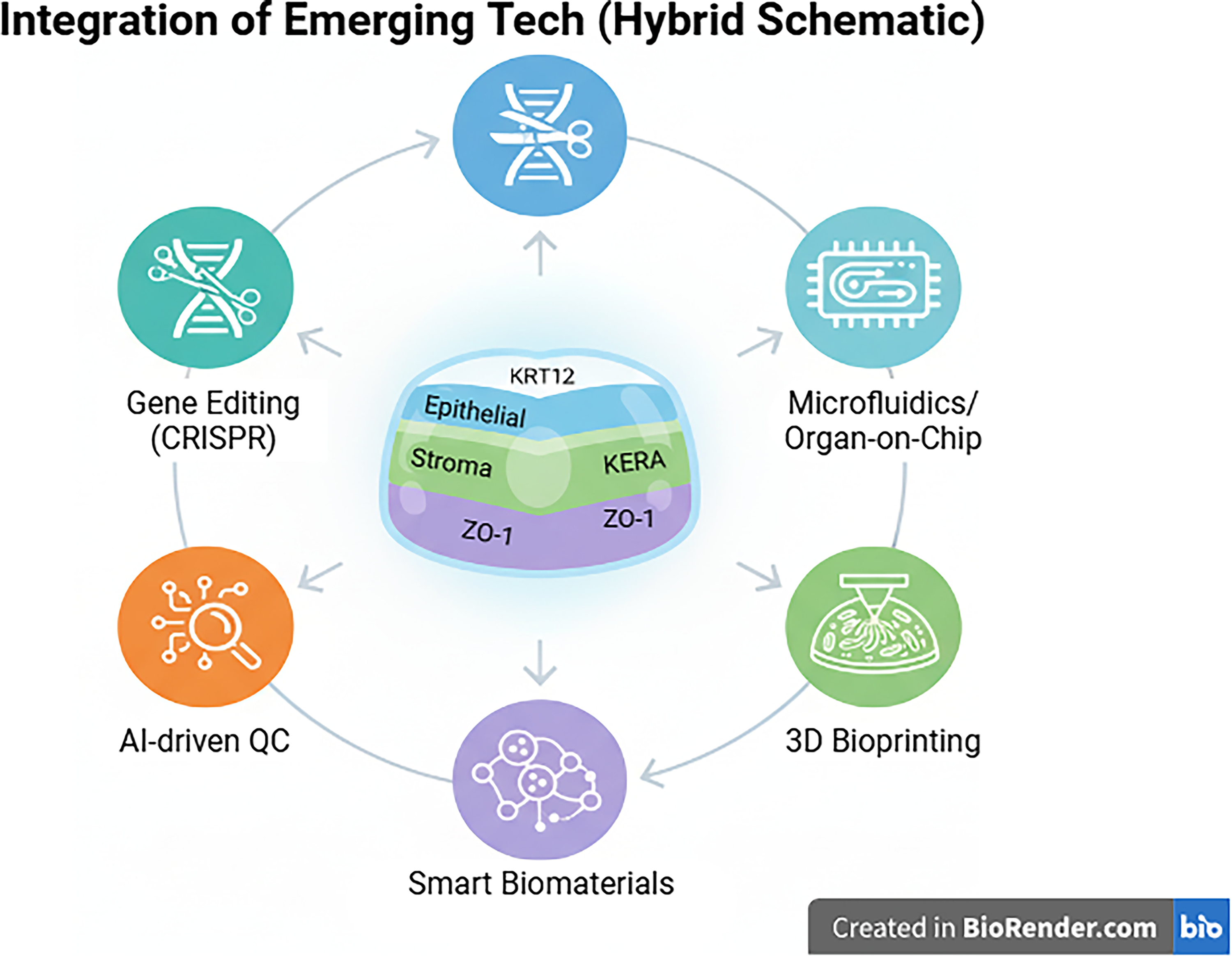
Emerging technologies for advanced corneal tissue engineering.
Conclusion
Corneal organoid engineering provides a viable, alternative donor-free way of restoring vision. Using endothelial, stromal, and transparency replication of the corneal lineages derived using iPSC with biomimetic scaffolds and precision bioprinting will be possible. The translation priorities are GMP scale-up, standardized assays of optical and pump function, strong tumorigenicity and immunogenicity testing, and reasonable regulatory frameworks. The next steps to be undertaken involve multicenter Phase I/II trials, manufacturing process validation, and combining with gene-correction and microfluidic maturation platforms. In the event of these milestones being achieved, organoid-based grafts may be reproducible, safe, and commonplace clinical options in 10 years. This will change the world’s access to permanent corneal treatments, and blindness will be minimized.
Authors’ Contributions
M. Azhar.: Writing—original draft preparation. R.M.: Supervision and final drafting. P.C.: Writing—original draft preparation. S.S.: Writing—original draft preparation. A.D.A.: Data curation and methodology. M. Abohashrh.: Data curation, conceptualization, and final drafting. All authors reviewed and approved the article.
Footnotes
Acknowledgment
The authors extend their appreciation to the Deanship of Research and Graduate Studies at King Khalid University for funding this work through the Large Research Project under grant number RGP.2/731/46.
Funding Information
The authors extend their appreciation to the Deanship of Research and Graduate Studies at King Khalid University for funding this work through Large Research Project under grant number RGP.2/731/46.
Disclosure Statement
No competing financial interests exist.